
Abstract
Keywords
Introduction
The COVID-19 pandemic has profoundly impacted healthcare systems worldwide, placing extraordinary demands on nursing professionals. Nurses, as frontline caregivers, have faced high exposure to infection, increased workloads, emotional strain, and disruptions in personal and professional life (Falatah, 2021). These cumulative stressors have significantly impacted not only nurses’ physical and emotional health but also their ability to provide holistic, person-centered care. Burnout syndrome—characterized by emotional exhaustion, depersonalization, and a diminished sense of personal accomplishment—represents a critical threat to the well-being of nurses and the therapeutic relationships they sustain with patients (Baatiema et al., 2024; Marković et al., 2024).
Holistic nursing is grounded in the belief that caring for others requires caring for the whole self—body, mind, emotion, spirit, and environment (Ambushe et al., 2023). The nurse is not only a provider of care but also a whole human being whose well-being is integral to healing relationships and safe, compassionate care. Burnout, therefore, is not simply a professional hazard but a disruption in the holistic integrity of the nurse. The American Holistic Nurses Association emphasizes that holistic practice must include efforts to maintain the wellness of nurses, fostering resilience, self-awareness, and self-care practices as essential elements of the profession (Cao et al., 2025; Frisch, 2001; Galanis et al., 2021). Although burnout among nurses has been widely studied, limited research has examined the experience of community-based nurses during the COVID-19 pandemic through a holistic nursing lens (Aguiar et al., 2024; Gonçalves & Matos, 2024). In Portugal, primary healthcare settings such as ACES Grande Porto V—Porto Ocidental played a critical role in managing the pandemic response at the community level. However, little is known about how nurses in these environments coped with pandemic-related stress and whether they experienced burnout, particularly in a way that considers their holistic needs and capacities.
This study aims to assess burnout levels among community nurses during the COVID-19 pandemic and explore relationships between burnout dimensions, work-related stressors, and coping strategies. Framed by Watson's Theory of Human Caring, which emphasizes transpersonal relationships and the wholeness of both the caregiver and the patient, the study contributes to holistic nursing science by identifying how frontline nurses manage internal and external stressors and which strategies may protect their well-being. Ultimately, the findings aim to inform interventions that promote the holistic well-being of nurses and sustain caring-healing environments in primary healthcare.
Theoretical Framework
This study is grounded in Watson's Theory of Human Caring, a seminal framework in holistic nursing that emphasizes the profound interconnection between the nurse and patient, as well as the importance of caring moments in promoting healing and well-being (Curcio et al., 2024). Watson's theory posits that nursing is not merely a set of tasks, but a human-to-human interaction that honors the wholeness of both the caregiver and the care recipient. The core tenets of this theory encompass the promotion of compassion, the fostering of a healing environment, and the acknowledgement of both the physical and spiritual dimensions of health (Ghanbari-Afra et al., 2022).
Key Components as Applied in This Study
Holistic Awareness: Watson's framework underscores that nurses are whole beings whose emotional, mental, and spiritual well-being critically influence the care they provide (Curcio et al., 2024). In the context of the COVID-19 pandemic, the study examines burnout not only as a professional risk but as an erosion of the nurse's holistic health. Recognizing burnout through this lens allows for a deeper understanding of how stressors disrupt the integrative functioning of nurses.
Transpersonal Caring Relationship: Central to Watson's theory is the concept of a transpersonal caring relationship—a profound, authentic connection between nurse and patient that transcends physical care (Delgado-Galeano et al., 2023). This study utilizes the theory to explore how burnout and related stressors may impair nurses’ ability to form these vital caring connections, thereby impacting both their own well-being and patient outcomes.
Caring Moments and the Healing Environment: Watson describes “caring moments” as opportunities for genuine human connection that facilitate healing (Wei & Watson, 2018). By situating the exploration of burnout within this context, the study aims to determine how chronic stress and emotional exhaustion may hinder the establishment of caring moments. Moreover, it examines whether effective coping strategies help maintain a healing environment, thereby contributing to resilience during a crisis.
Implications for Self-Care and Professional Sustainability: Emphasizing the interdependence of self-care and professional performance, Watson's theory reinforces the need for systemic and personal interventions that maintain the nurse's holistic integrity (Bagheri et al., 2023). The study's exploration of coping strategies—such as seeking social support and direct confrontation—serves as an inquiry into how these practices might sustain the holistic well-being of nurses, thus safeguarding the quality of holistic, patient-centered care.
By employing Watson's Theory of Human Caring as a guiding framework, this study not only measures burnout and related stress factors but also interprets these phenomena in the broader context of holistic wellness. The framework supports a dual focus: understanding the adverse effects of burnout on the nurse's overall well-being and identifying holistic strategies that promote resilience, ultimately contributing to the advancement of holistic nursing science and practice.
