
Abstract
Keywords
Introduction
Death, defined as the loss of vital functions, is a universal fact and an inevitable phenomenon experienced by all living things (Nowak, 2023). Individuals attribute certain meanings to the phenomenon of death, which is not easy to define. The meaning attributed to death varies depending on the individual's beliefs, traditions, and social environment (Hsu et al., 2009; Visser, 2019). Death is an annihilation for some, but for others it is the beginning of an immortal life (Testoni et al., 2015). It is sometimes reincarnation, the transformation of the body, which is thought to reduce death anxiety (Isami & Isami, 2023). Being aware of the fact that one is a being that has to die affects the person profoundly (Cohen, 2022). On the other hand, confronting the reality of death creates anxiety in the individual but can also be a reason that connects the individual to life and gives meaning to one's existence (Sköld, 2021). An individual who is aware of the reality of death can live one's life more meaningfully and with pleasure, and an individual who accepts this reality can move from a fearful and pessimistic mood to a life in which one can realize his/her values (Spitzenstätter & Schnell, 2022). Therefore, talking to patients in palliative care units, who are often expected to die, about death can help them understand their feelings and help them feel better (Collins et al., 2018). Given the deep personal and cultural meanings attached to death, addressing this reality within nursing practice requires an integrative approach that goes beyond physical care (Hsu et al., 2009).
Holistic nursing is a philosophy and practice that considers the individual as a whole—addressing physical, emotional, social, cultural, and spiritual needs. Especially in palliative care settings, holistic nursing plays a critical role in supporting patients and their families through end-of-life experiences. This approach emphasizes empathy, presence, and meaning-making, aligning closely with the complex needs of individuals facing death (Dossey et al., 2021). Palliative care is a holistic approach that aims to meet the physical, emotional, and spiritual needs of patients at the end of their lives. In this process, nurses meet the basic needs of the patient, such as body care, which helps the patient to cope with the deterioration of the body at the end of his/her life (Marchetti et al., 2023). However, this process can be emotionally challenging for nurses and may pose a risk of burnout (Parola et al., 2018). Confrontation with death can affect nurses’ personal and professional lives. Nurses working in palliative care units may have to re-evaluate their views and emotions about death (Collins et al., 2018; Cura & Ateş, 2020). In addition, frequently encountering death may cause nurses to question their own emotional resilience and professional values (Moran et al., 2021). This may affect nurses’ professional satisfaction and job performance (Parola et al., 2018). In holistic care, where emotional connection is a core component, such experiences may impact nurses’ ability to remain present and compassionate at the bedside. The death of a patient can lead to frustration and despair for nurses providing holistic patient care (Chew et al., 2021).
Nurses working in palliative care units frequently encounter death and this deeply affects their professional and personal lives. Nurses’ attitudes toward death and the associated concepts are important factors affecting the quality of end-of-life care. Determination of nurses’ views and attitudes about these concepts is of great importance for providing quality end-of-life care (Cybulska et al., 2022; Tran, 2020). Nurses’ views on death are affected by personal characteristics such as demographic characteristics, religious beliefs, and professional experiences. All these significantly determine nurses’ attitudes toward death and patient care in the death process (Wang et al., 2018). Delivery of quality care to patients facing death requires the ability to cope with stress and end-of-life knowledge (Harrington et al., 2019). Nurses who cannot accept their mortality may emotionally distance themselves from patients and their families or reflect their fears on patient care. Therefore, understanding nurses’ thoughts about dying patients and death will deepen our evaluations in this area and enable us to provide more effective and holistic health care services, especially in end-of-life care settings.
This study aims to gain an in-depth understanding of nurses’ perceptions of death and end-of-life care, as well as their communication needs. The findings are expected to provide guidance for the development of holistic nursing practices in palliative care. In particular, the study will offer valuable insights for enhancing nurses’ emotional resilience, strengthening communication skills related to death, and promoting patient-centered, multidimensional care approaches. Accordingly, this study seeks to contribute to the advancement of holistic nursing in both research and practice.
Q1: What do nurses think of death? RQ2: How do nurses approach the terminally ill patients’ request to talk about death? RQ3: When and with whom do nurses think they should talk about death? RQ4: What do nurses need to talk about death with terminally ill patients?
Ethical Considerations
This study was approved by the university's Health Sciences Ethics Research Committee (Date/Number: 2023/457). Before data collection, informed consent was taken from participants in line with the Declaration of Helsinki. All participants provided written informed consent prior to enrollment in the study. During the study, the participants were kept anonymous, and a random identification code was assigned to each participant to protect confidentiality (such as P1 and P2).
Method
Design
The study employed a descriptive qualitative design, and traditional content analysis was used as the analytical method, aiming to deeply explore nurses’ perceptions of the concept of death and their experiences in communicating with terminally ill patients (Sandelowski, 2010). A descriptive, exploratory qualitative design and content analysis approach were employed in the study. Qualitative research method involves an inquiry in which the researcher seeks to understand how or why a particular phenomenon has occurred. The researcher acts as a data collection tool (Miller, 2010). Qualitative content analysis involves the subjective interpretation of a text through a systematic coding process to identify themes or patterns (Hsieh & Shannon, 2005).
