
Abstract
Keywords
Introduction
Older adults are the fastest growing segment of society, experience the highest rate of chronic diseases and conditions, and require the highest long-term care costs of all age groups (World Health Organization, 2015). Healthy lifestyle is considered an important tool to prevent chronic conditions and institutionalization in older adults (World Health Organization, 2002).
There is substantial evidence from epidemiological studies among older adults that individual lifestyle factors, including physical activity, alcohol consumption, smoking behavior, and body weight, are associated with health and functioning (Bots, Tijhuis, Giampaoli, Kromhout, & Nissinen, 2008; Ebrahim, Wannamethee, Whincup, Walker, & Shaper, 2000; Knoops et al., 2004; Van Gool et al., 2003; Wannamethee, Ebrahim, Papacosta, & Shaper, 2005). However, these studies focused on one specific lifestyle factor and therefore lack the ability to make comparisons between lifestyle factors with regard to their association with functioning. This information could support targeted lifestyle advice to specific groups of older adults at risk of functional decline. Furthermore, these previous studies did not include repeated assessments of lifestyle over time following older persons well into old age during which age-related changes in lifestyle, health, and physical functioning occur.
Epidemiological studies have also examined the impact of an overall healthy lifestyle, using the sum of healthy individual lifestyle factors, on mortality risk. In older persons, adherence to more healthy lifestyle factors was associated with 65% to 75% lower mortality rates, even in the oldest-old (Rizzuto, Orsini, Qiu, Wang, & Fratiglioni, 2012; Van den Brandt, 2011). However, it is virtually unknown whether leading an overall healthy lifestyle, according to official recommendations for older persons, would slow down the rate of decline in functioning with aging in the different domains of functioning (Chakravarty et al., 2012; Lee, Kim, & Back, 2008). Moreover, no studies included multiple domains of functioning simultaneously to allow investigating which functioning domains benefit most from an overall healthy lifestyle in old age. In particular, few studies have investigated the role of lifestyle factors and an overall healthy lifestyle in social functioning. This knowledge will importantly contribute to the goal of adding healthy years to an increasing life span.
The aim of this prospective study was to investigate the association of an overall healthy lifestyle with 3-year change in physical, psychological, cognitive, and social functioning during 16 years of follow-up in 3,107 older men and women from the Longitudinal Aging Study Amsterdam.
Method
The Longitudinal Aging Study Amsterdam
A random sample stratified by age, sex, and expected 5-year mortality was drawn from the population registers of 11 municipalities in three areas—the western, northeastern, and southern parts of the Netherlands. In total, 3,107 subjects (response rate 62%) were enrolled in the baseline main examination (1992-1993) and 2,671 in the baseline medical examination, and were representative of the Dutch older population. Examinations were conducted in the participants’ home by trained interviewers and recorded for quality monitoring. Details regarding the sampling and data collection procedures, response rate, and attrition are described in detail elsewhere (Huisman et al., 2011). Follow-up medical examinations were conducted in 1995/1996 (N = 1,509), 1998/1999 (N = 1,382), 2001/2002 (N = 1,307), 2005/2006 (N = 981), and 2008/2009 (N = 761) during which lifestyle information was obtained. In 1996/1996, only participants born before 1931 were included in the sample of the medical examination. For each examination wave, participants with complete data on all four lifestyle factors and with data on at least one functioning domain were included (91.1%-94.5%). For the time lag models, only participants with complete data on either functioning domain (assessed during main examination) during at least two consecutive examination waves were included (70.1%-75.7%). Wave 2005/2006 was thus included as the last “baseline wave” for assessment of the lifestyle factors. Written informed consent was obtained from all participants. The study was approved by the Medical Ethics Committee of the VU University Medical Center.
