
Abstract
Objectives
First Nations people report high levels of wellness despite high rates of chronic illness. Our goal was to understand the factors associated with wellness among First Nations adults in Ontario who were considered frail.
Methods
Using the First Nations Regional Health Survey, we created a profile of First Nations adults (aged 45+) who were categorized as “frail” (weighted sample size = 8121). We used multivariate logistic regression to determine associations between wellness (as measured by self-reported physical, emotional, mental, and spiritual balance) and determinants of health.
Results
Rates of reported wellness were high among those who were frail, ranging from 56.7% reporting physical balance to 71.6% reporting mental balance. Three key elements were associated with wellness: the availability of resources, individual lifestyle factors, and cultural connection and identity.
Discussion
Our findings provide a profile of strength and wellness among older First Nations adults living with frailty.
Background
Recent aging research has focused on older adults with complex health needs, as overlapping comorbidities are frequently experienced later in life (Bunn et al., 2014; First Nations Information Governance Centre (FNIGC) & Walker, 2020). Adults who experience a combination of health deficits in old age have often been described as “frail” (Pan et al., 2019), a syndrome characterized by a reduction in physiological reserve, a limited ability to resist environmental stressors, and an increased risk of functional decline (Bergman et al., 2007; Strandberg & Pitkälä, 2007). Chronic illness has been identified as a major determinant of frailty, although it also can result from a broad array of symptoms and functional impairments (Onder et al., 2018). The occurrence of frailty is associated with increasing age, both among Canadian seniors (Hoover et al., 2013; Jones et al., 2005; Rockwood et al., 2011; Song et al., 2010) and among older First Nations people (FNIGC & Walker, 2020; Slater et al., 2020). However, similar to many individual chronic diseases, frailty appears to affect First Nations people at earlier ages (Jacklin et al., 2013; Slater et al., 2020). In fact, frailty levels among First Nations adults aged 45–54 years old are similar to those seen in the general Canadian population between the ages of 65 and 74 (FNIGC & Walker, 2020; Slater et al., 2020). Compared to other populations in Canada, First Nations populations also have higher rates of many chronic conditions, and an increased likelihood of experiencing multiple comorbid conditions (Caron-Malenfant & Morency, 2011; FNIGC, 2012, 2018; J. L. Reading, 2011; Riediger et al., 2014; Wilson et al., 2011). First Nations populations also experience limited access and prohibitive barriers to health and healthcare services (FNIGC, 2018; Slater et al., 2020). This is especially relevant as the population of older First Nations people in Canada is expected to dramatically increase, with those aged 65 and over expected to nearly triple in number by 2036 (Morency et al., 2015).
Despite facing challenges with health and healthcare, First Nations people report high levels of wellness (FNIGC & Walker, 2020). In part, this may be explained by the distinction between health and wellness, wherein the former typically assumes the biomedical understanding of physical robustness, whereas First Nations’ perceptions of wellness encompass knowledge, culture, language, worldviews, and spirituality (FNIGC, 2018). Broadly, wellness includes spiritual, mental, emotional, and physical health, and overall wellness is achieved when each domain is in balance (Castellano, 2015). Spiritual balance can be expressed through traditional and religious belief, emotional balance pertains to attitude and relationships, mental balance includes intuition and clarity, and physical health includes the body as a whole. While considerable diversity exists within and between First Nations across Canada, and each nation may have distinct understandings, beliefs, and practices, these indicators of wellness are core to understanding how First Nations people keep themselves “balanced” and healthy (FNIGC, 2018).
In Canada, over 90% of First Nations adults with chronic conditions report feeling balanced in the four domains of life (physical, emotional, mental, and spiritual); these findings are not significantly different from First Nations adults with no chronic conditions (FNIGC, 2018). First Nations seniors across Canada who are experiencing frailty are more likely to report feeling balanced in the four domains of life (i.e., physical, emotional, mental, and spiritual balance) compared to those who are not frail (FNIGC & Walker, 2020). However, little is known about the factors underlying these findings. Why do First Nations people report feeling well in the face of frailty? The primary objective of this cross-sectional study is to understand what contributes to feelings of wellness among First Nations adults in Ontario who are considered to be frail.
Methods
This work is part of a larger study on aging in First Nations populations in Ontario (Slater et al., 2020; Walker et al., 2019). Using a participatory approach, the study was co-developed by academic researchers and the Chiefs of Ontario and was guided by a First Nations-led approach based on principles of First Nations data sovereignty (Walker et al., 2017). The lead academic investigators have a longstanding, collaborative relationship with the Chiefs of Ontario and many First Nations communities across Ontario (Walker et al., 2018). Community partners were involved in all stages of the project and actively participated as co-investigators in the conception, design, analysis, and interpretation of the results. We engaged a First Nations Knowledge Circle, involving community members and traditional Knowledge Keepers, who contributed knowledge of aging and experiences with frailty and comorbidity, and navigating the health care system. The Knowledge Circle was engaged throughout the project to ensure that the results of this work were both grounded in and respected First Nations knowledge and processes.
