
Abstract
Keywords
Introduction
Spirituality is integral to holistic nursing care. As the American Holistic Nurses Association (AHNA) emphasizes, the holistic care process involves the intentional use of presence, authentic communication, and a therapeutic relationship to support the integration of body, mind, emotion, and spirit in healing (AHNA, 2025). Spirituality is viewed as a vital dimension of care, essential to fostering meaning, connection, and wholeness in both patients and practitioners. Research into spirituality and Spiritually Competent Practice continues to evolve (Rogers & Wattis, 2020). Within the nursing literature, references to spirituality span back to the 1950s (Blasdell, 2015), yet there is limited evidence surrounding the integration of spirituality and Spiritually Competent Practice into advanced practice holistic care (DeKoninck et al., 2016).
Advanced practice nursing is described by the International Council of Nurses (ICN) (2020) as an umbrella term often used to include both Nurse Practitioners and Clinical Nurse Specialists. Advanced Practice Nurses (APNs) typically hold a master's degree and can practice autonomously within their scope of practice. APNs’ level of practice requires expert knowledge and utilization of advanced clinical decision-making skills (ICN, 2020). Advanced practice nursing is expanding with role development in 80 countries (Miller et al., 2024). Adynski et al. (2024) suggest that APNs are seen as critical to all aspects of healthcare as they help support universal health coverage and the Sustainable Development Goals (United Nations, 2024). The exact APN role (in terms of definition, expectations, regulation, and scope of practice) varies globally, but shows the contributions APNs make to bridge the gaps in health-care disparities and deliver culturally sensitive, contextually relevant, holistic care to their patients (Miller et al., 2024). APNs can bring together the best of nursing with the best of medicine to provide holistic care by ensuring relationships with patients are based on kindness, compassion, and empathy which supports a deep understanding of a patient's spiritual needs (Collins-McNeil et al., 2015).
Spirituality should not be confused, or conflated, with religion. Chung et al. (2007) suggest that religion relates to specific doctrine or traditions, whereas spirituality connects more to personal values guiding one's identity, purpose, well-being, and relationships. There is a plethora of definitions for spirituality, leading to confusion for many practitioners (Swinton & Pattison, 2010). In the context of holistic nursing, spirituality is defined as “the aspect of humanity that refers to the way individuals seek and express meaning and purpose, and the way they experience connectedness to the moment, to self, to others, to nature, and to the significant or sacred” (Puchalski et al., 2009, p887). Rogers (2021) defines spirituality simply as that which gives us hope, meaning, and purpose. It is as unique as a fingerprint. For some, their faith may be connected to their spirituality, while many find hope, meaning and purpose layered within their work, families, or nature (for example). What is clear about spirituality is that it is an important aspect of healthcare for both patients and practitioners (Wattis et al., 2017), especially when considering simply their shared humanity and the fundamental relational nature of any type of holistic care.
Background and Significance
Within advanced practice nursing, spirituality underpins the holistic nature of the care provided and gives both patients and practitioners a sense of hope, meaning and purpose (Rogers, 2021; Wattis et al., 2017). Chrash et al. (2011) state that APNs should view holistic care in terms of body, mind, and spirit, with Pike et al. (2021) suggesting that these aspects should be integrated into APN competencies. However, incorporating spiritual care into holistic care has been viewed as a sensitive topic (Bergamo & White, 2016), with Younas (2017) finding that spiritual care is often neglected, despite the desire to provide holistic care. If spirituality is not integrated into practice, this may risk an absence of deep interpersonal connections, and patients may receive care that is more mechanized and task-centered rather than individualized, holistic, and person-centered (Wattis et al., 2017).
McSherry and Jamieson (2013) point to many factors which inhibit spirituality from being integrated into practice. For APNs these include a lack of understanding about spirituality (its meaning and relevance both personally and for others), a lack of practical skills to incorporate it into their clinical practice, and for some individuals, a fear of crossing professional boundaries (Carron & Cumbie, 2010). A multinational survey of APNs also found that many did not integrate spirituality into their practice due to a lack of time, while some did not perceive it to be as part of the APN role (DeKoninck et al., 2016). Therefore, while some APNs may have a strong desire to provide holistic care which integrates spirituality, they often feel pushed towards a biomedical approach which often prioritizes diagnosis and treatment (Guillaumie et al., 2019).
To overcome these barriers and enable APNs to provide spiritual care, they need to feel comfortable, prepared, and well equipped to do so (DeKoninck et al., 2016). Rogers (2021) suggests that supervision and reflection can support APNs to understand spirituality and how to integrate spiritual care into practice. Furthermore, both peer-learning from colleagues (Tanyi et al., 2009) and education on spirituality can be used to further support spiritual practice within patient care (Ali et al., 2019). In the United Kingdom, the Scottish Government (2023, p 5), whose work is being recognized globally, state that spiritual care is the bedrock of holistic care which “can empower and benefit both carer and cared for; nurturing the individual to celebrate and flourish during times of joy and growth, supporting people to find strength and comfort during times of transition, uncertainty, and illness.” While this identifies what spiritual care is, needed frameworks and models may specifically help APNs to operationalize spirituality (Carron & Cumbie, 2010; Rogers, 2021; Vincensi, 2019; Wattis et al., 2017). These frameworks focus on a personal understanding of spirituality, in addition to a willingness to build authentic, person-centered relationships with patients. The importance of self-awareness is crucial, as APNs must understand their own beliefs and biases, which if not considered, affects their ability to provide effective spiritual care for others (Vincensi & Solberg, 2017).
