
Abstract
Background
Older adults likely exhibit considerable differences in healthcare need and usage. Identifying differences in healthcare utilisation both between and within individuals over time may support future service development.
Objectives
To characterise temporal changes in healthcare utilisation among a nationally representative sample of community-dwelling older adults.
Methods
A latent transition analysis of the first three waves of The Irish Longitudinal Study on Ageing (TILDA) (N = 6128) was conducted.
Results
Three latent classes of healthcare utilisation were identified, ‘primary care only’; ‘primary care and outpatient visits’ and ‘multiple utilisation’. The classes were invariant across all three waves. Transition probabilities indicated dynamic changes over time, particularly for the ‘primary care and outpatient visits’ and ‘multiple utilisation’ statuses.
Discussion
Older adults exhibit temporal changes in healthcare utilisation which may reflect changes in healthcare need and disease progression. Further research is required to identify the factors which influence movement between healthcare utilisation patterns.
Keywords
Introduction
Improvements in life expectancy at birth have not been met with a commensurate improvement in healthy life expectancy (Murray et al., 2015), placing further demand on health services globally. This demand is augmented by the increasing global prevalence of multimorbidity (Academy of Medical Sciences, 2018). Multimorbidity commonly refers to the presence of multiple chronic conditions, with a threshold value of two or more conditions often applied (Johnston et al., 2019). Consequently, multimorbidity translates into increased healthcare usage across many points within the healthcare system, including increased physician visits, the prescribing of multiple medications, increased risk of hospitalisation and longer hospital admissions (Cassell et al., 2018; Glynn et al., 2011; Marengoni et al., 2011; Palladino et al., 2016). The greater the degree of multimorbidity, the greater the expenditure (Båhler et al., 2015).
Furthermore, the disproportionate rate of population growth among older adults further compounds the challenges posed by multimorbidity. Global projections predict that by 2050, the number of persons aged 60 years and older will approach 2.1 billion and that a faster rate of population growth will be observed among those aged 80 years and older (UNDESA, 2015). It has been projected that by 2035, in England, the proportion of older adults aged ≥65 years that will be living with four or more chronic conditions will increase from 10% to 17% (Kingston et al., 2018). Approximately half of those aged ≥65 years are projected to report two or more chronic conditions, with a greater increase predicted to occur in the 85+ years category (Kingston et al., 2018).
The greater degree of multimorbidity among older adults translates into greater expenditure on healthcare services. In England, from 2006/07 to 2012/2013, a 16% increase in acute hospital admissions was observed, equating to two million additional admissions, with those aged ≥65 years accounting for the largest proportion of these additional admissions (Smith et al., 2014). In the Republic of Ireland (ROI), it has been estimated that the management of chronic conditions accounts for three quarters of health expenditure, accounting for 80% of general practitioner (GP) consultations and 60% of hospital bed days (Department of Health and Children, 2008). However, attempts to predict hospitalisation remain poor.
A systematic review of 30 studies found that many studies had better capability at predicting mortality than risk of hospital admission (Kansagara et al., 2011). Furthermore, whilst healthcare costs associated with inpatient admission are likely to be greater (Tanke et al., 2019), the identification of hospital admission risk does little to inform on healthcare usage at primary care level. Multimorbidity accounts for a large proportion of service usage in primary care (Cassell et al., 2018; Glynn et al., 2011; Salisbury et al., 2011) and may relate to the gatekeeping function of GPs with respect to access to secondary care. Thus, any assessment of multimorbidity-related service usage within a context where strong gatekeeping occurs within primary care, such as is the case in the ROI, requires an assessment of usage behaviour across the primary–secondary care interface.
Considerable variability in the risks of morbidity exists across individuals of the same age, attributed to differences in biological, social and environmental factors (UNDESA, 2015). Furthermore, individual variability in health risk behaviours such as tobacco consumption introduces further heterogeneity in morbidity patterns and thus health service utilisation. For older adults, this context is further complicated by an amalgamation of multiple factors over the life course. Consequently, health and social care provision planning should take account of the considerable heterogeneity among older persons with regard to morbidity and healthcare utilisation.
Furthermore, the analysis of healthcare usage as a single snapshot in time does little to inform of temporal variations in healthcare utilisation behaviour. An alternative approach is to examine the trajectories of healthcare usage that older adults follow over time. Such an approach also provides an opportunity to examine the relative stability of these trajectories and to investigate the ‘dynamic and recursive nature’ of health services use (Andersen, 1995, p. 7). Longitudinal cohort studies provide a mechanism for analysis, with many longitudinal studies of ageing underway globally. However, previous studies of healthcare utilisation among older Irish adults have focused on examining different types of healthcare utilisation, for example, GP visits, outpatient visits etc. as independent outcomes (Hudson & Nolan, 2015; Mohan et al., 2019; Murphy et al., 2015; Roe et al., 2017). Those living with multimorbidity are likely to require multiple visits, to more than one service type, in order to ensure optimal clinical management. Furthermore, many such studies largely consider healthcare usage at a cross-sectional level and do not examine dynamic changes over time.
In order to develop a deeper understanding of variation in healthcare utilisation by older adults, a cohort likely to be living with multimorbidity, an assessment of both inter- and intra-individual differences is required. Such an exercise necessitates the examination of multiple healthcare service types and multiple data collection periods. Latent variable modelling offers the opportunity to simplify this large amount of information into subpopulations that share commonality. Latent class analysis (LCA) can be conducted to identify subpopulations who differ from one another in their response patterns to selected indicators. Such methodology provides an opportunity to characterise the considerable heterogeneity that is likely to exist among older adults. Latent variable modelling can also be applied within a longitudinal context to provide a simplified assessment of change over time while retaining the nuances of each subpopulation.
Latent transition analysis (LTA) is a longitudinal extension of the latent class model, incorporating two modelling traditions: LCA and autoregressive modelling (Nylund, 2007). Latent class analysis identifies unique subpopulations or groups at each point in the analysis and the autoregressive component identifies the transitions that occur among the classes over time (Nylund, 2007). Thus, LTA estimates class membership at each time point whilst also estimating the probability of transition from each class to another over time. In effect, LTA estimates the probability of latent class membership at time t+1, conditional upon membership at time t. Latent transition analysis allows researchers to identify latent classes or statuses summarising inter-individual patterns in healthcare utilisation at specific points in time, whilst also identifying intra-individual changes in healthcare utilisation over time.