Data Source
The First Nations Regional Health Survey (FNRHS) is a national cross-sectional survey and the only source of national health-related data for First Nations people living in First Nations communities. By “First Nations communities,” we mean those living in federally recognized Indian Reserves, which are tracts of land set aside for the use of Indian Bands according to the Indian Act (Indian Act, RSC 1985). To date, three phases of the FNRHS have been conducted; this project uses data from the Ontario Region Phase 2 of the FNRHS, which was conducted between August 2008 and November 2010 in 24 First Nations communities across Ontario.
The sample is designed to represent all First Nations people living in First Nations communities across Ontario. The two-stage sampling strategy involved: a) stratified selection of communities to participate in the survey and b) selection of individuals within the communities sampled (FNIGC, 2012). The weighted sample of the FNRHS Phase 2 represents a total of 79,903 First Nations people in Ontario.
Measures
Frailty
We followed the methodology used by a previous study of frailty in First Nations seniors (FNIGC & Walker, 2020; Slater et al., 2020) and applied a modified frailty index originally developed for use in the Canadian Community Health Survey and validated in the general Canadian population aged 65 years and older (Hoover et al., 2013). The frailty index counts the number of health problems or “deficits” (e.g., comorbidities, symptoms, and functional impairments) experienced by an individual, divided by the total number of deficits included in the index, to create a “frailty index” which ranges between 0 and 1 where higher values indicate greater levels of frailty. The modified frailty index used for the FNRHS contained 26 of the original 30 deficits (FNIGC & Walker, 2020). Based on the cut-offs defined for the general Canadian population (Hoover et al., 2013), we classified First Nations people as being frail (frailty index >0.21) versus those who are not frail (frailty index <0.1) or considered pre-frail (frailty index between 0.1–0.21).
Wellness
We considered a set of four questions in the FNRHS that asked respondents about life balance to describe a First Nations perspective of wellness. The questions ask: “How often do you feel that you are in balance in the four aspects of your life (physical, emotional, mental, and spiritual)?” and have possible responses of “all of the time,” “most of the time,” “some of the time,” and “almost none of the time.” For each question, we defined a binary variable by combining the responses of “all” with “most of the time” and “some” and “almost none of the time” to classify respondents as being in balance versus being not in balance.
Determinants of Health
The FNRHS asks respondents a number of questions across a number of domains, including demographic information, health and health care access, and lifestyle and health behaviors. We used a First Nations determinants of health framework to identify relevant social, demographic, and cultural factors (C. L. Reading & Wien, 2009) and ensured that we considered factors that contextualized risk and exposure over the life course. Following this framework, we categorized each determinant of health as being proximal, intermediate, or distal. Proximal determinants include factors that directly impact health such as health behaviors, whereas intermediate determinants include system capacity, resources, and infrastructure, and distal determinants include the social, political, and economic contexts that in turn influence intermediate and proximal determinants (C. L. Reading & Wien, 2009).
Based on the framework, we identified determinants of heath focused on lifestyle factors, living environment, food security, traditional culture, and residential school attendance, based on the availability of questions in the FNRHS and represented each determinant of health through a binary variable. Some questions in the FNRHS have simple categorical response variables (e.g., “Do you currently working for pay?” and “Do you use traditional medicine?” have response options of “yes,” “no,” “don’t know,” and “refused”; the FNRHS treats both “don’t know” and “refused” as missing data). Other questions have Likert scale responses (e.g., “Do you eat a nutritious balanced diet?” and “Do you take part in your local community’s cultural events?” have response options of “always/almost always,” “sometimes,” “rarely,” “never,” “don’t know,” and “refused,” with “don’t know” and “refused” treated as missing data). In these cases, we collapsed the “sometimes,” “rarely,” and “never” categories. In addition, the First Nations Information Governance Centre has derived standard composite variables from a combination of a number of different responses, including ones to identify crowded housing and food insecurity. Finally, in some cases, we combined responses from a number of related questions to form a composite variable. For example, the FNRHS asks seven different questions related to substance use; each question is specific to a substance with response options of “never,” “once or twice,” “ monthly,” “weekly,” “daily or almost daily,” “don’t know,” and “refused.” We created a binary variable to capture any illicit drug use (i.e., any answer other than “never,” “don’t know,” or “refused” for any of the seven substances).