One model, the concept of Spiritually Competent Practice was designed as a guide to encourage the integration of spiritual care into healthcare by overcoming the difficulties for practitioners associated with defining spirituality (Wattis et al., 2017). Spiritually Competent Practice is described as the “compassionate engagement with the whole person as a unique human being, in ways which will support them in finding a sense of meaning and purpose, where appropriate connecting or reconnecting with a community where they experience a sense of well-being, addressing suffering and developing coping strategies to improve their quality of life. This includes the practitioner accepting a person's beliefs and values, whether they are religious in foundation or not and practising with cultural competency” (Wattis et al., 2017, p. 3). This definition recognizes that for some individuals, spirituality is linked to religion, and for others not. It also emphasizes the importance of cross-cultural training in order to cultivate greater awareness and competence in working with patients from diverse spiritual backgrounds. Underscoring Spiritually Competent Practice is quite simply yet fundamentally the principle of unconditional acceptance and compassion in the way practitioners engage with and deliver care to patients.
Instrument Description, Reliability, and Scoring Guidance
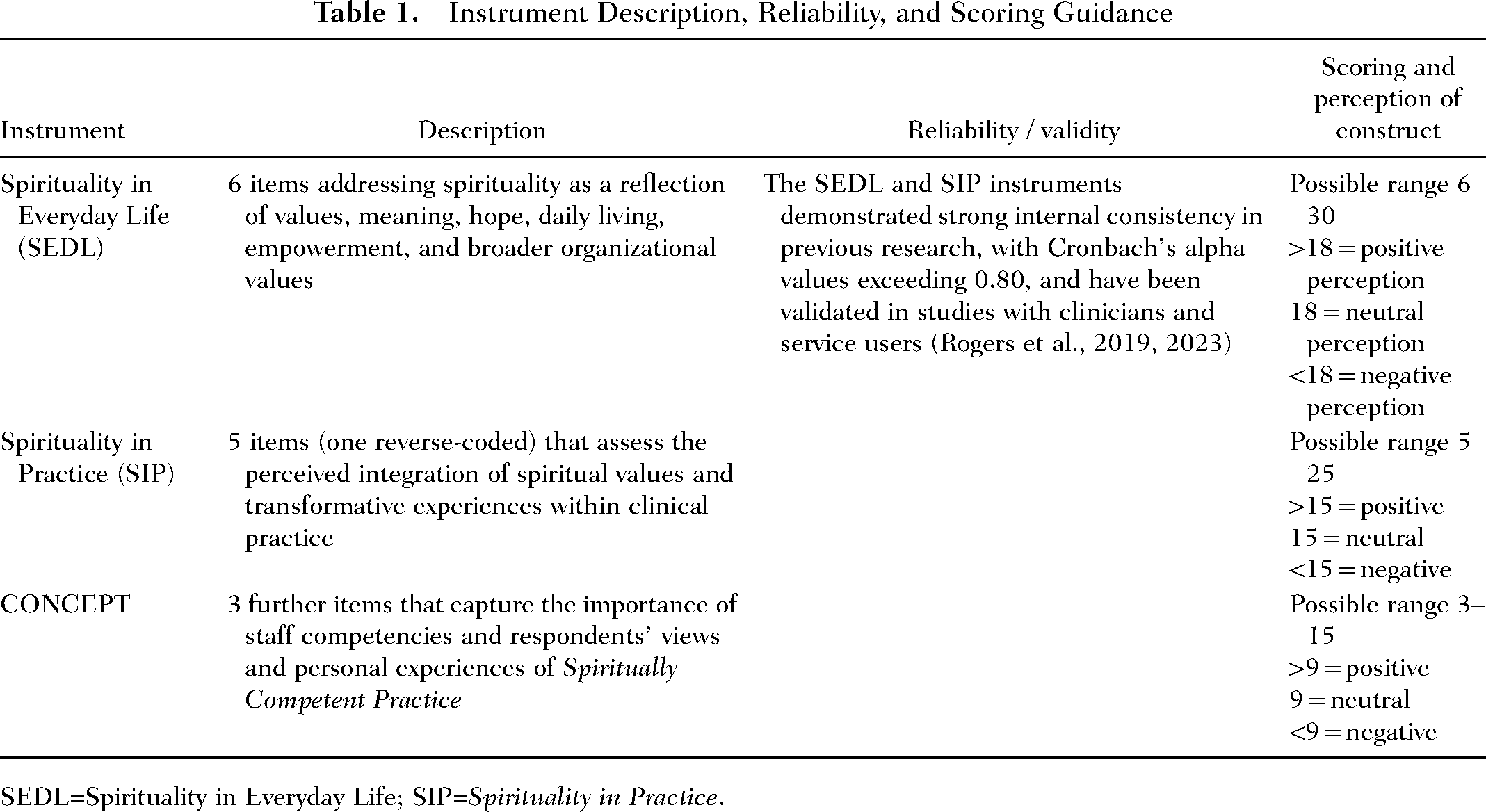
SEDL=Spirituality in Everyday Life; SIP=Spirituality in Practice.
