
Abstract
Introduction
To ensure that the increasingly longer lives of older people are worth living, attention needs to be paid to maintaining the positive sides of life during aging. The contributions of older persons to their own well-being and the well-being of their families and other people are of central interest in societies with a growing proportion of older people. World Health Organization (WHO) defined the policy goal active aging in 2002 as follows: “Active aging is the process of optimizing opportunities for health, participation and security in order to enhance quality of life as people age” (WHO, 2002). The same document also states, “these policies and programmes should be based on the rights, needs, preferences and capacities of older people.”
During the recent years, diverse use has been made of the term active aging. Some researchers have sought to categorize individuals and define an active aging phenotype based on the WHO definition. For example, the maintenance of positive subjective well-being; good physical, social, and mental health; good functional ability and fitness; and continued involvement in one’s family, peer group, and community throughout the aging process have been proposed as aspects that describe an active aging phenotype (Fernández-Ballesteros, Robine, Walker, & Kalache, 2013). Some attempts have been made to validate an empirical model of an active aging phenotype based on the WHO definition by using, for example, latent factor analysis in survey data. However, the authors concluded that it was not possible to create a statistical model that would fit their data (e.g., Bélanger, Ahmed, Filiatrault, Yu, & Zunzunegui, 2017; Paúl, Ribeiro, & Teixeira, 2012).
The WHO definition of active aging is a goal for societies aimed at spurring them to make provision for the participation of older individuals in valued activities through such means as social security schemes, environmental and urban planning, health services, civil society, and legislation. An example of how active aging is assessed at the societal level is the Active Aging Index which ranks countries according to different societal indicators such as participation of older people in the workforce or life expectancy (“Active Ageing Index Home,” 2017). However, the WHO definition does not refer to active aging as a state of well-being or as good quality of life of individuals. It is not a phenotypic definition that can be applied to individuals or groups of individuals. To assess the active aging of individuals, we first need a definition that centers on the individual.
To this end, we suggest the following definition: the striving for elements of well-being through activities relating to a person’s goals, functional capacities and opportunities. This definition encompasses four central sides in the active aging of individuals: their goals (what they want to do), their functional capacity (what they are able to do), their autonomy (perceived opportunities to do the valued activities), and their activities (what they actually do). We hypothesize that active aging maintains or promotes well-being.
In reviewing earlier suggestions for active aging assessment scales, we found a scale that had been developed through a multiphase process, and which assesses active aging as a way to promote well-being. In Thailand, researchers developed a seven-factor 36-item scale containing the following factors: being self-reliant, being actively engaged with society, developing spiritual wisdom, building up financial security, maintaining a healthy lifestyle, engaging in active learning, and strengthening family ties to ensure care in later life (Thanakwang, Isaramalai, & Hatthakit, 2014). The authors conclude that although the content of some factors may be culture-specific, the factors included in this scale describe the actions that, within their culture, older people themselves initiate to promote their own well-being. In this latter respect, the idea underlying our scale resembles that of the Thai-scale.
The goal of this study was to develop a quantitative scale for assessing active aging among older people that can be used in research and practice. This article reports the process of developing the University of Jyvaskyla Active Aging Scale (UJACAS) and describes the final scale.
Method
The Process of Developing the UJACAS
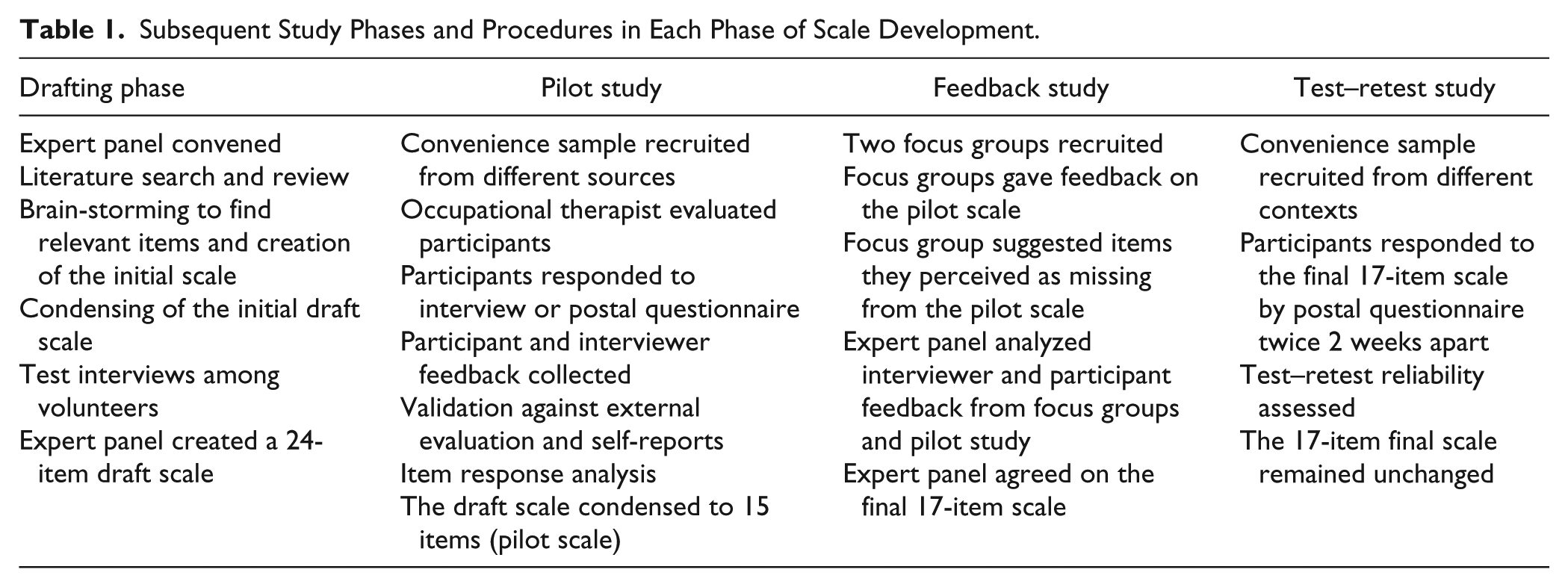