Procedure
The inclusion criteria for the study population were at least one year of palliative care experience to ensure participants had sufficient experience with end-of-life care, communicating with terminally ill patients, and facing death (Durmuş Sarıkahya et al., 2023). The exclusion criterion was having recently lost a first-degree relative, as studies have shown that personal grief experiences can increase emotional vulnerability and influence individuals’ perspectives on death (Ordu & Yılmaz, 2024). Participants were selected using the snowball sampling technique. In determining the sample size in qualitative research, it is recommended to select people until the interviewees’ statements reach saturation and excessiveness (Polit & Beck, 2004). Data saturation was checked throughout the research and when saturation was achieved, data collection was terminated with 16 participants (n = 16).
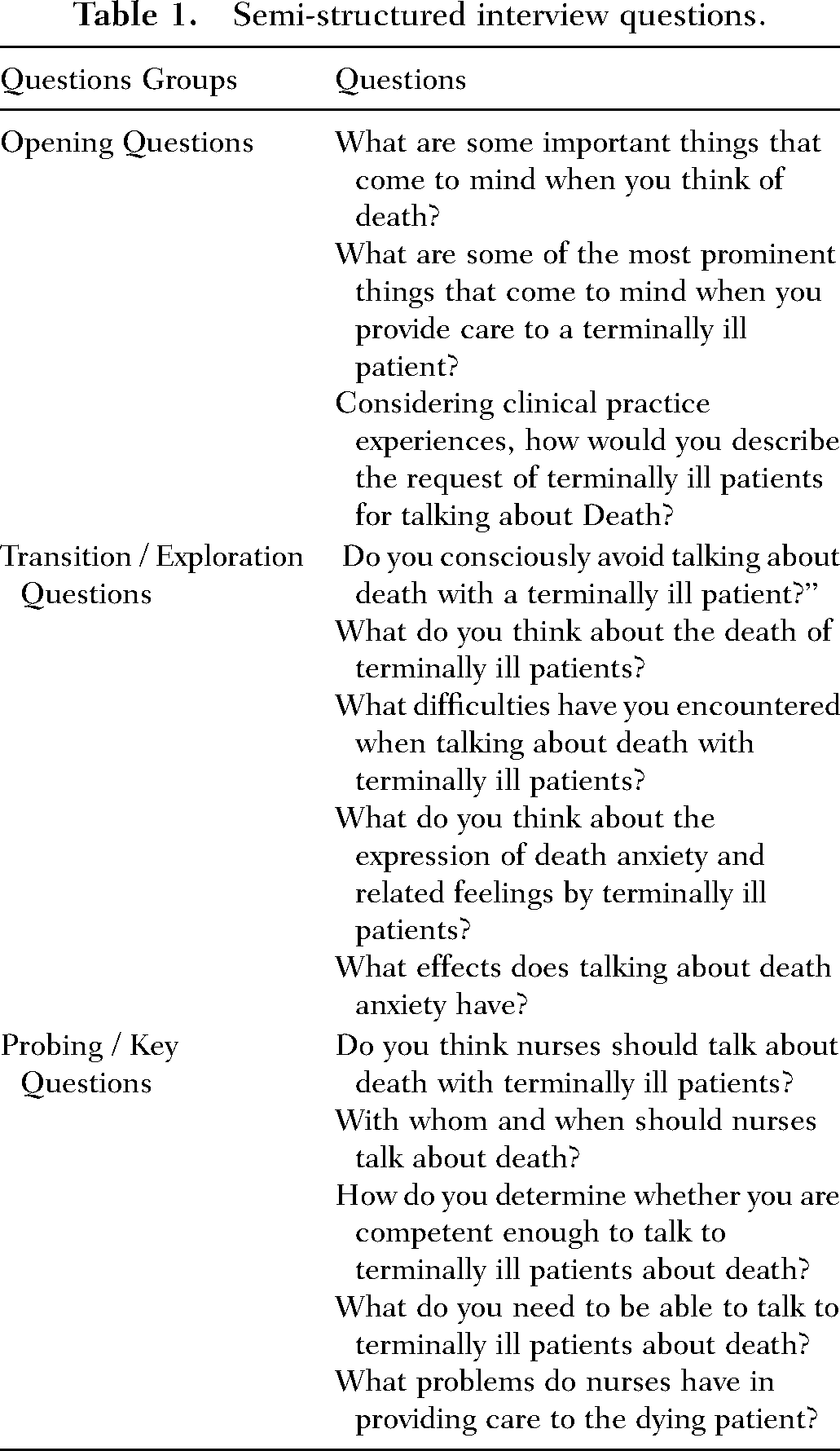
The study was conducted between March and May 2024. The data were collected in the clinic through semi-structured face-to-face interviews. The time of the interviews with the nurses was predetermined. The interviews were conducted in the nurses’ room, which was a suitable area for the interview (no noise, adequate light, and a table and chair suitable for the interview). The age, gender, and educational status of the participant were recorded in the first part of the semi-structured interview form. In addition, each nurse was asked to give themselves a nickname or code. In the second part of the form, general questions about death were asked to the nurses (Table 1). In addition, questions such as “Can you explain this a little more?” or “Can you give an example?” were asked when necessary. The researchers also took field notes during the interviews to record participants’ non-verbal emotions and behaviors. The observer researcher did not intervene in the interview process. Right after the interview, the researcher summarized the data, asked the participant if they had any experiences to add, completed the missing data, and ensured the participant's confirmation. The participants’ interviews were numbered as P1, P2, …, P16. The interviews continued until no further themes emerged and the data were considered sufficient for understanding the participants’ experiences. The interviews, which lasted approximately 30–40 min, were recorded using a digital voice recorder. The resulting data were transcribed without any intervention.