Analysis
To meet data governance requirements, we conducted all analyses at the Chiefs of Ontario (COO) offices in Toronto, Ontario, Canada, under the supervision of COO staff. We used SPSS version 25 with the Complex Sampling Module to account for the sampling design in the FNRHS. The First Nations Information Governance Centre provides weights for the survey data based on the complex stratified sampling procedure (FNIGC, 2012). Our analysis focused on the subset of adults, aged 45+, who were classified as frail based on the frailty index. We selected this age range as our previous work found that First Nations experience frailty at younger ages compared to non-First Nations adults (FNIGC & Walker, 2020; Slater et al., 2020).
We created a profile of First Nations adults who were frail by estimating percentages and 95% confidence intervals (CIs) across selected determinants of health. We also determined the percentage of frail First Nations adults who self-reported being in physical, emotional, mental, and spiritual balance as well as the percent who reported excellent or very good self-rated health. We treated each balance measure as a response variable and tested bivariate relationships between wellness and determinants of health (explanatory variables), estimating both crude and age-sex adjusted odds ratios (ORs) and associated 95% CIs using multivariate logistic regression. Following First Nations Information Governance Centre policies, small cell counts (≤5) were suppressed. Coefficients of variation (CV) were calculated for each estimate; any estimate with a CV >33.3 was suppressed due to high sampling variability. Estimates with a CV between 16.6 and 33.3 should be interpreted with caution; these are noted appropriately in the results.
Results
Overall, 838 adults aged 45 years and older responded to the FNRHS in Ontario, representing a weighted count of 22,944 people. Thirty-five percent (35.4%; weighted n = 8121) of these respondents were classified as being frail and make up the study sample analyzed in this work.
Profile of First Nations Adults Age 45 years and Older Who Meet the Frailty Criteria (Weighted n = 8121).
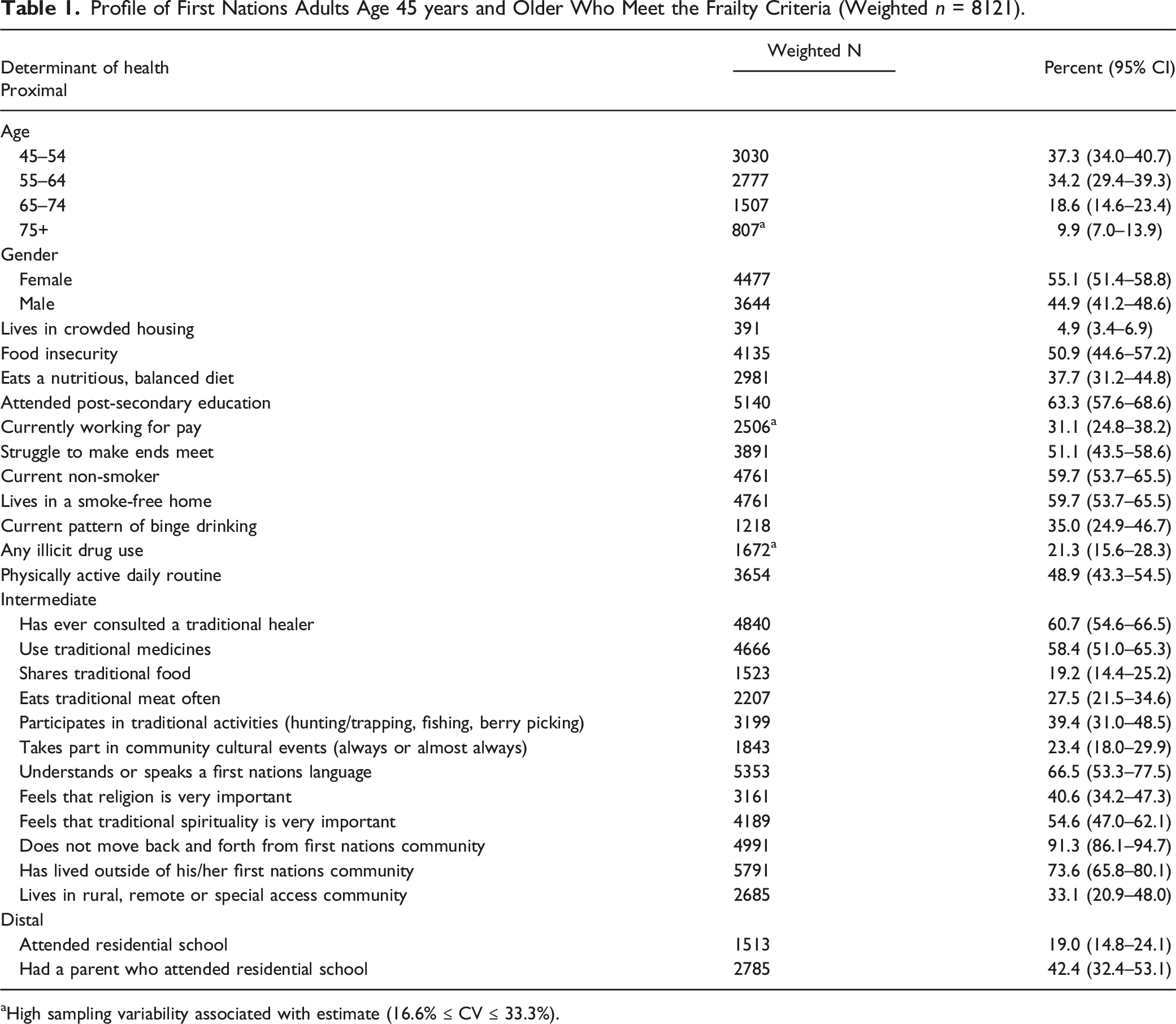
aHigh sampling variability associated with estimate (16.6% ≤ CV ≤ 33.3%).