The UJACAS scale development process is described in Table 1. First, an expert panel consisting of six members was convened that included representatives of gerontology, psychology, education, physiotherapy, sport sciences, statistics, and public health. The panel’s goal was to create a draft version of the assessment scale and throughout the scale development process decide on the phrasing of the items and which items to include in the final scale. The starting point for developing the scale items were the Activities and Participation categories of the International Classification of Functioning, Disability and Health (“Towards a Common Language for Functioning, Disability and Health, ICF,” 2002) which provide a valid, well-thought-out classification of essential life areas. The expert panel studied scales developed for similar or closely related topics, created potential scale items, and produced a 24-item draft questionnaire that was then tested in a pilot study. The pilot study goals were to assess the item properties, to condense the scale, and to assess its validity and reliability. The resulting condensed pilot scale with 15 items was exposed to two focus groups of older people consisting of four and five people to gain their input and views in the feedback study phase. The participant feedback on the scale led to the addition of two further items. The resulting final active aging scale comprised 17 items. The final phase of the scale development was test–retest analysis to determine the stability and reliability over time of the final UJACAS.
Subsequent Study Phases and Procedures in Each Phase of Scale Development.
Ethics
This project was approved by the Ethical Committee of the University of Jyvaskyla, Finland. The study was conducted according to the guidelines for good scientific and clinical practice laid down by the Declaration of Helsinki. Participants were informed about the research verbally and in writing. In the pilot study and test–retest study, the participants consented by returning the questionnaire. Focus group members and interview participants signed an informed consent form prior to the group meeting or interview.
Pilot Study
One hundred fifty-nine participants were recruited from different sources (a health center flue vaccination campaign, a rehabilitation trial, assisted living facilities, University of the Third Age, and through word of mouth) to guarantee a sufficiently heterogeneous convenience sample.
Interview with occupational therapist
In the absence of a true golden standard for rating of active aging, we considered that a trained occupational therapist could serve as an external evaluator for active aging. The occupational therapist evaluated the 45 participants’ activity in an interview based on the “Canadian Occupational Performance Measure” (COPM; 2017). Each interview lasted for 30 min and was started by asking the respondent to describe their daily routines in a typical week. The occupational therapist aimed at finding out about the participant’s meaningful activities and whether there were activities that he or she wanted to do but could not do or for some other reason did not do. Participants were also asked to describe their functional ability in their own words. Based on the interview, the occupational therapist gave the participant a score ranging from 0 (not active at all) to 10 (the highest level of activity and participation in meaningful activities). The score was not revealed to the participants, who subsequently took part in a separate interview focused on their own assessments of their own active aging and answered the pilot version of the active aging scale and the validation questions.
Active aging pilot scale and validation questions
The pilot scale assessing active aging comprised 24 items in four sides, each forming a subscale. Questions were phrased as follows and were answered on a five-point Likert-type scale. The four sides with the framing questions were as follows: Goals: “During the previous four weeks, I have wanted to . . .” Ability: “During the previous four weeks, I have or would have been able to . . .” Autonomy: “During the previous four weeks, my opportunity to . . .” Activity: “During the previous four weeks, I did . . .”
Response options were worded to suit the item and scored from 0 (lowest, for example, least active) to 4 (highest, for example, most active). Scores were computed by summing the scores of the individual items of each side to form a subscale and of the total questionnaire to form the total score. A maximum of two missing items was allowed for each subscale and eight for the total sum score. To correct for missing items, we used the following formulas: (sum score / items responded to) × items offered.
