
Abstract
Keywords
Background
With populations aging, multimorbidity defined as accumulating multiple chronic conditions has increased over the years (Barnett et al., 2012; Nunes et al., 2016; Rosella et al., 2018). The prevalence of multimorbidity is as high as 99% and 72% in primary care and general population studies (Fortin et al., 2012). The prevalence of multimorbidity increases with age with more than 65% of older adults being multimorbid after the age of 65 (Barnett et al., 2012; Roberts et al., 2015). Physical and mental disorders are highly comorbid reaching 31% in older adults, and the presence of a mental disorder increases with the number of physical disorders (Barnett et al., 2012).
Prior research shows that physical and mental multimorbidity is associated with increased health service use and excess health system costs in older adults (Vasiliadis et al., 2016) and mortality (Chwastiak et al., 2010; Rosella et al., 2018; Schiltz et al., 2019; Nunes et al., 2016; Walker et al., 2015; Willadsen et al., 2018). Years of life lost attributable to the presence of mental disorders in men and women reach 10.2 and 7.3 years, with the highest excess mortality in individuals with respiratory disorders and alcohol misuse (Erlangsen et al., 2017).
In developed countries, increasing socioeconomic inequalities have important consequences on the distribution of chronic conditions and mortality rates (Bor et al., 2017; Borell et al., 2014; Sommer et al., 2015). Higher mortality rates associated with mental disorders, respiratory diseases, and diabetes in the most versus least deprived areas have been observed (Plana-Ripoll et al., 2019; Rosella et al., 2018; Vanasse et al., 2012). In a recent follow-up of healthy civil servants in the Whitehall II cohort study, Dugravot et al. (2020) elaborated on the temporal pathways between social inequalities, multimorbidity, frailty, disability, and mortality. The study showed that socioeconomic status was the cause of these health outcomes, which in turn led to increased mortality. Multimorbidity conferred the most important risk of mortality, followed by frailty and disability. The authors concluded on the need for primary prevention and to better define multimorbidity in its nature and number of conditions (Dugravot et al., 2020).
If the impact of multimorbidity on excess mortality is known, few studies have examined the factors associated with mortality according to physical and mental multimorbidity and area-level socioeconomic status. To our knowledge, rare are the studies that have considered simultaneously important factors such as health behaviors (smoking and physical activity) (Whitley et al., 2014), psychosocial factors (satisfaction with life and social support) (Hülür et al., 2017; Holt-Lunstad et al., 2010), and health services use (Gaulin et al., 2019) in predicting mortality. Furthermore, most studies involved adults from the general population (Willadsen et al., 2018), selected populations as US veterans (Chwastiak et al., 2010), or older adults with cognitive impairment (Schiltz et al., 2019).
The aim of the current study was to examine, in a sample of community-living older adults, (1) the associations between physical and mental multimorbidity, individual and health system factors and mortality, stratified by area-level deprivation, and (2) the associations between individual and health system factors and mortality, stratified by the presence of physical and mental multimorbidity. The current study is based on individuals covered under a public health plan for whom information collected during a health survey was subsequently linked to health administrative data, minimizing information bias and allowing the study of a number of important psychosocial and clinical factors.
Methods
Study Population and Data Source
Data came from the “Étude sur la Santé des Aînés” (ESA)-Services study consisting of a convenience sample of 1811 older adults aged ≥65 years. Participants were recruited in primary care practices from 2011 to 2013 in one of the largest health regions of the province of Quebec covering approximately 1,325,000 inhabitants and representing rural, semi-urban, and urban areas. A list of all general practitioners (GPs) working full-time in the region was available (n = 744), of which 55% agreed to participate in the study. The methodology of the ESA-Services study has been described elsewhere (Préville et al., 2014).
Patients aged ≥65 years visiting one of the participating GPs received a pamphlet with a description of the study objectives and an invitation to participate in a face-to-face interview. Interested patients were contacted within 30 days by the study coordinator to confirm their interest and book an appointment. Structured computer-assisted interviews of approximately 90 minutes were conducted at the participant`s home by trained interviewers (health professionals and graduate students) to collect sociodemographic, behavioral, and health information. Before the interview, participants gave their written consent, and their cognitive status was assessed using the Mini-Mental State Examination (MMSE; Folstein et al., 1975). Participants with a MMSE score <22 and who were not able to complete the interview were excluded from continuing with the interview (n= 46). Participants also gave their health insurance number and consent to access their outpatient and inpatient health administrative data from the Régie de l’Assurance Maladie du Québec (RAMQ) and the Maintenance et Exploitation des Données pour l'Etude de la Clientèle Hospitalière (MED-ECHO). This information was linked to the province’s vital statistics registry. Individual health administrative data were available for 3 years prior and 3 years following the interview. The ESA-Services study was approved by the ethics committee of the CIUSSS de l'Estrie—CHUS.