Measures
The data were collected using a “Nurse Information Form” and a “Semi-structured Interview Form” developed by the researchers by reviewing the literature (Bergenholtz et al., 2020; Khalaf et al., 2018; Parola et al., 2018). The Nurse Information Form consists of three questions regarding the sociodemographic data of the nurses, and the Semi-Structured Interview Form consists of 13 open-ended questions regarding the death experiences of nurses working in palliative care units.
Validity and Reliability
One of the most convenient methods to ensure validity and reliability in qualitative research is to thoroughly explain each stage of the research and the methodology followed. It is also known that additional examination of the data by another expert contributes to validity (Denzin & Lincoln, 2008). The interviews were conducted by a researcher with a PhD in Nursing, who has formal training and experience in qualitative research. All interviews were conducted by a single researcher. After the audio recordings were transcribed, three researchers independently checked the accuracy and integrity of the transcription. The participants were informed that the data obtained would be used only for scientific purposes, that their names would not appear anywhere else, and that this study would not create a conflict of interest. During data collection, the participants’ answers were read aloud by the researcher and feedback was provided in the form of “Is this what you wanted to say?” to ensure the participant's confirmation. The records were summarized by the researcher, and if the participant had different experiences that they wanted to mention, they were asked to express them. This explains the credibility of the research. To ensure reliability, the research should be transparently reported and participants and other data sources should be identified (Baltacı, 2019; Connelly, 2016). Continuous and long-term interaction with the data, selection of key information sources, and closer interactions with participants were the strategies used to increase reliability. Two researchers independently reviewed and coded the transcripts. To ensure consistency of coding, the two researchers compared and reviewed the codes, and any disagreements were discussed and a consensus was reached. To enhance reliability, an independent researcher with expertise in qualitative research reviewed the coding scheme and confirmed the consistency and reliability of the findings. This ensured that the results were based on the data rather than the researcher's opinions. In terms of reliability, more than one researcher took part in ensuring the internal validity of the research. The interviews held with the participants were recorded using multiple methods such as audio recording and note-taking. Themes, categories, and sub-categories were created from the raw and analyzed data. These ensure the dependability of the research. The transferability of the research includes how sample selection is made, how results can be generalized, and how they can be transferred to the entire group. In addition, the collective views of the research team were utilized for appropriateness during data analysis. Transferability was ensured by reporting the context and full statements of the participants (Connelly, 2016; Polit & Beck, 2004). In this context, the participants’ answers to the questions were directly quoted and transferred to the findings of the study and themes were created. This creates data for researchers conducting similar studies.
Analysis
The traditional content analysis method proposed by Graneheim and Lundman (2004) was used for data analysis. Content analysis is frequently used in qualitative research (Kyngäs, 2020). In this study, the interview content was transcribed, and the texts were read several times by the researchers to reach a general understanding. The research team then generated initial codes or units of meaning that were categorized according to similarities and differences. Finally, the codes were reviewed and consensus was reached. This continued until the unifying themes emerged from the data. Data analysis was conducted manually by the researchers following the traditional content analysis approach, and MAXQDA 10 (YYY University VERBI Software 10) was used only to assist with data organization and coding (VERBI Software, 2010)
Results
The mean age of the participants was 33.38 ± 6.20 years. Of the participants, 14 were female and two were male. Fourteen had a bachelor's degree in nursing.