The SEDL domain was measured using an unweighted sum of responses to the following six items:
I believe spirituality is associated with values, ethics, and morals.
I believe spirituality is about finding meaning and purpose.
I believe spirituality is about having a sense of hope.
I believe spirituality concerns the way we live here and now.
I believe spirituality is about liberation and empowerment.
I believe spirituality concerns not only individual but wider organizational values.
The SIP domain was measured using an unweighted sum of responses to the following five items, with reverse coding applied to the starred item:
I believe spiritual values are relevant in health-care delivery.
I believe spirituality is integral to health services and care.
I believe an awareness of spirituality is part of the health-care process.
I believe healthcare given should be a transformative experience.
I believe the intellect is more important than spirituality. *
For the CONCEPT domain, three additional items dealt with respondents’ views and personal experiences of Spiritually Competent Practice, using the same scoring system as the main scales (from 1 point (Strongly Disagree) to 5 points (Strongly Agree)):
Spiritual competencies of staff are an important part of good holistic practice.
Spiritually competent practice is a useful concept which should be integrated into health-care settings.
Spiritually competent practice is understood well by those health-care staff working with me.
The secondary outcome measure Importance of staff competencies and spiritually competent practice as a concept was defined to be the sum of scores obtained on these items, and the guidance is included in Table 1.
Additional items, scored in the same way, elicited factual information or personal opinions. The following item was treated as a “stand-alone” predictor, Integration in practice (INT), rather than an outcome measure, and hence did not contribute to any of the above domains:
I believe spirituality is integrated within the healthcare provided by me.
Responses from the following two items were summed to form an additional predictor variable (with reverse coding applied to the starred item) Distinct [DIS], representing perception of spirituality as a distinct concept from religion:
I believe spirituality can be distinguished from religion
I believe spirituality is associated with a place of worship*
Additional demographic information and job-related information were also captured from respondents including gender; age group; APN role/speciality; years worked as APN; region of primary practice location; ethnicity; highest level of education; and whether or not respondents had a faith, religion, or spirituality.
To address the secondary aim, the summed CONCEPT score was used as an outcome in parallel multiple regression analysis using the same predictor set, in order to explore factors associated with the perceived usefulness of Spiritually Competent Practice as a conceptual model.
Assumptions for regression analysis were verified using standard diagnostics: distributions of primary outcome scores and residuals were checked and standardized residuals were plotted against predicted values. The extent of any relationship between the primary outcomes was assessed.
The secondary outcome measures were also assessed in multiple regression analyses using the same set of predictors as in the multiple analyses of the primary outcomes.
To assess the internal consistency reliability of the SEDL, SIP, and CONCEPT scales, Cronbach's alpha coefficients were calculated.
Results
Sample characteristics are summarized in Table 2.
Descriptive Summary of Sample
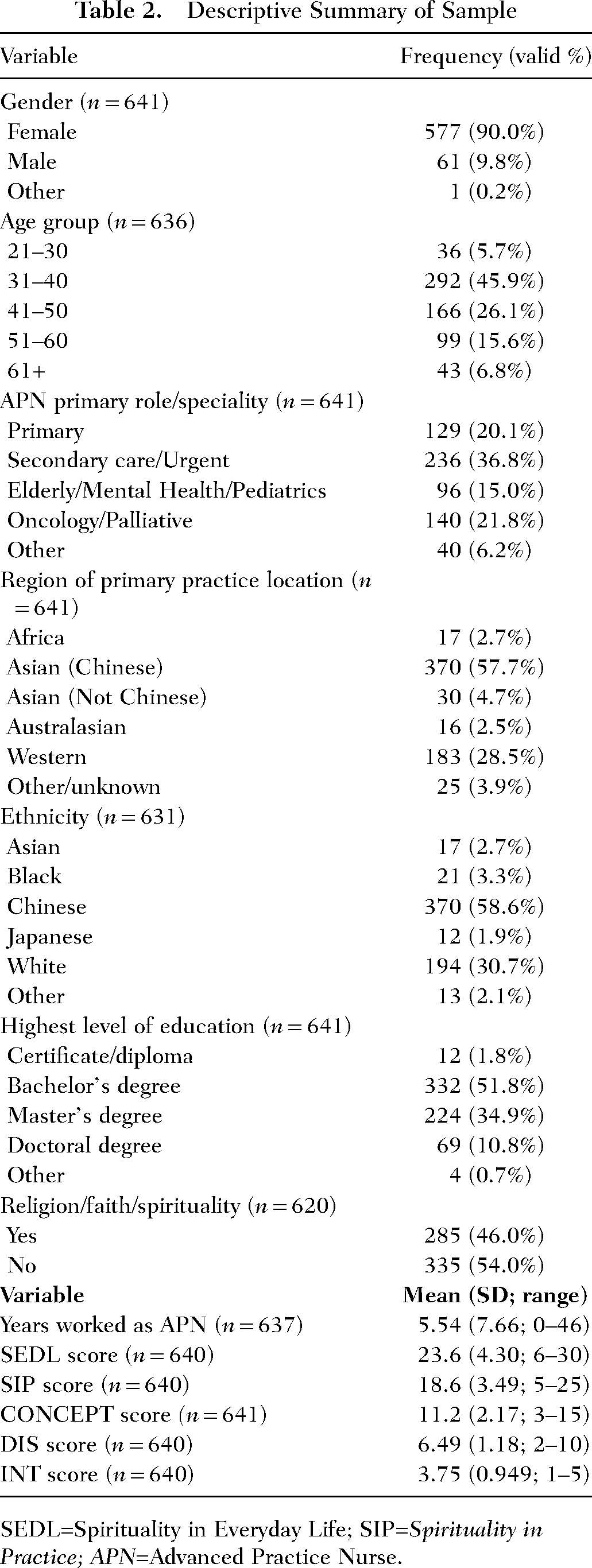
SEDL=Spirituality in Everyday Life; SIP=Spirituality in Practice; APN=Advanced Practice Nurse.