Materials and Method
Study Design and Participants
This is a quantitative, cross-sectional, descriptive, and correlational study. The target population of this study is nursing professionals from ACES Grande Porto V—Porto Ocidental. Due to the impossibility of accessing all these professionals, a nonprobabilistic sample was used, which, according to Fortin, is a form of selection in which each element of the population does not have an equal probability of being chosen to construct the sample. According to the same author, there are several types of nonprobabilistic samples, which in the present diagnosis were convenience/accidental sampling, formed by individuals who are easily accessible and present in a specific location (Fortin, 2000). A total of 178 nursing professionals were invited to participate, and 75 completed the questionnaire and were included in the final sample.
Inclusion Criteria
Nursing professionals who perform functions at ACES Grande Porto V—Porto Ocidental, Portugal.
Exclusion Criteria
Nursing professionals who refuse to participate in the study and nursing professionals who do not answer at least 80% of the questions in the questionnaire.
Data Collection
Data for this study were collected through an online questionnaire created using Microsoft Forms. This approach facilitated effective, quick, and practical access to participants, who were nurses working at the ACES Grande Porto V—Porto Ocidental. The questionnaire was distributed via institutional email after obtaining the necessary ethical and institutional authorizations.
The questionnaire consisted of three sections:
Sociodemographic and professional characterization, including gender, age, marital status, household composition, educational background, employment contract type, and years of experience, among others; Questions related to working conditions during the COVID-19 pandemic, such as place and schedule of work, role in COVID-19 case management, use of personal protective equipment, and the personal impact of the pandemic; Professional Wear Questionnaire for Nurses—Reduced Version (QDPE-R), validated for use in Portugal. This instrument assesses Burnout Syndrome and associated factors, such as emotional exhaustion, depersonalization, personal accomplishment, coping strategies, and work-related stress factors (Rodrigues, 2017).
Participation was voluntary and anonymous, and informed consent was obtained before accessing the questionnaire. Data collection began following approval from the Ethics Committee, the management of ACES Grande Porto V—Porto Ocidental, and the original author of the QDPE-R instrument.
Research Questions
The following central research questions guided this study:
What is the relationship between the dimensions of Burnout syndrome and work-related stress factors among nursing professionals during the COVID-19 pandemic? What is the relationship between the dimensions of Burnout syndrome and coping strategies among nursing professionals during the COVID-19 pandemic?
Based on these guiding questions, the study aimed to:
Determine the level of Burnout syndrome among nurses at ACES Grande Porto V—Porto Ocidental; Identify the most affected dimensions of Burnout syndrome among these nurses; Analyze the relationship between sociodemographic variables (gender, age, and marital status) and the dimensions of Burnout syndrome; Examine the relationship between professional variables (years of nursing experience, workplace, and number of weekly working hours) and Burnout syndrome dimensions; Explore the association between fear of SARS-CoV-2 infection and Burnout syndrome; Investigate how Burnout dimensions correlate with stress factors such as work overload, contact with death and pain, role ambiguity, and interpersonal conflict; Assess the relationship between Burnout dimensions and coping strategies, including social support, distancing, and direct confrontation.
Ethical Considerations
This study was conducted in full compliance with the ethical standards for research involving human participants. Approval was obtained from the Ethics Committee of the University of Trás-os-Montes e Alto Douro (UTAD) and the management of ACES Grande Porto V—Porto Ocidental prior to data collection. Informed consent was obtained from all participants, who were provided with information about the study's purpose, its voluntary nature, and the procedures involved. Participation was entirely anonymous, and no identifying personal data were collected.
Confidentiality and data protection were maintained throughout the research process. Access to the raw data was restricted to the research team, and all data were securely stored in password-protected files. Participation was voluntary, and no financial or other incentives were offered. Participants retained the right to withdraw from the study at any point without consequence.
Permission to use the QDPE-R was obtained from its original author. The study adhered to the ethical principles outlined in the Declaration of Helsinki and followed all applicable national and institutional guidelines for the protection of human subjects in research.
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences. Descriptive statistics (mean, standard deviation, frequency distribution) were used to summarize participant characteristics. Inferential statistics, including t-tests and ANOVA, were applied to assess differences in stress and anxiety levels across different demographic and professional variables. A significance level of p < .05 was considered statistically significant.
Results
A total of 75 nurses participated in the study. The majority were female (86.7%), married (50.7%), and fell within the 41–50 age group (38.6%; Table 1). Most participants had been working in the nursing profession for over 10 years (91%), performed shift work (68%), and spent more than 50% of their work time in direct patient care (84%).