Lifestyle Assessment
Lifestyle was assessed at each examination. International guidelines were used to assess meeting lifestyle recommendations. Self-reported smoking status was categorized as never, former, or current. Participants who had quit smoking >20 years ago were considered never smokers (Kenfield, Stampfer, Rosner, & Colditz, 2008). The number of alcohol drinks per week was assessed. Participants were categorized into nondrinkers, moderate drinkers, and excessive drinkers (>7 drinks per week for women and >14 drinks per week for men; Dutch Health Council, 2006; U.S. Department of Health and Human Services & U.S. Department of Agriculture, 2015). Physical activity in the past 2 weeks was obtained by using the LASA physical activity questionnaire (LAPAQ) which was validated against pedometer counts and activity diaries in older persons (Stel et al., 2004). The average total time spent per day on at least moderate-intensity activities (walking outdoors, bicycling, heavy household activities, and sports activities) was calculated and dichotomized according to the physical activity recommendation for older adults: <150 versus 150+ min/week (Physical Activity Guidelines Advisory Committee, 2008; World Health Organization, 2010). Measured body weight and height were used to calculate the body mass index (BMI, kg/m2). A BMI ≥ 20 kg/m2 and <30 kg/m2 was considered to indicate a healthy body weight for older adults (Heiat, Vaccarino, & Krumholz, 2001; Janssen, 2007; World Health Organization, 2000).
A healthy lifestyle score was calculated as the sum of healthy lifestyle factors per person. Healthy lifestyle factors were never smoking (or had quit >20 years ago), moderate alcohol consumption, meeting the physical activity recommendation, and a healthy body weight. Non-drinking was not included in the healthy lifestyle factor for alcohol as previous research has shown that Dutch older nondrinkers often are former drinkers who had to quit because of deteriorating health (Comijs, Aartsen, Visser, & Deeg, 2012). The healthy lifestyle score ranged from 0 (unhealthy lifestyle) to 4 (healthy lifestyle).
Outcome Measures
Four domains of functioning that previously were distinguished in the concept of successful aging were considered, including physical, psychological, cognitive, and social functioning (Baltes & Baltes, 1990). Each domain was assessed at each examination and used as an outcome measure.
Measured gait speed during a standardized walk test was used as an indicator of physical functioning, as gait speed is the strongest, objectively assessed predictor of future disability and also an important predictor of early mortality in older persons (Guralnik et al., 2000; Studenksi et al., 2011). Participants were instructed to walk 3 m, make a 180° turn, and walk back 3 m as fast as possible. Time needed to perform the test was recorded and used to calculate walking speed. Faster walking speed indicates better physical functioning. Participants not able to perform the complete test due to physical or cognitive problems (0.2%-7.8% depending on examination wave) were excluded from the analyses.
Depressive symptoms in the previous week, assessed by the 20-item Center for Epidemiologic Studies Depression (CESD) scale, was used as an indicator of psychological functioning (Radloff, 1977). The scale, ranging from 0 to 60, has been widely used in older populations and is a valid and reliable instrument for Dutch older adults (Beekman et al., 1997). A lower score indicates better psychological functioning. The CESD has been shown a valid measure of the full spectrum of depressive symptoms in this older population (Beekman et al., 1995).
Cognitive functioning was assessed using the Mini Mental State Examination scale, a frequently used screening instrument for global cognitive dysfunction (Folstein, Folstein, & McHugh, 1975). The instrument is not suitable for diagnosis of dementia but can be used to monitor change in cognitive status over time (Tombaugh & McIntyre, 1992). Scores range from 0 to 30. A higher score indicates better cognitive functioning.
Social relationships are seen as an important component of successful aging and one of the important life goals (Charles & Carstensen, 2009). This is most clear for measures of social involvement that capture both the structure and the content of relationships (Holt-Lunstad, Smith, & Layton, 2010). Social functioning was assessed by the number of personal network members identified by name where contact frequency was at least monthly, thereby capturing the engagement of respondents in social activity. Relationships were identified with a domain-specific approach (Van Tilburg, 1998). First, in each of seven domains of role-type relationships (e.g., kin and neighbors), the following question was asked: “Name the persons you have frequent contact with and who are also important to you.” Only persons above the age of 18 were included and the partners were excluded. Next, for each relationship identified, contact frequency was assessed in eight categories, ranging from less than once a year to daily, to identify socially active relationships. Only relationships with at least a monthly contact frequency were included.
