
Abstract
Aging is accompanied by inherent changes that impact an individual's physical, mental, psychological, and social well-being through various age-related diseases and social disconnectedness (Beard et al., 2015; Kojima et al., 2019). Older adults living in long-term care (LTC) facilities often lead physically inactive lifestyles (Chen, 2010; Parry et al., 2019), thus compounding the loss of functional ability, independence, and social isolation. Physical activity is recommended to reduce the risk of chronic disease, prevent decline in physical and cognitive functioning (Cunningham et al., 2020), improve muscle strength, and improve muscle endurance for older adults living in institutional LTC facilities (Narsakka et al., 2023).
Maintaining functional independence and the ability to perform activities of daily living (ADL) are important for older adults living in LTC facilities (Marty et al., 2017) both of which might be related to the risk for sarcopenia (Cruz-Jentoft et al., 2019; De Souza et al., 2022) and a number of additional health concerns (Sverdrup et al., 2018). Physical inactivity is a primary modifiable risk factor for the prevention of sarcopenia and frailty in older adults (Mijnarends et al., 2016). According to the European Working Group on Sarcopenia in Older People (EWGSOP2), sarcopenia is a progressive muscle disease characterized by loss of muscle mass and strength (Cruz-Jentoft et al., 2019). Regarding overall health, sarcopenia is associated with increased risk of falls (Cruz-Jentoft et al., 2019; Schaap et al., 2017), frailty (Cruz-Jentoff et al., 2019), loss of independence (Dos Santos et al., 2017; Hoogendijk et al., 2019), decreased quality of life (Beaudart et al., 2017), and impaired cognition (De Souza et al., 2022).
While regular exercise can improve muscle strength and physical fitness for older adults, finding suitable exercise programs for older adults living in LTC facilities remains a challenge. Due to various mobility restrictions of older adults living in LTC facilities, many physical activity programs may not be appropriate for this population. Chair-based exercise (CBE) is a viable program that is completed from a seated position and can incorporate various exercise components including aerobic exercise, strength training, and stretching, while remaining low-impact and having a low fall risk. In a systematic review of CBE programs, nine out of ten studies reported an improvement in outcomes for older adults in the areas of physical function, cognitive function, or well-being while seven out of ten studies reported improvements in physical performance outcomes (Cordes et al., 2021). Despite the low mobility levels and high frailty levels of residents in LTC, CBE interventions can have a positive impact on health-related outcomes, and evidence-based CBE programs are recommended for LTC residents multiple times per week (Cordes et al., 2021).
Vitality Acupunch (VA) is a modified version of the healthy-beat acupunch exercise program, which is appropriate for community-dwelling older adults with probable sarcopenia (Jones et al., 2021; Tsai et al., 2020). The program improved functional fitness of older adults living in LTC facilities in Taiwan (Chou et al., 2022; Tung et al., 2022). Due to the low number of reported CBE studies (Cordes et al., 2021) and the need for multicultural exploration of the VA program to other regions (Chou et al., 2022), Chou et al.'s (2022) CBE VA program was replicated as the first pilot project in the United States (US). The VA program incorporates concepts of the whole person through a mind-body-based practice, including physical activity, deep breathing, and relaxation, while integrating key elements of traditional Chinese medicine (TCM) associated with body meridians and acupressure points. According to the National Center for Complementary and Integrative Health (2019), it is not uncommon for older adults to turn to complementary and integrative practice approaches as part of their own self-care and well-being. Incorporating a VA program tailored to the unique needs of older adults in LTC facilities offers opportunities to expand current knowledge on integrative health therapies as part of holistic nursing care.
This pilot project aimed to test the effects of a 24-week VA exercise program on muscle mass, muscle strength, muscle endurance, functional fitness, ADL, quality of life (QoL), and sleep quality of older adults in LTC facilities with probable sarcopenia in the US. Secondary aims included understanding the experiences of residents in a LTC facility who participated in a 24-week VA exercise program. The VA exercise program aimed to improve physical and psychosocial outcomes for older adults residing in LTC facilities, thus implementing a holistic approach to LTC in an underserved population.