A greater understanding of inter- and intra-individual differences in longitudinal healthcare usage may support the future development of healthcare models. Integrated care for older persons has increasingly become an international goal. In 2017, the World Health Organization (WHO) published evidence-based guidance for healthcare providers on community-based approaches to detect and respond to declines in the functioning of older adults (WHO, 2017). Within these guidelines, an emphasis is placed on adopting a person-centred and integrated care approach. The ROI is currently embarking on ambitious reform of its healthcare system. In 2017, a 10-year plan, Sláintecare, was published with cross-parliamentary consensus (Houses of the Oireachtas, 2017). This new strategy outlines a move away from the current mixture of public and private healthcare provision towards universal healthcare and an integrated care strategy, focusing on a continuum of care throughout the lifespan (Houses of the Oireachtas, 2017). It seeks to move away from hospital delivered care to providing primary care within the individual’s own community (Houses of the Oireachtas, 2017).
As this strategy begins to be implemented, it may be beneficial to characterise existing inter- and intra-individual differences in healthcare utilisation across multiple healthcare services using data from a longitudinal cohort study of older adults. The Irish Longitudinal Study on Ageing (TILDA) is a nationally representative sample of community-dwelling Irish adults aged 50 years and older and commenced data collection in 2009 (Kenny et al., 2010). The TILDA study collects data on the health, economic and social circumstances of respondents to support improvements in policy that pertain to older Irish adults. Irish Longitudinal Study on Ageing is modelled on the Health and Retirement Study (HRS) conducted in the United States to allow for comparability with the HRS and other international longitudinal studies of ageing based upon the HRS design. Comparable questions on healthcare utilisation have been included in several international longitudinal studies of ageing including the Mexican Health and Aging Study (Wong et al., 2017), the Survey of Health, Ageing and Retirement in Europe (Börsch-Supan et al., 2013), the Japanese Study of Aging and Retirement (Ichimura et al., 2009) and the China Health and Retirement Longitudinal Study (Zhao et al., 2014).
The purpose of this article is to identify whether latent subpopulations, characterised by different patterns of healthcare utilisation, are present within a nationally representative sample of community-dwelling older adults. The study further seeks to identify if these subpopulations are equivalent across three consecutive measurement occasions, encompassing 6 years, and to determine the probabilities of transitioning from one latent class to another over time. By doing so, this article characterises healthcare utilisation by older community-dwelling Irish adults between 2009 and 2015, prior to a transformative period of healthcare reform in Ireland (2017 onwards), thereby serving as a benchmark for future evaluations in addition to facilitating international comparisons in healthcare utilisation by older adults.
Method
Sampling and Participants
Sample characteristics for participants at each wave.
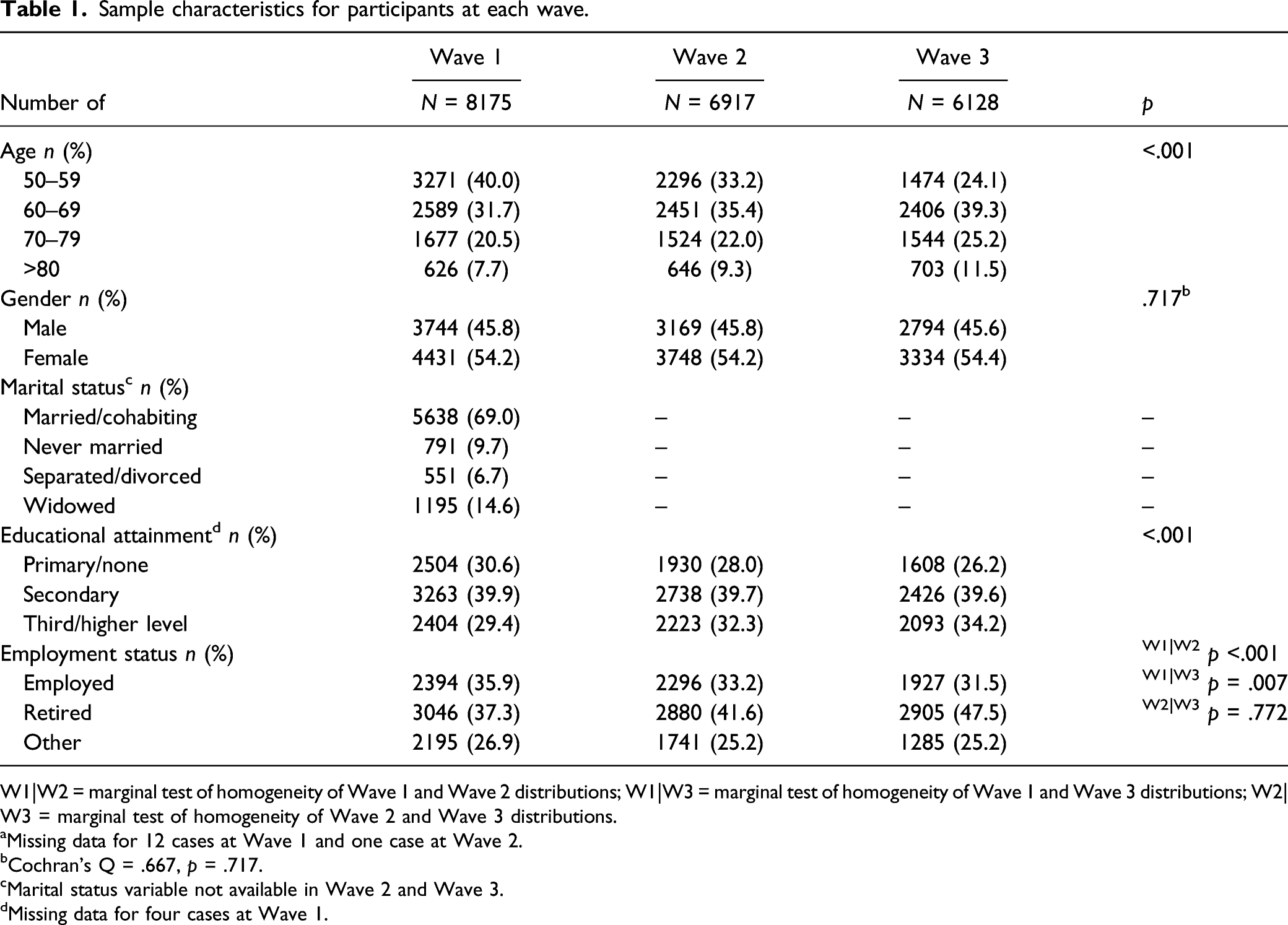
W1|W2 = marginal test of homogeneity of Wave 1 and Wave 2 distributions; W1|W3 = marginal test of homogeneity of Wave 1 and Wave 3 distributions; W2|W3 = marginal test of homogeneity of Wave 2 and Wave 3 distributions.
aMissing data for 12 cases at Wave 1 and one case at Wave 2.
bCochran’s Q = .667, p = .717.
cMarital status variable not available in Wave 2 and Wave 3.
dMissing data for four cases at Wave 1.