Working Conditions During the COVID-19 Pandemic Among Community Nurses in Portugal
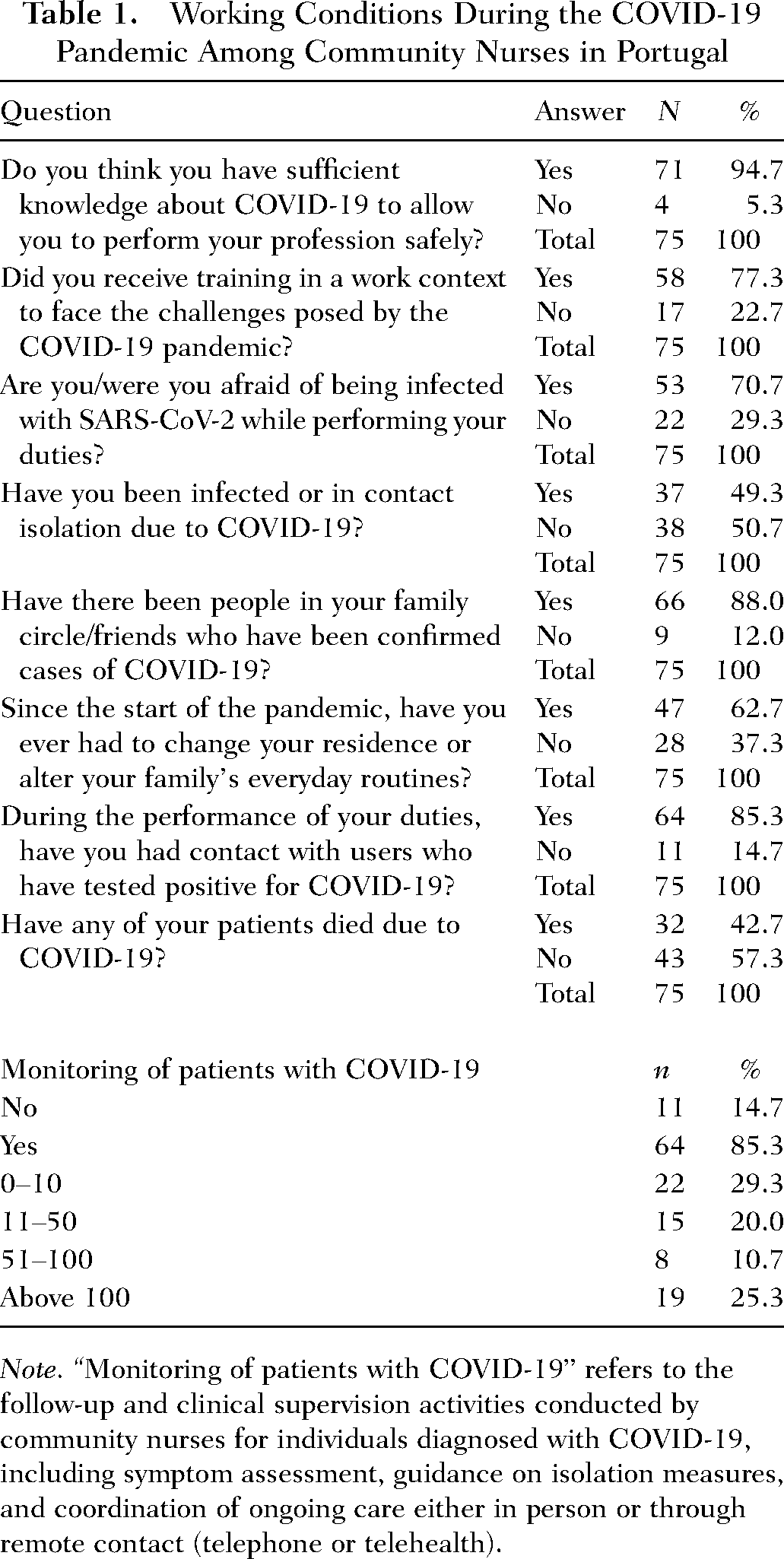
Note. “Monitoring of patients with COVID-19” refers to the follow-up and clinical supervision activities conducted by community nurses for individuals diagnosed with COVID-19, including symptom assessment, guidance on isolation measures, and coordination of ongoing care either in person or through remote contact (telephone or telehealth).
Working Conditions During the COVID-19 Pandemic
Analyzing Part II of this questionnaire, which included the Survey on Working Conditions During the COVID-19 Pandemic, 94.7% of nurses stated that they had sufficient knowledge about COVID-19, which allowed them to perform their profession safely. In this sense, most nurses (77.3%) reported having received in-service training to address the challenges posed by COVID-19. However, 22.7% indicated that they had not received any in-service training to face this new reality. Respondents demonstrated that among the nursing class, there was a fear of being infected with SARS-CoV-2 (70.7%), as 85.3% of nurses had contact with infected patients while performing their duties. Approximately half of the participants (49.3%) tested positive for SARS-CoV-2 or were isolated due to contact. Of the participants (88%), they had family members/friends with COVID-19, which may have caused several constraints and implications in the personal lives of the nurses working at ACES Grande Porto V—Porto Ocidental, namely the change in family routines or even change of residence (62.7%; Table 1). When asked if any of their users had died due to COVID-19, most of the participants answered negatively (57.3%).