Theoretical Framework
The goal of holistic nursing is to provide care for the whole individual, including the unique physical, psychological, social, cultural, and spiritual needs (Hao et al., 2017). This concept of holism is consistent with concepts of TCM including “unity of heaven and humanity” and “unity of the body and mind” (Hao et al., 2017). While acupressure and acupuncture have been long-accepted forms of complimentary alternative medicine based in TCM, both require precision and additional training to perform, which may not be attainable for individuals in LTC. Acupunch integrates the concepts of meridian theory in TCM in which various punching styles are used to engage the body and limb's natural swinging motions to vibrate acupoints along the body's 14 meridians (Tsai et al., 2020). Like holism in which the body is seen as a whole organism, the premise of meridian theory is that the pathways of the body are interconnected (Hao et al., 2017). Stimulating meridians allows for the free flow of blood, energy, and qi through the body to promote circulation and maintain health (Zhang et al., 2015).
Methods
Design
A mixed methods experimental design was used in which qualitative data were embedded within an intervention trial. The mixed methods experimental design was used to test and compare the effects of a 24-week VA program compared to no treatment controls on muscle mass, strength and endurance, functional fitness, ADL, QoL, and sleep for institutional older adults with probable sarcopenia in the Southern US. The focus groups and one-to-one interview were embedded in this larger design after the intervention for the purpose of understanding participants’ response to the program.
Hypotheses and Research Question
Based on the principles of meridian theory in Traditional Chinese Medicine, it was hypothesized that:
Residents in a long-term care facility who participate in a 24-week Vitality Acupunch exercise intervention would have significantly higher scores for muscle mass, muscle strength and endurance, and functional fitness than residents in long-term care who did not participate in Vitality Acupunch.
Residents in a long-term care facility who participate in a 24-week Vitality Acupunch exercise intervention would have significantly higher scores for sleep quality, activities of daily living, and quality of life than residents in long-term care who did not participate in Vitality Acupunch.
What were participants’ experiences with Vitality Acupunch?
How do qualitative findings from focus groups and a one-to-one interview provide greater understanding of the quantitative results?
Sample and Setting
Participants were recruited from three LTC facilities in the Southern US. Two facilities served as intervention sites and one as control. Residents within the LTC facilities were notified about informational sessions through flyers posted within the facility, announcements made by facility leaders, and reminders made during morning rounding by facility staff. Informational sessions were held at each of the three facilities. Participants were provided the opportunity to ask questions to the PI. Those interested in participation were screened for eligibility through completion of a paper questionnaire and physical measurements in a quiet and private location at the participants’ residence. Eligibility criteria included 65 years and older, having lived in the facility for at least three months, intact cognitive function as evidenced by a Short Portable Mental Status Questionnaire (Pfeiffer, 1975) score of eight or greater, and the ability to speak and read English. Initially, calf circumference (less than 33 cm for men and women) and handgrip strength (less than 27 kg for men and 16 kg for women) were used as indications of probable sarcopenia. However, over 40% of adults aged 65 and older in the United States are obese (Stierman et al., 2021). Older adults who are obese and have reduced skeletal muscle strength are at risk for sarcopenic obesity, which can further reduce health-related outcomes (Ozkok et al., 2022) and lead to increased frailty (Jarosz & Bellar, 2009). In 2019, the EWGSOP2 replaced reduced muscle mass as the primary indicator for sarcopenia with reduced muscle strength as the primary indicator for probable sarcopenia (Cruz-Jentoff et al., 2019). Therefore, only muscle strength was used as an eligibility measure for possible sarcopenia.
Upon confirmed eligibility and consent, participant facilities were randomly assigned through simple randomization by the flip of a coin to either the VA experimental group or the wait-list control group based on the long-term care facilities where they lived. The outcome of the coin flip, heads or tails, has an equal probability, providing a fair and practical method for randomization. The facilities were randomized by location (two facilities were in one community and the third facility was in a nearby community). Though there were three total facilities, the two located in one community were considered as one site for the purposes of randomization and in consideration of comparable sample sizes across intervention and control groups. Heads was designated as the intervention site while tails was designated as the control site. All participants received one pre-test and two post-tests, three months apart, during the study.