Design and Variables
Data collection during the TILDA study involved a Computer Assisted Personal Interview (CAPI), conducted on a two-yearly basis. Following completion of the CAPI, respondents were provided with a self-completion questionnaire. At Wave 1 and Wave 3, participants were also invited to take part in a health assessment (Kenny et al., 2010). In the present study, LTA was conducted using data exclusively from the CAPI.
The derivation of latent classes was based upon four indicators available in each wave of the TILDA data. During the CAPI interview, respondents were asked the following questions: in the last 12 months, about how often did you visit your GP; in the last 12 months, how many times did you visit a hospital Emergency Department (ED) as a patient; in the last 12 months, about how many visits did you make to a hospital as an outpatient; in the last 12 months, on how many occasions were you admitted to hospital overnight? In the case of outpatient hospital visits, respondents were advised that outpatient visits included all types of consultations, tests, operations, procedures or treatments (Kenny et al., 2010). These questions remained the same in subsequent data collection waves. Respondents self-reported a total count value for each of these questions. Number of GP visits was reported in the following categories none, 1–4, 5–9, 10–14 and 15+ visits. For ED, outpatient and inpatient visits data were presented in the following categories: none, single visit and multiple visits (2+).
Ethical Approval
Ethical approval for each wave of TILDA data collection was granted by Faculty of Health Sciences Research Ethics Committee, Trinity College Dublin. Ethical approval for secondary data analysis of TILDA data was included in the original overall ethical approval of TILDA. Ethical approval for secondary data analysis conducted in the present study was also granted by Ulster University’s School of Psychology Filter Committee.
Analytical Plan
Analysis was completed using Mplus version 8.1 (Muthén & Muthén, 1998–2018). Analysis was guided as per the methodology outlined by Ryoo et al. (2018). Ryoo et al. (2018) propose that model building within LTA should follow a stepwise approach that is largely influenced by the researcher’s goals. Measurement invariance is a crucial step to the successful application of LTA, with the first step to assess the equivalence of the optimal number of classes at each time point. Where this has been satisfied the fit of two LTA models, one with freely estimated parameters and one with constrained parameters can be compared. The establishment of measurement invariance allows for greater confidence in the interpretation of transition parameters and thus the model as a whole (Collins & Lanza, 2009).
Preliminary analysis was conducted at a cross-sectional level, with LCA conducted on Waves 1 to 3 separately. Measurement models ranging 1–5 latent classes were specified for each of the three time points as a preliminary step to model building. Manifest indicators used at each wave included GP visits, ED visits, outpatient visits and inpatient admissions. These indicators were coded as follows: • GP: none = 0; 1–4 = 1; 5–9 = 2; 10–14 = 3; 15+ = 4 • ED: none = 0; single visit = 1; and multiple visits (2+) = 2 • Outpatient: none = 0; single visit = 1; and multiple visits (2+) = 2 • Inpatient: none = 0; single visit = 1; and multiple visits (2+) = 2
Latent class analysis was conducted using the Maximum Likelihood estimator. Selection of the optimum number of classes at each wave was based upon a review of the Akaike Information Criterion (AIC; Akaike, 1981), Bayesian Information Criterion (BIC; Schwarz, 1978), sample size-adjusted BIC (ssBIC; Sclove, 1987) and entropy. Lower AIC and BIC values indicate better model fit. Entropy assesses the accuracy of classification into the most likely class and can range from 0 to 1; higher scores represent greater classification accuracy. The Vuong-Lo-Mendell-Rubin likelihood ratio test and the Lo-Mendell-Rubin (LMR)–adjusted likelihood ratio test were used to compare neighbouring class models (e.g. two versus. three class, etc.) to determine whether the inclusion of an additional class led to an improvement in model fit. A non-significant LMR p value favours the selection of the k-1 solution. Furthermore, the size of the smallest class and the substantive value of each class were reviewed to ensure interpretability of the classes in light of each additional class enumerated. Latent transition model examined using three waves of The Irish Longitudinal Study on Ageing data, where Outpx represents outpatient visits and Inpx represents inpatient admissions.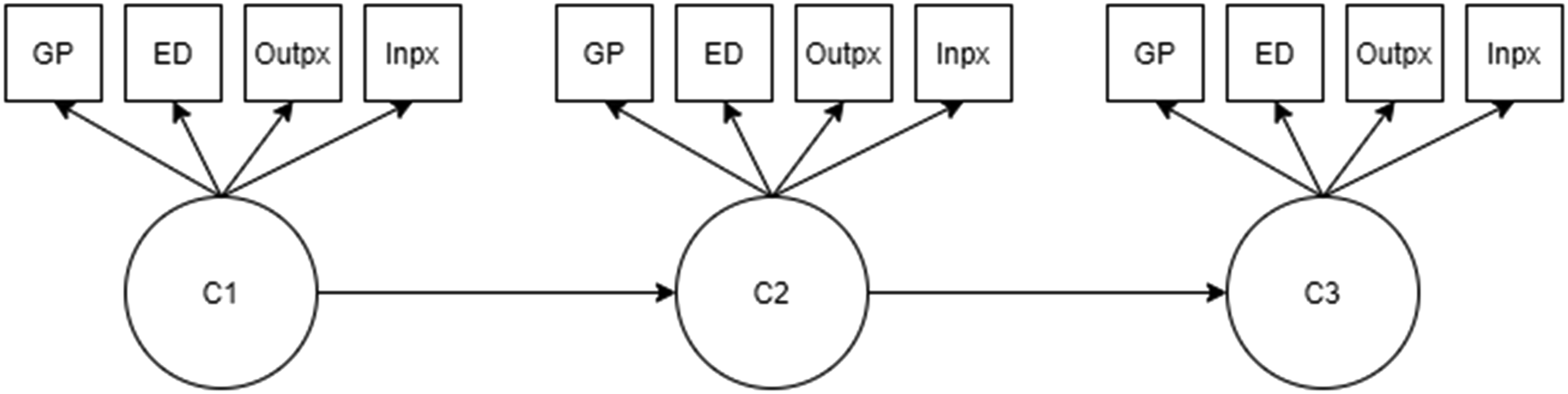
In the LTA model building (Figure 1), model fit was examined primarily by comparing differences in BIC values at each step, with lower BIC values considered to provide better fit (Asparouhov, 2020). Raftery (1995) provides guidance such that a BIC difference of >10 provides very strong evidence for a better fitting model. Measurement invariance over time was conducted by comparing a model with freely estimated item-response probabilities with one in which these were constrained to be equal over time. Measurement invariance assumes that any observed class differences in terms of latent class prevalence are purely quantitative in nature, with some classes larger than others and remaining so over time (Zammit et al., 2020).