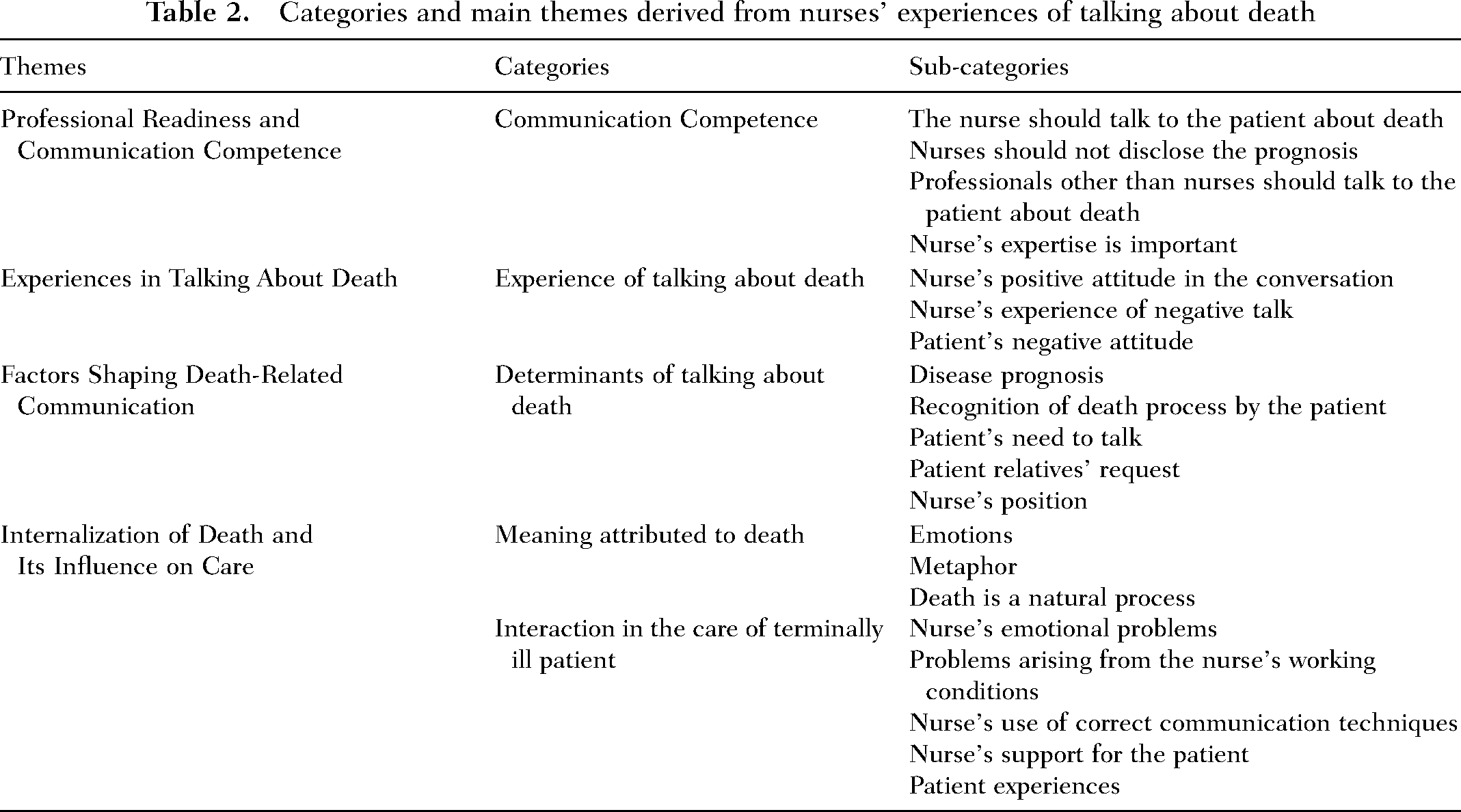
A total of 469 primary codes were obtained. From these, 20 sub-categories, five categories, and two themes were created (Table 2). The themes were “Professional Readiness and Communication Competence,” “Experiences in Talking About Death,” “Factors Shaping Death-Related Communication,” and “Internalization of Death and Its Influence on Care.”
Semi-structured interview questions.
Categories and main themes derived from nurses’ experiences of talking about death
First Theme: Professional Readiness and Communication Competence
The first theme that emerged from the data was qualification, which consisted of the categories of competence, experience of talking about death, and determinants of talking about death.
The Nurse Should Talk to the Patient About Death
Nurses providing care to patients receiving palliative care stated that it was necessary to talk to patients about death. They said that they continuously interacted and communicated with patients and their relatives throughout the day, and therefore, they thought that they should talk to the patient about death. One nurse said, “it is a process that differs according to the patient's demand … if the patient is expecting that …” (P1). Another nurse said, “if the patient brings up the subject, it can be discussed” (P13).
Nurses Should Not Disclose the Prognosis
Nurses often stated that discussing the prognosis of their illness with patients was not within their job descriptions and that they were not responsible for this matter. One nurse (K10) said, “The doctor should talk to the patient; the nurse should definitely not interfere in this matter.” Another nurse (K6) said, “They shouldn't be a burden to the nurses.”
Professionals Other Than Nurses Should Talk to the Patient About Death
In response to the question “Should death be discussed with terminally ill patients?,” it was observed that nurses prioritized being educated on the subject. Nurse P12 said, “Absolutely not. Well-equipped people with psychological training should handle this.” emphasizing psychological counselors and spiritual support staff other than nurses. Nurse P4 said, “There are psychological counselors or spiritual support units. I think it would be more appropriate for them to do have this talk. I think people with more detailed education should do it.” In addition, nurse P1 emphasized that physicians should talk to patients and their relatives about death and said, “I mean, this is a matter of competence. Of course, there is the issue of whether the patient understands or not, and there is also the issue of whether the patient understands or not. It depends on the education level. So, these are different factors. It would be more appropriate for the doctor to have this talk.”