Ethical Considerations
The study was approved by the University Institutional Review Board and each of the participating LTC facilities. Participants signed informed consent before both quantitative and qualitative data were collected. After obtaining informed consent, the participants completed questionnaires via pen and paper. Physical measurements were collected by trained research assistants. Participants were assigned a unique two-digit identifier. The two-digit identifiers were used during data collection. Unique identifiers and informed consents were stored in separate locations.
Intervention
This study replicates a completed study that took place in Taiwan (Tung et al., 2023). The VA program was a non-invasive exercise program that took 40 minutes to complete and included three phases with a fiveminute rest in the middle: (a) activating qi and blood, warm-up exercises that allow the body to accumulate heat and promote flexibility of the joints to loosen up the body (5 movements, 8 minutes), (b) punching meridians: both hands were used to exert a vibrating effect according to the rhythms that stimulate the 14 meridians in the entire body to improve aerobic endurance (14 movements, 19 minutes), and (c) relaxing body and mind, muscle relaxing exercises to rest the body and cease the qi (5 movements, 8 minutes) (Tsai et al., 2020). The five fist forms (dragon fist, tiger fist, trunk fist, phoenix fist, and palm beat), the meridian vibration technique, and punching (vibrate meridians by clenched fist with empty palm), were applied. Participants completed all exercises from a seated position.
The VA exercise program was led by instructors who were trained and certified in VA. Participants in the experimental group received the VA program three times per week, 40 minutes per session for 24 weeks (Tung et al., 2023). Participants in the wait-list control group continued with their daily activities as usual. After the 24-week study, the VA program was made available to the waitlist control group. To remain in the final data analysis, participants were required to attend over 50% of the total number of classes. The overall attendance rate of the intervention group over 24 weeks was 90%.
Measures
Quantitative
Qualitative
An interview guide consisting of six open-ended questions was used to elicit participants’ experiences with VA. There was no need to refine the interview questions during data collection. Probes were used as needed to gain an in-depth understanding of participants’ experiences. Examples of questions included: “Why did you choose to participate in Vitality Acupunch?” and “Describe your general experience with attending the Vitality Acupunch class.” Probes were used to gain greater insight and understanding.
Data Collection
Quantitative
The effects of VA were tested on the primary outcome variables (muscle mass, muscle strength, muscle endurance, and functional fitness) and secondary outcome variables (ADL, QoL, and sleep quality) at baseline, month three, and after the 24-week intervention. Data were collected by the trained research assistants who were blinded to group assignment. The primary investigator (PI) oversaw all data collection. Study personnel attended a twohour workshop during which they were trained in how to perform each measure to ensure consistency.
Qualitative
Focus groups and the one-to-one interview were conducted by the PI and trained research assistant in a quiet private location at the facility. Focus groups and the interview were audio recorded, transcribed verbatim, and verified. Detailed notes regarding the tone of the interview or focus groups, non-verbal communication, environmental observations, and distractions were documented throughout each session by a research assistant.
Data Analysis
Quantitative
All statistical tests were performed using IBM SPSS software version 29 for Windows (IBM Corporation, Armonk, NY, USA). Prior to conducting any analyses, variables were tested to ensure that the assumptions required for the statistical tests to be used were met. Pearson's Chi-squared or Fisher's exact tests when expected cell counts were less than five and independent t-tests were used to examine baseline differences between the groups. A repeated measures analysis of variance (ANOVA) was conducted to determine time and group effects. The nonparametric Kruskal–Wallis test was used when required assumptions for performing parametric tests were violated. Statistical significance was set at p < .05.
Qualitative
Descriptive analysis was conducted to identify and analyze recurring patterns in the data. Descriptive analysis provides a straightforward description of participant experiences, particularly in situations where limited data on a topic exists (Sandelowski, 2010). Credibility in qualitative research can be achieved through peer review, reflexivity, member checking, and creating rich thick description (Creswell, 2013). The researchers engaged in peer debriefing sessions and documented the discussions. Field notes and journal entries were considered during analysis. The team reflected on their own biases regarding Chinese medicine approaches and how biases might influence analysis. To ensure reliability and validity, the research team engaged in meetings to discuss and review the interpretations. Inter-coder reliability was established by having multiple coders independently analyze data and assess the level of agreement. Any discrepancies were resolved through discussion and consensus among the coders.