Results
Descriptive statistics for healthcare utilisation across three waves of TILDA data collection.
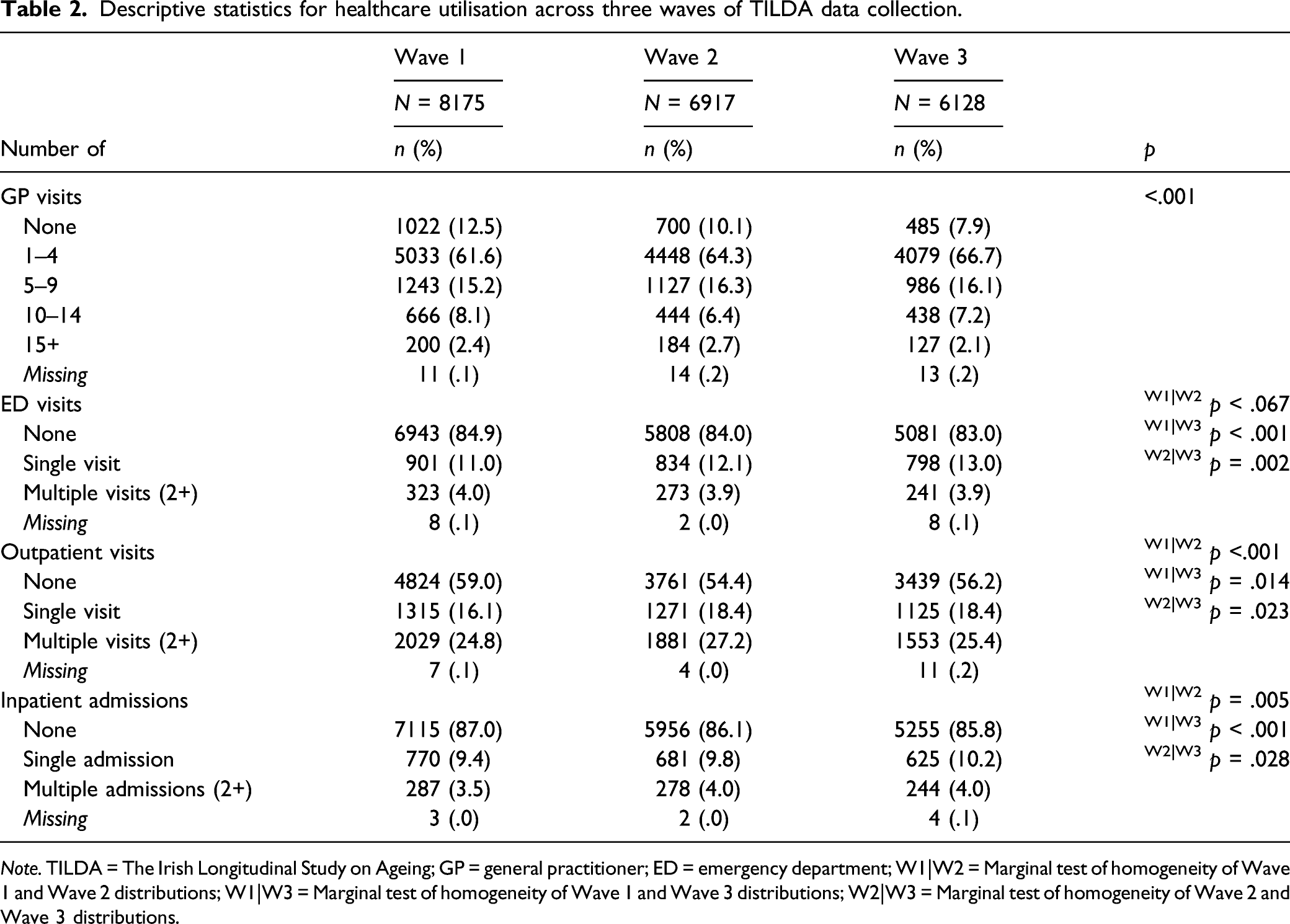
Note. TILDA = The Irish Longitudinal Study on Ageing; GP = general practitioner; ED = emergency department; W1|W2 = Marginal test of homogeneity of Wave 1 and Wave 2 distributions; W1|W3 = Marginal test of homogeneity of Wave 1 and Wave 3 distributions; W2|W3 = Marginal test of homogeneity of Wave 2 and Wave 3 distributions.
Results of LCA for healthcare utilisation indicators at each wave of TILDA data collection.
