
Abstract
Introduction
Poor childhood conditions can be seen as “the launch pad for a lifetime of health problems” (Raphael, 2011, p. 24). Research consistently shows that growing up under disadvantageous circumstances, such as in poor financial conditions or not living with both parents, is associated with poor later-life health (Gilman et al., 2003; Gruenewald et al., 2012; Kumari et al., 2013; Latham-Mintus & Aman, 2019; Pakpahan et al., 2017). Such experiences may have an immediate impact on the nervous, endocrine, and immune systems that remains apparent in adulthood and later life (Danese & McEwen, 2012). Life course epidemiologists have argued that adversity experienced in childhood may also be harmful for later-life health in an indirect way. Poor childhood circumstances may initiate a chain of risk, that is, they may increase the risk of subsequent experiences or events that are detrimental for health (Kuh et al., 2003).
Consistent with the idea of chains of risk, research shows that children who grew up in poor economic circumstances tend to have a lower socioeconomic position as adults (Barboza Solís et al., 2016; Jenkins & Siedler, 2007), which is, in turn, associated with poorer adult health (Barboza Solís et al., 2016; Präg & Richards, 2019; Robert & House, 1996; Whitley et al., 2018). The intergenerational transmission of divorce is also well documented (Dronkers & Härkönen, 2008). People who experienced the divorce of their parents in childhood are moreover relatively likely to become parents at a young age (Quinlivan et al., 2004; Woodward et al., 2004). Divorce and early transitions to parenthood are both, in turn, known antecedents of poor later-life health (Grundy & Read, 2015; Lorenz et al., 2006; Rote, 2017; Sironi et al., 2020).
The current study’s focus is on a potential chain of risk via health lifestyles. Cockerham (2005) has argued that the disposition toward particular health lifestyles is the result of the interplay between life chances and life choices. Both life chances–the lifestyle options that are available to particular people–and life choices–the choices that people make from the options available–are, in part, shaped by structural variables, such as class circumstances and the so-called collectivities, that is, “collections of actors linked together through particular social relationships, such as kinship” (Cockerham, 2005, p. 59). Fewer lifestyle options for healthy living are available when growing up in poor economic conditions, for instance because healthy diets tend to be less affordable than unhealthy alternatives (Drewnowski, 2013) and because lack of money or access to transport are a particularly strong barrier to sports participation for members of families with a lower socioeconomic position (Chinn et al., 1999).
Health behavioral choices within the set of options that are available are also shaped by structural factors via socialization patterns and experiences (Cockerham, 2005). Growing up in poor economic conditions or in a single parent family may be detrimental for the acquisition of cultural capital, that is, the symbolic and informational resources, such as knowledge, values, and norms, that are acquired through social learning (Abel, 2008). People who grew up under such circumstances may thus have relatively poor opportunities for the social learning of healthy lifestyle behavior. Plausibly due to limited life opportunities and exposure to material hardship, people with a low socioeconomic position are relatively likely to view their health as something beyond their control, to think less of the future, and to think less about how they can stay healthy, all of which is, in turn, associated with unhealthy lifestyle choices (Wardle & Steptoe, 2003). Certain forms of unhealthy behavior, such as smoking or drinking, may provide persons with a short-term reduction of the stress associated with having grown up under disadvantageous circumstances, albeit at the expense of a broad range of longer-term health outcomes (McEwen & Stellar, 1993). Growing up in a disrupted family or under poor economic circumstances is furthermore associated with greater impulsivity (Peterson & Zill, 1986), which, in turn, is associated with unhealthy eating, drinking, and smoking behavior (Hofmann et al., 2008).
Adverse health effects of various forms of health behavior may offset or compound each other (Shaw & Agahi, 2012). Therefore, many scholars have recently adopted a holistic perspective on health behavior and considered various aspects of health behavior, such as smoking, drinking, diet, and physical activity, conjointly, rather than in isolation, to provide insights into which behavioral combinations should be prioritized for interventions (Burgard et al., 2020; Griffin et al., 2014; Saint Onge & Krueger, 2017; Shaw & Agahi, 2012). Although research in which multiple aspects of health behavior are combined into an index has provided valuable insights on the antecedents and later-life consequences of health behavior in general (e.g., Barboza Solís et al., 2016; Zaninotto et al., 2020), it should be noted that various forms of health behavior are only weakly associated (Newsom et al., 2005). Many people’s behavioral patterns are discordant, that is, neither uniformly healthy nor uniformly unhealthy (Saint Onge & Krueger, 2017). This suggests that health behavior is a multidimensional concept that cannot fully be captured with an index.
Acknowledging the multidimensional nature of health behavior, the current study uses latent class analysis to distinguish distinct health behavior profiles that vary on the so-called smoking, nutrition, alcohol, and physical activity (SNAP) behavioral dimensions among people aged 50–80 years in Great Britain. It also assesses how disadvantageous early-life circumstances, such as growing up under poor economic conditions or not with both parents, are associated with having particular health behavior profiles and the extent to which effects of disadvantageous early-life characteristics on later-life health is attributable to differences in health behavior profiles.
The outcome of interest is allostatic load, that is, the physiological wear and tear of the body due to repeated or chronic exposures to stressors (McEwen & Stellar, 1993). When people are confronted with stressful challenges, neural, neuroendocrine, and neuroendocrine–immune mechanisms are activated in response. Although beneficial in the short term, this response called allostasis–stability through change–comes with increased physiological wear and tear over time. This long-term damage is called allostatic load. McEwen (1998) has argued that health behavior should be regarded as part of the overall notion of allostasis. This is because suboptimal health behavior, for example, smoking or drinking, may help individuals to cope with stress and challenges in the short term, while being physiologically damaging in the long term (e.g., Barboza Solís et al., 2016; Gruenewald et al., 2012).