Summary Analysis of Primary Outcome Measures
SEDL and SIP scales both showed good internal consistency with reliability analysis, with alpha values of 0.882 for the SEDL scale and 0.779 for the SIP scales. These levels represented similar levels of reliability to those found in a previous assessment of these measures of 0.864 for the SEDL scale and 0.852 for the SIP scales (Rogers et al., 2023). Analysis after removal of deleted items showed slight reductions or negligible changes in reliability as expected. Therefore no items were removed from either scale, and analysis progressed.
The mean SEDL score reported by respondents was 23.6, representing 3.93 points per constituent item on average. This score approaches the value given to a mean response Agree – i.e., a substantial more favorable than neutral view of the place of SEDL. Respondents used the full range of scores in answering each question. Scores obtained by respondents were very similar to scores obtained from mental health practitioners reported by Ali et al. (2019) and service users (Rogers et al., 2023) in response to a similar set of items.
The mean SIP score reported by respondents was 18.6, representing 3.72 points per constituent item on average. This score approaches the value given to a mean response Agree—i.e., a substantial more favorable than neutral view of the place of SIP. These scores were also very similar to corresponding scores obtained by mental health practitioners reported by Ali et al. (2019) and from service users reported by (Rogers et al., 2023), albeit from a slightly different set of constituent items.
Figure 1 indicates that respondents’ views of SEDL were approximately normally distributed, with most respondents giving generally neutral or slightly positive ratings to this concept. Figure 2 indicates that respondents’ views of SIP were slightly left-skewed, with a minority of respondents considering that it had little or no place, but with a majority considering it to be of substantive value. Respondents used almost the full range of scores in answering each question.
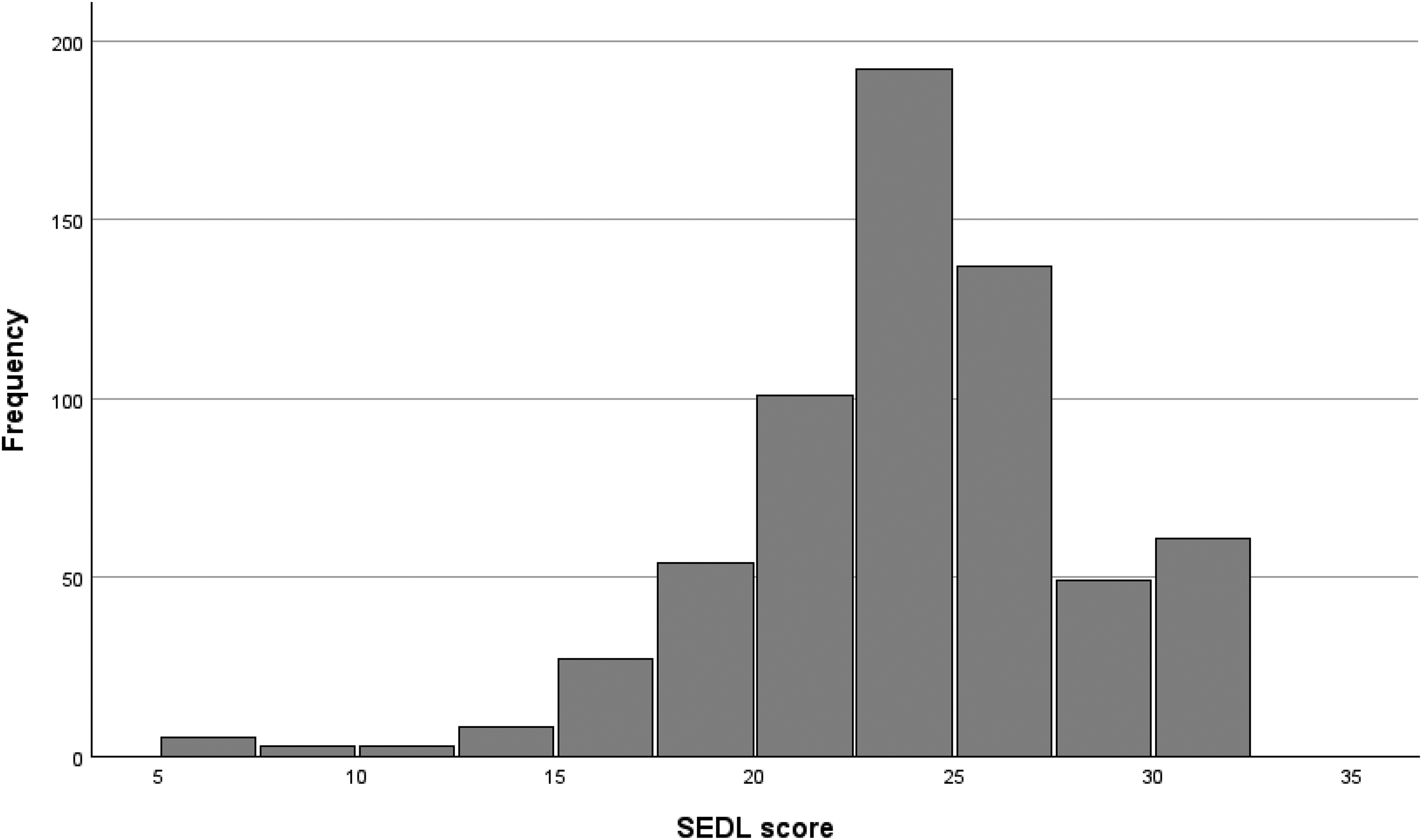
Distribution of SEDL scores. SEDL=Spirituality in Everyday Life.