Measures
Mortality
The main outcome of interest was all-cause mortality within the 3 years following the interview. Data on mortality were ascertained from the vital statistics death registry which is part of the Quebec Integrated Chronic Disease Surveillance System where data are updated annually (Blais et al., 2014).
Physical and mental multimorbidity
The presence of a disorder was based on either the presence of a self-reported or physician diagnosis from health administrative data. In the current study, 15 physical disorders were self-reported in the ESA-Services questionnaire using the following question: “To your knowledge, and according to a physician, do you have arthropathy, cancer, cardiovascular disease, dermatologic conditions, diabetes, eye disease, gastrointestinal diseases, headaches, hyperlipidemia, hypertension, liver disease, respiratory tract disease, thyroid problem, musculoskeletal conditions, and genitourinary problem?” Although there is no standardized list of chronic disorders to assess multimorbidity, the 15 physical disorders represent the most frequent diagnoses of chronic conditions for older adults aged ≥65 years (Diederichs et al., 2011; Fortin et al., 2017). The self-reported presence of an anxiety disorder, major depression, and bipolar disorder was assessed with the structured mental diagnostic module of the ESA-Services questionnaire, which was based on the Diagnostic and Statistical Manual of Mental Disorders criteria, fifth edition (DSM-V; American Psychiatric Association and DSM-5 Task Force, 2013).
Physical and mental disorders diagnosed by physicians in the 3 years preceding the interview were extracted from the administrative registries using codes from the ninth and tenth revisions of the International Classification of Diseases (ICD). The exhaustive list of ICD codes used has been previously reported (Gontijo Guerra et al., 2019).
Individual factors
Functional status was measured using questions from the revised Système de Mesure de l'Autonomie Fonctionnelle (SMAF)-IADL subscale (Demers et al., 2010; Desrosiers et al., 1995). Participants rated their autonomy from 1 to 5, ranging from autonomous to dependent, on tasks related to housekeeping, preparing meals, shopping, doing the laundry, using the telephone, using means of transportation, taking medications, and handling finances. Individual scores ranged from 8 to 40, which were categorized into low versus high functional status based on the IADL lower quartile. Satisfaction with life was measured with the 5-item Satisfaction with Life Scale with scores ranging from 5 to 25 (Diener et al., 1985). Social support was based on three (yes/no) questions assessing the presence of a confidant, someone that can provide much-needed help, and someone close that gives affection, which are similar to questions found in Canadian Community Health Surveys (Statistics Canada, 2012). Social support was rated present for participants reporting social support in each of the three domains. Cognitive functioning was assessed with MMSE scores ranging from 22 to 30. Smoking status (current smoking vs nonsmoking and past smoking), physical activity (number of sessions a week carried out moderate to vigorous physical activity ≥20 minutes) (Marques et al., 2016), and the presence of possible abuse or witnessing physical violence during childhood were also measured in the questionnaire. The following sociodemographic characteristics were considered: age (65–69, 70–74, 75–79, 80–84, 85–89, or ≥90 years), education (≤7 or >7 years), and marital status (with partner or without partner).
Health system factors
Information on health services used in the 3 years prior to the interview was extracted from health administrative registries and included the number of hospitalizations, visits to an emergency department, and outpatient visits. Continuity of care (COC) was measured using a COC index, adapted from Bice and Boxerman (1977), based on the number of medical visits and the number of unreferred physicians visited by the patient in the 3 years following the interview. A COC score of 1 indicated perfect continuity of care, whereas a score of 0 indicated an absence of continuity of care. The COC index was categorized into quartiles for the purpose of the analyses. Patient satisfaction with the last medical visit was assessed in the ESA-Services questionnaire with questions on overall satisfaction and satisfaction with the explanations received from the physician (Pitrou et al., 2020). Responses were recorded using 5-point Likert scales ranging from 1 to 5 (not at all to totally satisfied) and categorized as totally satisfied versus not.
Material and social deprivation
Area-level deprivation scores were ascertained using the Pampalon index (Pampalon et al., 2009) composed of indicators of material deprivation (income, employment, and education) and social deprivation (single-resident homes, single persons, and single parent families). The Pampalon index is based on the smallest area unit used in Canadian censuses, with an average of 400–700 persons. Participants’ postal codes found in the administrative registries were used to link to geographic area units. The Pampalon index was categorized to identify the areas of residence as follows: least deprived areas (first quintile), moderately deprived areas (second and third quintiles), and most deprived areas (fourth and fifth quintiles).