Data and Methods
Analytical Approach
Latent class analysis (LCA) (McCutcheon, 1987) will be used to identify distinct health behavior profiles that vary on multiple SNAP dimensions. Health behavior profiles are operationalized here as a latent categorical variable underlying response patterns on a range of survey questions covering different SNAP dimensions. Given that, LCA uses the expectation–maximization (EM) algorithm that may only produce a local rather than the global maximum of the log-likelihood function dependent on the initial parameter values chosen in the first iteration, all latent class models are estimated 250 times with different starting values. A model with two latent classes is first estimated and the number of classes is then increased until the addition of a latent class does not lead to a model fit improvement as indicated by the Bayesian information criterion (BIC) score (Schwarz, 1978). Given the current study’s considerable sample size (see next subsection), BIC is arguably the most appropriate criterion to detect the number of classes because it sufficiently penalizes model complexity to avoid overfitting (Dziak et al., 2020; Tein et al., 2013). The AIC score (Akaike, 1974) is a commonly used alternative criterion to determine the number of classes, but, although it may work well with small samples, it is marred by high overfitting rates in larger samples (Dziak et al., 2020).
After estimating the LCA model with the optimal number of classes, the posterior probabilities of class memberships for each class will be stored for every respondent. Multinomial logistic regression will subsequently be used to predict class membership, whereby uncertainty regarding class membership is taken into account through the use of weights inversely related to the class membership classification errors (Bolck et al., 2004).
Linear regression is used to predict allostatic load. In a first model, allostatic load is regressed on early-life characteristics and a range of contemporaneous controls. The health behavior profiles identified in the LCA are added in a second model. Weights inversely related to the membership classification errors are again used to take uncertainty regarding class membership into account (Bakk & Vermunt, 2016). Bootstrapping is used to estimate the indirect effect of early-life characteristics via health behavior profiles on allostatic load (Preacher & Hayes, 2008).
Sample
Data are from the UK Household Longitudinal Study (UKHLS) (University of Essex, Institute for Social and Economic Research, NatCen Social Research, & Kantar Public, 2018, 2019). The UKHLS is a prospective, nationally representative study. Nurse visits took place in Wave 2, collected between 2010 and 2012. During these visits, physical measures, blood samples, and other health-related information were collected.
Analyses were restricted to 4700 people who participated in both Wave 1 and Wave 2, were aged between 50 and 80 years when Wave 2 data were collected, and had a valid blood sample analytical weight. 51 respondents were dropped because they reported that they did not live with at least one biological parent while growing up. This made it impossible to derive information on childhood socioeconomic circumstances. This exclusion procedure resulted in a final analytical sample of 4649 respondents.
Participation in the UKHLS nurse health assessment was selective. Most notably, no nurse visits were carried out in Northern Ireland. Furthermore, people with particular sociodemographic characteristics (e.g., people who were not married, lower educated, or not born in the UK) were underrepresented. The UKHLS team therefore prepared weights specially for the biomarker data to enable estimation samples to be representative of the general population of Great Britain (Benzeval et al., 2014). These supplied biomarker weights were used in this study.
Measures
Given the analytical approach, three types of measures are distinguished: manifest items, explanatory variables, and the distal outcome. Manifest items are observed realizations of the underlying dimensions of the latent health behavior profiles. The distal outcome is a measure of later-life health predicted by one’s health behavior profile. Explanatory variables considered are background variables that are plausibly predictive of having a particular health behavior profile as well as of allostatic load.
Manifest Items
Six smoking, nutrition, alcohol, and physical activity items were considered. With regard to smoking, current smokers, former smokers, and people who never smoked were distinguished. Two nutrition items were included: one capturing the frequency of fruit consumption and other capturing the frequency of vegetable consumption. Respondents were asked how often they consumed fruit and how often they consumed vegetables in a usual week, with response categories being never, 1–3 days per week, 4–6 days per week, or every day. The two bottom categories were combined into a new category for all respondents who consumed fruit, respectively vegetables, 0–3 days per week because very few respondents reported never eating any fruit or vegetables.
Respondents were also asked how often in the last week they consumed at least one alcoholic drink, and how many types of alcoholic drinks (beer or cider; alcohol shots, wine, and alcopops) they had on the day in the last week on which they drank the most. Alcohol consumption was subsequently converted to alcohol units, with one unit being equal to 10 ml of pure alcohol. Following the guidelines for low-risk drinking agreed upon by the UK chief medical officers (Department of Health and Social Care, 2016), respondents were categorized as nondrinkers, people with low-risk drinking behavior (≤14 units per week), or people with risky drinking behavior (>14 units per week).
Two physical activity items were considered. The question how many days of the past 4 weeks respondents had walked for at least 10 minutes continuously was used to capture the frequency of low-intensity physical activities (cf. Hughes & Kumari, 2017). A distinction was made between respondents who did so on not more than seven of the last 28 days, respondents who did so between 8 and 21 of the last 28 days, and respondents who did so on 22 or more of the last 28 days. A range of moderate-intensity sports were also considered, whereby a distinction was made between respondents who had done sports two times or less in the last year, respondents who had done sports more than twice in the last year, but less than weekly, and respondents who had done sports at least weekly.