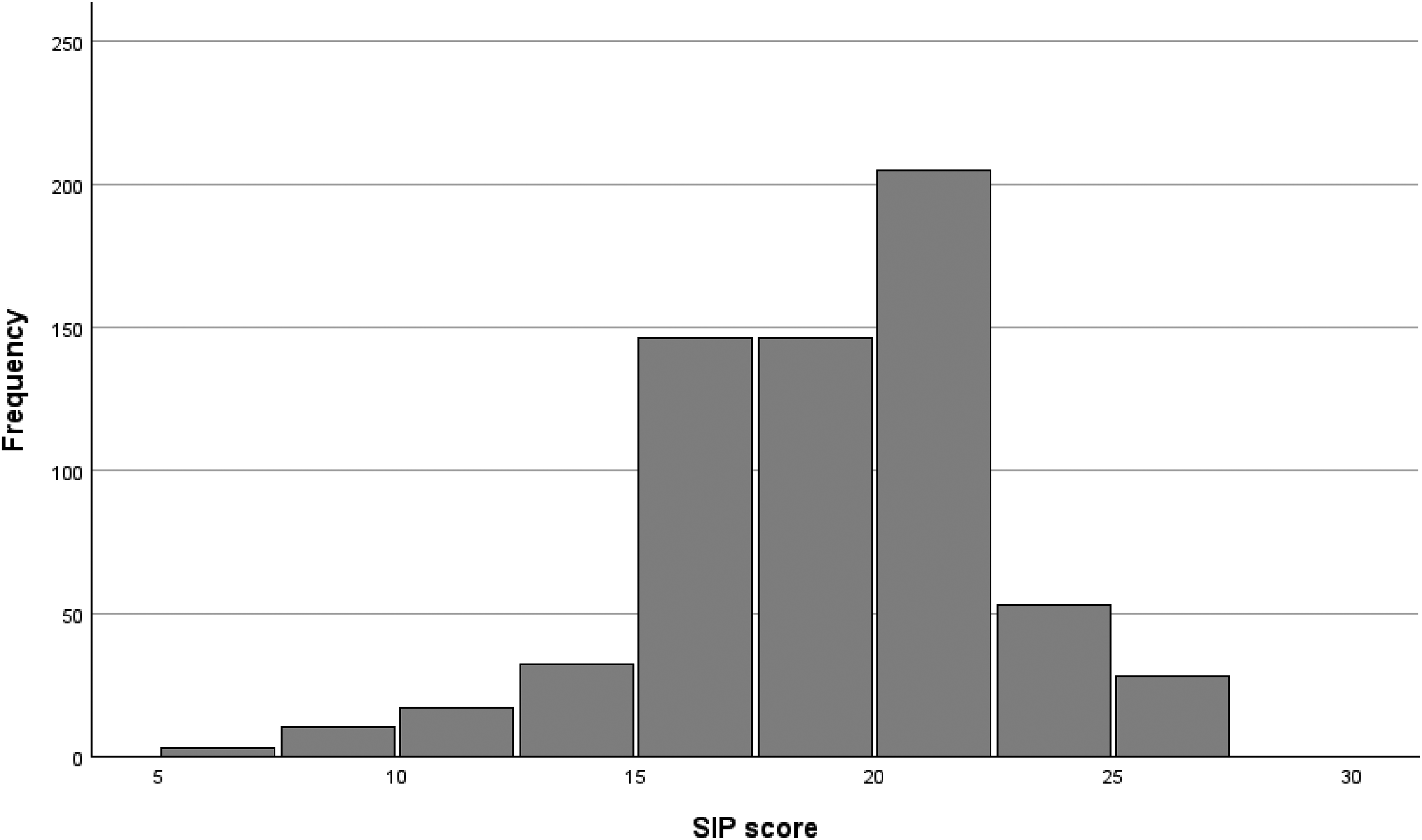
Distribution of SIP scores. SIP=Spirituality in Practice.
The outcome measures of SEDL and SIP were strongly correlated (r = 0.831; p < 0.001).