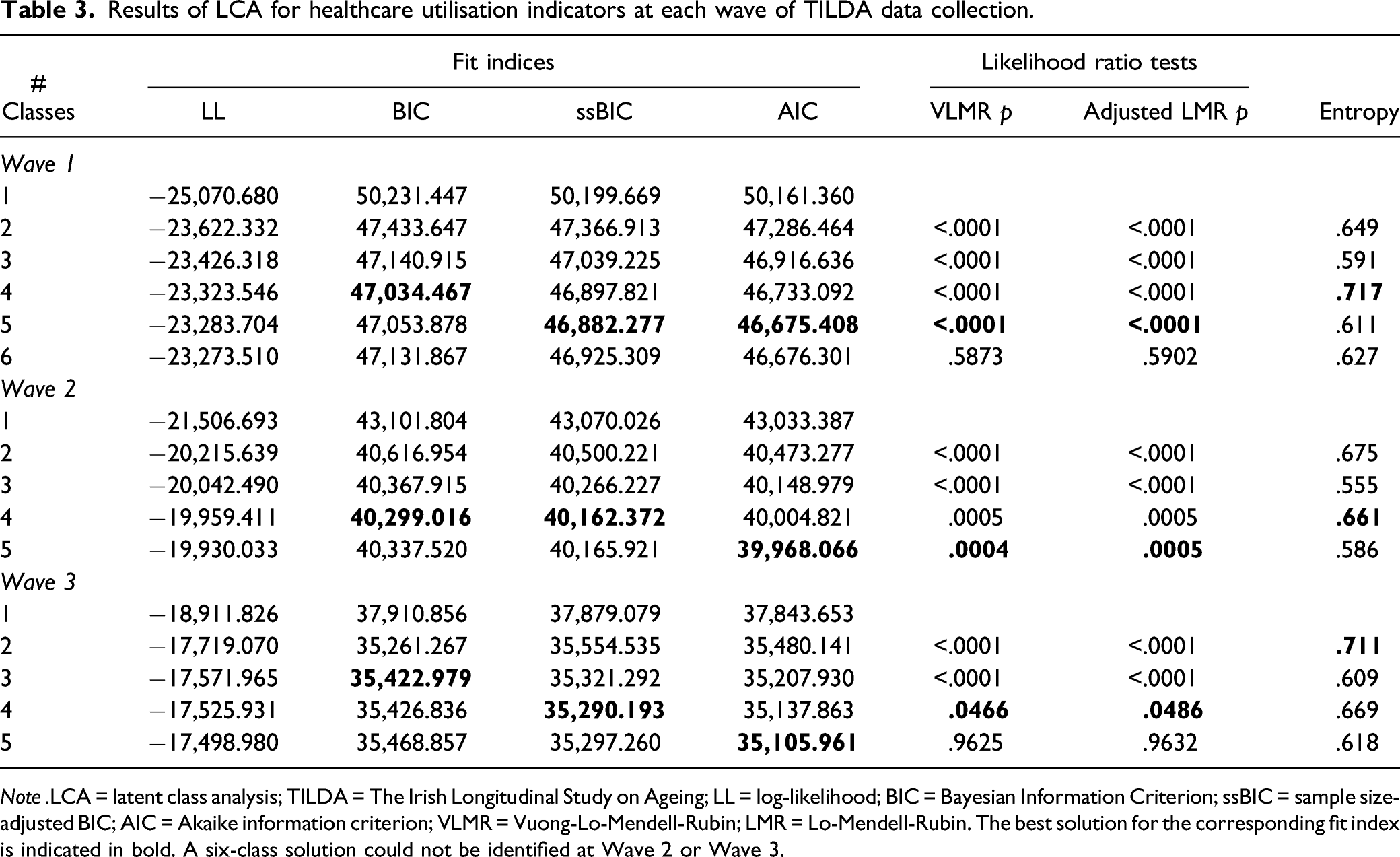
Note .LCA = latent class analysis; TILDA = The Irish Longitudinal Study on Ageing; LL = log-likelihood; BIC = Bayesian Information Criterion; ssBIC = sample size-adjusted BIC; AIC = Akaike information criterion; VLMR = Vuong-Lo-Mendell-Rubin; LMR = Lo-Mendell-Rubin. The best solution for the corresponding fit index is indicated in bold. A six-class solution could not be identified at Wave 2 or Wave 3.
At Wave 1 BIC and entropy indicated a four-class solution, whilst ssBIC and AIC suggested a five-class solution. The likelihood ratio tests favoured the selection of a four-class solution. An examination of the probability plots
For Wave 2 BIC, ssBIC and entropy favoured a four-class solution. The AIC suggested a five-class model as the optimal solution. The likelihood ratio tests could not be conducted as a six-class solution was not identified within the data irrespective of an increase to 2000 starts and 500 final stage optimisations. The inclusion of a fourth class resulted in the identification of two classes in the middle of the distribution that were not qualitatively different from one another
At Wave 3, the BIC favoured a 3-class solution, the ssBIC favoured a 4-class solution, AIC favoured a 5-class solution and entropy favoured a 2-class solution. The likelihood ratio tests favoured a 4-class solution. A 6-class solution could not be identified within the data. The inclusion of a fourth class did not add any meaningful contribution despite having a more favourable ssBIC
Results of longitudinal measurement invariance for three class LTA (N = 6128).

Note. LTA = latent transition analysis; BIC = Bayesian Information Criterion; ssBIC = sample size-adjusted BIC; AIC = Akaike information criterion.