Statistical Analyses
Descriptive statistics were conducted using counts and frequencies for categorical variables, and means and standard deviations (SD) for continuous variables. Chi-square and Student t-tests were used to test differences in proportions and means, respectively. Cox regression analyses were carried out to assess the individual and health system factors associated with mortality, and they were stratified by area-level deprivation. In these models, physical and mental multimorbidity (PMM) was categorized into six dummy variables: (i) 0-3 physical conditions without a mental disorder; (ii) 0-3 physical conditions with a mental disorder; (iii) 4-6 physical conditions without a mental disorder; (iv) 4-6 physical conditions with a mental disorder; (v) ≥7 physical conditions without a mental disorder; (vi) ≥7 physical conditions with a mental disorder. Additional sensitivity analyses were also carried out to assess the association between PMM and cancer mortality as either a primary, secondary, or tertiary cause of death. Cox regression analyses were also carried out to assess the individual and health system factors associated with mortality and this stratified by the presence of PMM. In these analyses, PMM was defined as a dichotomous variable reflecting the presence of ≥2 physical disorders with a mental disorder. Additional sensitivity analyses were also carried out by removing from this group individuals without any multimorbidity, that is, individuals with ≤1 physical or ≤1 mental disorder. Hazard ratios (HRs) were reported with their 95% confidence intervals (95% CIs). All hypotheses were tested at a 95% significance level. Statistical analyses were performed using SAS version V.9.3 (SAS Institute, 2011).
Results
Sample characteristics as a function of 3-year mortality, N = 1570.
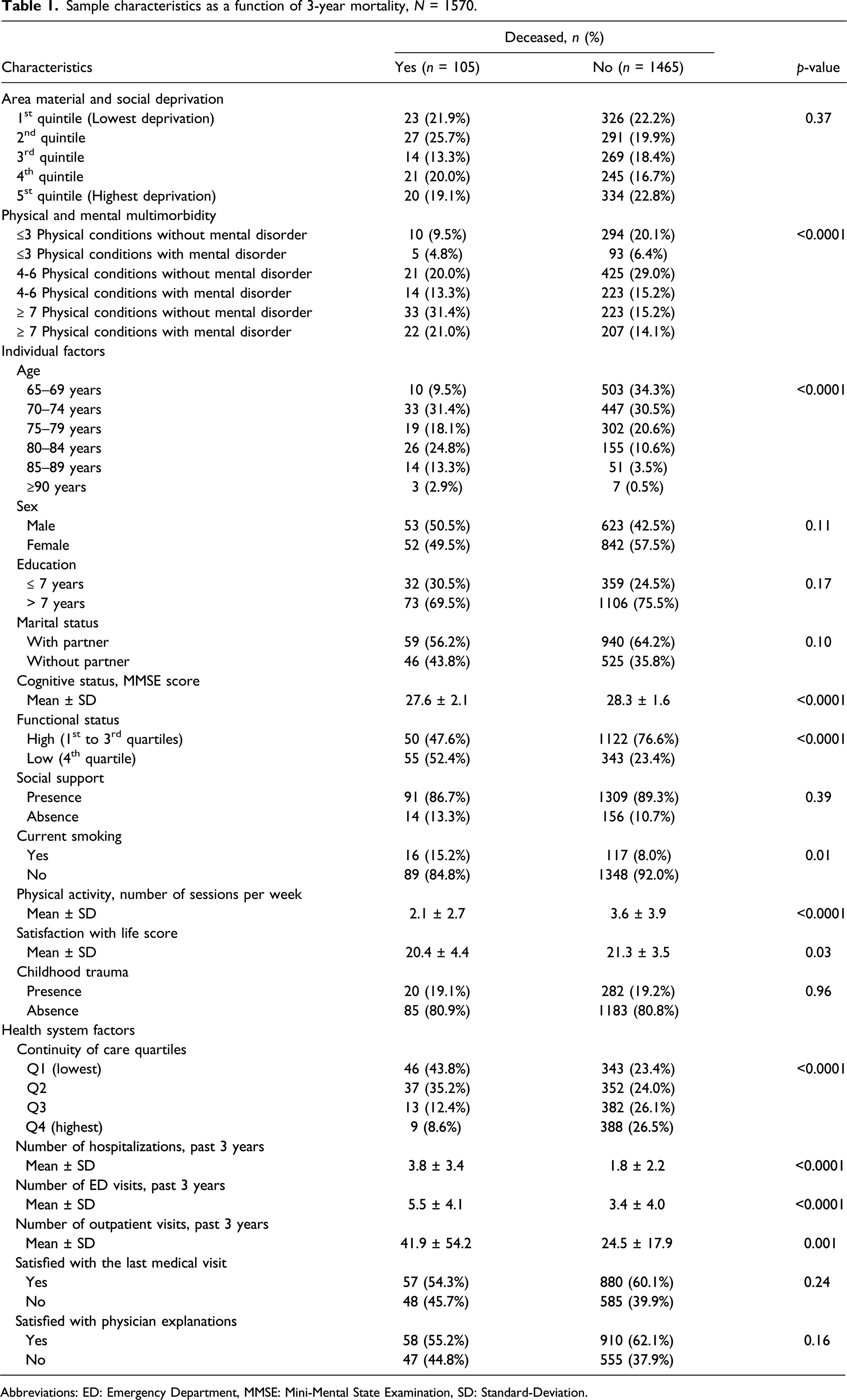
Abbreviations: ED: Emergency Department, MMSE: Mini-Mental State Examination, SD: Standard-Deviation.