Nurse's Expertise Is Important
Another issue emphasized by nurses in terms of competence was having expertise. The nurses’ ability to be professional and educated was included in this expertise sub-category. One of the nurses (P6) said, “… If they have appropriate education, have effective listening skills, and do not have prejudices, if it will not affect the subsequent treatment, they should talk. … With whom the patient will bond is unknown so that the nurse can talk.” The other (P2) stated “I mean, if the nurse has received education on this subject, they should talk about it. Umm, but if the nurse has no education on this subject, I think they should definitely not talk about it. Umm, I mean, if they are going to talk about it, they can give more broadly, promising information about how to spend the last days of life happier.” It was determined that nurses considered expertise as a competence to talk to patients about death.
Second Theme: Experiences in Talking About Death
Nurse's Positive Attitude in the Conversation
It was determined that the sub-category of nurse's positive attitude was included under the experience of talking about death. At this point, nurses’ expectations about themselves included approaches such as encouraging the patient to talk, consoling them, answering their questions, and promising hope. The nurses’ statements about their experiences of talking were as follows; “Consoling, trying to reduce their pain. These are what we will do in the last period” (P3); ‘… The questions in the patient's mind are cleared, so I tell the patient that this is not the end” (P1); “Psychologically, not only the patient but also the nurse should be ready here. If the patient believes that they can answer the questions discussed, I think they are ready” (P15).
Nurse's Experience of Negative Talk
It was observed that negative emotions were also prominent in the experiences of the nurses participating in the study in talking to patients about death. It was determined that the nurses were especially worried about expressing their thoughts to patients and thought that they could not give adequate answers to the patients’ questions about death and another obstacle was that the nurses did not want to establish a bond with the patient. P8 said, “I listen to the patients’ speeches about death and refrain from making judgmental and emotionally manipulative statements ….” P2 said, “Patients with terminal illnesses are divided into two and there are two extremes at this stage. One of them tries to live more religiously, you know, we can think of it as completing their flaws. They say they haven’t done this or that during their lifetime and try to live more religiously and fulfill their religious obligations. Or they deny God's existence and become rebellious. Both extremes live really sharply, and they don’t have a lot of circular aspects. As I mentioned in the first question, everyone's perspective of death is different, so you have to approach it accordingly. In particular it can be very dangerous to talk to this rebellious group. There are also a lot of people who don’t talk or don’t want to talk.”
Patient's Negative Attitude
It was determined that the patient's negative attitude was effective in nurses’ experience of talking to the patient about death. Especially the patient's inability to cope with the idea of death stood out. In this regard, one of the nurses (P7) said, “As a unit, we provide care to many terminally ill patients. We witness too many deaths. This exhausts us. At the same time, since terminally ill patients can be more bad-tempered and uncooperative, it becomes difficult to provide care, they may not accept it.”
Third Theme: Experiences in Talking About Death
Disease Prognosis
Disease prognosis was included under the sub-category of determinants of talking about death. According to the nurses, the patient's condition was the most important factor for talking to patients about death. In this regard, a nurse (P7) said, “Unfortunately, patients are not able to talk because they usually do not accept death until their last days and their state of consciousness changes.” Another nurse (P8) said, “Patients should be conscious and willing to express their feelings. In addition, it is also related to events such as time, place, suitability when something is called a need.” In addition to all these, the timing of the conversation was also emphasized. In this regard, nurses used the following statements: “A conversation can be made with terminally ill patients. However, if the patient is not ready, this conversation is postponed” (P16), “I think they can talk to the patient's relatives if the patient's hope for treatment and recovery is over, only supportive treatment is given, and it is said that death can occur at any time as a prognosis. Of course, the temperament of the patient's relatives is also very important. If the patient does not request it, it should not be spoken. It is difficult to predict the time, it depends on the patient and family” (P6).
Recognition of Death Process by the Patient
According to our nurses working in the palliative care unit, one of the determinants of talking about death was the patient's awareness that they were in the death process. According to the nurses, the patient's awareness made talking about death easier. The nurse P1 said, “What do I need … the patient needs to be knowledgeable about the disease to talk about it. It is necessary to know what stage the patient is at right now. Is there a treatment for this disease? I mean, we need to know them and talk accordingly.”
Patient's Need to Talk
Nurses agreed that communicating with patients who preferred to express themselves by talking and considered this as a need was a determinant under the theme of qualification. The nurse P15 said, “Yes, because even though they are terminally ill, psychologically, they need to relax and talk,” and P5 said, “We are human beings. We communicate by talking. That's why talking is a need, that's why talking is good,” and emphasized the patient's need to talk.
Patient Relatives’ Request
Patient relatives are undoubtedly as important as the patient in patient care. Nurses also communicate with patients’ relatives for reasons such as the fact that terminal illnesses require prolonged hospitalization and sometimes treatment consent is taken from patients’ relatives or guardians. About talking to patient relatives, a nurse (P2) said, “Since I started working in the palliative care unit, I think of myself as a diary. We write in the diary and relax, and patient relatives spill their feelings to us and relax. They are not really looking for an answer, they just want to talk.” Another nurse (P9) stated, “Umm, first of all, the relatives should be contacted. Umm, I would like to talk when the patient's relatives are not very aware of this process, as far as I have observed.”