The pilot questionnaire included validation questions on socio-demographic background, health, quality of life, life-space mobility, physical activity, participation and autonomy, and opportunities to provide feedback about the study. To gain an idea of their goals, people were asked how strongly they agreed with the claim “I have special interests in my life” with five-point Likert-type scale response options ranging from strongly agree to strongly disagree. Poor health as a barrier to active aging was elicited with a question “To what extent has your health or functional ability prevented you from doing activities that you wanted to do during the four previous weeks?” The opportunity for active aging was elicited with a question “To what extent have other matters related to your life or environment prevented you from the activities that you wanted to do during the past four weeks?” For both questions, responses were given on a five-point Likert-type scale ranging from very much to not at all. Autonomy was assessed with a question “Do you feel that you have sufficient control over your own life? Do you think that your opportunities to live the way you wish are very good, good, fair, bad, or very bad?” (Cardol, de Haan, de Jong, van den Bos, & de Groot, 2001). Self-rated health was elicited with a question “How do you perceive your health at the moment?” on a five-point response scale ranging from very good to very poor (Subramanian, Huijts, & Avendano, 2010). Quality of life was elicited with a question “How do you rate your quality of life?” using a similar response scale (The World Health Organization Quality of Life [WHOQOL] Group, 1998). To evaluate the community mobility of the participants, the questionnaire included two questions drawn from the University of Alabama at Birmingham Life-Space Assessment (Baker, Bodner, & Allman, 2003). Question LS5 was “Have you been outside your own municipality during the last for weeks?” Question LS4 was as follows: “Have you been outside your own neighborhood during the last for weeks?” The response options for both were as follows: No (scored 0); Yes, less than once a week (scored 1); Yes, one to three times a week (scored 2); Yes, four to six times a week (scored 3); Yes, daily (scored 4). Based on these responses, a life-space mobility score ranging from 0 to 36 was calculated as follows: sum score = (4 × LS4 score) + (5 × LS5 score).
Feedback Study
Two focus groups of older people (five and four members, respectively) gave their perceptions of the relevance of the items comprising the 15-item pilot scale. The focus groups were recruited from the University of the Third Age and through word of mouth. Each focus group discussion lasted 2 hr and was led by an expert panel member while other researchers made notes of the comments made. In the discussion, each item on the scale was discussed for its relevance, clarity, and possible interpretation from a respondent’s perspective. An important discussion topic concerned potential aspects of active aging that were missing from the scale.
The expert panel considered the participants’ feedback from the focus groups, the pilot study interviews, and questionnaires along with the feedback received from the interviewers. The expert panel continued their discussions until a consensus was reached on the number of items and their phrasing.
Test–Retest Study
The final UJACAS that was examined for test–retest reliability comprised 17 items. The scores were calculated as in the pilot study. A maximum of two missing items from each subscale were allowed.
Statistical Methods
Single-item properties were described by using the logit measures from one-parameter logistic (Rasch) model. Rasch modeling was conducted for sub-scores and the total score. Rasch model assumes that items capture different levels of an essentially unidimensional underlying trait. In the model, each item receives fit index estimates indicating how plausible the model is with any given item. We report infit mean-square values, which indicate how predictable the item is. Values in the range of 0.6 to 1.4 indicate optimal predictability, whereas higher values suggest random noise and lower values too high a level of predictability. Finally, we calculated point-biserial correlations to estimate item-total correlations. Low correlations (less than 0.20) may indicate poor item discrimination. We report Cronbach reliability coefficient alphas as estimates of the lower bound of reliability for subscales scores and total score. We calculated person and item separation reliabilities as indices of the ability to separate the active aging levels of persons and items. We assessed scale dimensionality by plotting eigenvalues of the correlation matrix into Cattell’s scree plot. Parallel analysis was conducted to estimate eigenvalues resulting from the modeling of random noise data. Observed data eigenvalues exceeding eigenvalues from the parallel analysis were considered material.
We assessed the validity of the 15-item pilot UJACAS scale against the occupational therapist’s assessment of active aging, against the participants’ own assessments of their active aging level and against separate self-reported questions by calculating correlation coefficients. We assessed the test–retest reliability of the subscales and total scale with intra-class correlation coefficients and t-tests for repeated measures and for individual items with kappa coefficients.
Results
The pilot study comprised a convenience sample of 159 participants. Of these, 45 attended the occupational therapist’s evaluation that formed an external criterion for active aging. Altogether 114 people responded independently to the pilot scale in the postal questionnaire and returned it to us by mail. The participants were 65 to 94 years old (mean age 73.4 years, SD 6.8), 68% were women, 62% rated their health as good or very good, 32% as average, and 6% as poor or very poor. In all, 75% reported no difficulty walking a distance of 2 km, whereas the rest reported minor or major difficulties or inability to walk such a distance. Tertiary education was reported by 64%.
Based on the Rasch model and feedback from the participants, we identified nine items in the 24-item pilot scale that had low variability, low infit or low person or item separation, or showed random effects in the responses. These items were omitted (shown in Table 2). The resulting pilot scale contained 15 items. Table 3 shows the item properties of these items in the pilot data. The reliability indices for all the subscales and the total scale were ≥0.68, and thus good. The Rasch modeling of pilot scale showed that the total score consisting of the four sub-scores captures a unidimensional latent construct of active aging.
The Items of the UJACAS at the Different Study Phases.