Most of the nurses surveyed had been in contact with patients infected with SARS-CoV-2 (85.3%). Of these 64 nurses, 22 (29.3%) had treated 10 or fewer patients with this diagnosis; 15 (20.0%) had treated between 11 and 50 patients; eight (10.7%) had treated between 51 and 100 patients, and nineteen nurses (25,3%) had treated more than 100 patients (Table 1).
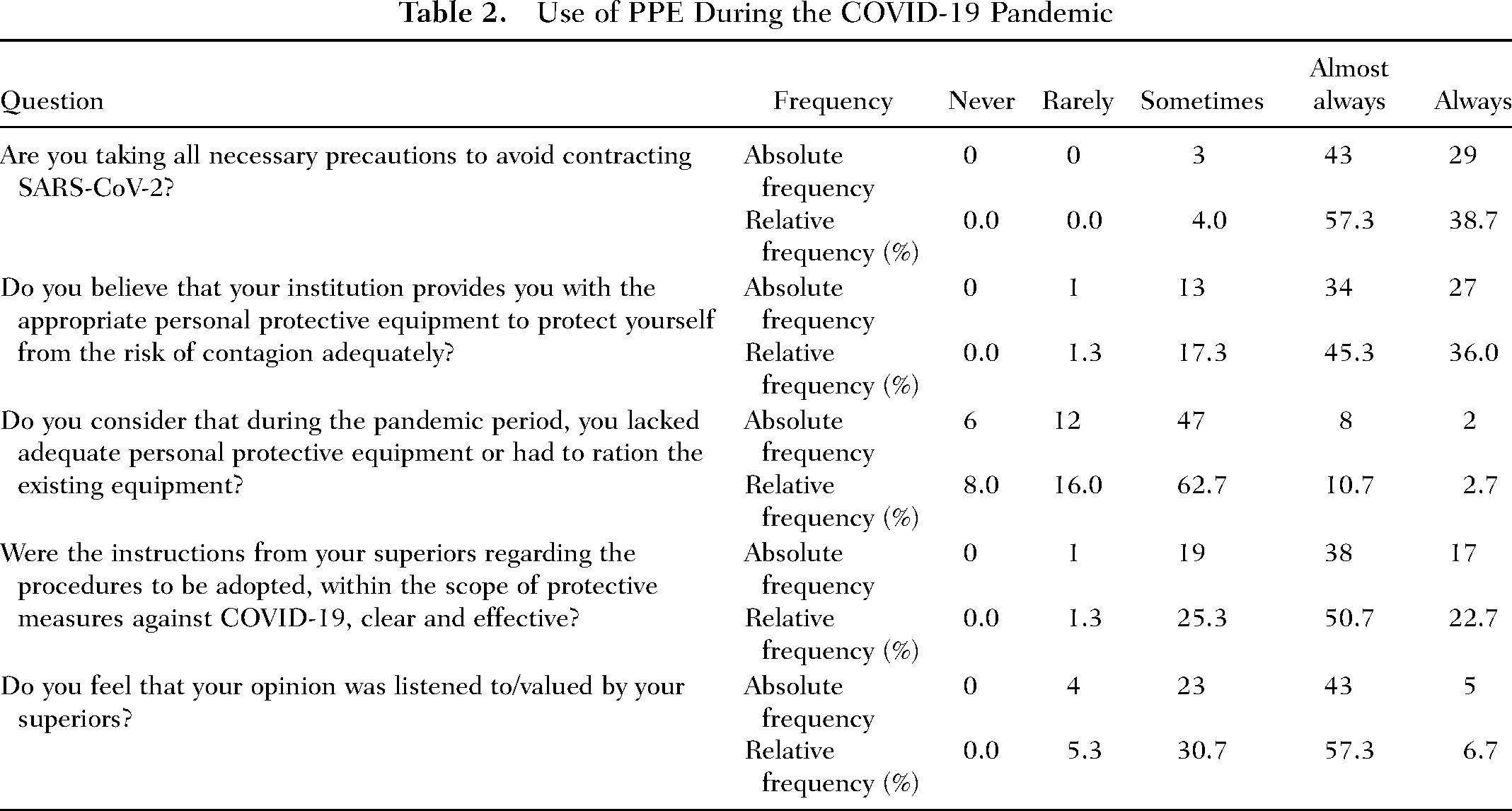
When analyzing the nurses’ opinions regarding the use of personal protective equipment (PPE) and various aspects related to institutional support during the pandemic crisis, it is concluded that 96,0% stated that they had always or almost always taken all necessary precautions to avoid being infected by SARS-CoV-2. Most nurses (81.3%) also considered that the institution (always or almost always) provided them with PPE appropriate for the performance of their duties. However, 62.7% of nurses stated that during the pandemic crisis, there was a lack of adequate personal protective equipment or that it was necessary to ration the existing equipment. Regarding instructions from superiors during the pandemic period, the majority of respondents (73.3%) stated that the instructions were always or almost always clear and compelling. When nurses were asked whether their opinions were valued by their superiors, 30.7% said that their views were only sometimes valued, and 57.3% stated that this happened almost always. Only 6.7% indicated that their opinions were always heard/valued by their superiors, and 5.3% noted that their views were seldom valued by their superiors (Table 2).