Nurse's Position
While the other categories in the determinants of talking about death were associated with the patient, this category was related to how the nurse felt and evaluated her/himself in this conversation. The nurse's approach, wanting to help the patient cope with the fear of death and wanting to provide information on legal issues, in the death process, would help the nurse to determine her competence in the patient's death process. The nurse P6 said, “… If they want to talk, I talk; if they want me to listen, I listen. I avoid guiding them because this is each person's journey, their own experience. It doesn’t feel right to make judgments. However, their need to talk should definitely be met, they should not be ignored. I inform them about the legal issues they are curious about,” and P1 said, “I think that every patient should express themselves. Keeping it to oneself will not solve anything. I think that talking about the facts will also be psychologically relaxing. I mean, I think that talking about death will be beneficial for the patient.” P7 stated that they supported the patient saying, “I think that if the patient has the chance to express their feelings when they talk about death, they will be more accepting and calmer.”
Fourth Theme: Internalization of Death and Its Influence on Care
After the interviews with the nurses working in the palliative care unit, the theme of “Internalization of Death and Its Influence on Care” emerged in line with the categories of “Meaning attributed to death” and “Interaction in the care of terminally ill patient.”
Meaning Attributed to Death
Emotions
It was determined that most of the expressions regarding death included emotions such as fear, regret, incompleteness, loneliness, sadness, and pain. Nurses’ expressions on this subject were as follows: “Loss, feeling of emptiness, missing” (P14), “I recall the unknown after death, unfinished dreams and tasks, and separation from loved ones” (P7), and “I mean, unfortunately, death is a reality that we fear but will live” (P10).
Metaphor
The nurses identified death with concepts such as starting a new journey, liberation, and separation. Nurse P2 said, “Uncertainty, fear, feeling of unreadiness, new journey. All these vary according to how the individual has lived until that age. Umm, everyone's perspective is different ….” Nurse P12 used the expressions “Longing, reunion,” whereas nurse P8 used the expressions “Loneliness, beginning, big event, liberation, pain, loss.”
Death is a Natural Process
The common opinion of the participants in the study was that death is a natural process. It was observed that nurses attributed different meanings to death according to the type of death and the age of the patients. In this regard, a nurse (P9) said, “I mean, if they are my relatives, umm, it would be more difficult to finalize the process. So, I see this process as a natural process rather than making my patients suffer more.” When asked about the things they recalled when death was mentioned, nurse P16 said, “Cancer patient, elderly, traffic accident.” When asked about the difficulties experienced when talking about death with terminally ill patients, the same nurse said, “If it is a young patient, when I come face to face with him/her and when they constantly ask the question, ‘Am I going to die?’”
Interaction in the Care of Terminally Ill Patient
Nurse's Emotional Problems
This category was included in the category of “nursing in the care of terminally ill patient.” The nurses who provided care to terminally ill patients stated that they had to cope with some emotions in this process and that this affected their communication with the patient. Nurse P3 said, “… I am affected because I have an emotional structure.” Nurse P6 explained as, “… Too much empathy can affect our mental state and cause sadness. Not being able to understand the patient or their relatives, not being aware of their sensitivities or misunderstanding them, breaking their hearts is a sad, guilty situation. Trying to be professional but trying to touch emotions, trying to be supportive is exhausting. It is difficult to protect the boundaries. We don’t have a single patient; it is much more exhausting to provide this care to multiple patients every shift. Physical care and treatment is easy, but emotional support is something that exhausts us in the long term and can blunt our emotions or cause extreme despair.”
Problems Arising From the Nurse's Working Conditions
Nurses working in the palliative care unit pointed out that in addition to their current duties and work intensity, their burden increased due to providing care to terminally ill patients which reduced their willingness to work. While stating this, the nurse with the code number P6 said, “The only thing I can do is to be with my patient or their relatives as much as I can be with them as long as they request. Of course, the workload, other patients, working hours, homework balance also limit me, unfortunately, our facilities are limited.” Another nurse (P5) said, “We feel sadness for the dying patient. The more we provide care, the more the caregivers may feel fatigue, boredom, and a decrease in the desire to work.”
Nurse's Use of Correct Communication Techniques
The use of correct communication techniques is very important for nurses and this was emphasized by almost all participants. Empathizing, keeping calm, trying to be professional, and effectively communicating were behaviors that nurses paid attention to when talking to a terminally ill patient. Nurse P1 said, “When providing care to a terminally ill patient, I approach the patient with empathy, I don’t apply anything to the patient that I don’t want to be done to me. I want to answer this question as empathy.” While the participant P10 answered, “First of all, the tone and style of speech is very important. The nurse should speak in a tone that can relax them, calm them down, and make them feel safe. The sense of empathy should be high. In other words, they should speak as if they understand the patient, not as if they feel sorry for the patient, but as if they understand.”