Results
Quantitative
A total of 40 older adults residing in three LTC facilities with probable sarcopenia were enrolled in an intervention group (n = 24) and a control group (n = 16) in September 2022. Of those enrolled, 27 (67.5%) completed the 24-week study (ending May 2023) and were included in the analyses. Thirteen older adults (32.5%) withdrew from the study due to death (n = 1), leaving the LTC facility (n = 3), or other reasons including bone fractures, new onset dementia, acute hospitalizations, COVID-19 infections, and preferred not to disclose (n = 9). The numerical breakdown of baseline demographic and clinical characteristics of the sample can be found in Table 1. Demographics did not differ significantly between the two groups except for level of education. The intervention group had more participants with less than a high school education compared to the control group. The mean age of all participants was 85.32 ± 8.33 years. Most participants were women (87.5%), widowed (57.5%), and had at least a high school education (80%). Of all the participants, 37 (92.5%) had at least one chronic disease; high blood pressure (62.5%) and arthritis (62.5%) were the most frequently reported chronic illnesses. The mean SPMSQ score was 8.97 ± 0.89.
Intervention and Control Group: Baseline Comparisons
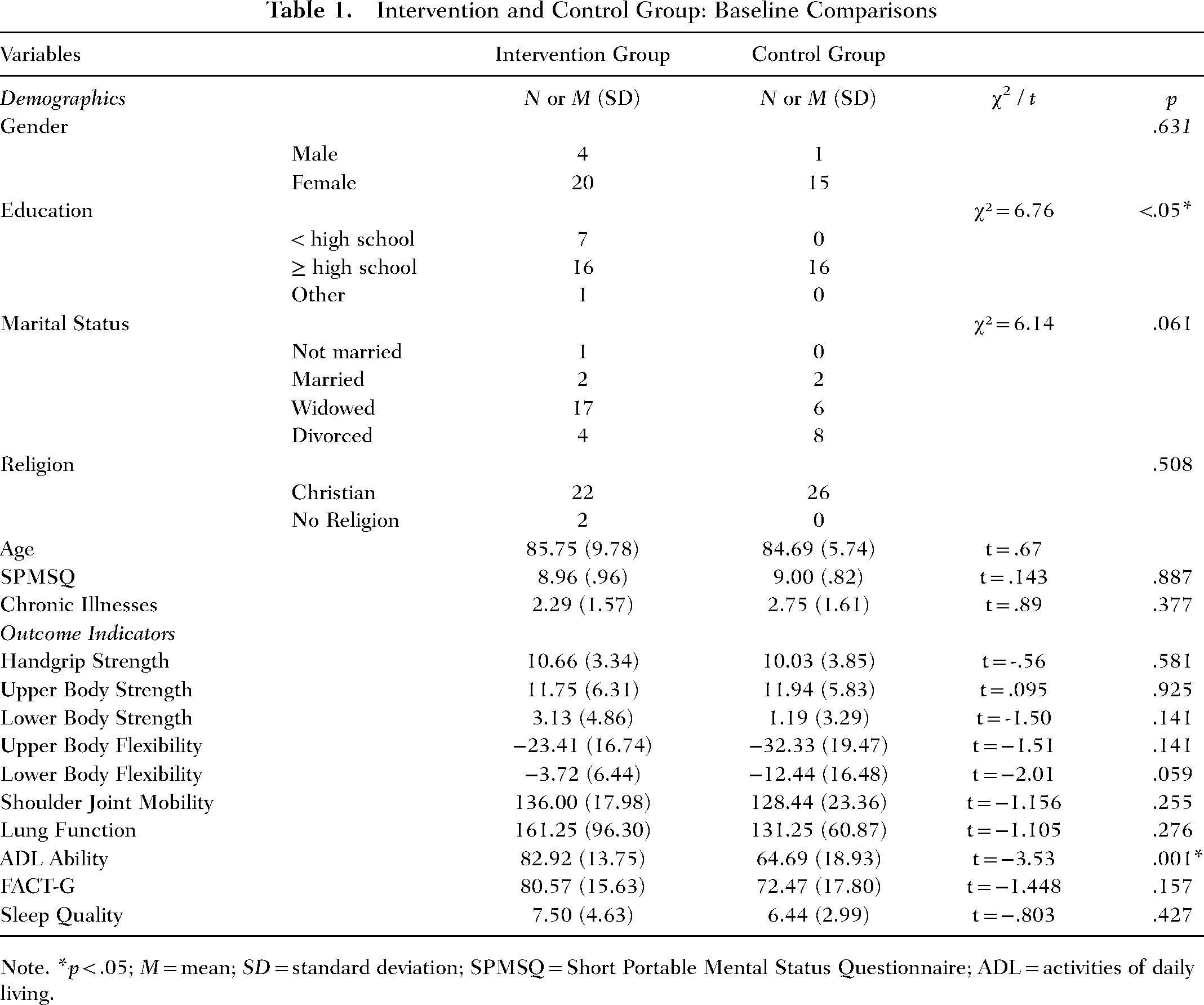
Note. *p < .05; M = mean; SD = standard deviation; SPMSQ = Short Portable Mental Status Questionnaire; ADL = activities of daily living.