Based upon the pattern of probabilities for each of the four indicators of healthcare utilisation, the three latent statuses were defined as ‘primary care and outpatient visits’ (LS1), ‘multiple utilisation’ (LS2) and ‘primary care only utilisation’ (LS3) (Supplementary Material Table A1). LS1 was defined as ‘primary care and outpatient visits’ as it was characterised by higher probability of GP and outpatient visits in combination with a low probability of endorsement for ED visits or inpatient admissions. The multiple utilisation status (LS2) showed moderate probabilities of endorsement of the various categories of GP visits, with thus, a low probability of endorsing the ‘no GP visit’ category. Furthermore, probabilities of endorsement of ED visits, outpatient visits and inpatient admissions were much higher for LS2 than either of the other latent statuses. The primary care only utilisation (LS3) status consisted of a high probability (.771) of endorsing 1–4 GP visits within the last year and low probabilities of endorsement of secondary healthcare such as ED, outpatient or inpatient healthcare usage. (Figure 2) Probabilities for item parameters (ρ estimates) for healthcare utilisation across three waves of data collection (N = 6128).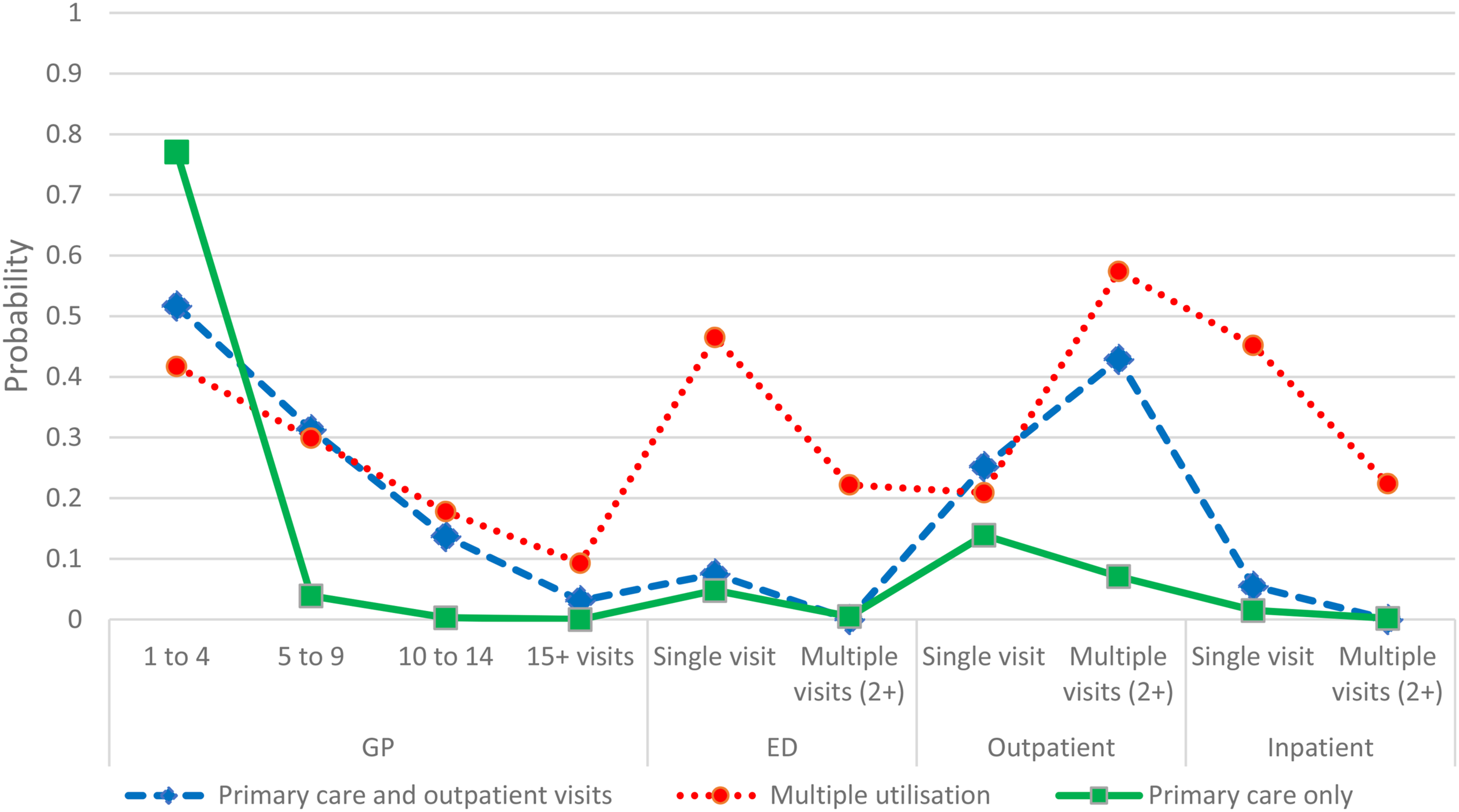
Latent status prevalence probabilities (δ) estimates and transition matrix (τ) estimates of healthcare utilisation over three time points (N = 6128).
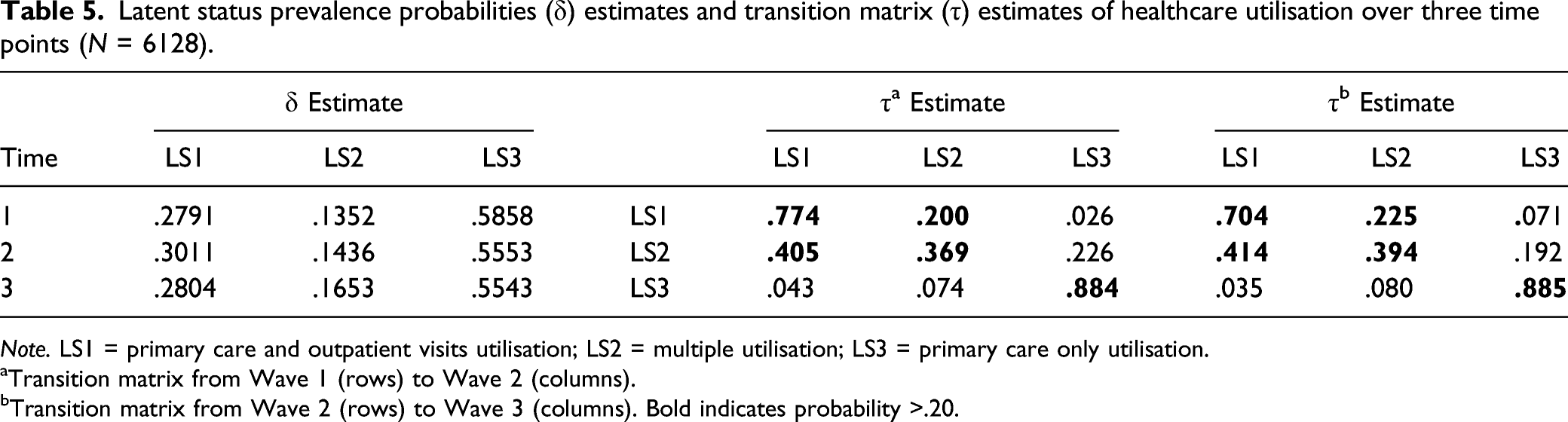
Note. LS1 = primary care and outpatient visits utilisation; LS2 = multiple utilisation; LS3 = primary care only utilisation.
aTransition matrix from Wave 1 (rows) to Wave 2 (columns).
bTransition matrix from Wave 2 (rows) to Wave 3 (columns). Bold indicates probability >.20.
The primary care and outpatient visits status (LS1) tended to stay within this status from Wave 1 to Wave 2 (.774) and also from Wave 2 to Wave 3 (.704). Similarly, the primary care only utilisation (LS3) status tended to stay within the LS3 group from Wave 1 to Wave 2 (.884) and from Wave 2 to Wave 3 (.885). The multiple utilisation (LS2) status were more likely to transition into primary care and outpatient visits (LS1) (.405) from Wave 1 to Wave 2 rather than stay within LS2 (.369). The multiple utilisation group was also less likely to transition into the primary care only utilisation group (.226) in comparison to staying within LS2 from Wave 1 to Wave 2. When the transition from Wave 2 to Wave 3 was examined, the multiple utilisation group were more likely to transition into the primary care and outpatient visits status (.414) than remain within LS2 (.394) or to transition into the primary care only utilisation group (.192). Those in the primary care only status (LS3) exhibited a high likelihood of remaining in this status between both Wave 1 and Wave 2 (.884) and between Wave 2 and Wave 3 (.885).