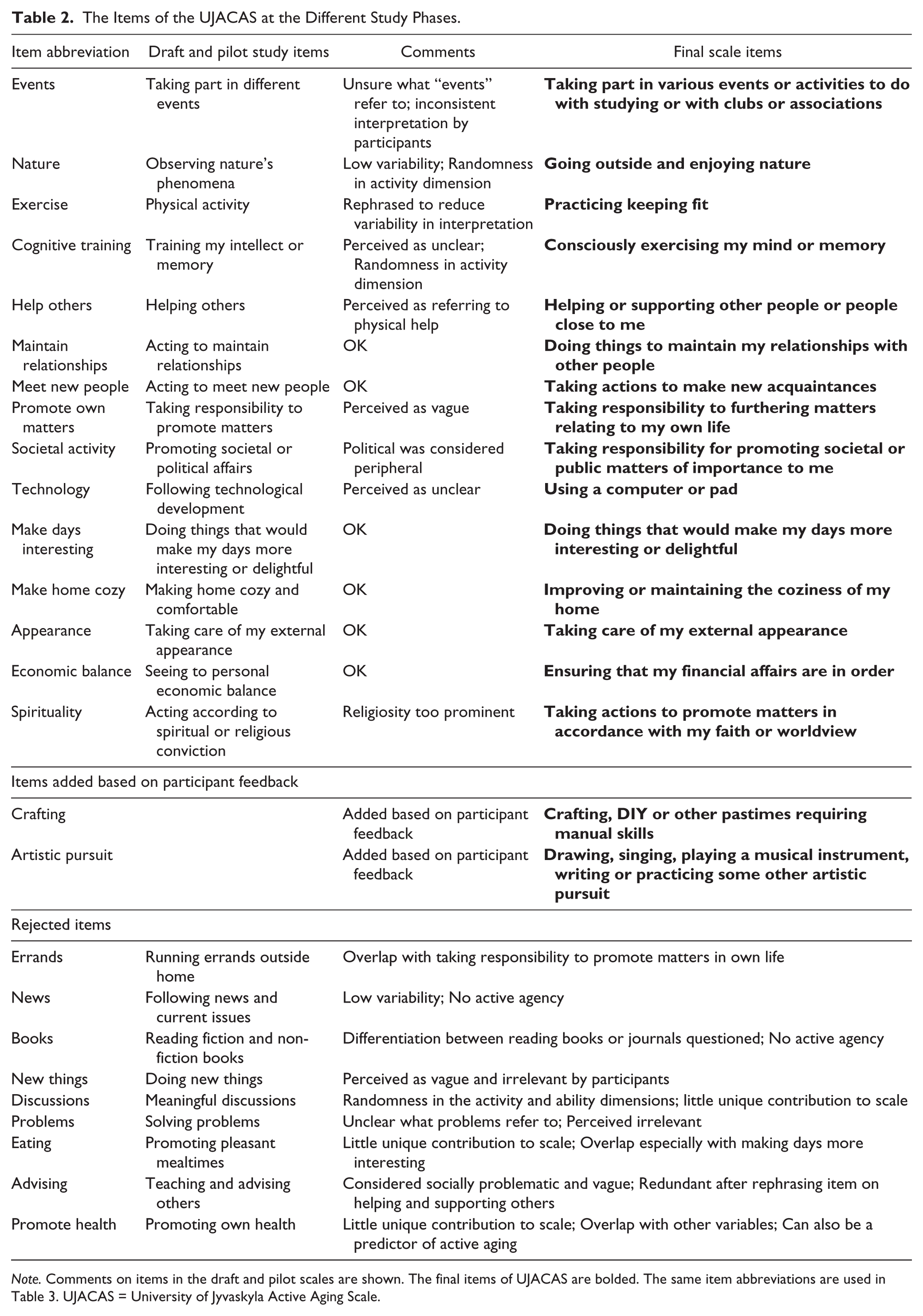
Note. Comments on items in the draft and pilot scales are shown. The final items of UJACAS are bolded. The same item abbreviations are used in Table 3. UJACAS = University of Jyvaskyla Active Aging Scale.
Measurement Properties of the University of Jyvaskyla Active Aging Pilot Scale, Subscales Including Measure Est, Its SE, Infit, and Pbc.