Potential Confounders
Baseline age, sex, education level, partner in household, number of chronic diseases, and self-rated health were used as potential confounders. Education level was assessed by asking the respondent for the highest education level completed and was categorized into high (university, college, higher vocational, general secondary, and intermediate vocational education), middle (general intermediate and lower vocational education), and low (elementary education or less). Partner in household was dichotomized as yes/no. Self-reported chronic diseases included chronic nonspecific lung disease, cardiac disease, peripheral atherosclerosis, stroke, diabetes mellitus, arthritis, and cancer. The number of chronic diseases was categorized as none, one, and two or more. For self-rated health, participants were asked the following: How is your health in general? Response options ranged from 1 (very good) to 5 (poor). Self-rated health was included as a measure of underlying health that is not captured by self-reported chronic diseases.
Statistical Analyses
Data were analyzed using SPSS version 19.0 (SPSS Inc., Chicago, Illinois). Linear mixed models were used to determine the annual decline in physical, psychological, cognitive, and social functioning after adjustment for sex, baseline age, education level, partner in household, number of chronic diseases, and self-rated health. To investigate whether those with a more healthy lifestyle experienced a slower decline in functioning in 3 years, linear mixed models with a 3-year time lag were used to examine the association of time-varying individual lifestyle factors and the healthy lifestyle score at each examination with physical, psychological, cognitive, and social functioning 3 years later, adjusting for baseline functioning as well as sex, baseline age, time, education level, partner in household, number of chronic diseases, and self-rated health. When investigating a single lifestyle factor, additional adjustment was made for the other three lifestyle variables in the model. All lifestyle variables were included in a time-dependent manner. For the random part of the models, an unstructured covariance structure was used. Potential interaction was tested between the healthy lifestyle score and baseline age to determine whether the observed associations differed between young-old and old-old participants, and between the healthy lifestyle score and sex to determine whether the observed associations differed between men and women. A p value of <.05 was considered to be statistical significant. To allow comparison of the associations between domains of functioning, all functioning measures were also expressed per standard deviation so that the regression coefficients can be interpreted as standardized coefficients.
Results
Across the examination waves, 52.8% to 74.6% of the participants were never smoking, 54.3% to 59.8% were moderate alcohol drinker, 66.6% to 75.4% met the physical activity recommendation, and 72.1% to 79.3% had a healthy body weight (Table 1). An overall healthy lifestyle (meeting the recommendation for all four lifestyle factors) was observed for 18.6% to 25.2% across examinations. The four functioning domains were weakly associated with each other in the expected directions (correlation coefficients varied between .06 and .27 across all examination waves).