Distal Outcome
Allostatic load is a measure of the physiological wear and tear of the body due to repeated or chronic exposure to stressors. McEwen and Stellar (1993), who coined the concept, defined it as “the cost of chronic exposure to fluctuating or heightened neural or neuroendocrine response resulting from repeated or chronic environmental challenge that an individual reacts to as being particularly stressful” (p. 2093). Allostatic load is typically measured with an index of markers of various biological systems (for an overview of various operationalizations, see Johnson et al., 2017). Johnson et al. (2017) recently pointed out that there is no standard method of calculating an allostatic load index in the scholarly literature. What they deemed particularly problematic was the absence of hypothalamic–pituitary–adrenal (HPA) axis biomarkers in the operationalizations of allostatic load in approximately half of the studies they considered in their review. They argued that the absence of HPA-axis markers made the operationalization of allostatic load inconsistent with McEwen and Stellar’s conceptual definition in which the neuroendocrine response to stress was central. However, the UKHLS data used here did include an HPA-axis marker: dehydroepiandrosterone sulphate (DHEA-S). Dehydroepiandrosterone (DHEA) and its sulfate form DHEA-S are the most common steroid hormones in the body and their levels decline with age (Benzeval et al., 2014). In addition to DHEA-S, 12 other markers of cardiovascular (systolic blood pressure, diastolic blood pressure, and resting heart rate), metabolic (waist-to-height ratio, total cholesterol-to-HDL cholesterol ratio, HDL cholesterol, triglycerides, glycated hamoglobin (HbA1c), and insulin-like growth factor-1), kidney liver function (creatinine clearance rate), and immune response (C-reactive protein and fibrinogen) biological systems were included in the allostatic load measure.
Consistent with earlier work (Seeman et al., 2001), all 13 indicators were dichotomized based on quartiles in the weighted sex-specific distributions, whereby scores in the least favorable quartile were coded as one (See Supplementary Appendix A). The dichotomized items were summed into a scale ranging from 0 to 13, with higher scores indicating a poorer physiological condition. The scale’s internal consistency was acceptable (KR-20 = .59).
Explanatory Variables
Early-life characteristics taken into account included whether or not respondents lived with both biological parents when they were 16 years old and whether or not they were born in the United Kingdom. Parental socioeconomic position when growing up was also taken into account. Respondents were asked to list the occupations of their parents when they were aged 14 years, and these occupations were subsequently coded according to the National Statistics Socioeconomic Classification. A distinction was made between parents with disadvantaged (“semi-routine and routine”), intermediate (“intermediate,” “small employers and own account,” and “lower supervisory and technical”), and advantaged (“management and professional”) socioeconomic positions. When the respondent reported that the parent was not working when the respondent was 14 years old, the parent was also coded as having low socioeconomic position. Where the socioeconomic positions of the father and the mother differed, the parental socioeconomic position was coded according to the parent with the highest socioeconomic position.
Early-life health was also considered. Respondents were asked if they were ever diagnosed with any of a range of diseases and health conditions, including diabetes, coronary heart disease, and clinical depression. Respondents who answered affirmatively were subsequently asked at what age they were told that they had this health condition. Respondents who were diagnosed with any of the listed health conditions at the age of 18 years or younger were coded as having health problems when growing up. Diseases most commonly mentioned as being diagnosed with when growing up were asthma and chronic bronchitis.
Sample Characteristics, Means, and Percentages.
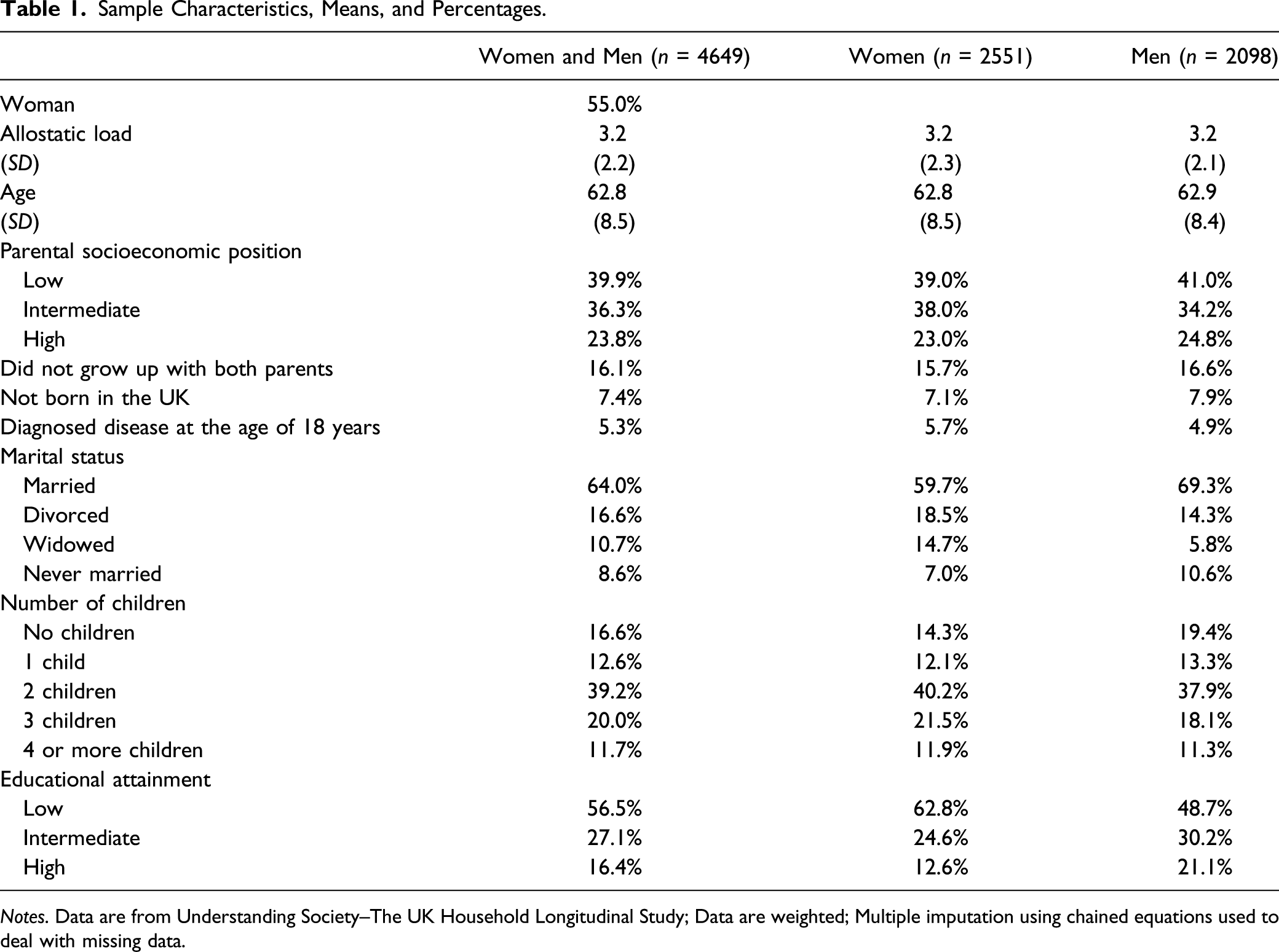
Notes. Data are from Understanding Society–The UK Household Longitudinal Study; Data are weighted; Multiple imputation using chained equations used to deal with missing data.
Missing Values