Use of PPE During the COVID-19 Pandemic
Burnout Dimensions and Stress Levels
The results from the QDPE-R showed low levels of Burnout syndrome and stress across all its dimensions (Table 3). Among the various stressors, work overload (M = 2.77) and contact with pain and death (M = 3.33) were the most significant. The most reported coping strategies were seeking social support (M = 2.90) and confrontation (M = 2.79).
Results of the QDPE-R Questionnaire
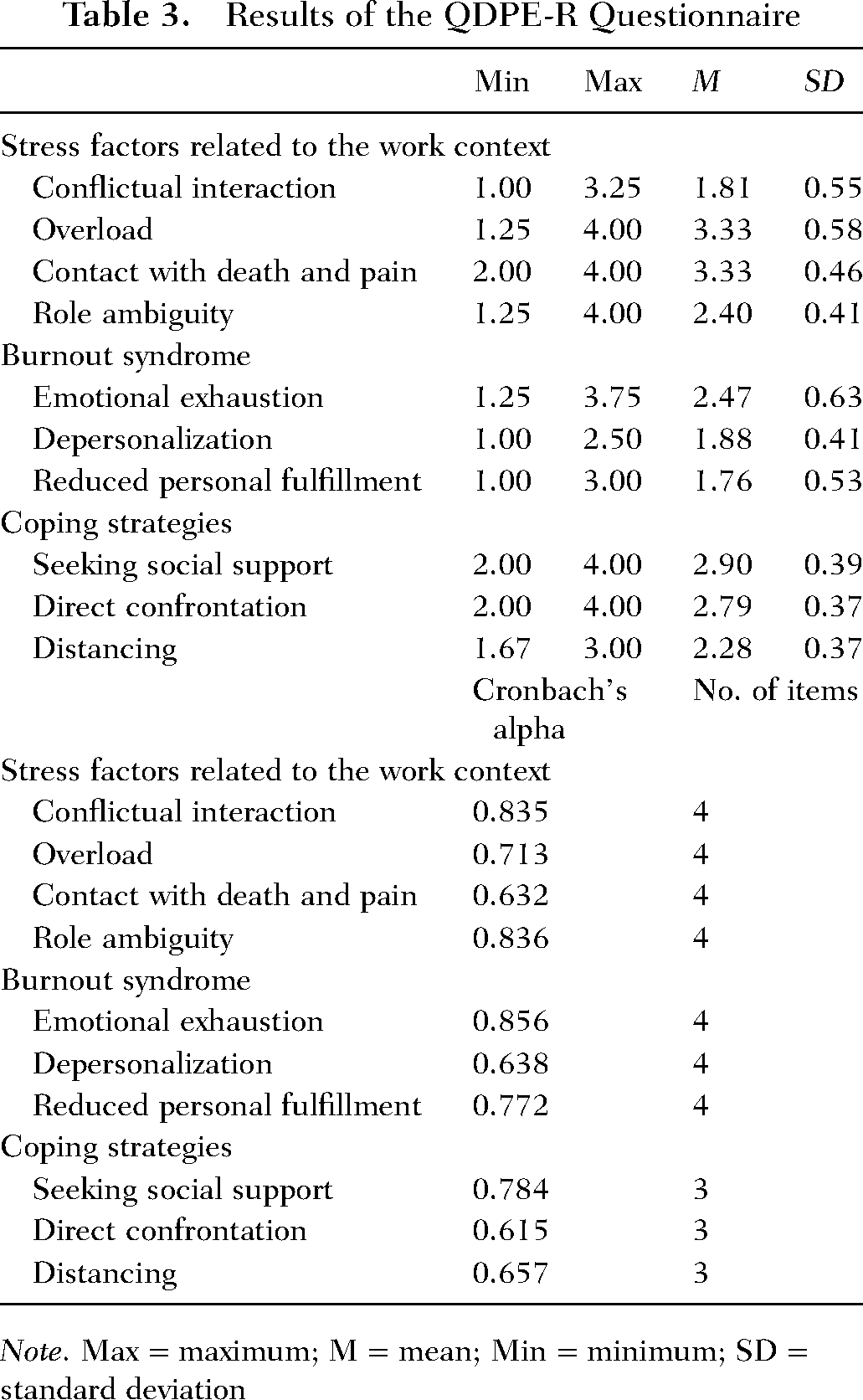
Note. Max = maximum; M = mean; Min = minimum; SD = standard deviation
Internal consistency for the QDPE-R was acceptable, as confirmed by Cronbach's alpha values for each subscale (Table 3).