Characteristics of the Study Participants at the Baseline (1992-1993) and Four Follow-Up Examination Waves: The Longitudinal Aging Study Amsterdam.
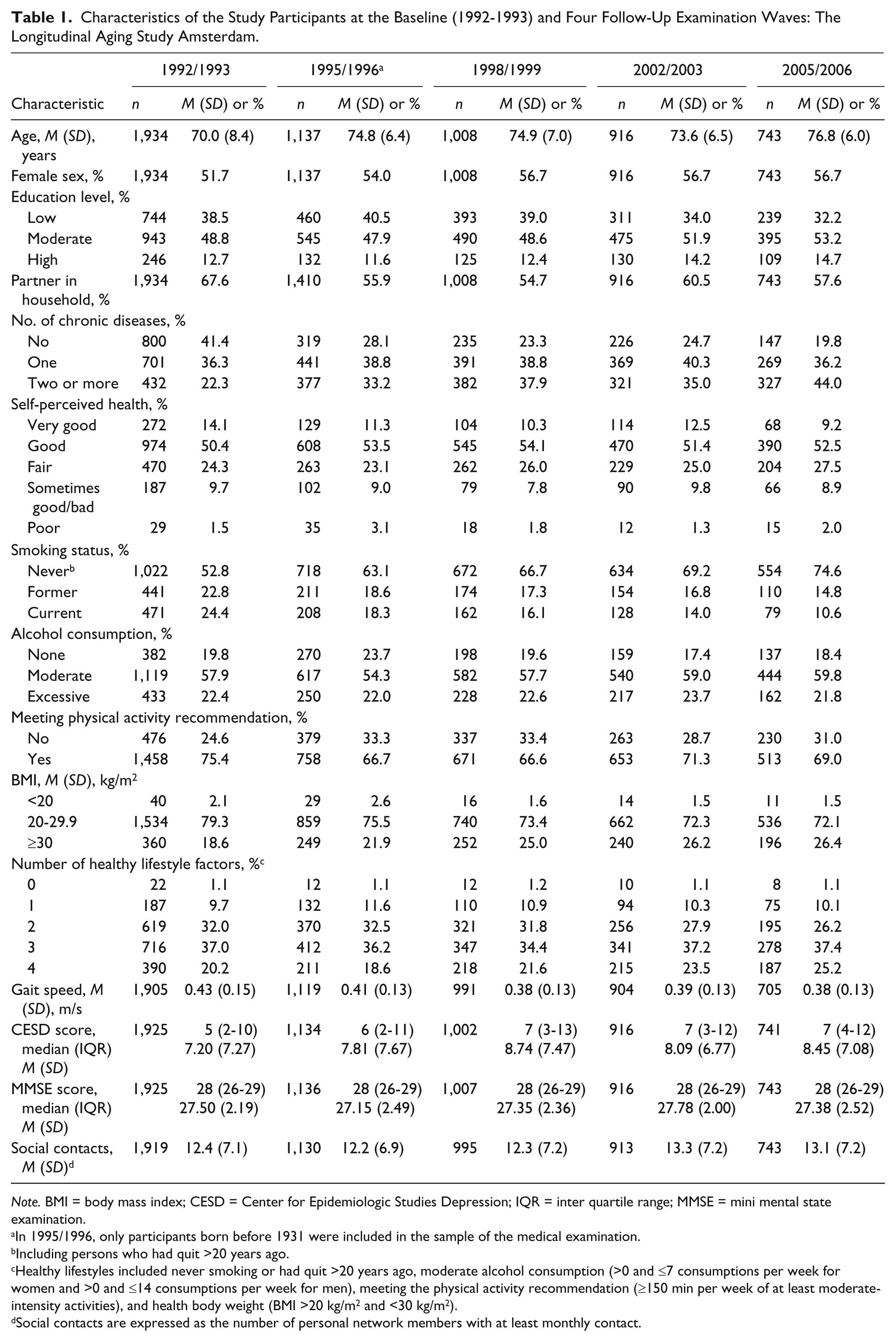
Note. BMI = body mass index; CESD = Center for Epidemiologic Studies Depression; IQR = inter quartile range; MMSE = mini mental state examination.
In 1995/1996, only participants born before 1931 were included in the sample of the medical examination.
Including persons who had quit >20 years ago.
Healthy lifestyles included never smoking or had quit >20 years ago, moderate alcohol consumption (>0 and ≤7 consumptions per week for women and >0 and ≤14 consumptions per week for men), meeting the physical activity recommendation (≥150 min per week of at least moderate-intensity activities), and health body weight (BMI >20 kg/m2 and <30 kg/m2).
Social contacts are expressed as the number of personal network members with at least monthly contact.
Compared with persons excluded from the time lag models due to missing data on lifestyle factors or missing follow-up data, those included were younger, higher educated, more often had a partner, had less chronic diseases, and better self-rated health. They also had a better functioning level across all domains and a healthier lifestyle except for smoking. These differences were consistent across examination waves (data not shown).
During follow-up (between 1992/1993 and 2008/2009), after adjustment for sex, baseline age, education level, partner in household, number of chronic diseases, and self-rated health, the average annual decline in gait speed was −0.0066 m/s (95% confidence interval [CI] = [−0.0072, −0.0061]) or −1.76%, the average annual increase in CESD score 0.059 [0.031, 0.087] points or 0.57%, the average annual decrease in MMSE score −0.090 points [−0.102, −0.079] or −0.33%, and social contacts −0.035 [−0.064, −0.006] or −0.30%.
Never smoking was associated with a slower decline in physical, emotional, and social functioning (Table 2). Moderate alcohol consumption was not associated with better functioning in any of the four functioning domains. Including the nondrinkers in the moderate group did not change these results. Meeting the physical activity recommendation was associated with a slower decline in physical and cognitive functioning, while having a healthy body weight was associated with a slower decline in physical and emotional functioning. The interaction between baseline age and meeting the physical activity recommendation was statistically significant for gait speed (p = .012), CESD score (p = .010), and MMSE score (p < .001), indicating that the association between meeting the physical activity recommendation and decline in physical and cognitive functioning was stronger in those who were older at baseline.
The Time-Lag Associations a of Four Time-Varying Healthy Lifestyle Factors With Physical, Psychological, Cognitive, and Social Functioning After 3 Years of Follow-Up in Older Participants of the Longitudinal Aging Study Amsterdam.