Results of transition probability invariance for three latent status solution (N = 6128).

Note. BIC = Bayesian Information Criterion; ssBIC = sample size-adjusted BIC; AIC = Akaike information criterion.
Discussion
The present study identified three latent subpopulations, characterised by divergent patterns of longitudinal healthcare utilisation, within a nationally representative sample of community-dwelling older Irish adults. Two of the latent classes comprised of healthcare utilisation across both primary and secondary care. The three latent classes were replicated across three waves of data, representing a six-year period, with measurement invariance established over the three waves of data collection.
The primary care only latent status may indicate a subpopulation who have a low level of healthcare need, and thus do not require outpatient, ED or hospital services. The identification of this latent status may also point to ‘compression of morbidity’ among successive generations (Fries, 2005). The compression of morbidity occurs if the age at first appearance of chronic disease increases more rapidly than life expectancy (Fries, 2005). An examination of chronic health and healthcare utilisation in the Great British General Household Survey found the rate of sickness fell across birth cohorts born between 1890 and 2008, particularly before birth year 1930 (Mason et al., 2015). At Wave 1 (2009), the TILDA cohort was comprised of birth cohorts from before 1929 (those 80+ years) to 1959 (those aged 50 years). Improvements in vaccinations, treatment of infectious disease and sanitation would have differential impacts upon successive birth cohorts examined in the present study.
Alternatively, accessibility of services, in terms of proximity or availability, may influence the choice of healthcare service accessed. A previous study within the TILDA cohort has shown that geographic accessibility to GP services does not influence variation in the utilisation of GP services but the number of GPs available does influence utilisation for those who can exercise choice in GP selection, that is, private patients who are not in receipt of public health coverage (Mohan et al., 2019).
The multiple utilisation (LS2) status, which exhibited a likelihood of endorsing all four healthcare indicators, was found to be the smallest group, comprised of 14–17% of the sample. The use of multiple healthcare services may be driven by several factors including multimorbidity and increasing levels of frailty (Han et al., 2019; Palladino et al., 2016). The identification of the primary care and outpatient visits status is not surprising, given that within the Irish healthcare system GPs largely act as the gatekeepers to other forms of healthcare usage, particularly in the form of referral to specialists (Glynn et al., 2011). This status could infer a somewhat healthier cohort who did not require emergency presentation to acute hospital services or may indicate effective disease management across the primary and secondary care interface. The primary care only status was the largest latent status, comprised of 55–58% of the sample at each wave, and the most stable of statuses over time, indicating a potential low level of healthcare need or a low level of healthcare engagement by a considerable proportion of community-dwelling older Irish adults. The results indicated that movement between statuses over time was more likely to occur for the LS1 (primary care and outpatient visits) and LS2 (multiple utilisation) than for LS3 (primary care only).
Those in the multiple utilisation status were more likely to transition into the primary care and outpatient visits status than remain in multiple utilisation and were less likely to transition into primary care only status between Waves 1 and 2. This could suggest some improvement in chronic disease management, resulting in a lower likelihood of presenting to acute hospital service, but not such an improvement that subsequent service utilisation would occur at primary care only. Alternatively, higher social care spending and greater availability of nursing and residential care have been shown to be associated with fewer hospital admissions, reduced length of hospital stay and reduced expenditure on secondary healthcare (Spiers et al., 2019). Changes in psychosocial circumstances may also explain transitions between the latent statuses over time. Previous research conducted using the TILDA cohort found that changes in public healthcare entitlements to be associated with changes in GP visits but not other healthcare service use (Nolan et al., 2016). The identification of a transition from LS2 to LS1 between Wave 1 and Wave 2, as well as between Wave 2 and Wave 3, indicates that this is not an isolated occurrence, but a replicable transition that occurs for some older adults. As it is a transition that comprises a reduction in multiple service utilisation, the identification of modifiable factors which influence this transition may serve as a target for future intervention to reduce utilisation of acute care services.
The probability of transitioning from primary care and outpatient visits to multiple utilisation was slightly higher from Wave 2 to Wave 3, suggesting a deterioration in healthcare status and could be indicative of those participants who were in multiple utilisation at Wave 1, had transitioned into primary care and outpatient visits at Wave 2 and who were then transitioning back to multiple utilisation by Wave 3. Healthcare utilisation has also been shown to increase in the final year of life (Ní Chróinín et al., 2018). Further analysis of the factors which influence transition into and out of the respective latent statuses over time has been conducted, but was considered beyond the scope of this article.
All of the latent statuses identified were characterised by moderate to high probabilities of GP visit endorsement, which may lend support to the view that GPs are central to healthcare for older people within Irish society (Barrett et al., 2011; Collins et al., 2018). Such a finding supports the contention that primary care must be adequately resourced in Irish society in order to meet the demands exerted by an ageing population with high levels of multimorbidity (Health Service Executive, 2015). However, it has also been argued that healthcare utilisation is a function of healthcare supply and that models of healthcare spending fail to recognise the complex relationship between healthcare supply and demand (Birch et al., 2015). Demand is partly determined by supply and so is not an independent measure of population needs (Birch et al., 2015). Nevertheless, examining where healthcare is currently being accessed is a valuable exercise, particularly in advance of transformative changes in healthcare provision and supply location. As the Sláintecare policy begins to embed, additional assessments of healthcare utilisation within the TILDA cohort can be compared with the findings outlined in the present study.
The identification of heterogeneity in healthcare utilisation within the TILDA cohort provides clarity to the contention that all older adults are frequent attenders to the different healthcare access points across the primary-secondary care interface. The multiple utilisation status, whilst present across all time points, was the smallest of the three latent statuses identified, indicating that multiple types of healthcare usage by older people may not be as prevalent as the general concern regarding adequate healthcare provision for this cohort would suggest.