The sample included 1636 respondents (35.2%) with missing information on at least one variable of interest. Information on blood pressure (n = 711), drinking behavior (n = 551), HbA1c (n = 337), and C-reactive protein (n = 144) was missing most often. For all variables except the manifest items used to identify the latent categorical health behavior profiles, multiple imputation with chained equations were used to deal with missing information (Brand et al., 2019). The missing at random (MAR) assumption underlying this way of imputing missing information entails that any differences between the distributions of missing values and the distributions of observed values are to be explained by variables included in the imputation model. The findings from the substantive analyses on 20 imputed data sets were combined into a single set of results following Rubin’s rules (Little & Rubin, 1989), which take the variability in results between the imputed datasets into account. The iterative nature of the EM algorithm allows LCA-models to be estimated with missing observations on manifest health behavior items (Dempster et al., 1977), whereby MAR is also assumed.
Results
Four Health Behavior Profiles
A comparison of fit statistics indicated that a solution with four classes fitted optimally with our data (See Supplemental Appendix B). The BIC was lowest when a 4-class solution was chosen. The Akaike information criterion (AIC), which penalizes model complexity much more weakly, showed an “elbow” at the 4-class point, that is, there were only small further AIC declines with the addition of higher-order classes. Figure 1 provides an overview of the class conditional response probabilities on the considered manifest health behavior dimensions. The response probabilities displayed in green represent the class-conditional likelihood of being in the most favorable category in the particular behavioral dimension, respectively: never smoked, daily fruit consumption, daily vegetable consumption, nondrinker, walking for 10+ minutes continuously on 22 or more days out of the last 28 days, and at least weekly sports participation. In contrast, the response probabilities displayed in red respectively represent the class-conditional likelihood of being a current smoker, consuming fruit only 0–3 days a week, consuming vegetables only 0–3 days a week, drinking beyond sensible limits, walking for 10 minutes or more on not more than 7 days out of the last 28, and participating in sport fewer than three times a year. Class-conditional response probabilities.
The latent health behavior profile with the largest prevalence was characterized by a low probability of smoking and a high probability of frequent consumption of fruit and vegetables. Moreover, people with this profile were relatively likely to be physically active as indicated by a high probability of frequent walking and participation in sports. A final feature of this profile that stands out is the high probability of risky drinking behavior and the low probability of nondrinking. This profile was labeled broadly healthy, but high alcohol consumption.
The second profile also scored favorably on most health behavior dimensions. Fruit and vegetable consumption was high in this profile, and, albeit slightly higher than in the first profile, and levels of smoking were low. Moreover, people with this health behavior profile were highly likely to be nondrinkers. A negative characteristic of this profile was the high likelihood of nonparticipation in sports and of rarely walking for more than 10 minutes continuously. This profile was labeled low smoking and drinking, healthy nutrition, and physically inactive.
The third latent health behavior profile identified was characterized by relatively poor scores on most dimensions. People with this profile were relatively likely to smoke and their consumption of fruit and vegetables tended to be low. As with the second profile, they had a high likelihood of nonparticipation in sports and rarely walked for more than 10 minutes. However, they were considerably less likely to report risky drinking behavior and more likely to be nondrinkers than their counterparts in the first health behavior profile. The label broadly unhealthy, but low alcohol consumption was therefore assigned to this profile.
As with the broadly healthy, but high alcohol consumption profile, people assigned to the final, and least prevalent, profile were relatively likely to have risky drinking behavior. On each of the other dimensions, they scored much more poorly than people with broadly healthy, but high alcohol consumption profile, albeit not quite as poorly as the people with the broadly unhealthy, but low alcohol consumption profile. This profile was therefore labeled broadly moderately unhealthy and high alcohol consumption.