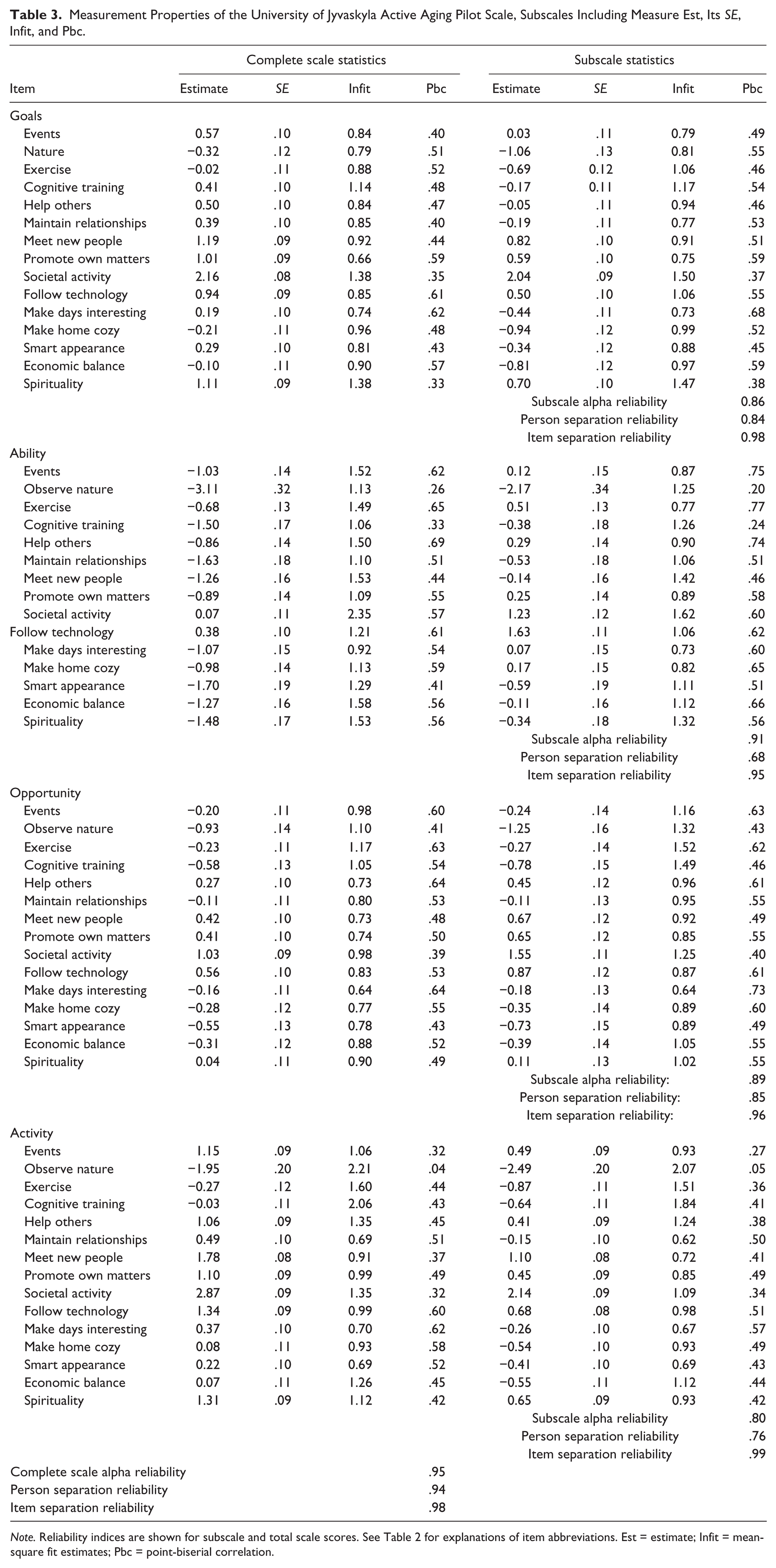
Note. Reliability indices are shown for subscale and total scale scores. See Table 2 for explanations of item abbreviations. Est = estimate; Infit = mean-square fit estimates; Pbc = point-biserial correlation.
Scale Validity
The mean value for participants’ own assessment of active aging was 7.77 (SD 1.70), and for occupational therapist’s assessment, 8.71 (SD 1.74). The correlation between these two assessments was r = .508 (p < .001, n = 44). The higher were the occupational therapist’s assessment and the participants’ own assessment of their active aging, the higher were the scores in the UJACAS scale (Table 4). The occupational therapist’s evaluation correlated most closely correlated with the ability dimension of UJACAS while the self-assessments captured the four dimensions more uniformly. If people reported barriers to active aging, the UJACAS scores were lower, whereas good self-rated health, quality of life, autonomy, and high life-space mobility correlated with higher UJACAS scores, indicating a higher level of active aging. Parallel correlations were observed for interviewees and postal questionnaire respondents. Similarly, no material gender differences were observed in the correlations; however, the correlations of UJACAS scores and self-rated health were somewhat weaker for men.
Pearson Correlation Coefficients Between the University of Jyvaskyla Active Aging Scale Scores and the Validation Variables (N = 155, Except for the Occupation Therapist’s Assessment N = 44-45).