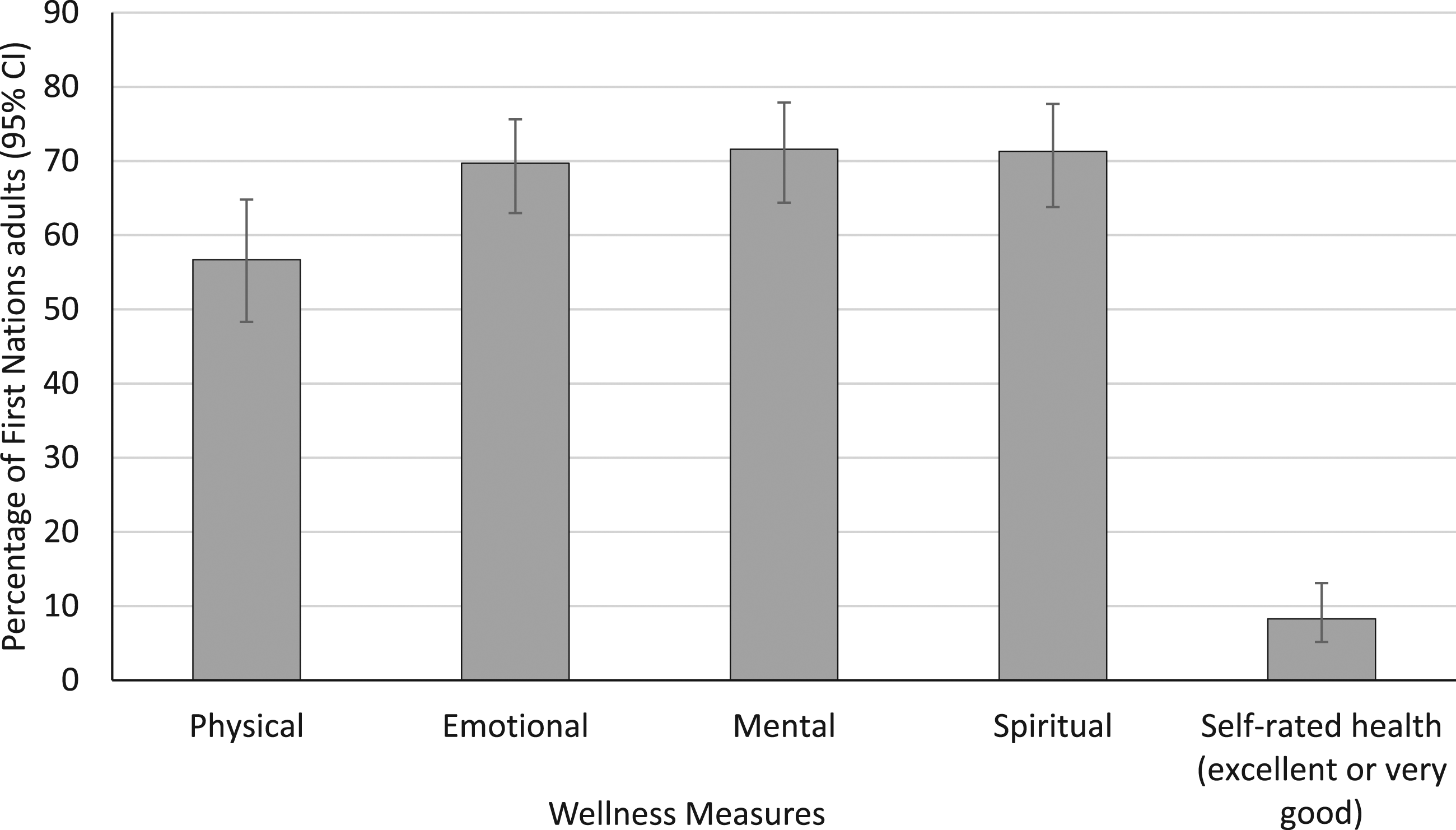
Wellness measures among First Nations adults 45+ who meet the frailty criteria (weighted n = 8121).