It has been argued that healthcare policy planning based solely on demographic projections for population ageing is a fallacy, as it may overestimate the level of healthcare required if one assumes the relationship between age and health does not vary over time (Mason et al., 2015). Age alone has been shown to exhibit a weak relationship with healthcare costs (Howdon & Rice, 2018), with the relationship between age and health also shown to vary across birth cohorts (Mason et al., 2015). Healthcare utilisation increases in the final year of life (Diernberger et al., 2021; Ní Chróinín et al., 2018). Time to death has been shown to have a significant relationship with healthcare expenditure and may serve as a proxy for morbidity (Howdon & Rice, 2018). Latent transition analysis of prospective cohort studies may serve to support healthcare policy planning by modelling temporal changes in healthcare utilisation as a fundamental step in identifying the relative influence of covariates on transitions between different statues over time.
The analysis presented herein must be considered in light of several methodological limitations. The number of categories of GP visits was different from the other healthcare utilisation indicators. It is possible the fewer category levels in the ED visits, outpatient visits and inpatient admission variables may absorb some of the heterogeneity in existence within the sample. The publicly available form of the TILDA data reports categorical information where necessary to ensure the anonymity of respondents is maintained. Thus, in the present study, the lack of a more granulated assessment of secondary care healthcare usage could not be overcome. Furthermore, we must also acknowledge that supply factors, such as availability of GPs have not been accounted for within the present analysis.
The present study utilises self-reported healthcare utilisation data which is subject to recall bias on the part of the participant. Furthermore, the disparity between the interview questions regarding healthcare utilisation (in the last 12 months) versus other study questions (since the last time of interview approximately 24 months) also increases the risk of reporting error. Wallace et al., (2018) compared healthcare utilisation rates of a sub-sample of TILDA participants with a comparable cohort where such information was available in an electronic medical record. In multivariate analyses adjusted for confounders such as age, gender, number of prescribed medications, education, social class and health insurance coverage, no difference was reported between both cohorts in terms of number of GP visits and outpatient visits. However, TILDA respondents reported more ED visits. Wallace et al. (2018) propose that the possibility of underreporting of ED visits in the GP’s electronic medical record must also be considered, given that patients may not report all ED visits to their GP and issues can arise with respect to the receipt of electronic notifications for ED visits from secondary care. Thus, whilst the limitations of self-reported healthcare utilisation data must be borne in mind, such reporting need not undermine the value of such information, which ordinarily may be more difficult to gather by other means. The use of TILDA data provides comprehensive individual level data which would not necessarily be available if healthcare utilisation was assessed using administrative data sources.
An examination of the covariates that define the classes was not conducted. The literature is conflicted on whether to include covariates when enumerating latent class models. Nylund-Gibson and Masyn (2016) have found that miss-specified covariate effects can lead to the over-extraction of classes and recommend that class enumeration is conducted before the inclusion of covariates. Additional analyses examining the influence of covariates on the transitions between classes has been conducted but is not reported here due to space constraints and will be submitted for publication as a separate manuscript.
Notwithstanding the aforementioned limitations, the study findings indicate considerable heterogeneity in healthcare utilisation by older community-dwelling Irish adults, prior to a period of proposed transformation within the Irish healthcare system. This serves to provide a baseline context against which future evaluation of healthcare utilisation by older adults under the Sláintecare system can be compared. The analysis presented here has identified that only one in six community-dwelling older Irish adults use multiple healthcare services at both primary and secondary care levels. A further 30% utilise GP and outpatient services. Notably, considerable movement between these two types of usage profiles was shown to occur over time.
Movement from primary care and outpatient visits to multiple utilisation may occur as a consequence of a deterioration in the clinical status of the individual against a backdrop of prolonged waiting times for outpatient specialist services. Despite some reduction in waiting lists following the austerity impacts of the 2008 financial crisis, by December 2015, a total of 375,440 Irish people were awaiting an outpatient appointment, with 5,262 waiting >18 months and 9887 waiting >15 months (Health Service Executive: HSE, 2015). Clinical deterioration may lead to an ED visit with or without an accompanying emergency hospital admission. Internationally, an overall trend towards a reduction in the number of available acute care beds has been observed (Appleby, 2013). In Ireland, inpatient hospital beds decreased by 25.5% from 1980 to 2015 during a period of considerable government supported privatisation of the healthcare system (Mercille, 2018). From 2008 to 2017, a 10% reduction in acute beds occurred (Government of Ireland, 2018). During the same period, inpatient and day cases were found to increase by 25.2%, whilst ED attendances rose by 14.6% (Government of Ireland, 2018).
Systems characterised by reductions in inpatient bed capacity must ensure that the healthcare system remains responsive to changes in the health status of older adults. Otherwise, they run the risk of perpetuating a cycle of admission, premature discharge and emergency admission, placing additional pressure on what is often a resource limited service. Hospital admissions themselves can lead to declines in functioning of older adults (Covinsky et al., 2003), stressing the need for a model of care that provides the appropriate level of healthcare in the right setting for the individual. It is increasingly being recognised that older adults may benefit more from integrated models of care provided within the communities in which they live, which is the aim of the Sláintecare model (Department of Health Northern Ireland, 2016; Ham et al., 2013; Houses of the Oireachtas, 2017).
Conclusion
To date, there has been a lack of studies that have examined longitudinal changes in multiple healthcare service type utilisation by older adults. Longitudinal heterogeneity in healthcare utilisation by community-dwelling older adults was observed in the present study, indicating that a more nuanced assessment of temporal trends in healthcare utilisation by older adults is required. As the Irish healthcare system embarks on a period of considerable transformation, understanding the pre-transformation levels of healthcare utilisation by community-dwelling older adults provides a baseline assessment for future evaluations in the post-transformation period.
Supplemental Material
sj-pdf-1-jah-10.1177_08982643211041818 – Supplemental Material for Heterogeneity in Longitudinal Healthcare Utilisation by Older Adults: A Latent Transition Analysis of the Irish Longitudinal Study on Ageing
Supplemental Material, sj-pdf-1-jah-10.1177_08982643211041818 for Heterogeneity in Longitudinal Healthcare Utilisation by Older Adults: A Latent Transition Analysis of the Irish Longitudinal Study on Ageing by Ann S Doherty, Ruth Miller, John Mallett and Gary Adamson in Journal of Aging and Health
Footnotes
Acknowledgments
We thank The Irish Longitudinal Study on Ageing (TILDA) and also the Irish Social Science Data Archive (ISSDA) for providing the data to conduct this research study, accessed via the ISSDA-www.ucd.ie/issda.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementray material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.