Although some Cronbach's alpha coefficients were below the conventional threshold of 0.70, these values are considered acceptable for exploratory studies using short, validated subscales. Each subscale of the QDPE-R contains only three to four items, and moderate reliability is common in such brief measures. Furthermore, the coefficients obtained in this study are consistent with those reported in the original Portuguese validation of the QDPE-R (Rodrigues, 2017). As noted by Nunnally and Bernstein (1994) and (R. F. DeVellis, 1991), alpha values between .60 and .70 can be acceptable in exploratory research and early-stage investigations.
Correlations and Associations
No statistically significant associations were found between the sociodemographic variables (gender, age, marital status) and the dimensions of Burnout Syndrome. Similarly, the professional variables (years of experience, weekly working hours, and workplace) did not show significant correlations with burnout (Table 4).
Relationship Between the Sociodemographic and Professional Variables and the Dimensions of Burnout Syndrome
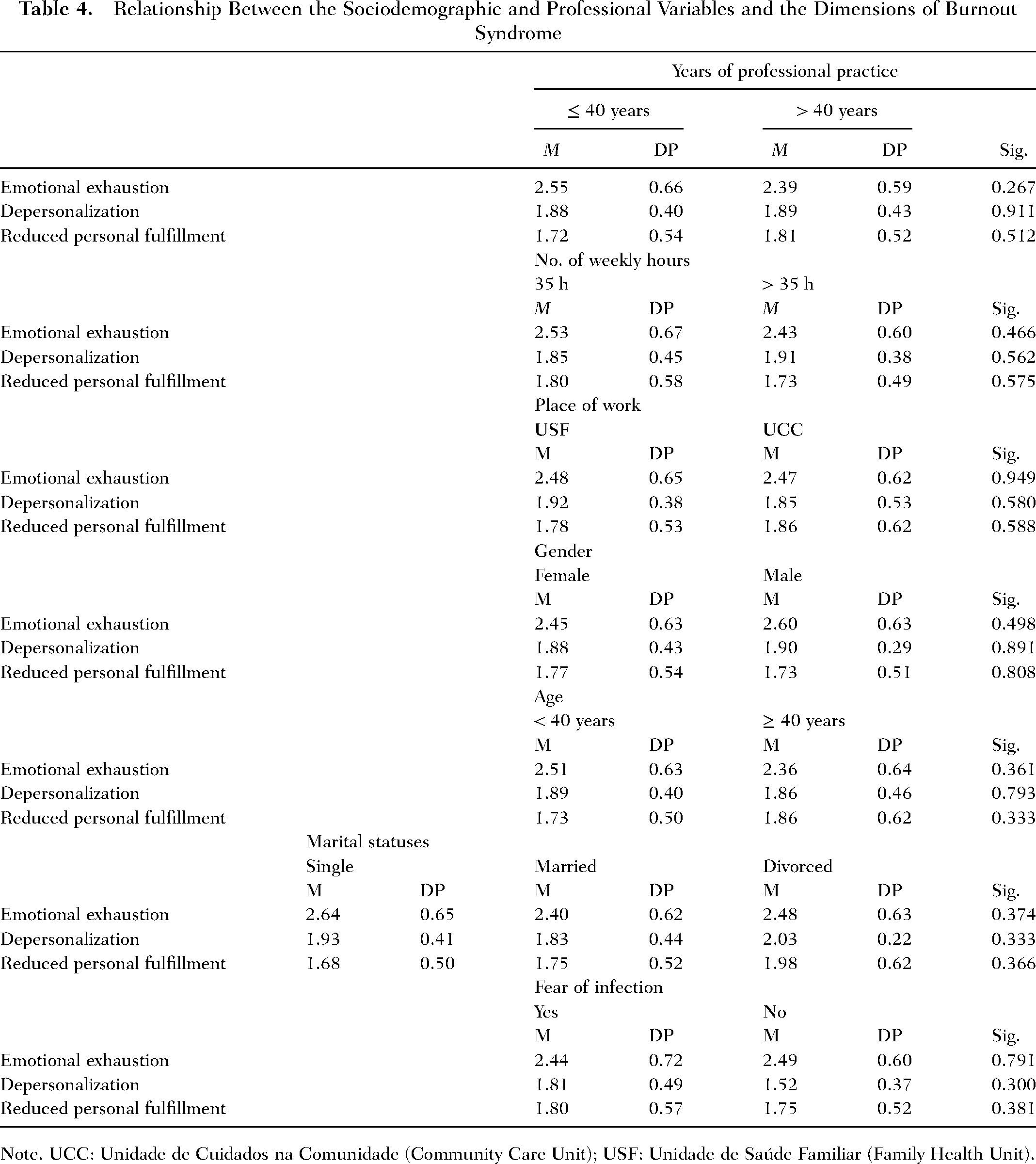
Note. UCC: Unidade de Cuidados na Comunidade (Community Care Unit); USF: Unidade de Saúde Familiar (Family Health Unit).