We found a number of factors that were positively and negatively associated with each of the four balance measures (Figure 2). Associations with spiritual, mental, emotional, and physical health.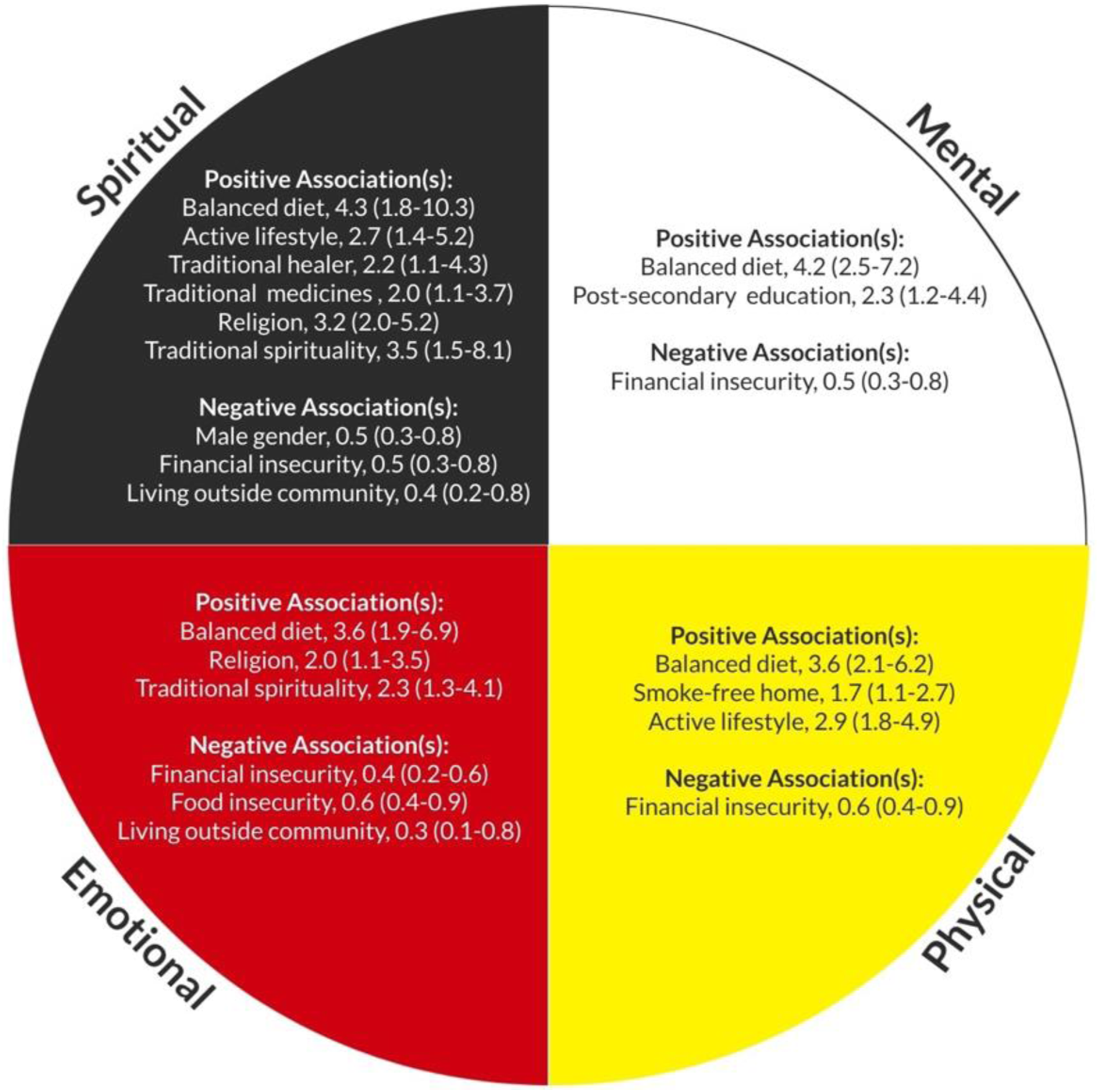
Positive Associations With Balance Measures
Adjusting for age and sex, First Nations adults with frailty were more likely to report being in physical balance if they ate a balanced diet (OR: 3.6, 95% CI: 2.1–6.2), lived in a smoke-free home (OR: 1.7, 1.1–2.7), and had an active daily routine (OR: 2.9, 1.8–4.9) (Appendix). Emotional balance was more likely in those who ate a balanced diet (OR: 3.6, 1.9–6.9) and those who felt that religion (OR: 2.0, 1.1–3.5) or traditional spirituality (OR: 2.3, 1.3–4.1) was important. Mental balance was associated with post-secondary education attendance (OR: 2.3, 1.2–4.4), and having a balanced diet (OR: 4.2, 2.5–7.2). Lastly, spiritual balance was associated with having an active daily routine (OR: 2.7, 1.4–5.2), having a balanced diet (OR: 4.3, 1.8–10.3), consulting with a traditional healer (OR: 2.2, 1.1–4.3), using traditional medicines (OR: 2.0, 1.1–3.7), and feeling that religion (OR: 3.2, 2.0–5.2) or traditional spirituality (OR: 3.5, 1.5–8.1) are important.