Nurse's Support for the Patient
It was determined that the participants not only practiced nursing practices while providing care to the terminally ill patients but also tried to facilitate the process by supporting them in all aspects. Nurse P2 said, “Letting them go peacefully, painlessly, and happily makes me feel peaceful” and nurse P6 said, “I wonder if they are in pain. A physical or mental pain. Can I do something to ease this pain? What is it like to be so close to death? How brave should I be when I communicate? Would I upset my patient?”
Patient Experiences
It was determined that some of the experiences of patients during hospitalization such as being left alone by relatives or the patient's beliefs were effective in nurses’ internalization of death. A nurse (P8) who used expressions such as “patient relatives, unconsciousness of patient relatives, unwillingness of patients, patients’ abdication, abandonment by relatives” demonstrated the effect of patient experiences on the extent of nurses’ interaction in the care of terminally ill patients.
Discussion
In this study, the perceptions of nurses working in palliative clinics about the concept of death and their experiences in communicating with terminally ill patients were explored. The findings revealed the “Professional Readiness and Communication Competence,” “Experiences in Talking About Death,” “Factors Shaping Death-Related Communication,” and “Internalization of Death and Its Influence on Care.” It was seen that the qualification of nurses in talking about death was shaped by multiple factors such as their level of competence, their experience of talking about death, the attitudes of patients and their relatives, disease prognosis, and communication needs. Some nurses emphasized that it was important to talk about death depending on patient demand, while others stated that this responsibility should belong to psychological counselors or doctors. Alshammari, Sim, Lapkin, and McErlean (2023) conducted a study with nurses working in a palliative unit and reported that nurses had negative attitudes about talking to patients and their families about death and managing their emotions. Many nurses believe that terminally ill patients should be informed about their prognosis. Such awareness can help patients to face their condition and make informed decisions about their care (Kyota & Kanda, 2019; Marván et al., 2017). Although they believed that death should be discussed with patients, they pointed out that they were not authorized to do so and that they did not feel educated about talking about death with patients. Some studies in the literature support this finding (Üzar-Özçetin et al., 2021). Many nurses, including recent graduates, feel that they are not well-prepared for end-of-life care, demonstrating a lack of educational preparation during their education. Although palliative care is included in the nursing curriculum, it is recognized that there is a need for more comprehensive education on how to effectively communicate with patients and their families about death (Croxon et al., 2018; Zartaloudi et al., 2021; Zheng et al., 2016). In the literature, it has been observed that a significant number of nurses did not feel well prepared to manage problems related to death, even if they had received a certain level of education (Ay & Öz, 2019; Zartaloudi et al., 2021). This suggests that the current educational curricula remain insufficient to provide the skills needed in the care of terminally ill patients and provide sufficient confidence.
The nurses who participated in the study stated that death-related conversations should only take place when they felt ready and believed that they were adequate to answer the patient's questions. However, it was observed that negative emotions were significantly prominent in the conversations nurses had with patients about death. In particular, they expressed that they were hesitant to express their thoughts to patients and that they were worried about not being able to give adequate answers to questions about death. It was stated that nurses often experienced negative feelings toward death and generally avoided complex issues due to pre-acquired negative thoughts about death (Puente-Fernández et al., 2020). Lack of emotional preparedness hinders nurses from talking to terminally ill patients about death and makes them feel unprepared to manage such conversations. This can lead many nurses to avoid death topics (Meller et al., 2019; Zartaloudi et al., 2021). These findings suggest that nurses have difficulty in communicating with patients about death and terminal illnesses due to lack of knowledge and emotional preparation.
Patients’ ability to cope with death differs considerably and is influenced by personal, psychological, and social factors. Some patients reach a positive state of acceptance (Littva & Kralova, 2020), others express a wish to die, which may be associated with pain, depression, and anxiety (Wilson et al., 2016). This affects the patient's quality of life. Nurses participating in the study stated that they had difficulty in providing care to patients who could not cope with death. The difficulties that nurses experience when providing care to patients who have difficulty coping with death are often associated with emotional burnout, empathy fatigue, and management of professional boundaries. Such cases not only demonstrate nurses’ fulfillment of the role of providing physical care, but also the need for psychosocial support (Choi & Lee, 2022). In particular, nurses working in palliative care play an important role in alleviating patients’ physical symptoms as well as meeting their emotional, spiritual, and social needs. In this context, it is necessary to support nurses in developing strategies for coping with death, developing resilience, and strengthening communication skills to provide effective care.
Disease prognosis may increase the need to talk about death. In our study, nurses stated that they had difficulty in communicating with patients with severe prognosis, especially due to physical symptoms such as loss of consciousness, but their relatives were more open to talking about death at this stage. In addition, nurses stated that the patient's knowledge about the disease made it easier to talk to the patient about death. In studies, it was determined that patients and their relatives were more open to conversations about death with nurses and helped them prepare for the death process (Collins et al., 2018; Mori et al., 2017). Some patients may avoid talking about death (Bergenholtz et al., 2020). This provides an important opportunity to understand the needs of patients and their relatives and provide them with appropriate support. Clear and empathic communication about death not only allows patients to express themselves but also helps to meet the emotional needs of their relatives. For nurses to be able to communicate effectively in this process requires a comprehensive approach that includes not only technical knowledge and skills, but also competencies such as empathy, listening, and cultural sensitivity.