The 3-year all-cause mortality rate was 6.7% (n = 105 deaths). The causes of death are summarized in the Supplementary Table (S1), with the most common being cancer followed by cardiovascular diseases. Descriptive analyses also showed that the number of physical conditions was associated with mortality (mean ± SD = 6.39 ± 2.49 compared to 5.21 ± 2 .45 for non-deceased participants, p < 0.0001). The proportion of each physical condition with respect to mortality and PMM is presented in the Supplementary Table (S2). A higher proportion of cancer, diabetes, cardiovascular, genitourinary, and musculoskeletal conditions was ascertained in deceased individuals without a mental disorder. A higher proportion of cancer, diabetes, cardiovascular, and liver diseases was ascertained in deceased individuals with a mental disorder.
Factors associated with 3-year mortality stratified by area material and social deprivation, N = 1570.
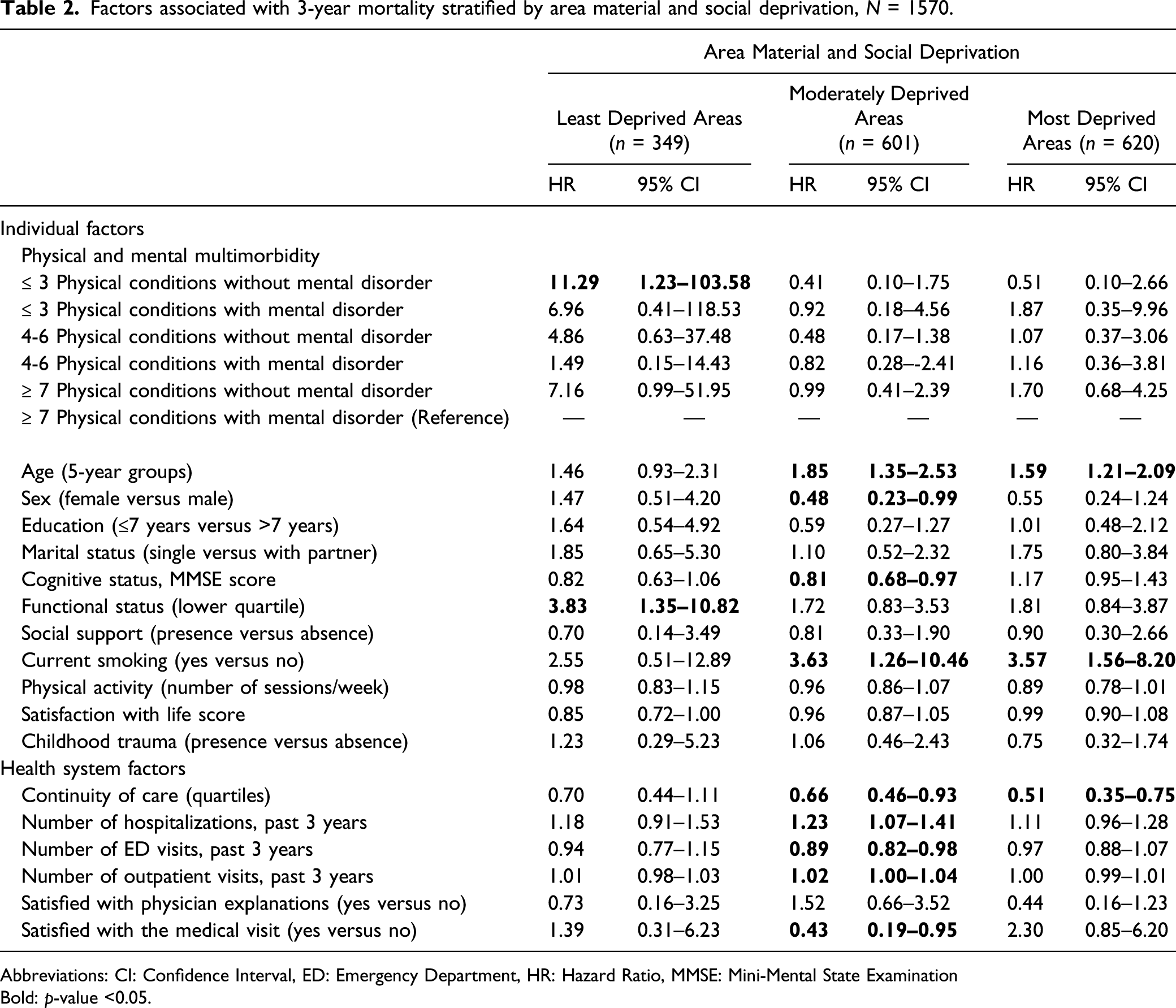
Abbreviations: CI: Confidence Interval, ED: Emergency Department, HR: Hazard Ratio, MMSE: Mini-Mental State Examination
Bold: p-value <0.05.