Negative Associations With Balance Measures
Those who reported struggling to make ends meet (i.e., financial insecurity) were less likely to report being in physical (OR: 0.6, 0.4–0.9), emotional (OR: 0.4, 0.2–0.6), mental (OR: 0.5, 0.3–0.8) or spiritual balance (OR: 0.5, 0.3–0.8). Those who reported food insecurity were also less likely to report emotional balance (OR: 0.6. 0.4–0.9). Lastly, those who reported previously living outside of their First Nations community were less likely to report being in emotional (OR: 0.3, 0.1–0.8) or spiritual balance (OR: 0.4, 0.2–0.8).
Discussion
First Nations adults living in First Nations communities in Ontario report high levels of wellness, despite being categorized as frail, similar to findings reported at a national level (FNIGC & Walker, 2020). We identified a number of proximal and intermediate factors that are associated with the experience of wellness in First Nations adults who are living with frailty. Upon further examination, these factors appear to fall into three key elements: resources, individual lifestyle factors, and cultural connection and identity. Resources (e.g., living in a smoke-free home, financial security) are likely pre-existing, pre-dating the development of frailty and are thus difficult for individuals or clinicians to change or intervene on, though speak to the importance of inclusive health policy (Richmond & Cook, 2016). Individual lifestyle factors such as diet or activity levels can potentially be modified, and also seem to contribute to improved well-being among those living with frailty. Lastly, cultural connection and identity, such as living within a First Nations community or using traditional spirituality or medicine, seems to be associated with higher levels of balance in First Nations adults living with frailty.
First Nations Peoples often emphasize a holistic understanding of good health in old age, in contrast to the biomedical model dominant in Western discourse (Castellano, 2015; Vukic et al., 2011). Restricted largely to physical health, frailty and self-rated health are generally medicalized, deficit-based concepts which fail to capture aspects of wellness such as spirituality. For First Nations people, contributors to aging well can include many factors, including living a healthy lifestyle, engaging with community, and maintaining traditional cultural values (Brooks-Cleator et al., 2019; Pace & Grenier, 2016). These variations in the definition of health may partially explain the discrepancy between the large proportion of First Nations people reporting high levels of wellness and balance and the small proportion reporting high levels of self-rated health (Slater et al., 2020). A study of mental health among Indigenous peoples living in Canada used a broad definition of mental health and found a large proportion of Indigenous peoples reporting high levels of mental wellness despite the high rates of mental illness seen in the same populations. While not an Indigenous concept of health, this more inclusive definition included psychological and social well-being as well as general life satisfaction and the authors suggest that amidst socioeconomic disadvantages and high rates of physical health conditions, these results point to substantial resilience in Indigenous populations in Canada (Fuller-Thomson et al., 2020).
Importantly, recent research has shown that many older adults do not identify with the label of “frailty” as it has a negative connotation and it may even signify resignation or defeat (Grenier, 2006; Pan et al., 2019; Warmoth et al., 2016). This also appears to be true in First Nations communities, where focus groups with older members of a First Nations community has shown that the notion of aging well and staying well is more important than the concept of frailty (Walker et al., 2019). The concepts of resilience and adaptation appear to be preferred by older adults over the label of “frailty” (Pan et al., 2019). Resilience, promoted by physical health, a sense of self, social belonging, self-belief, and altruism, has been suggested as being inversely associated with frailty (Rebagliati et al., 2016; Whitson et al., 2016; Woo et al., 2005); however, others have argued that resilience does not simply equate to the absence of frailty (Kuchel, 2018). The results from this study support the notion that resilience can instead be characterized as adaptation in the face of adversity, whereby several pathways exist to help First Nations adults experiencing frailty to achieve wellness (Kirmayer et al., 2011).