Multiple Regression Parameters (Primary Outcomes)
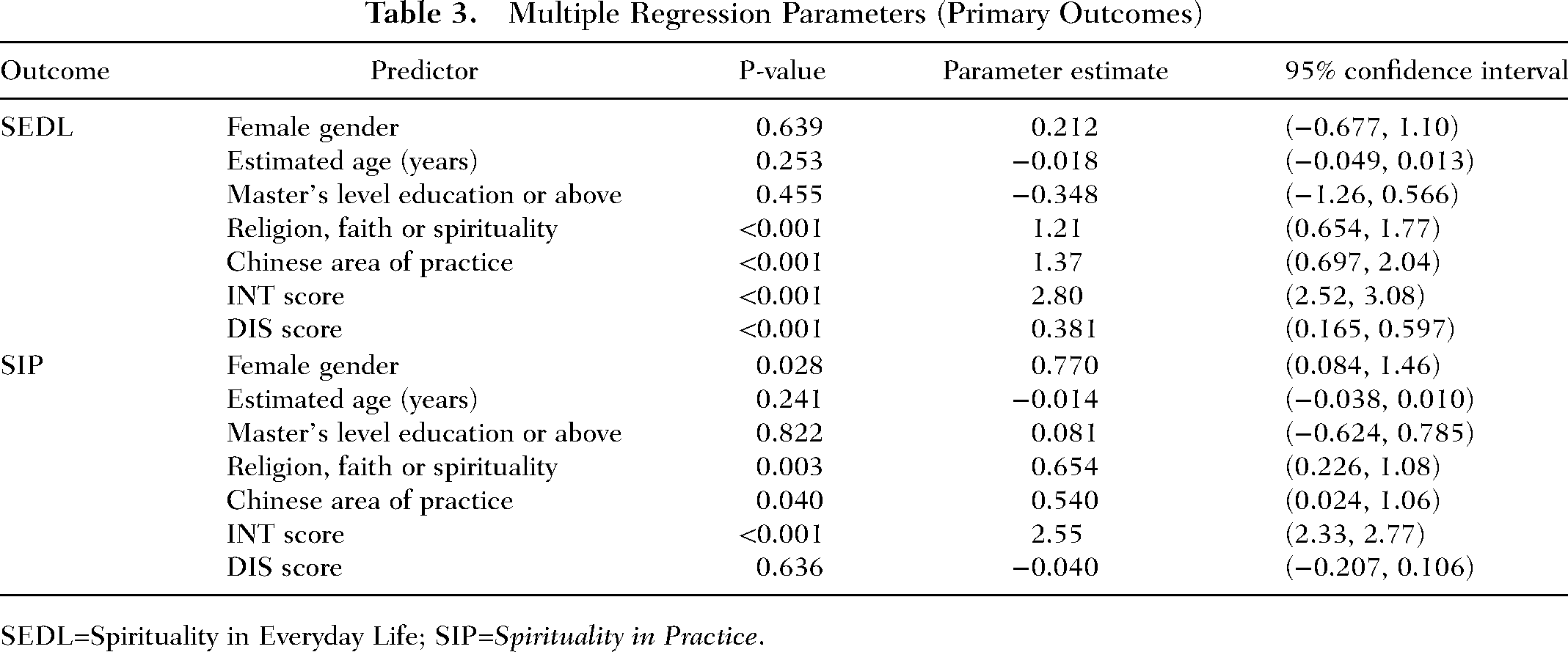
SEDL=Spirituality in Everyday Life; SIP=Spirituality in Practice.
Hence self-reported religion, faith or spirituality was associated with a mean increase of 1.21 points on the SEDL scale and a mean increase of 0.654 points on the SIP scale. A respondent whose primary area of practice was China scored on average 1.37 points more on the SEDL scale and 0.54 points more on the SIP scale than respondents from elsewhere in the world. Each additional point on the INT scale was associated with a mean increase of 2.80 points on the SEDL scale and a mean increase of 2.55 points on the SIP scale. Each additional point on the DIS scale was associated with a mean increase of 0.381 points on the SEDL scale. None of the demographic variables remaining in the multiple models (age, gender or educational qualifications) were significantly associated with either outcome at the 5% significance level.
Residuals were almost normally distributed in both models following residual analysis. There was no evidence for any violation of regression assumptions with plots of standardized residuals against standardized predicted values.
Analysis of secondary outcome measures: Reliability analysis found the CONCEPT scale to show fairly good internal consistency, with an alpha value of 0.698. The analysis proceeded with no items removed from this scale.
The mean CONCEPT score reported by respondents was 11.2, representing 3.73 points per constituent item on average. This score approaches the value given to a mean response Agree—i.e., a substantial more favorable than neutral view of the place of SEDL. Respondents used the full range of scores in answering each question.
Regression model parameters are summarized in Table 4.