Early-Life Circumstances and Later-Life Health Behavior Profiles
Results of Multinomial Logistic Regression Analyses Predicting Class Membership and Average Marginal Effects.
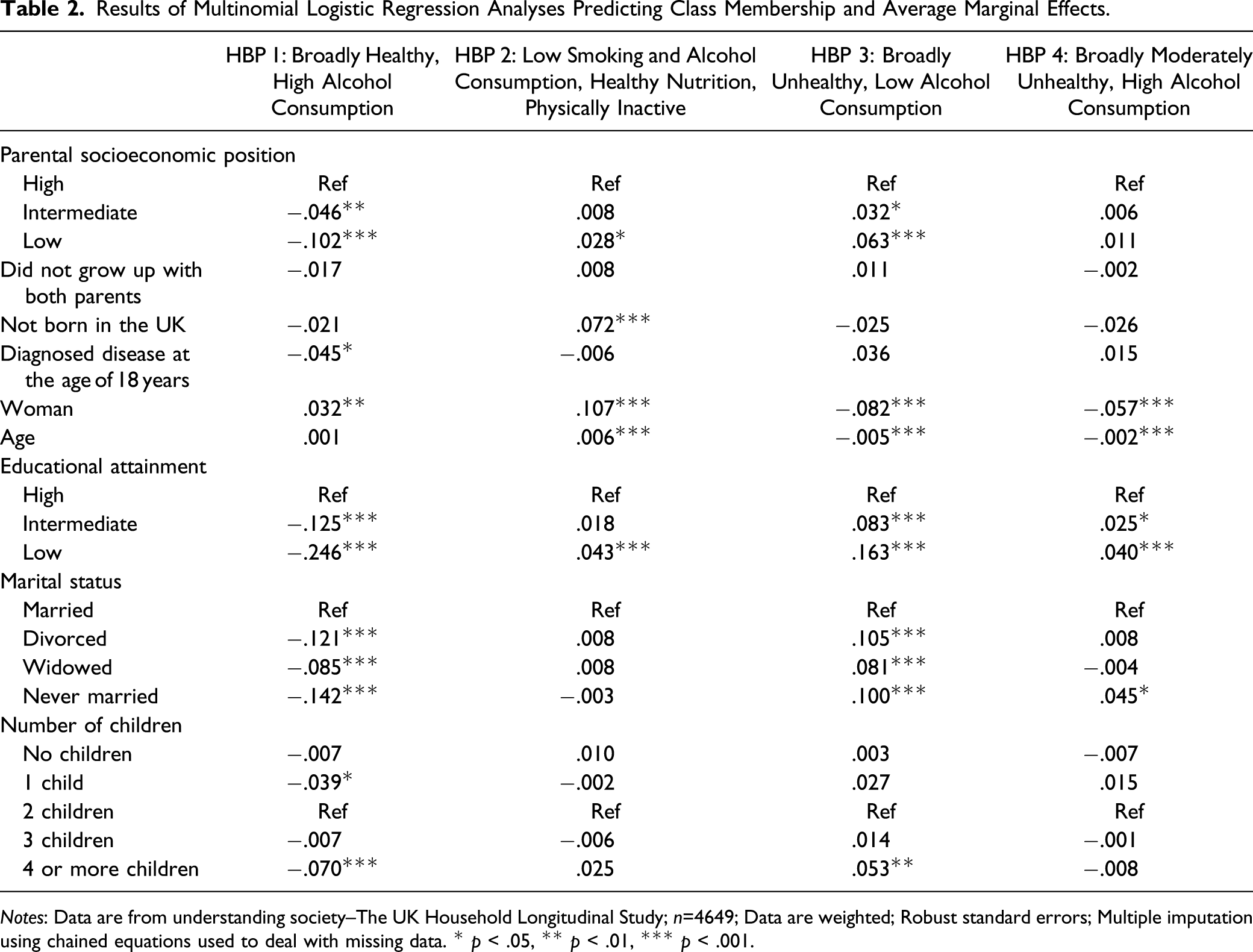
Notes: Data are from understanding society–The UK Household Longitudinal Study; n=4649; Data are weighted; Robust standard errors; Multiple imputation using chained equations used to deal with missing data. * p < .05, ** p < .01, *** p < .001.
The analyses showed that early-life circumstances predicted later-life health behavior profiles. Compared to people whose parents had high socioeconomic position, people whose parents had a lower socioeconomic position were more likely to have the broadly unhealthy and low alcohol consumption or the low smoking and alcohol consumption, healthy nutrition, and physically inactive health behavior profiles and less likely to have the broadly healthy, and high alcohol consumption health behavior profile. These effects were most pronounced for people whose parents had a low socioeconomic, rather than intermediate, position. Moreover, people born outside the UK were more likely than their UK-born counterparts to have a low smoking and alcohol consumption, healthy nutrition, and physically inactive health behavior profile, and being diagnosed with a disease at the age of 18 years or younger was associated with a lower likelihood of the broadly healthy and high alcohol consumption health behavior profile.
The model moreover showed that women were more likely than men to have the broadly healthy, but high alcohol consumption and low smoking and alcohol consumption, healthy nutrition, and physically inactive health behavior profiles and less likely to have the broadly unhealthy, but low alcohol consumption and broadly moderately unhealthy and high alcohol consumption health behavior profiles. Higher age was also associated with a lower likelihood of having the latter two health behavior profiles and a higher likelihood of having the low smoking and alcohol consumption, healthy nutrition, and physically inactive health behavior profile.