The results regarding the relationship between the fear of being infected by SARS-CoV-2 and the dimensions of Burnout syndrome are shown in Table 4, showing that nurses who reported fear of being infected had a higher average value in the dimension of Emotional Exhaustion (M = 2.49) and Depersonalization (M = 1.92) compared to those who were not afraid of being infected. Regarding the dimension of Reduced Personal Fulfillment, the average value was higher in nurses who reported not being afraid of being infected by SARS-CoV-2.
The correlation between the dimensions of Burnout syndrome and stress factors related to the work context did not yield statistically significant results (Table 5).
Correlation Between the Dimensions of Burnout Syndrome and Stress Factors Related to the Work Context

Discussion
This study aimed to investigate the prevalence and relationships between burnout syndrome, work-related stress factors, and coping strategies among nursing professionals during the COVID-19 pandemic. The results revealed low levels of burnout across all its dimensions—emotional exhaustion, depersonalization, and reduced personal fulfillment—despite the challenging context of the pandemic (Diogo Gonçalves et al., 2025; Lluch et al., 2022). While participants reported considerable exposure to COVID-19 patients, frequent fear of infection, and disruptions in personal life, these stressors did not translate into statistically significant levels of burnout.
Furthermore, the most prominent stressors identified were contact with death and pain, and work overload, aligning with findings in other literature on healthcare professionals during crises. Nevertheless, the statistical analysis did not reveal significant correlations between stressors and burnout dimensions, which suggests that although nurses perceived these elements as present, they may have employed effective resilience or coping mechanisms that mitigated their psychological impact (Gonçalves & Matos, 2024; National Academies of Sciences et al., 2021).
In terms of coping strategies, the most frequently reported were seeking social support and confrontation, strategies often associated with positive psychological outcomes. However, like stress factors, their correlation with burnout dimensions was not statistically significant. This could indicate that, although these coping strategies were employed, their protective effect against burnout may not have been strong enough to produce measurable outcomes in this sample, or that the sample size limited the ability to detect such effects (Maher et al., 2013).
Contrary to expectations and other studies conducted during the pandemic, no significant associations were found between burnout and sociodemographic (e.g., age, gender, marital status) or professional variables (e.g., years of experience, weekly working hours). These findings may reflect the complexity and multifactorial nature of burnout, which observable external variables may not be able to determine solely (Steffey et al., 2023). They may also indicate the presence of institutional and personal resources that supported nurses’ resilience—such as adequate PPE, clear communication from leadership, emotional and peer support networks, access to training and supervision, as well as personal factors including professional experience, adaptability, and self-care practices.
Overall, the results contribute to a growing body of research suggesting that the impact of pandemic-related stressors on burnout is not uniform and may depend on various contextual and individual resilience factors. The generally low levels of burnout found in this study may reflect successful institutional support, professional experience, or other unmeasured variables such as organizational culture or personal coping resources.
Implications for Holistic Nursing Science and Practice
The findings of this study offer several contributions to the advancement of holistic nursing practice, education, and research, particularly in the context of high-stress public health crises.
Supporting Nurse Resilience Through Holistic Self-Care
The low levels of burnout identified, despite prolonged exposure to stressors, suggest that some community nurses demonstrated significant resilience (Abdulmohdi, 2023). This highlights the importance of promoting self-care practices and inner resources, such as emotional awareness, mindfulness, reflective practice, and spiritual connection—cornerstones of holistic nursing. Institutions should integrate self-care training, peer support programs, and reflective debriefings as standard components of professional development for nurses (Diogo Gonçalves & Matos, 2025).
Informing Holistic Organizational Practices
The pandemic revealed the importance of organizational environments that support the holistic well-being of staff (Errichiello & Pianese, 2021). Strategies such as valuing nurses’ input, ensuring adequate protective resources, and fostering clear and compassionate leadership are consistent with creating a healing and caring work environment. Holistic nursing encourages institutional structures that see nurses not merely as employees, but as whole persons whose work environments must nourish their personal and professional growth (Zamanzadeh et al., 2015).