Three-year risk of cancer mortality stratified by area material and social deprivation, N = 1570.
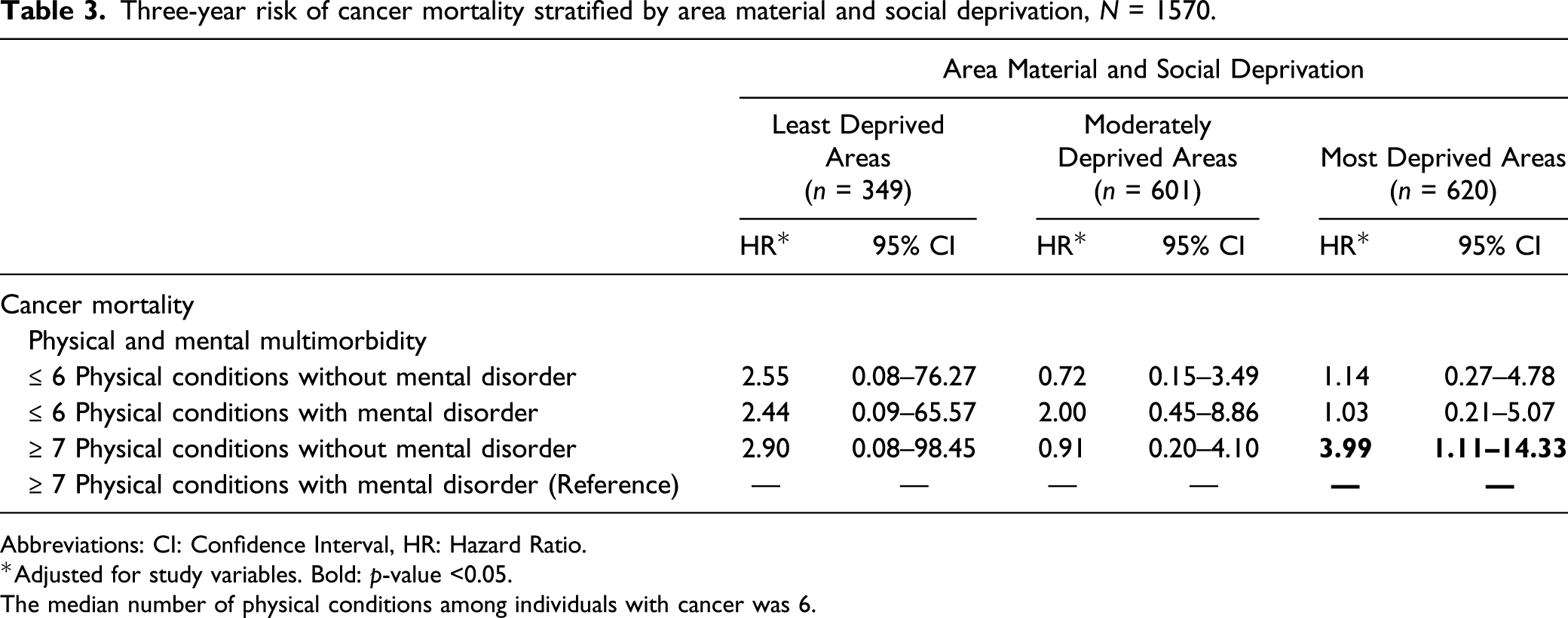
Abbreviations: CI: Confidence Interval, HR: Hazard Ratio.
*Adjusted for study variables. Bold: p-value <0.05.
The median number of physical conditions among individuals with cancer was 6.
Factors associated with 3-year mortality stratified by physical and mental multimorbidity, N = 1570.