Results of the repeated measures ANOVA tests revealed significant within-group differences on range of joint motion, ADL ability, QoL, and sleep quality. Significant between-group differences were found only for range of joint motion (see Table 2). Nonparametric comparisons using Kruskal–Wallis tests are reported in Table 3. Comparisons revealed significant differences in upper body flexibility and hand grip strength.
Means, Standard Deviations, and Repeated Measure ANOVA Statistics for Study Variables (N = 27)
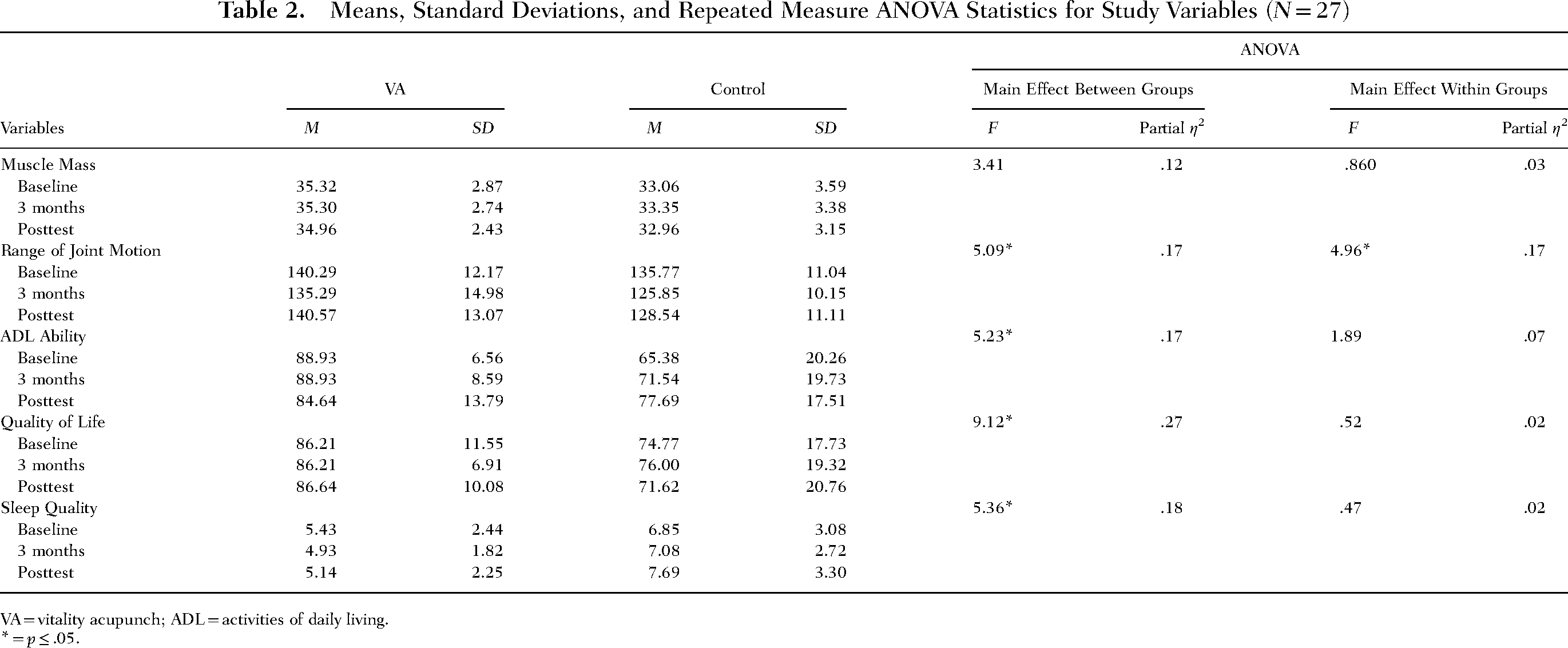
VA = vitality acupunch; ADL = activities of daily living.