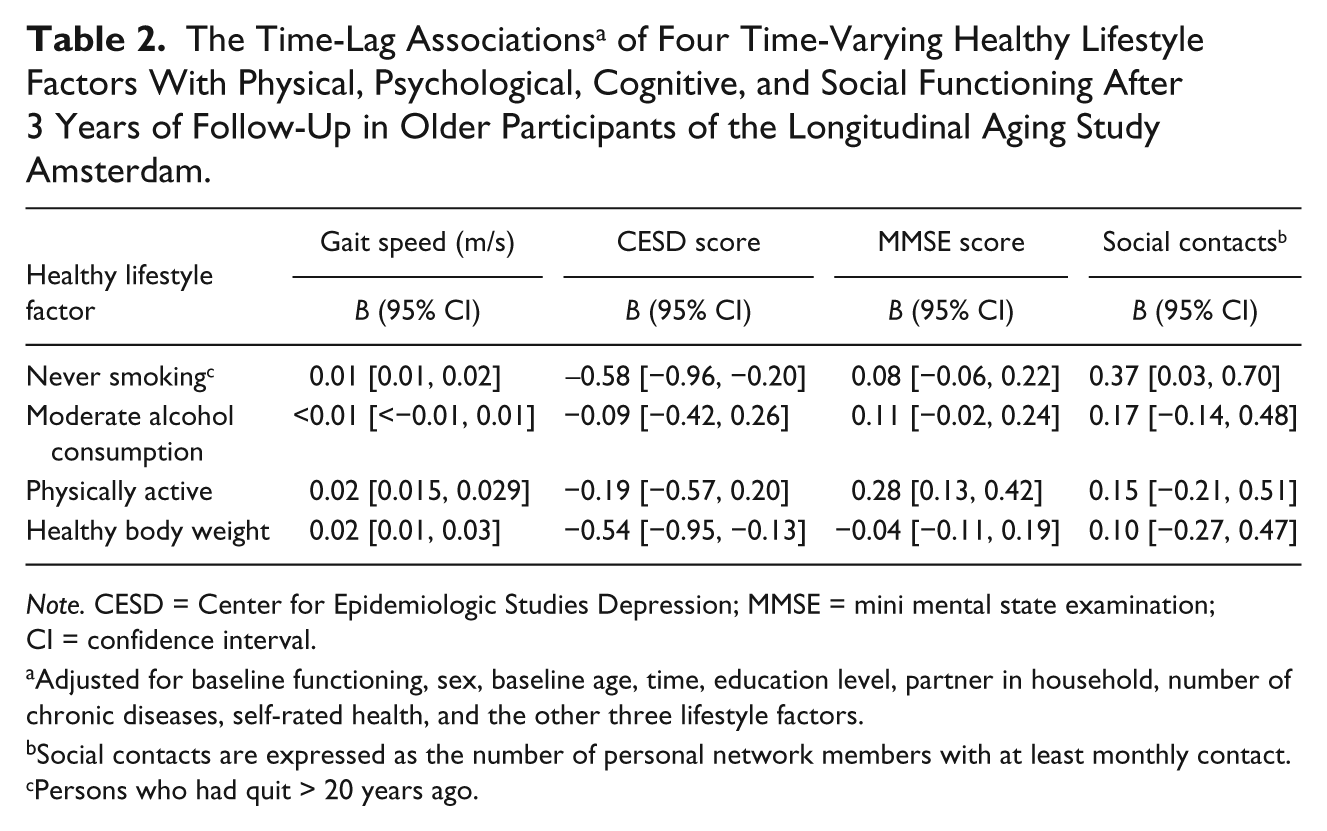
Note. CESD = Center for Epidemiologic Studies Depression; MMSE = mini mental state examination; CI = confidence interval.
Adjusted for baseline functioning, sex, baseline age, time, education level, partner in household, number of chronic diseases, self-rated health, and the other three lifestyle factors.
Social contacts are expressed as the number of personal network members with at least monthly contact.
Persons who had quit > 20 years ago.