Our findings suggest that cultural connection and identity appears to be strongly associated with both emotional and spiritual balance among First Nations adults living with frailty. Kirmayer et al. (2011) describe sources of resilience as being dynamic and emerging from interactions between individuals and communities. While colonization has hindered the preservation of traditional knowledge, beliefs, and practices, the cultural knowledge of First Nations people continues to be maintained and expressed though ways of living, contributing to a foundation of resilience (George et al., 2018; Health Canada, 2015). For example, active involvement in the community as an Elder has been shown to contribute to overall well-being (Baskin & Davey, 2015; Pace & Grenier, 2016). This may be reflected in our results, as those who previously lived outside of their communities were less likely to report spiritual balance, potentially due to the lack of recognition of Elder roles within their community. Consistent with the literature (George et al., 2018), our findings also highlight the importance of traditional healing practices for spiritual balance in First Nations adults. George et al. (2018) surveyed First Nations communities in Ontario and found that over half of those who did not use traditional healing practices were interested in doing so; however, many lacked the knowledge to implement the practice.
Our findings suggest that a healthy lifestyle, including diet and exercise, is associated with wellness and balance across all four domains. As a proximal determinant of health, lifestyle factors such as having a balanced diet have a direct impact on health in old age. Lifestyle factors also have a cumulative effect throughout the life course, where a poor diet in youth can lead to increased susceptibility to illness in old age (Kim, 2019; C. L. Reading & Wien, 2009). While the connection between nutrition and improved physical health in old age has been well established, our results also point to the widespread influence of a nutritional diet on emotional, spiritual, and mental health as well. Conversations with First Nations community members in Northern Ontario highlighted the cultural significance of traditional foods in First Nations communities (Socha et al., 2012). Although these foods have higher nutritional value than processed foods, their lack of availability in many First Nations communities often makes them difficult to include in one’s diet (Haman et al., 2010). Interestingly, a balanced diet was found to be associated with spiritual, mental, and emotional balance, but eating and sharing traditional food was not a significant finding. This may in part be related to the limited availability of traditional foods in many First Nations communities (Haman et al., 2010).
Limitations
This study examined associations between determinants of health and the four domains of wellness and balance among First Nations adults who are categorized as frail. First, in interpreting our results and examining the relationships between balance domains and life factors, it is important to acknowledge that this is a cross-sectional study. Secondly, as we were guided by the First Nations concept of wellness which focus on four domains of balance, we did not assess whether those domains themselves were correlated. One can imagine that the domains of emotional, mental, and spiritual balance may be similar. Lastly, our data came from participants living in First Nations communities so may not be generalizable to people living outside of First Nations communities or in urban settings. Our results also reflect the time of data collection of Phase 2 of the FNRHS (data collected between 2008–2010), as this was the best available source of the rich data required to study both frailty and resilience factors among First Nations adults.
Conclusion
Our findings provide a profile of strength and wellness among First Nations adults living with frailty. As First Nations communities take steps to improve well-being through health system transformations that offer sustainable, culturally based and holistic care options (Assembly of First Nations, 2017), understanding that the availability of resources, individual lifestyle factors, and cultural connection and identity are associated with wellness allows for the development of strengths-based interventions to improve outcomes for people living with frailty (Beswick et al., 2008; Clegg & Young, 2011; Ellis et al., 2011; Morley et al., 2013; Rodriguez-Mañas & Fried, 2015).
Footnotes
Factors Associated with Being in Physical,Emotional,Mental,and Spiritual Balance (Crude Odds Ratios,95% Confidence Intervals).