Compared to their highly educated counterparts, people with lower levels of educational attainment were more likely to have the broadly unhealthy and low alcohol consumption, the low smoking and alcohol consumption, healthy nutrition, and physically inactive, or the broadly moderately unhealthy and high alcohol consumption health behavior profiles and less likely to have the broadly healthy and high alcohol consumption health behavior profile. These effects were most pronounced for people with low, rather than intermediate, levels of education. Married people were more likely to have the broadly healthy and high alcohol consumption health behavior profile and less likely to have the broadly unhealthy and low alcohol consumption health behavior profile than divorced, widowed, and never married people. Few health behavior differences by number of children were found.
Allostatic Load
Results of Linear Regression Models of Allostatic Load.
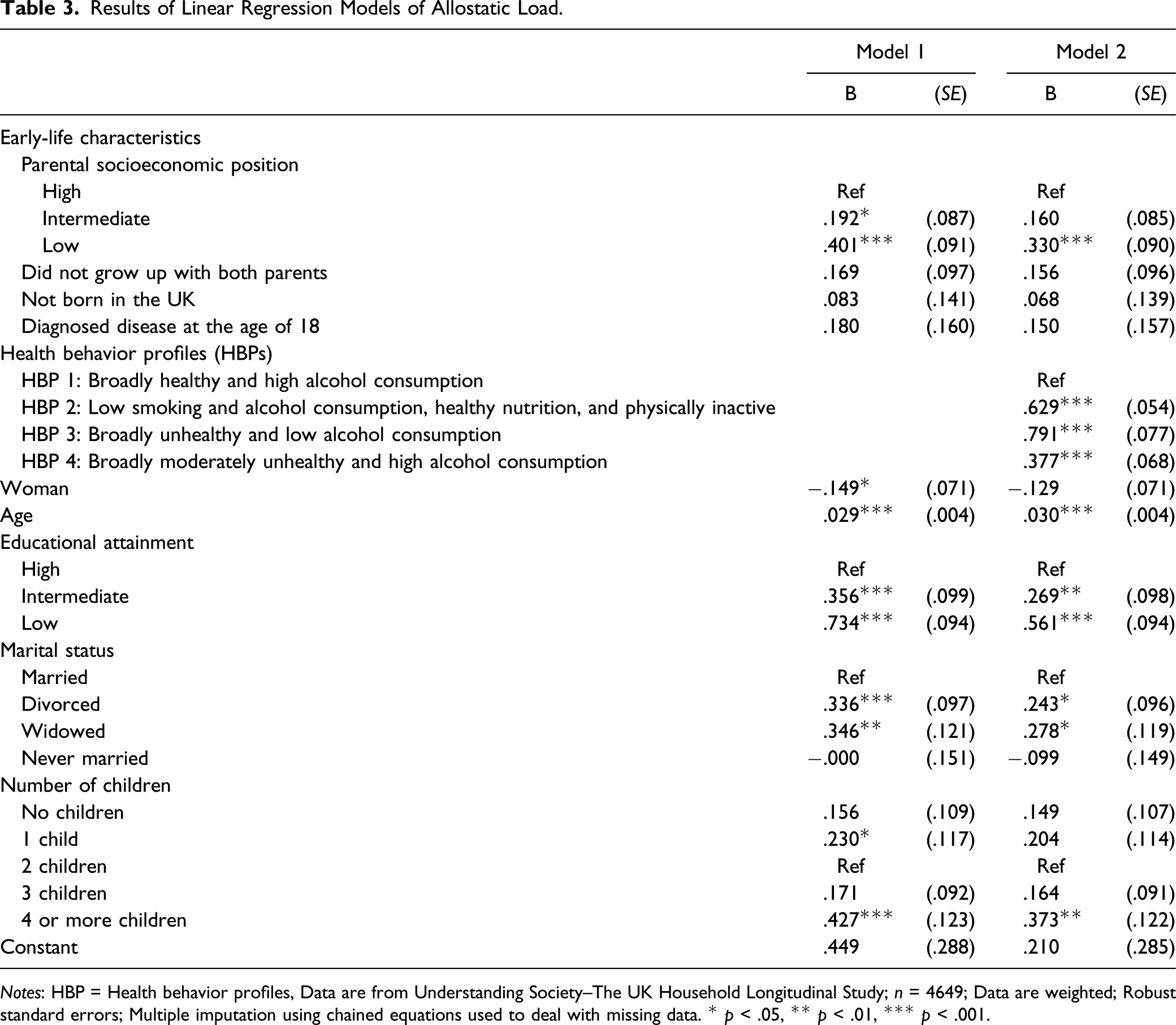
Notes: HBP = Health behavior profiles, Data are from Understanding Society–The UK Household Longitudinal Study; n = 4649; Data are weighted; Robust standard errors; Multiple imputation using chained equations used to deal with missing data. * p < .05, ** p < .01, *** p < .001.
In the second model, the health behavior profiles identified in the LCA were added. People with a broadly healthy and high alcohol consumption had significantly lower allostatic load than people in any of the other health behavior profiles. Allostatic load was Furthermore significantly higher for people with a low smoking and alcohol consumption, healthy nutrition ,and physically inactive (Δb = .251, p < .01) or broadly unhealthy and low alcohol consumption (Δb = .414, p < .001) health behavior profile than for people with a broadly moderately unhealthy and high alcohol consumption profile.
Decomposition of Coefficients of Parental Socio-Economic Position.