Multiple Regression Parameters (Secondary Outcome)
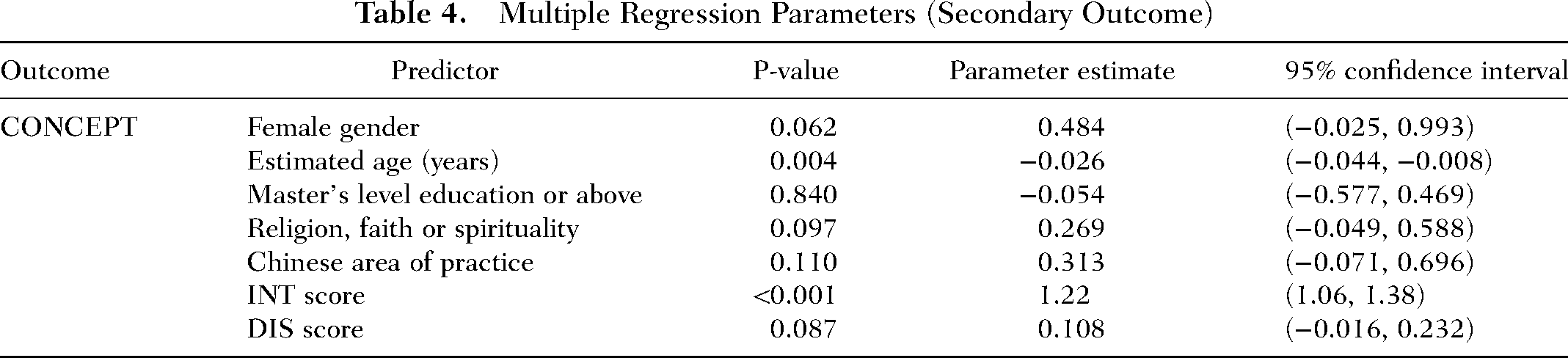
Hence each year of increasing age was associated with a mean decrease of 0.026 points on the CONCEPT scale. Each additional point on the INT scale was associated with a mean increase of 1.22 points on the CONCEPT scale. None of the other included variables (gender, level of education, religion/faith/spirituality, Chinese area of practice, and DIS score) were significantly associated with the CONCEPT outcome at the 5% significance level.
The close correlation between the two primary measures indicates that respondents had broadly similar perceptions of the concepts of SEDL and SIP. This suggests a possible degree of redundancy of measures and is consistent with findings of the corresponding study reporting mental health service user data; however, further work on a larger sample would be needed for a fuller assessment of congruence.
Nursing is typically a female majority field, and it is estimated that only 11% of the APN population are male, which suggests that the gender representation within the study (9.8% male respondents) is not dissimilar to global figures (World Health Organization, 2020). While a significant correlation was observed between gender and SIP score, but not between gender and SEDL score, the low proportion of male respondents in the sample leads to a degree of uncertainty in the gender effect on both scales.
The DIS score showed the reverse effect to the gender factor, showing correlation with SEDL but not SIP. This may suggest a difference in the perception of the separation of religion from SIP, compared to in one's personal life. There has been an increase in research into spirituality within healthcare across the last two decades (de Diego-Cordero et al., 2022), both within professionals’ work and personal well-being. Further research into the utilization of spirituality across both domains may help explain the differences in correlative variables across both scores.
Key predictors of higher levels of perception of SEDL and SIP included self-reported religion or faith, current primary practice located in China, and higher scores on the single-item INT scale, i.e., a stronger belief that spirituality is integrated into practice. There is existing research into spirituality within Chinese professionals but a relative lack of comparison to other regions. There has been research into comparing Western and Chinese attitudes surrounding spirituality, both developing measurement tools and the distinction between religiousness and spirituality (Li et al., 2018) across both regions. However, these results may also be affected by the proportion of participants who identified China as their region of practice, and as discussed in the analysis; exploration of other Asian cultures may provide a wider spread of participants.
Demographic attributes have non-significant effects on SEDL or SIP scores aside from gender and region of practice. Age and level of education were not significantly correlated with either measure, suggesting a fundamental relationship with spirituality in the APN population which is constant over time and is not determined by educational achievement. Interestingly, this does not correlate with the findings of DeKoninck's work, which suggested younger APNs would be more likely to integrate spirituality into their work (DeKoninck et al., 2016). However, our study revealed that a secondary measure, the CONCEPT score, was correlated with age, suggesting that younger age was associated with a higher awareness and perceived importance of spirituality as a concept. This may suggest a distinction between beliefs about the role of spirituality within healthcare and APNs’ ability to integrate it into practice.
Implications for Nursing and Health Policy
The findings from this study reinforce the importance of spirituality as a meaningful dimension in both the personal and professional lives of APNs globally. The consistently positive perceptions of SEDL and SIP suggest that APNs recognize the value of spiritual awareness, even if the extent of integration into care may vary. This underscores the need for spiritual competence to be more explicitly addressed within APN education, training, and role development. In the context of holistic nursing science, the study findings point to the nuanced, contextual nature of spirituality in care—they support the advancement of holistic nursing as a discipline that not only recognizes the whole person but also seeks to understand how culture, belief systems, and personal meaning-making influence care delivery. This affirms the AHNA's emphasis on person-centered, relationship-based practice grounded in spiritual and cultural awareness.
From a policy perspective, these results call for a more explicit inclusion of spiritual competence within APN competencies, standards of practice, and accreditation frameworks across global contexts. Educational institutions and professional bodies should support curriculum design that encourages critical reflection on spirituality, enhances self-awareness, and provides practical skills for spiritual assessment and intervention—particularly in culturally diverse settings.
Strengths and Limitations of the Study
The research gained insight into perceptions and use of spirituality in APNs globally. A strength of the research was the large (n = 641) sample of APNs, as well as the diversity of this sample, with participants from 55 countries across the world. This allowed for a broad understanding of the use and perception of spirituality and Spiritually Competent Practice in APNs in multiple cultures. Results pointed to how APNs view spirituality both within and outside of their work. However, there are considerations to acknowledge in terms of this sample. There is a high percentage of Chinese participants, which could mean a deviation in the understanding of spirituality in terms of ethno-centric understanding of spirituality.