Adherence to more lifestyle recommendations was consistently associated with a slower 3-year rate of decline in functioning level across all four domains (P for trend < .02; Table 3). An overall healthy lifestyle (=adherence to all four lifestyle recommendations) was associated with a slower rate of decline on all four functioning domains compared with no or one healthy lifestyle factor. Participants with an overall healthy lifestyle experienced on average a 0.04 m/s or 10.6% slower decline in gait speed and a 1.1 points or 10.8% slower increase in CESD score as compared with participants who adhered to no or one healthy lifestyle recommendation. Furthermore, they had a 0.47 or 1.8% slower decline in MMSE score and 0.58 or 4.9% slower decline in social contacts. These associations were similar for men and women and did not differ with time or baseline age, with a single exception: the association of an overall healthy lifestyle with decline in MMSE score became stronger with higher baseline age (p value for interaction <.001).
The Time-Lag Associations a of the Time-Varying Number of Healthy Lifestyle Factors With Physical, Psychological, Cognitive, and Social Functioning After 3 Years of Follow-Up in Older Participants of the Longitudinal Aging Study Amsterdam.
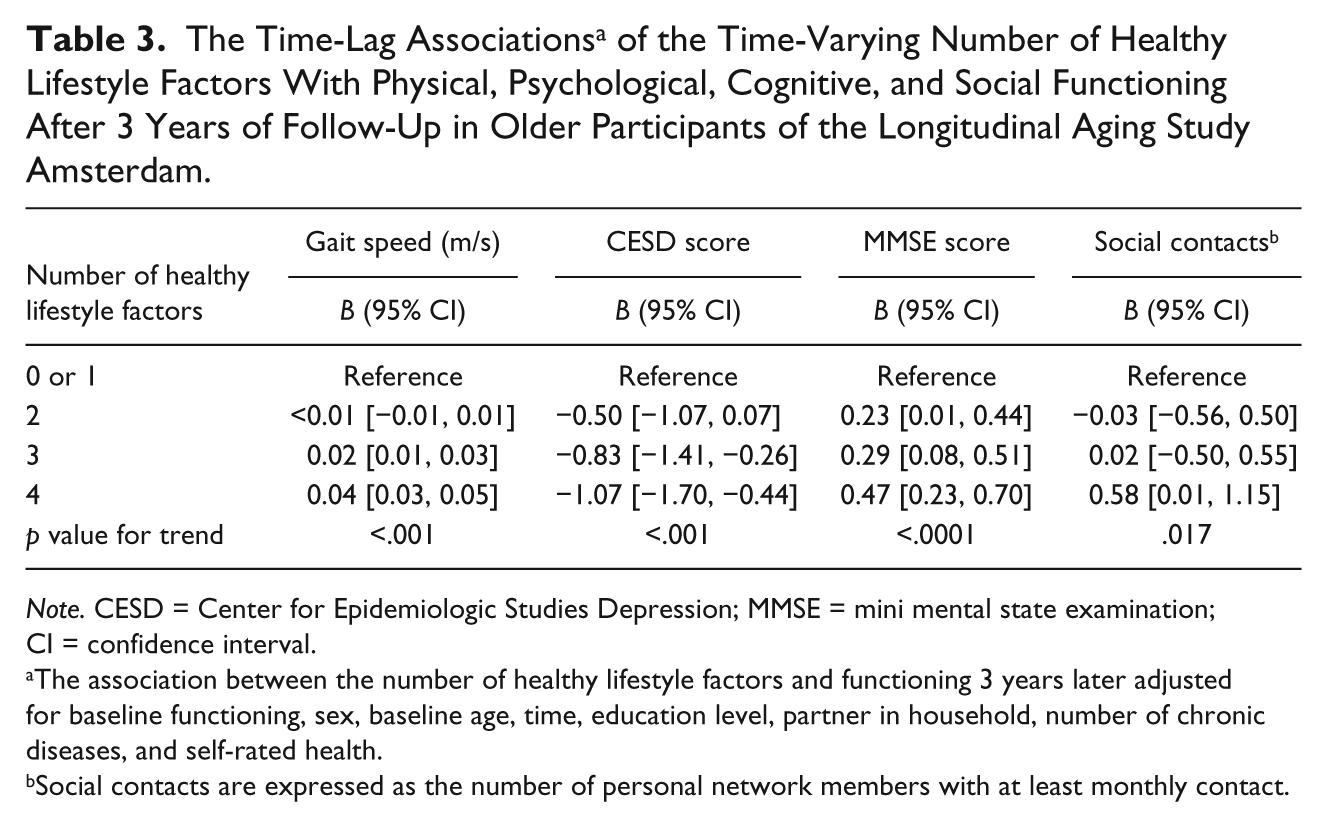
Note. CESD = Center for Epidemiologic Studies Depression; MMSE = mini mental state examination; CI = confidence interval.