* = p ≤ .05.
Means, Standard Deviations, and Kruskal–Wallis Statistics for Study Variables (N = 27)
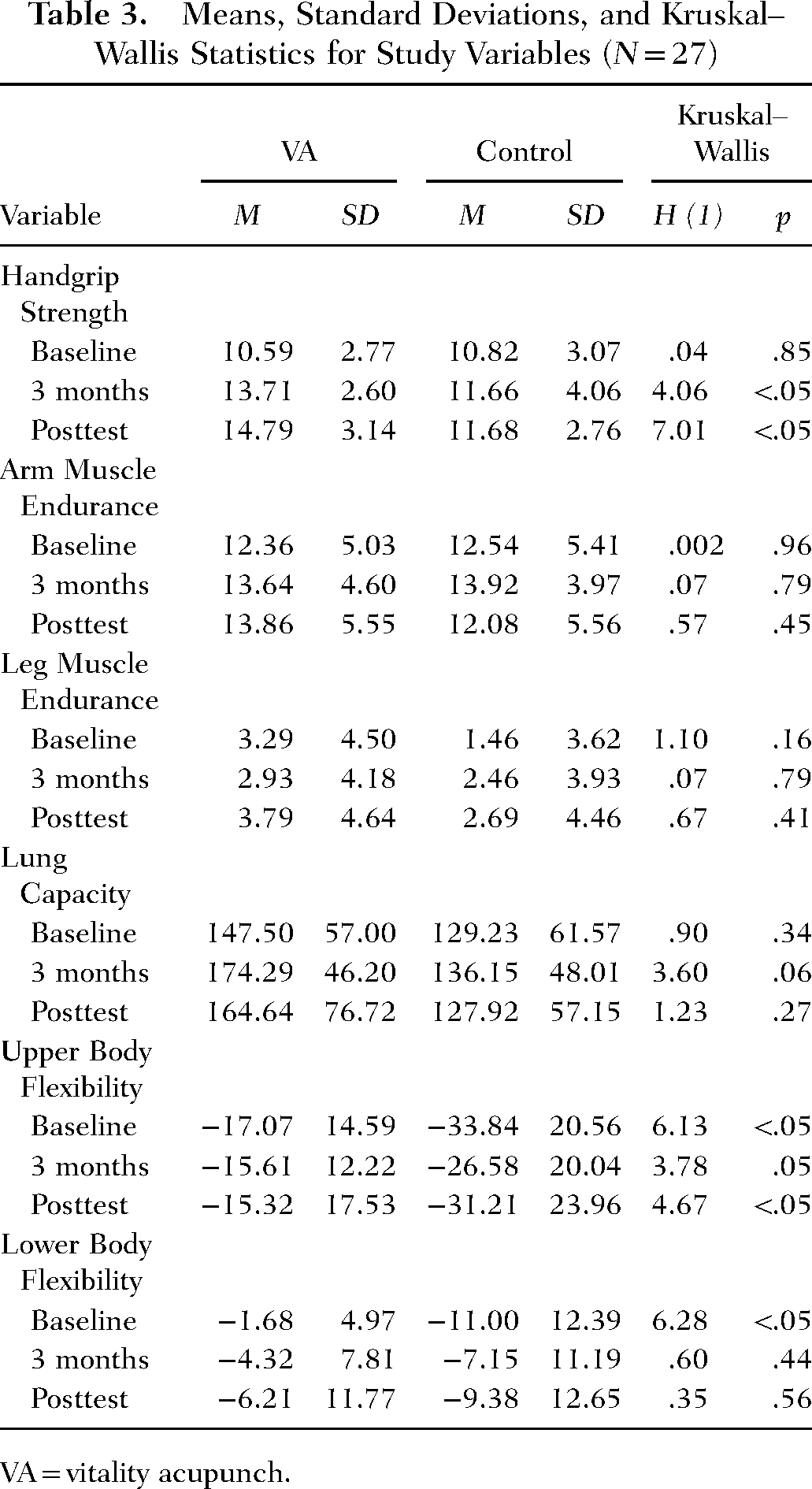
VA = vitality acupunch.