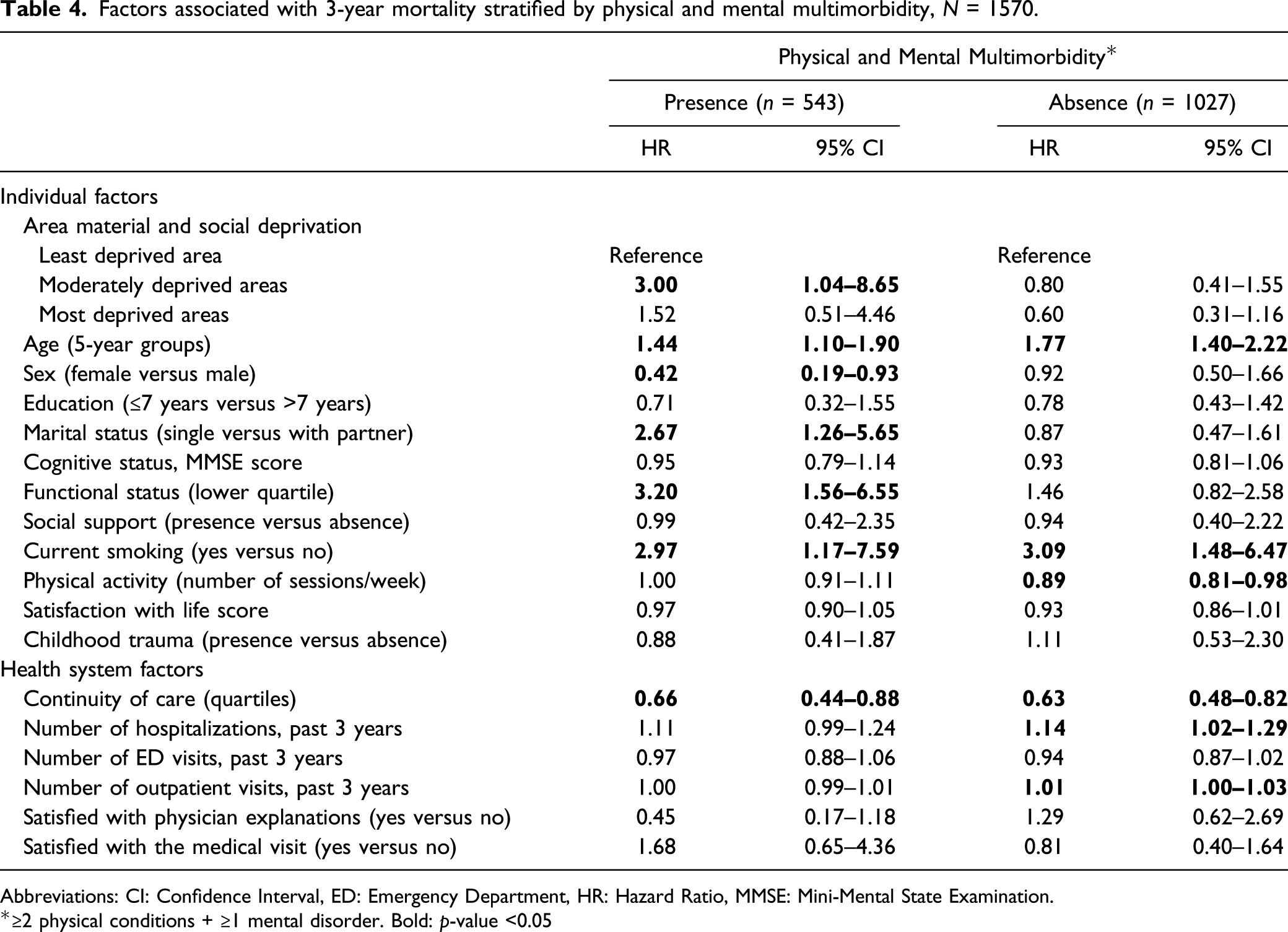
Abbreviations: CI: Confidence Interval, ED: Emergency Department, HR: Hazard Ratio, MMSE: Mini-Mental State Examination.
*≥2 physical conditions + ≥1 mental disorder. Bold: p-value <0.05
Discussion
This study reported on the factors associated with mortality in primary care older adults and contributes to the literature by looking specifically at the factors in those with and without PMM and living in least to most socially and materially deprived areas. The current findings are based on a 3-year follow-up study that includes health survey and administrative data allowing for the study of a range of socioeconomic, lifestyle, and clinical factors.