The association between the number of healthy lifestyle factors and functioning 3 years later adjusted for baseline functioning, sex, baseline age, time, education level, partner in household, number of chronic diseases, and self-rated health.
Social contacts are expressed as the number of personal network members with at least monthly contact.
To be able to compare the impact of an overall healthy lifestyle between the four functioning domains, Figure 1 shows the standardized regression coefficients of the associations with decline in physical, psychological, cognitive, and social functioning. Adherence to more healthy lifestyle factors had the greatest impact on the decline in the physical functioning domain (standardized coefficient 0.28, small to medium effect size) and the least impact on the decline in the social functioning domain (standardized coefficient 0.08, small effect size).
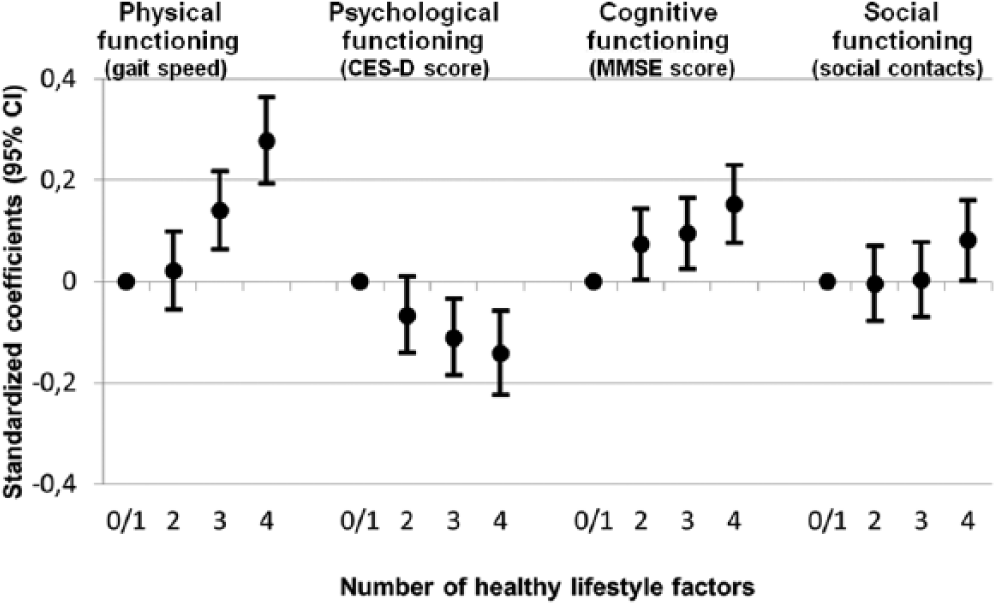
Associations between the number of healthy lifestyle factors and 3-year decline in four domains of functioning during 16 years of follow-up: The Longitudinal Aging Study Amsterdam.
Discussion
The results of this prospective study among a nationally representative sample of older men and women show that leading a lifestyle according to official, international lifestyle recommendations for older adults is associated with a 1.8% to 10.8% slower decline in physical, psychological, cognitive, and social functioning with aging. The benefits of an overall healthy lifestyle were still present, and sometimes even highest, in the oldest participants and did not differ between men and women.
The difference in decline in gait speed between those with an overall healthy lifestyle and those with no or one healthy lifestyle factor was 0.04 m/s. The meaningful change in gait speed based on a standardized walking test is estimated to range between 0.03 and 0.05 m/s (Kwon et al., 2009). Furthermore, every 0.1 m/s slower gait speed is associated with a 12% higher mortality (Studenksi et al., 2011). With respect to psychological functioning, we observed that persons with an overall healthy lifestyle had a 1.1 point slower increase in CESD score compared with those with no or one healthy lifestyle factor. The standardized coefficient corresponds with a small effect size and may have some clinical significance. An overall lifestyle was associated with a slower decline in MMSE score over time and thus could help to maintain cognitive reserve in old age. For social functioning, the relatively small change in social contacts over time may be caused by an opposing trend: relationships with kin become more intensive with age, whereas relationships with friends and nonkin decrease in frequency (Shaw, Krause, Liang, & Bennett, 2007; Van Tilburg, 1998). In this light, the result that an overall lifestyle contributes to a slower decline in social functioning over time can be considered significant.