Shaping Holistic Nursing Education and Policy
Nursing curricula and continuing education should include training in holistic stress management techniques, the use of caring-healing modalities, and the development of emotional intelligence (Ranjbar, 2015). Furthermore, policies at the unit and system levels should embed holistic frameworks into workforce well-being initiatives.
Guiding Future Holistic Nursing Research
This study lays the groundwork for future research into holistic protective factors, such as meaning-making, compassion satisfaction, and spiritual well-being, among nurses in crisis contexts. Mixed-method and longitudinal studies can build upon this work to explore how holistic frameworks can prevent burnout over time and sustain healing relationships in community settings.
In sum, this study emphasizes the value of a holistic approach to nurse well-being, not only for the individual practitioner but also for the integrity of patient care and the sustainability of healthcare systems. Embedding holistic principles into organizational culture and nursing education is vital to nurturing a resilient and compassionate nursing workforce.
Limitations
Several limitations should be considered when interpreting these findings. First, the sample size (n = 75) was relatively small and limited to a single health region (ACES Grande Porto V—Porto Ocidental), which may limit the generalizability of the results. Additionally, the use of a convenience sample introduces potential selection bias, as those experiencing higher burnout may have been less likely to participate.
Second, data collection relied on self-reported measures, which are subject to bias, including social desirability and recall bias. Participants may have underreported psychological distress due to stigma or professional identity concerns.
Third, the cross-sectional design does not permit causal inferences or the examination of temporal dynamics in burnout development. Longitudinal data would be necessary to assess how burnout symptoms evolve over time and in response to interventions.
Finally, although the QDPE-R is a validated and widely used instrument in Portugal, it provides a limited scope on other important psychological variables, such as anxiety, depression, or organizational support, which could further explain the variance in burnout levels.
Future Research
Future studies should consider adopting a longitudinal design to investigate how burnout levels and coping strategies evolve, particularly in response to emerging public health crises. Expanding the sample size and involving diverse healthcare settings would also improve the robustness and generalizability of findings.
Additionally, incorporating qualitative methods, such as interviews or focus groups, could provide richer insight into the subjective experience of stress and coping in nursing practice. This would help capture nuances not easily detected through standardized questionnaires.
Moreover, future research should explore moderating and mediating variables, such as resilience, emotional intelligence, and organizational support structures, to understand what protects some healthcare workers from burnout while others remain vulnerable. The role of institutional interventions, such as mental health support programs or leadership communication, also warrants further evaluation.
Conclusion
This study examined burnout levels, stressors, and coping strategies among community nurses in Portugal during the COVID-19 pandemic, adopting a holistic nursing perspective. Despite the intense pandemic context—characterized by frequent exposure to infection, emotional strain, and disruptions to personal life—nurses reported low levels of burnout and employed primarily positive coping strategies, such as seeking social support and direct confrontation. Although no statistically significant associations were identified between burnout and demographic, professional, or psychological variables, the findings suggest the presence of resilience and possible holistic protective factors within the work environment or personal practices.
Interpreted through Watson's Theory of Human Caring, these results highlight the capacity of nurses to sustain inner balance and maintain caring–healing relationships even in times of crisis. Such resilience underscores the importance of nurturing the holistic integrity of nurses’ bodies, minds, and spirits—as central to preserving the quality of care and the well-being of the caregiver.
Promoting holistic self-care, supportive institutional environments, and reflective practices can help safeguard nurses’ ability to remain present, compassionate, and whole. These findings reinforce the need for continued integration of holistic principles into nursing education, leadership, and workplace culture, and call for further research on interventions that foster holistic resilience among healthcare professionals.
Footnotes
Author's Contribution
MM: conceptualization, methodology, supervision, resources and project administration; SG: writing—original draft and visualization; SG, MJM, and AC: investigation and validation; MJM, AC, SG, and MM: writing—review and editing.
Consent to Participate
Participation was voluntary and anonymous, and informed consent was obtained prior to accessing the questionnaire.
Consent to Publication
Authors grant the publisher the right to publish their work.
Ethical Statement
The study was conducted following ethical guidelines, and approval was obtained from the Ethics Committee of the University of Trás-os-Montes e Alto Douro (Doc102-CE-UTAD-2022). Data confidentiality and anonymity were maintained throughout the research process.
Data Availability Statement
Data supporting the findings and conclusions are available upon request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Patient Consent
Participation was voluntary and anonymous, and informed consent was obtained prior to accessing the questionnaire. Data collection began following approval from the Ethics Committee of the University of Trás-os-Montes e Alto Douro, the management of ACES Grande Porto V—Porto Ocidental, and the original author of the QDPE-R instrument.