The findings of the current study should be interpreted while considering that the sample included community-living older adults living in a public healthcare system, where medical consultations, hospitalizations, and, for the majority, medications are covered (Lamoureux-Lamarche et al., 2016; Vasiliadis et al., 2013a; Vasiliadis et al., 2013b). Furthermore, although older adults were recruited in primary care practices, most older adults in the province of Quebec consult at least once in a given year, and more than 80% of them have a family doctor (Dubé-Linteau et al., 2013). Although higher overall mortality rates have been observed in most versus least socioeconomically deprived areas (Borell et al., 2014; Marí-Dell'Olmo et al., 2015), once lifestyle factors such as smoking, physical activity, and diet were controlled for, there was only a small increase in mortality risk in those living in areas with higher deprivation (Major et al., 2010).
Amongst the different levels of area deprivation, PMM status was not associated with all-cause mortality in individuals living in the most and moderately deprived areas. Amongst most favored areas, individuals with ≤3 physical conditions without a mental disorder had a higher risk of overall mortality as opposed to individuals with ≥7 physical conditions with a mental disorder. When looking at cancer mortality, individuals living in the most deprived areas with ≥7 physical conditions with a mental disorder had a decreased risk of mortality than those without a mental disorder. When examining mortality stratified by PMM, there was an increased risk of mortality in individuals with ≥2 physical conditions and ≥1 mental disorder living in moderately deprived areas compared to those living in least deprived areas. Such socioeconomic inequalities in mortality risks were not observed for individuals without PMM. Overall, the current findings do not show increased mortality associated with the highest physical and mental disease burden and this across area deprivation but do show socioeconomic inequalities in individuals living with a mental disorder.
These observations may reflect earlier policies to increase the number of residents attached to a primary care physician in the province of Quebec, with priority given to vulnerable populations (Breton et al., 2017; Breton et al., 2017). A population-registry study in Quebec showed that residents living in the most deprived areas were more likely to be attached to a primary care provider than individuals living in more favorable areas, with the lowest average rates of attachment observed in the middle area deprivation quintiles (Cacheiro-Millette, 2019), which may in part explain the increased mortality rate observed in the moderately as opposed to the least deprived areas in individuals with PMM. The registry study also showed that older adults aged ≥70 years not reporting significant health problems and residents, irrespective of age, with only physical conditions waited up to 25% longer to be attached, while those with physical and mental disorders had shorter wait times by 18% than healthy non vulnerable adults (Cacheiro-Millette, 2019). This may be reflected in the findings of lower cancer mortality in the most socioeconomically disadvantaged individuals with the highest physical and mental disease burden and suggests more timely access to care and better follow-up that may have included access to mental health professionals in specialty services leading to better outcomes for those individuals. Earlier population-based studies have shown socioeconomic inequities in accessing mental health services (Chartier-Otis et al., 2010; Vasiliadis et al., 2009).
When looking at health system factors, a higher continuity of care was inversely associated with mortality, and this was observed in the moderate and most deprived areas, as well as PMM groups. This finding is consistent with previous reports (Pereira Gray et al., 2018) including those in primary care settings and focusing on older adults (Leleu & Minvielle, 2013; Maarsingh et al., 2016). Continuity of care, however, did not predict mortality in individuals living in least deprived areas. These differences highlight the importance of follow-up care in populations living in socioeconomically deprived areas where there may exist an accumulation of vulnerabilities and lifestyle behaviors that can be mitigated with closer follow-up. In fact, continuity of care remained significant even after adjusting for outpatient and inpatient visits, and this was observed in individuals living in the most deprived areas. Decreased rates of readmission have been shown in older adults living in proximity to general medical services and where psychiatric services are more available (Vasiliadis et al., 2018). Future longitudinal research could focus on better documenting the impact of continuity of care on future hospitalizations for different socioeconomic groups while documenting available general and psychiatric resources within areas. This would help in informing resource allocation in different socioeconomic areas to better meet population needs. Moreover, perceived satisfaction with medical consultations was associated with lower mortality in moderately deprived areas, which is consistent with other reports (Kennedy et al., 2014). This finding further highlights the importance of quality and patient-centered primary care in that it may lead to improved adherence to recommendations and reduced mortality (Tevis et al., 2015).
With regard to lifestyle factors, current smoking was a predictive factor of mortality in individuals living in moderately and most disadvantaged areas, but not in those from more affluent areas. The differences observed may reflect better access to smoking cessation support programs in advantaged populations. Research has shown that smokers from disadvantaged socioeconomic positions were more likely to quit smoking cessation support and continue smoking, as opposed to those from more affluent positions who were more likely to remain in treatment and be abstinent (Hiscock et al., 2011). It was interesting to note that physical activity reduced mortality in individuals without PMM, while no association was observed when stratifying by area levels of material and social deprivation. This observation underlines the importance of healthy lifestyles in preventing multimorbidity in general, and in turn mortality (Dugravot et al., 2020).