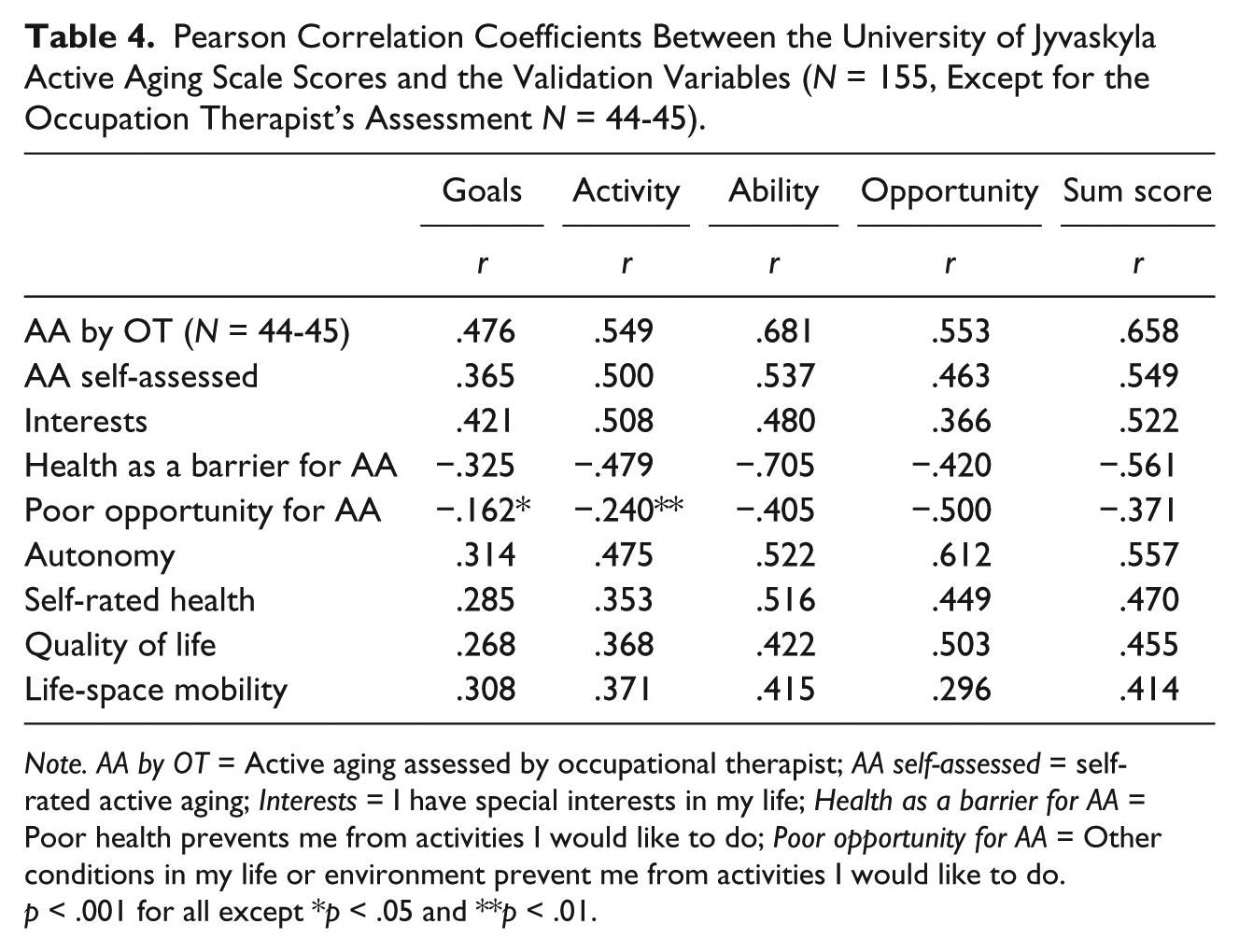
Note. AA by OT = Active aging assessed by occupational therapist; AA self-assessed = self-rated active aging; Interests = I have special interests in my life; Health as a barrier for AA = Poor health prevents me from activities I would like to do; Poor opportunity for AA = Other conditions in my life or environment prevent me from activities I would like to do.
p < .001 for all except *p < .05 and **p < .01.
Focus Group Interviews
The focus group members were aged 60 to 84 years and included both men and women. The meetings were held at the Gerontology Research Center where the participants arrived independently. The focus groups considered the 15 items in the pilot scale to be relevant for their life. The most important concern raised by focus group members was social desirability in responses. In the pilot scale, the frequency of performing the activity was the first question asked. The participants felt that they were expected to engage in all the activities to a high degree. The respondents emphasized that the relevance of one’s own goals should be the starting point, and that engaging in different activities as much as they found personally satisfying should be sufficient. Based on this feedback, we revised the order of the dimensions so that the first question concerned the goal dimension. Finally, based on the focus group comments on what was felt to be missing from the scale, we added two new items related to the hobbies in the scale, as these were considered essential for active aging (see Table 2). The focus groups also suggested including an item about nutrition, but we decided against this, as the pilot study had shown low variability in the item and led to its rejection.
Test–Retest Repeatability
The final version of the UJACAS comprised 17 items each with four dimensions. The total score ranges from 0 to 272, with higher scores indicating more active aging. For the test–retest study, a convenience sample of 67 respondents answered the questions twice approximately 2 weeks apart. The participants were 65 to 86 years old (mean age 72.9 years, SD, 5.6); 82% were women and 83% reported no difficulty walking a distance of 2 km. The means and intra-class correlations for the test–retest analyses are shown in Table 5. The smallest potential value for all subscales is 0 and the highest 68. For the total score, the corresponding limits are 0 and 272, respectively. The responses showed no apparent clustering toward minimum or maximum values, except for the ability dimension where 12 people (17%) received the maximum score. However, floor and ceiling effects were not observed for the total score. The intra-class correlation coefficients between the two surveys carried out approximately 2 weeks apart were high for all sub-scores and the total score (for all ICC > .886, p < .001), and the results for men and women were practically parallel. The kappa coefficient was computed for each individual item and indicated that the agreement found over time was significantly greater than by chance; kappa coefficients were >.21 for each item in the subscales goals (.21-.62), ability (.24-.80), and activity (.24-.61). For the opportunity subscale, the kappa coefficients ranged from .17 and .60, but the item on societal matters had agreement equal to chance (kappa = .057).