This research is considered to have high external validity due to the distribution and diversity of participants, its high completion rate and real-world, multi-site setting. However, because of this, it is difficult to have a widely agreed upon definition of spirituality, as participants are likely to define spirituality in different ways due to their own personal experiences, education or training, culture, religion, and socio-economic circumstances. Hence, internal validity is correspondingly lowered, due to the incongruence in defining spirituality, the role of religion cross-culturally and the influence of social norms in spirituality decision-making and use. The research highlights that practitioners globally use spirituality in both practice and in their everyday life, although the underlying reasons for these choices were unable to be determined. Thus, it is proposed further qualitative research would need to be undertaken to understand the reasons for the use of SIP. While further depth is needed, this research has uncovered the use of spirituality globally, both in practice and its relation to SEDL.
The SEDL and SIP measures employed in this study are validated measures which have been utilized in previous research (Rogers et al., 2019, 2023) to gain insight into attitudes to spirituality in individuals using mental health services, in mental health practitioners, and into the relevance of Spirituality Competent Practice.
It may be unreasonable and even counterproductive to suggest a universally understood definition of spirituality due to its interpersonal and sociocultural influences. This study has not investigated any variation in the meaning of spirituality to respondents from difficult cultures who completed the survey based on their own definition of spirituality, which was unknown to the research team.
Ultimately, the study contributes to a growing body of evidence positioning spirituality as a vital, evidence-informed aspect of holistic nursing care which may encourage further exploration into how APNs can bridge the personal-professional divide in spiritual practice and possibly how these conceptual tools can be meaningfully adapted in further research.
Recommendations for Further Research
Research which aims to further understand APN perceptions and integration of spirituality into practice would be beneficial, including exploration of individual definitions and lived experiences of spirituality. Additionally, a study examining the differences between Western and Eastern perceptions of spirituality would be valuable, particularly in view of the large response rate from China in this study. This could foster greater understanding of APNs’ conceptualizations of spirituality, and what it means for individuals utilizing spirituality in their practice, as well as begin to uncover sociocultural differences in spiritual perspectives a deeper level. Further research may also support the development and refinement of frameworks and conceptual tools/models to guide education, reflective practice, and implementation. Such research would also help inform evidence-based strategies for integrating spirituality in APN education and clinical guidelines, thereby advancing the science and practice of holistic nursing.
Implications for Practice
The integration of spirituality in advanced practice nursing (APN) holds significant potential for improving holistic patient care. To achieve this, efforts should focus on enhancing APNs’ understanding and implementation of Spiritually Competent Practice through targeted education and training. Educational curricula for both undergraduate nursing degrees and APN programs should incorporate comprehensive modules on spirituality, emphasizing its role in fostering hope, meaning, and purpose for both patients and practitioners—which in turn enables more holistic and person-centered care. Additionally, frameworks for integrating spirituality into clinical practice should be developed and tailored to address identified barriers, such as lack of confidence or limited resources. Fostering spiritually competent environments may be aided by the tools used in this study—particularly for younger APNs who appear more attuned to its value. These tools can serve as both reflective and developmental instruments, enabling practitioners and educators to assess and strengthen spiritual integration in clinical care. Integrating such frameworks into mentorship, continuing professional development and cross-collaboration may enhance the delivery of more compassionate, whole-person care. Understanding the sociocultural dimensions of spirituality, particularly the differences in perceptions between Western and Eastern contexts, can further refine these frameworks and ensure they are culturally sensitive. By equipping APNs with the necessary tools, knowledge, and confidence to address spiritual needs, health-care systems can enhance patient outcomes and support a more holistic approach to care.
Conclusion
Spirituality is a vital aspect of advanced practice nursing, promoting holistic care and providing both patients and practitioners with a sense of hope, meaning, and purpose. Despite its importance, spirituality remains underutilized due to barriers such as limited education and lack of confidence among APNs. Addressing these gaps through updated educational programs, practical tools, and training in spiritual care can empower APNs to integrate spirituality effectively into their practice. Understanding the sociocultural dimensions of spirituality and its impact on both professional and personal domains will further enhance its integration into nursing care, improving patient outcomes, and advancing the quality and delivery of holistic nursing and healthcare.
Footnotes
Acknowledgments
Thanks to our Research Assistants: Siena Forance, Kati Tikkanen, Yolanda Figas, Catherine Stephenson, and Harriet Slater. Acknowledgement that this study was supported by the International Council of Nurses Nurse Practitioner Advanced Practice Nurse Network (ICN NPAPNN), with significant contributions made by several of its members. This data has been lawfully acquired.
Contribution to the Wider Global Clinical Community
The results from this study illuminate Advanced Practice Nurses perceptions of spirituality globally.
Ethical Considerations
Ethical approval was obtained from the University of Huddersfield's School Research Ethics Panel (SREIC/2021/105). All participants provided consent.
No Trial or Protocol Registration
No Conflicts of Interest
Patient or Public Contribution
Members of the public participated in conception of the study through discussion at a Spirituality and Compassion Special Interest Group. They received updates on the study throughout.