It was also interesting to note the association between functional status and mortality amongst individuals living in the least deprived areas. Functional status was also associated with increased mortality in individuals with PMM. These results concord with previous research showing that disability predicts all-cause mortality in older adults (Wu et al., 2016), and that once socio-economic status has been considered, multimorbidity and disability are more proximal risk factors to mortality (Dugravot et al., 2020). Higher cognitive status was associated with reduced mortality in moderately deprived areas. This is consistent with previous reports showing that cognitive impairment was associated with a higher mortality risk in older adults (Lee et al., 2018; Yu et al., 2019). Others have reported higher detection of cognitive decline, better access to specialized services, and follow-up of these conditions in wealthier areas (Qian et al., 2014). The absence of an association in the least and most deprived areas needs further investigation, considering that cognitive aging may be different according to deprivation areas.
Strengths and Limitations
The current study has a number of strengths and limitations. First, the use of combined self-reported and administrative data to assess PMM reduced information bias. Previous research recommended combining different data sources to estimate the presence of chronic disorders in population studies, the concordance between self-reported and administrative data being highly variable (Gontijo Guerra et al., 2019). Second, health system factors were obtained from administrative data, therefore minimizing recall of health services used. Third, socioeconomic position was based on the Pampalon index, which is a standardized and robust indicator of area material and social deprivation frequently used for health monitoring and planning in population studies in Canada (Pampalon et al., 2009).
Among the limitations, we cannot exclude a selection bias. First, the study sample included primary care older adults aged 65 years and over, and therefore the conclusions are generalizable to individuals reaching this age and seeking health services. This survivorship bias limits the extrapolation of study associations to individuals who died before the age of 65 years and to those who live in other health system contexts. Second, compared to individuals that were excluded from the analytical sample due to missing information, those in the current study were more educated, had better functional and cognitive status, and more likely to report social support and be satisfied with medical visits. The potential selection bias associated with these differences and impact on results is difficult to predict. However, individuals in the current study were also more likely to report 2-3 physical conditions with a mental disorder, four physical conditions and more with and without a mental disorder, and on average 2.3 more physical conditions. No difference was observed on the other study factors such as lifestyle behaviors or use of health services. The selection bias appears to be minimized. Third, PMM was defined according to thresholds and not on specific comorbid conditions. Different disorder-specific multimorbidity may play an important role in the risk of mortality (Jani et al., 2019), which should be explored in future mortality studies. However, in the current study, the breakdown of the types of disorders associated with mortality risk was similar in those with ≥2 physical conditions with and without a mental disorder. Fourth, a number of self-reported study variables such as measures of functional status, lifestyle factors, and childhood trauma may have been subject to social desirability bias. This bias was minimized by using a standardized questionnaire and having interviews conducted in the most isolated area of the house, and a keypad was provided to answer questions related to adverse childhood experiences. We do not expect the bias to be differential between mortality groups. Finally, the generalizability of the results may be limited to older adults without cognitive impairment (those with cognitive difficulties were excluded from the sample) and to similar public health systems as in Quebec where access to health care is covered for residents.
Recommendations
The results of this study are relevant for primary care physicians and public health specialists. Despite a universal medical coverage with access to health care for all, health inequalities persist. First, we report socioeconomic differences in mortality rates for older adults with PMM. Future research needs to assess whether socio-economic and area level deprivation differences exist in follow-up care and access to specialized services. Second, smoking was an important risk factor of mortality, while continuity of care was associated with a reduced mortality in those living in deprived areas. These findings call attention for the prevention of PMM in general, with strategies aiming at tobacco smoking cessation and physical activity promotion. Primary care physicians should be encouraged and given the resources to maintain optimal continuity and follow-up care, especially in at-risk populations. Lastly, the approach of PMM as opposed to the single-disease framework should be strengthened in primary care.
Supplemental Material
sj-pdf-1-jah-10.1177_0898264321997715 – Supplemental Material for The Factors Associated with 3-Year Mortality Stratified by Physical and Mental Multimorbidity and Area of Residence Deprivation in Primary Care Community-Living Older Adults
Supplemental Material, sj-pdf-1-jah-10.1177_0898264321997715 for The Factors Associated with 3-Year Mortality Stratified by Physical and Mental Multimorbidity and Area of Residence Deprivation in Primary Care Community-Living Older Adults by Helen-Maria Vasiliadis, Samantha Gontijo Guerra, Djamal Berbiche and Isabelle E. Pitrou in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was financially supported by Quebec Health Research Fund (FRQ-S), 22251.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.