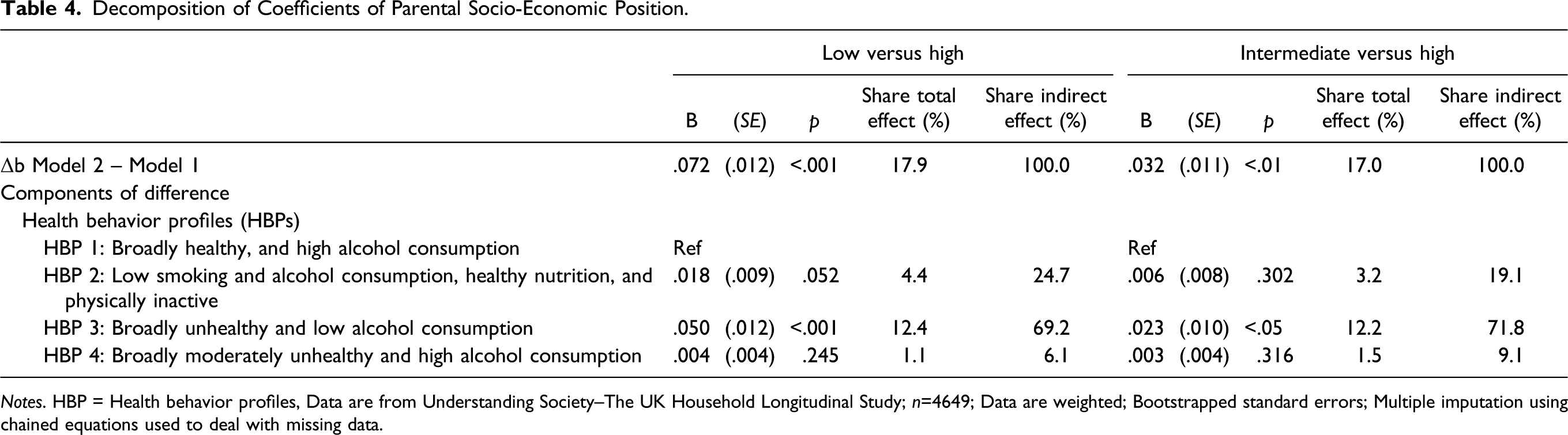
Notes. HBP = Health behavior profiles, Data are from Understanding Society–The UK Household Longitudinal Study; n=4649; Data are weighted; Bootstrapped standard errors; Multiple imputation using chained equations used to deal with missing data.
Discussion
It is well established that growing up under disadvantageous circumstances, such as in poor financial conditions, is associated with poor later-life health. The current study assessed a potential pathway from early-life circumstances to later-life health via health behavior. Latent class analysis (LCA) was used to distinguish particular health behavior profiles that vary on multiple behavioral dimensions–smoking, nutrition, alcohol consumption, and physical activity (SNAP) – among people aged 50–80 years in Great Britain. Multinomial logistic regression analyses then shed light on how disadvantageous early-life circumstances are associated with having particular health behavior profiles. Finally, the current study assessed to what extent the effects of disadvantageous early-life circumstances on allostatic load–an objective measure of the physiological wear and tear of the body–were mediated by the health behavior profiles identified in the latent class analysis.
Four distinct health behavior profiles were identified among the older British population: (1) broadly healthy and high alcohol consumption, (2) low smoking and alcohol consumption, healthy nutrition, and physically inactive, (3) broadly unhealthy and low alcohol consumption, and (4) broadly moderately unhealthy and high alcohol consumption. Marked differences in health behavior profiles were found by parental socioeconomic position, but few systematic differences were found by the other early-life characteristics considered: growing up in a single-parent family, not being born in the UK, and being diagnosed with a health condition at the age of 18 years or younger.
The analyses furthermore showed that people who grew up in a high socioeconomic position family had lower later-life allostatic load than their counterparts who grew up in families with a lower socioeconomic position, and that these differences could to a substantial extent be attributed to differences in health behavior profiles. The lion’s share of the indirect effects of parental socioeconomic position via health behavior profiles was due to people with low and intermediate socioeconomic position parents’ high likelihood to have the health behavior profile associated with the highest allostatic load in later life (broadly unhealthy and low alcohol consumption) and their low likelihood to have the health profile with the lowest allostatic load (broadly healthy and high alcohol consumption).
The current study extended earlier work by life course epidemiologists on later-life health by assessing a chain risk between early-life circumstances and later-life health via health behavior, in a way that acknowledged that health behavior is a multidimensional concept. Much earlier work explored chains of risks via socioeconomic circumstances in adulthood (e.g., Luo & Waite, 2005; Surachman et al., 2019), and the few studies that explored chains of risk via health behavior have tended to combine multiple aspects of health behavior into an index (Barboza Solís et al., 2016). Combining multiple aspects of health behavior into an index is, however, at odds with the increasingly dominant view that health behavior is a multidimensional concept. One of the reasons for this is that various forms of health behavior are only weakly associated (Newsom et al., 2005). In line with this argument, a reliability analysis indicated that the six health behavior items considered in the current study did not form an internally consistent scale together (α = .35). Moreover, the effects of various forms of health behavior may offset or compound each other (e.g., Shaw & Agahi, 2012). The results presented here are a case in point. The two most prevalent health behavior profiles (broadly healthy and high alcohol consumption and low smoking and alcohol consumption, healthy nutrition, and physically inactive) were both characterized by favorable scores on three of the four SNAP dimensions of health behavior. This implies that people with either of these two health behavior profiles would have roughly similar scores on an index in which multiple aspects of health behavior are simply summed. Nevertheless, the analyses indicated that early-life antecedents as well as the associations with allostatic load differed notably between these two behavior profiles. This underlines the importance of acknowledging the multidimensional nature of health behavior when investigating the mediating pathways of early-life characteristics on later-life health via health behavior.