In the study, nurses agreed that communicating with patients who preferred to express themselves by talking and saw this as a need was a determinant under the qualification theme. Patients’ need to talk about death may show individual differences. While some patients think that talking about death can provide emotional support for themselves and their loved ones (Collins et al., 2018), others may avoid such conversations (Bergenholtz et al., 2020; Mori et al., 2017). In this context, understanding patients’ individual preferences and designing the communication process according to their needs can improve the quality of care. Patients who are willing to express themselves may feel more comfortable in death-related conversations and this process may lead to a better understanding of their fears, expectations, and emotional needs. This can contribute to the emotional preparation of not only the patient but also their loved ones for the death process.
Since nurses encounter death frequently, they tend to deeply question the meaning of death. Some nurses accept that death is a natural part of life, while others feel fear and anxiety about death (Cybulska et al., 2022). In our study, nurses stated that the emotions they thought of when death was mentioned were fear, regret, incompleteness, loneliness, sadness, and pain. Our findings are consistent with the results of the study conducted by Khalaf et al. (2018). As in this study, nurses generally characterize death as a peaceful process (Nakata, 2020). Such emotional reactions of nurses toward death are associated with the fact that they often encounter death and accompany patients due to the nature of their work. For some nurses, questioning the meaning of death can make life and the profession more meaningful, while for others it can be a source of emotional burnout and stress. In this context, it is evident that nurses need safe spaces and professional support mechanisms where they can express their emotions. Considering death a peaceful transition may reflect a positive attitude in nurses’ perspectives. This approach supports nurses’ effort to ensure that patients and their relatives feel comfort and confidence in their final moments. However, it is important to take measures such as regular psychological support, stress management training, and supervision applications to alleviate the emotional burden experienced by nurses in this process.
The care of terminally ill patients can be a huge emotional burden for nurses. Nurses need psychological and emotional support when they face death and suffering daily. Nurses working in palliative care units may face problems such as emotional exhaustion and burnout while providing emotional support to patients and their families (Renn–Żurek et al., 2014; Testoni et al., 2018). This emotional burden may negatively affect the job satisfaction and general well-being of nurses. In our study, nurses also stated that providing care to terminally ill patients caused burnout over time. It is extremely important for nurses working in the care of terminally ill patients to have access to training programs and regular psychosocial support to increase their professional resilience. Moreover, a balanced distribution of workload within the team and strengthening supervision mechanisms can help reduce the burnout levels of nurses.
Nurses are healthcare professionals who interact directly with patients, so strengthening their communication skills is crucial. Limited contact with patients and their families receiving palliative care limits opportunities to develop communication skills in the clinical setting. Simulation-based learning experiences can be used to support communication skills (Bearzot et al., 2024; Smith et al., 2018).
This study has several limitations. First, although the inclusion criterion required at least one year of palliative care experience, we did not collect detailed information on participants’ total years of experience or the type and extent of training they received for their roles. The absence of this contextual information may limit the interpretation and transferability of the findings. In addition, the study was conducted with a small sample from a single setting, which may restrict generalizability. Future research should explore how training background, clinical experience, and organizational support influence nurses’ communication practices in end-of-life care.
Conclusion and Recommendations
In this study, the perceptions of nurses working in palliative care clinics about the concept of death and their experiences with terminally ill patients were revealed. The findings showed that nurses’ experiences of talking to patients about death were characterized by their concerns about communicating with patients and their relatives about death, lack of education, psychological burden, and management of professional boundaries. More comprehensive training in palliative care and communication should be included in the curriculum to improve nurses’ ability to effectively communicate with terminally ill patients. Furthermore, communication skills should be strengthened through interdisciplinary training sessions organized with health professionals such as doctors and psychologists in the work environment.
It was observed that the nurses’ level of internalization of death changed their approach to this issue. For some nurses, facing death caused emotional burnout and stress, while for others it was an opportunity to find meaning in life and profession. Negative opinions about the care of terminally ill patients and death caused health professionals to experience great stress and frustration, and as a result, they resorted to avoidance many times. The study showed that nurses’ competencies related to the perception of death and the ability to talk about death should be supported not only by technical knowledge, but also by factors such as empathy, communication skills, and resilience. Practices such as mindfulness, management of empathy fatigue, and self-care should be encouraged to increase nurses’ emotional resilience.
Footnotes
Acknowledgments
We would like to thank all the participants.
Data Availability Statement
The data supporting this study's findings are available from the corresponding author upon reasonable request.
Ethical Approval and Informed Consent Statements
This study was approved by the Necmettin Erbakan University's Health Sciences Ethics Research Committee (Date/Number: 2023/457). Before data collection, informed consent was taken from participants in line with the Declaration of Helsinki. All participants provided written informed consent prior to enrollment in the study. During the study, the participants were kept anonymous, and a random identification code was assigned to each participant to protect confidentiality (such as P1, P2).