From 1996 to 2007, the percentage of older adults in the United States with an overall healthy lifestyle (defined as no current smoking, any exercise, ≥5 servings/day of fruits and vegetables, and BMI<25 kg/m2) decreased from 9.0% to 6.9% in those aged 60 to 69 years and from 12.0% to 9.9% in those aged ≥70 years (Ford et al., 2010). Studies partly conducted in other countries during this same time period confirm the reduced prevalence rates of healthy lifestyle factors in (older) adults with the exception of smoking (Centers for Disease Control and Prevention; Janssen, Shields, Craig, & Tremblay, 2011; Visser, Pluijm, van der Horst, Poppelaars, & Deeg, 2005; Yang et al., 2012). Based on previous research showing that an unhealthy lifestyle of older adults is associated with higher mortality rates, the lifestyle deterioration of older persons is predicted to negatively affect life expectancy in the future (Olshansky et al., 2005; Van den Brandt, 2011). The current study importantly extends the findings by showing that the overall lifestyle deterioration of older adults may also negatively impact a comprehensive range of functioning and may therefore hamper successful aging in the general population. Several short-term intervention studies focusing on physical activity or weight loss showed that lifestyle improvement in old age is beneficial for health and physical functioning (LIFE Study Investigators et al., 2006; Whelton et al., 1998). To what extend an overall lifestyle modification in old age may impact health and physical functioning needs to be determined in long-term randomized controlled trials.
Strength of this study is the inclusion of four important domains of functioning in old age as outcome measures, thereby extending the results of previous studies that mainly focused on morbidity and mortality. Further strengths are the extensive follow-up period of 16 years, the nationally representative sample, and the use of linear mixed models with time lag allowing incorporating all available information on lifestyle and functioning at different examination waves. The use of dichotomized lifestyle variables based on international lifestyle recommendations allows for a clear public health interpretation of the study findings.
The potential limitations of our study include (selective) attrition. As persons with an unhealthy lifestyle have a higher mortality risk, participants with an unhealthy lifestyle and still alive at older age may have a better tolerance for the unhealthy lifestyle. Indeed, a slight increase in the percentage of older persons with an overall healthy lifestyle was seen with each follow-up examination. This so called “depletion of susceptibles” effect may have caused an underestimation of the observed associations.
A second potential limitation is that lifestyle was based on self-report with the exception of BMI. Response bias, including social desirability bias, may have caused an underestimation of the observed associations. Also, other important lifestyle factors, including dietary intake, sleep, stress management, and medication compliance, were not included in our study. Finally, this is an observational study and causality can only be inferred. However, the results using the time lag model support a preventive role of lifestyle on functioning in old age.
In conclusion, the results of this study indicate that an overall healthy lifestyle in old age, consisting of never smoking, moderate alcohol consumption, being physically active, and having a healthy body weight, is associated with slower declines in physical, psychological, cognitive, and social functioning with aging. A healthy lifestyle seems beneficial up to very old age. As only one out of five older adults had an overall healthy lifestyle in this study, there is considerable room for lifestyle improvement. Health professionals should communicate that a healthy lifestyle benefits all domains of functioning with aging, in addition to preventing disease and increasing life expectancy. Also, older adults should be encouraged to discuss healthy lifestyle changes with their health professional, that is, through public awareness campaigns. These efforts may help to reverse the deteriorating lifestyle trends over time observed among older adults and may lead to more successful aging in the general population by adding well-functioning years to an increasing life span.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Longitudinal Aging Study Amsterdam is supported by a grant from the Netherlands Ministry of Health Welfare and Sports, Directorate of Long-Term Care. Funding for this article was also provided by the European Union FP7 MooDFOOD Project “Multi-country cOllaborative project on the rOle of Diet, FOod-related behaviour, and Obesity in the prevention of Depression” (grant agreement no. 613598).