Means and Standard Deviations of University of Jyvaskyla Active Aging Subscale Cores and Total Score at First (T1) and Second (T2) Assessments. ICC Coefficients Between the Assessments (N = 68).
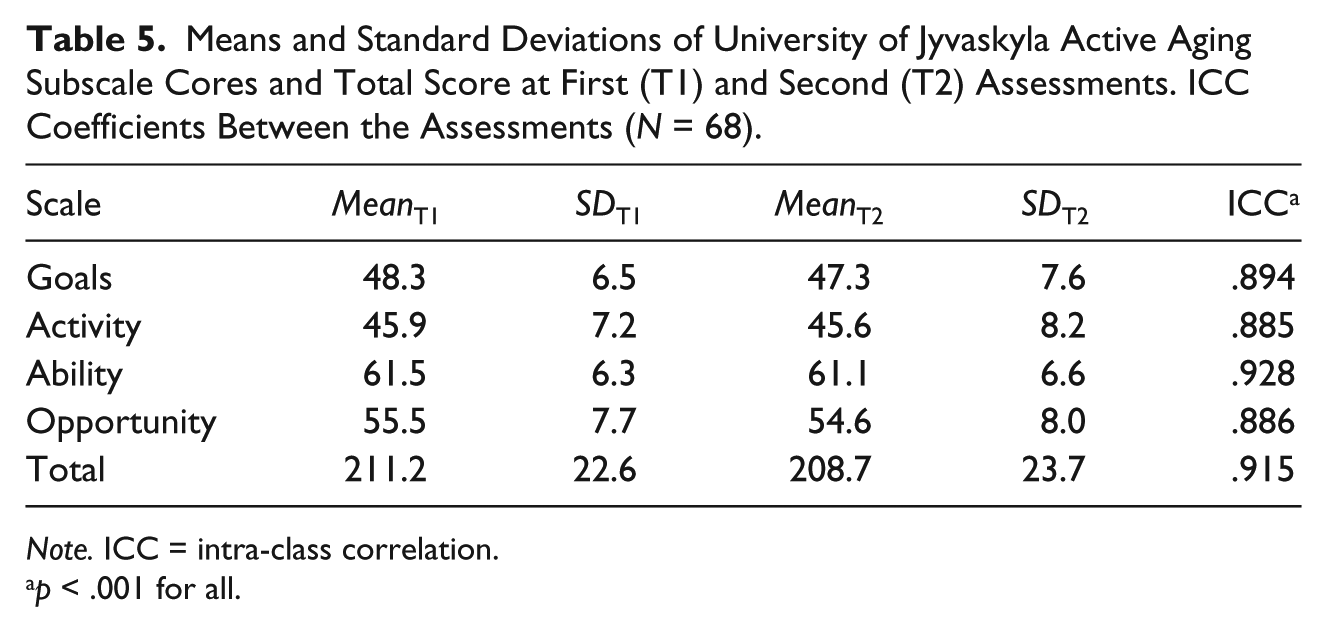
Note. ICC = intra-class correlation.
p < .001 for all.
Discussion
We have developed a novel scale to assess active aging from the point of view of older individuals that can be used in research or practice. The crucial difference between this and previous studies arises from the realization that before we can assess the active aging of individuals, we need to define what active aging entails. We defined active aging at the level of the individual as the striving for elements of well-being through activities relating to a person’s goals, functional capacities, and opportunities. The UJACAS questionnaire comprises 17 items each of which is assessed for four sides yielding four sub-scores. The minimum total score is 0 and the maximum 272. UJACAS can be administered as a questionnaire or as an interview, and both the sub-scores and total score are valid and reliable. The item analyses showed that the UJACAS sub-scores capture an underlying single construct that reflects active aging and that the total score describes active aging in a condensed form and reflects a unilateral construct. We are not aware of any earlier scales that have been developed by applying an approach corresponding to that of the UJACAS.
We consider that what the older people truly want to do is essential for active aging. Most of the earlier scales related to aspects of active aging have simply addressed the ability of people to do different activities (e.g., Kempen, Miedema, Ormel, & Molenaar, 1996; Saito, Izawa, Omori, & Watanabe, 2016) while some have also addressed the actual activities done (e.g., Jette, Haley, Ni, Olarsch, & Moed, 2008) or autonomy in life situations (Wilkie, Peat, Thomas, Hooper, & Croft, 2005). However, knowledge of what older people’s goals are remains unclear in these cases. Goals inspire people to act according to those goals (Ryan & Deci, 2000) and may help older people to maintain the activities that they value most (Baltes, 1997), even in the face of functional decline. Research has indicated that goal pursuit relates to higher activity participation in terms of engagement in physical activity and higher life-space mobility (Saajanaho, Rantakokko, et al., 2015; Saajanaho, Viljanen, et al., 2014) Therefore, it is presumable that goal setting is a primary element also in active aging. Knowledge about people’s goals allows for analysis of potential congruence or discrepancy between goals and activities performed or between goals and the ability or opportunity to realize them. In the future, UJACAS will enable analysis of what people actually wish to do and what they actually do, and what they are able or have the have opportunity to do, thus providing a more comprehensive picture of active aging.