Determinant of health
Physical
Emotional
Mental
Spiritual
Proximal
Age
45–54
0.4 (0.2–1.2)
0.6 (0.3–1.4)
0.9 (0.4–2.0)
0.8 (0.3–1.7)
55–64
0.9 (0.3–1.7)
0.6 (0.2–1.5)
0.5 (0.2–1.5)
0.6 (0.3–1.4)
65–74
1.2 (0.5–2.6)
1.1 (0.4–2.9)
1.3 (0.5–3.3)
2.0 (0.8–5.2)
75+
Reference
Reference
Reference
Reference
Gender: Male
1.0 (0.5–2.0)
0.6 (0.3–1.1)
0.5 (0.2–1.0)
0.5 (0.3–0.8)
Lives in crowded housing
0.9 (0.4–2.1)
0.7 (0.3–1.9)
0.5 (0.2–1.1)
0.7 (0.3–1.6)
Food insecurity
0.8 (0.5–1.3)
0.6 (0.4–0.9)
0.7 (0.4–1.3)
0.7 (0.4–1.4)
Eats a nutritious, balanced diet
3.6 (2.1–6.2)
3.6 (1.9–6.9)
4.2 (2.5–7.2)
4.3 (1.8–10.3)
Attended post-secondary education
1.1 (0.6–2.0)
1.3 (0.7–2.5)
2.3 (1.2–4.4)
1.3 (0.7–2.1)
Currently working for pay
1.0 (0.6–1.6)
1.3 (0.7–2.4)
1.6 (0.8–3.1)
0.9 (0.5–1.7)
Struggle to make ends meet
0.6 (0.4–0.9)
0.4 (0.2–0.6)
0.5 (0.3–0.8)
0.5 (0.3–0.8)
Current non-smoker
1.3 (0.7–2.3)
1.3 (0.6–2.5)
1.0 (0.5–1.8)
1.1 (0.6–1.9)
Lives in a smoke-free home
1.7 (1.1–2.7)
1.7 (0.9–3.1)
1.4 (0.7–2.9)
1.7 (1.0–2.9)
Current pattern of binge drinking
2.0 (0.7–5.2)
1.1 (0.4–2.8)
1.0 (0.4–2.6)
0.9 (0.4–2.4)
Any illicit drug use
0.8 (0.4–1.7)
0.7 (0.3–1.7)
1.0 (0.4–2.5)
0.6 (0.3–1.5)
Physically active daily routine
2.9 (1.8–4.9)
2.1 (1.0–4.4)
1.8 (0.9–3.8)
2.7 (1.4–5.2)
Intermediate
Has ever consulted a traditional healer
0.9 (0.6–1.5)
1.9 (1.0–3.7)
1.5 (0.7–3.0)
2.2 (1.1–4.3)
Use traditional medicines
1.2 (0.7–2.0)
1.6 (0.8–3.0)
1.4 (0.7–2.8)
2.0 (1.1–3.7)
Shares traditional food
1.4 (0.7–2.7)
1.1 (0.6–2.0)
0.5 (0.2–1.5)
1.5 (0.8–3.0)
Eats traditional meat often
1.5 (0.8–2.8)
1.3 (0.7–2.5)
1.0 (0.5–2.4)
1.5 (0.9–2.4)
Participates in traditional activities (hunting/trapping, fishing, berry picking)
1.0 (0.6–1.8)
0.7 (0.4–1.2)
0.5 (0.3–1.1)
0.5 (0.3–1.0)
Takes part in community cultural events (always or almost always)
1.3 (0.6–2.7)
1.4 (0.6–3.4)
0.8 (0.3–2.5)
1.6 (0.5–5.0)
Understands or speaks a first nations language
1.5 (0.7–3.1)
1.5 (0.8–2.8)
1.2 (0.6–2.5)
1.3 (0.6–2.8)
Feels that religion is very important
1.4 (0.8–2.7)
2.0 (1.1–3.5)
1.2 (0.7–2.3)
3.2 (2.0–5.2)
Feels that traditional spirituality is very important
1.5 (0.9–2.6)
2.3 (1.3–4.1)
1.6 (0.9–2.9)
3.5 (1.5–8.1)
Does not move back and forth from first nations community
1.2 (0.3–4.4)
1.1 (0.3–4.4)
1.1 (0.2–5.2)
1.5 (0.4–6.2)
Has lived outside of his/her first nations community
0.8 (0.4–1.7)
0.3 (0.1–0.8)
0.7 (0.3–1.5)
0.4 (0.2–0.8)
Lives in rural, remote or special access community
1.5 (0.8–2.9)
1.0 (0.5–1.8)
1.2 (0.7–2.0)
1.1 (0.5–2.2)
Distal
Attended residential school
0.7 (0.3–1.8)
0.5 (0.2–1.2)
0.4 (0.1–1.1)
0.4 (0.2–1.1)
Had a parent who attended residential school
1.4 (0.7–2.7)
1.7 (0.8–3.6)
1.1 (0.5–2.4)
2.1 (0.9–5.0)
Acknowledgments
The authors would like to acknowledge the important contributions of the First Nations Aging Study Knowledge Circle: Derek Debassige and Annie O’Brien, and the Dementia Research Community Advisory Council and Anishinaabemowin Language Group on Manitoulin Island. We also would like to acknowledge the contributions of David Henry, Susan Bronskill, Janet Smylie, Donna Loft, Karen Pitawanakwat, Graham Mecredy, and Maureen Gustafson.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Canadian Institutes of Health Research (Operating Grant).
Ethical Approval
This project was reviewed and approved by the Research Ethics Board of Laurentian University. In addition, it was reviewed and approved for relevance and compliance to the First Nations principles of research and data ownership, control, access and possession (OCAP ®) by the First Nations Health Coordination Unit, which is coordinated and supported by the Chiefs of Ontario.