The main limitation of the current study is that the analyses are cross sectional. Allostatic load was regressed on health behavior profiles, but it is not implausible that health status may also predispose people to a specific health behavior profile. In particular, having a low smoking and alcohol consumption, healthy nutrition, and physically inactive health behavior profile may be driven by health problems. Health problems may, for instance, be a barrier for physical activity (Xiang, 2016) and a reason for medical practitioners to urge the person with health problems to abstain from alcohol and smoking. However, earlier research showed that only few persons diagnosed with a new chronic condition adopt healthier behaviors (Newsom et al., 2012). Moreover, this study did not show an association between being diagnosed with a disease when growing up and having this particular health behavior profile. Nevertheless, analyses of birth cohort data with frequently repeated measures of health status and health behavior are needed to shed light on the ways in which health behavior profiles and health mutually shape each other.
A second notable limitation is that the information on early-life circumstances used in the current study was collected retrospectively, as were some important control variables. Retrospectively collected information may be of lower quality than prospectively collected information (cf. Sironi et al., 2020) because it may be prone to recall bias. In a recent study, in which prospective and prospective data on British people in their 50s were compared, no systematic differences in the distribution of important early-life characteristics (socioeconomic position of father when growing up and parental separation between birth and age of 16 years) were found, but the authors noted that retrospectively collected early-life characteristics were slightly, but statistically significantly, more strongly associated with later-life health than were prospectively collected early-life characteristics (Jivraj et al., 2020). This suggests that the magnitude of the impact of parental socioeconomic position on later-life allostatic load may be overestimated in the current study.
Recall bias may also explain the considerably higher levels of reported childlessness among men than among women in the sample analyzed here. Rendall et al. (1999) analyzed fertility histories in the British Household Panel Study and the Panel Study on Income Dynamics concluded that between one-third and half of the men’s nonmarital births and births within previous marriages were missed when information on fertility histories was collected retrospectively. Men’s higher levels of reported childlessness in the current study may, however, to some extent also capture the fact that, in couples, men tend to be older than women. Female partners of male respondents are thus typically born later than female respondents. This is important because the median of birth year of female respondents was 1948, and women born in the second half of 1940s form a cohort with a considerably lower prevalence of childlessness than subsequent cohorts of women (Berrington, 2017).
It should also be considered that whereas multinomial logistic regression was used to predict health behavior profiles, the indirect effects of parental socioeconomic position were calculated based on linear probability estimates of class membership (cf. Preacher & Hayes, 2008). However, these linear probability estimates (see Supplemental Appendix C) were very similar to average marginal effects from the multinomial logistic regression model of class membership presented in Table 2.
Older adults’ health behavior patterns tend to be highly stable over time (Burgard et al., 2020), and even after the development of health conditions, people find it difficult to adopt a healthier lifestyle (Newsom et al., 2012). This suggests that efforts to disrupt the chain of risk from early-life socioeconomic disadvantage to poorer later-life health via health behavior may be most promising if they focus on early phases in the life course. Recent reviews suggested that interventions targeting disadvantaged children may yield modest improvements in health behavior among this group (Craike et al., 2018; Wijtzes et al., 2017). However, the body of evidence on which interventions can be based is still very limited considering the need to battle the suboptimal health behavior choices that follow from growing up under disadvantageous circumstances. Wijtzes et al. (2017) therefore recently called for increasing scholarly attention for the long-term effectiveness of interventions aiming to improve health behavior among children growing up under disadvantageous circumstances. The current study’s finding of an important pathway from early-life socioeconomic disadvantage to poorer later-life health via a disposition for suboptimal health behavior underlines the urgency of this call.
Supplemental Material
sj-pdf-1-jah-10.1177_0898264320981233 – Supplemental Material for Early-Life Circumstances, Health Behavior Profiles, and Later-Life Health in Great Britain
Supplemental Material, sj-pdf-1-jah-10.1177_0898264320981233 for Early-Life Circumstances, Health Behavior Profiles, and Later-Life Health in Great Britain by Thijs van den Broek in Journal of Aging and Health
Footnotes
Acknowledgments
Understanding Society is an initiative funded by the Economic and Social Research Council and various government departments, with scientific leadership by the Institute for Social and Economic Research, University of Essex, and survey delivery by NatCen Social Research and Kantar Public. The research data are distributed by the UK Data Service. This work was conducted as part of the author’s Understanding Society Biomarker Fellowship. This fellowship was funded by ESRC ES/M008592/1. The author would like to thank Paul Clarke, Emily Grundy, Amanda Hughes, Meena Kumari, Mike Murphy, and Anna Nieboer for their valuable comments on earlier versions of this manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council, under grant no ES/M008592/1.
Ethics Statement
The University of Essex Ethics Committee has approved all data collection on Understanding Society main study and innovation panel waves, including asking consent for all data linkages except to health records. Requesting consent for health record linkage was approved at Wave one by the National Research Ethics Service (NRES) Oxfordshire REC A (08/H0604/124), at BHPS Wave 18 by the NRES Royal Free Hospital and Medical School (08/H0720/60), and at Wave four by NRES Southampton REC A (11/SC/0274). Approval for the collection of biosocial data by trained nurses in Waves two and three of the main survey was obtained from the National Research Ethics Service (Understanding Society - UK Household Longitudinal Study: A Biosocial Component, Oxfordshire A REC, Reference: 10/H0604/2).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.