Developing the scale was a multifaceted process in which we placed high importance on participant feedback and on quantitatively analyzing item properties. We started with a draft scale produced by an expert panel, collected a pilot dataset for item response analyses and for testing validity, conducted two focus group discussions, and tested the scale’s reliability in a test–retest study. Consequently, the number of items in the pilot study version of the UJACAS and the test–retest study of UJACAS differ, and for some items, wording differed across the different study phases. In sum, we believe that the validity analysis conducted in the pilot sample is reliable. It is possible that the score distributions in the pilot sample were slightly truncated as the pilot sample included rather high functioning and highly educated people. Consequently, the correlations may be underestimates rather than overestimates of the associations of the UJACAS scores with the indicators of activity and well-being, suggesting that had there been more variability, the correlations might have been higher. Nevertheless, all the indicators of validity and reliability are good.
User involvement in aging research has been emphasized for more than two decades and has gradually become increasingly prevalent (Walker, 2007). Its benefits of it are, first of all, that older people, as is their right, are able to influence the research that is being conducted on them. Second, the chance of producing findings of relevance for the well-being of older people is likely to be higher if they have been invited to contribute their own understandings of the issue. However, in the final scale, we did not include an item they frequently brought up, that is, eating and nutrition. The item was included in the pilot study, where the item analysis showed that practically all the respondents selected the highest response option, and thus the variable did not contribute to scale variability. In this case, participants’ views and the item analysis pointed in opposite directions regarding the inclusion of the item in the UJACAS scale. Overall, the content of the scale was perceived essential for meeting its objectives and the questionnaire was considered acceptable. Participant burden was perceived reasonable with interviews taking from 10 to 25 min in most cases.
The scale is intended to be used among older people able to respond independently and is not limited to a specific segment of the older population. We have successfully interviewed people ranging from residents of an assisted living facility to very vigorous community-living older people. We set the recall period for 4 weeks so that it would be long enough to smooth out possible exceptional situations during the previous week, such as unusual weather conditions, sickness, travel, or a visit. The scale discriminates between more and less active respondents. The validation analyses suggest that higher scores are more favorable than lower scores, but whether the scores have a linear or, for example, a curved association with the indicators of well-being remains to be investigated.
Study Limitations
As part of the multifaceted study process, two different convenience samples of older people were recruited. Convenience samples are nonprobability samples that may not fully represent the characteristics of their age peers in the population. We recruited the participants from different sources to guarantee variability in terms of active aging. When studying the associations between variables, it is more important to have a broad range of responses than sample representativeness. We report mean values only for the final 17-item UJACAS, which was used in the test–retest study. The test–retest study participants were relatively young (average age 73 years) and high functioning with 83% having no difficulty even in an advanced mobility task. We believe that the reported means are therefore rather high and need to be confirmed by a future study among a representative sample of older people. However, we do not believe that this essentially influenced the reliability as evaluated by test–retest intra-class correlations. Consequently, reference values for the UJACAS scores are not yet available and future studies will be needed to produce them. The individual items of the UJACAS may not be fully reliable when used separately; however, absolute agreement is typically not expected for individual items of a scale. The lower end of kappa coefficients observed for individual items except one was .21, which indicates fair agreement, whereas the higher end observed (.80) suggests a strong agreement (Landis & Koch, 1977). It is also worth noting that the more categories the items have, the lower the kappa values tend to be. The sub-scores and total score showed high test–retest agreement and indicate that overall active aging can be reliably assessed. Another potential limitation of the UJACAS is its unknown cultural generalizability. We consider the scale to be generalizable to the Northern European and other Western countries. Although the items are rather universal and even have some similarities with the previous scale developed in Thailand (Thanakwang et al., 2014), the scale requires validation when used in a different cultural or societal context.
The strengths of the study are the definition of active aging at the level of the individual that was used as the foundation for its development, the novelty of developing a scale for assessing active aging as a quantifiable construct, the item response analyses, and the participant involvement. Participant burden in responding to the UJACAS was rather low and the focus groups suggested that the clarity of the items was good or acceptable. Finally, an important strength of this study is its potential for regenerating the study of active aging, which has thus far been hindered by the lack of a valid method of assessment.
The UJACAS may expand the epidemiology of aging by introducing active aging as a quantifiable entity that may be either low or high, and thus, it enables the analysis of, for example, individual physical and psychological characteristics as well as environmental and social factors as determinants or modifiers of active aging. In our upcoming cohort study, we plan to assess, for example, whether the four sides of active aging have different predictors, whether active aging changes with age, and whether active aging helps alleviate decline in well-being when people face functional decline and other losses. The UJACAS may be used to monitor changes and to evaluate the effectiveness of different interventions and technological solutions in promoting active aging. Eventually, the UJACAS may be used for the evaluation of implementation research and policy formulation. The UJACAS is available at www.gerec.fi/en/agnes/ujacas.
Footnotes
Acknowledgements
We wish to thank Dr. Timo Hinrichs for his contribution to the drafting phase of the scale.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by the European Research Council (ERC Advanced Grant 693045 to TR).