Upper Body Flexibility
Initial group differences were determined between the control and experimental groups on the upper body flexibility variable. To account for these differences, a repeated-measures ANCOVA was conducted with baseline scores as the covariate on upper body flexibility scores at threemonths and post-intervention. Results indicated no differences were seen in on the Back Scratch Tests between groups (p = .817).
Hand Grip Strength
The Bonferroni correction was applied for post-hoc comparisons resulting in an adjusted alpha of 0.025. The Kruskal–Wallis tests indicated that the handgrip strength was not significantly different for the control and interventions at three months H(1) = 4.058, p = .044. Handgrip strength was significantly higher in the experimental group compared with the control condition at posttest H(1) = 7.009, p = .008.
Qualitative
Eighteen individuals participated in focus groups at one facility, and one person completed a one-to-one interview at the second facility. All individuals that participated in the VA intervention were invited to participate in the focus group sessions. To accommodate special hearing needs of the participants, focus group participants were split into two groups at one of the intervention sites by room location within the facility. Due to attrition and participant discharge from the facility, one individual interview was conducted at the second site. The primary reason for participation in VA was to improve themselves either physically or mentally. Participants said, “I need the exercise,” “I was curious,” while another added “I wanted learn something new.” “I’m 98 years old and I want to stay young” offered one person. VA was considered a form of physical therapy for a participant with back problems whose surgeon encouraged him to participate in order to avoid surgery. VA served as motivation for participants to “get up and moving in the morning” and “keep ourselves going.” The ability to do the exercises sitting down and in a wheelchair was an attraction for others who had a hard time standing due to neuropathy, balance problems, and cerebellar ataxia. The fact that the program was offered at the facility was appreciated by one individual.
Participants shared diverse experiences with VA. While apprehensive in the beginning because VA was something unfamiliar, many shared how over time they came to look forward to the sessions and enjoyed them. One person felt special to have “been chosen” to participate. Having a scheduled activity at a specific time and day with a designated and dedicated facilitator was appreciated. Learning a new program was promoted by mastering exercises a few at a time and group encouragement. The uniqueness of the program was recognized and compared with previous exercise experiences, “. . . having your fists in a certain motion and hitting certain parts. That was very different” and “I never used to hit myself” offered two participants.
In the beginning, some felt that the exercises were difficult, were unsure if they could correctly perform them, and were skeptical about how VA might affect them, if at all. For example, “We were all so tired in the beginning; now it's not all that hard anymore,” and “We got a little bit better at it” said two participants. Others reflected, “In the beginning I thought, ‘Oh, I can’t do that’; But you can” and “I didn’t think coordinating hands and legs was possible but finally was able to achieve that which surprised me.” As time passed, participants recognized they felt better, “I thought maybe it might be just this run-of-the-mill exercise, but after we got started, then we all enjoyed it and got benefit from it,” and “Now I miss it because I feel better after I come.” While psychological outcomes were not directly assessed, these findings speak to confidence and the positive impact of learning a new skill. “At first, I wondered, ‘What could this do?’ then realized the flexibility (improved) and the way it helped my body,” stated another participant. One person who “had trouble with (her) shoulders” felt the range of motion had improved. Follow-up assessments promoted “a sense of achievement” when improvements were noted.
The program and exercise names were unfamiliar. Acupunch “is different, a word I’m not used to—I expected it to be something else instead of the exercises that we learned” shared a participant. Exercise names did not seem to describe the movement that another participant imagined.
VA had a positive impact on participants’ daily life. Increased strength “especially in my arms,” the ability to “move a little easier,” and improved flexibility were reported. One participant shared that they “had syncope, and I haven’t had a syncope since we’ve been doing it.” Another person said, “I can still run—so that might have something to do with it.” VA motivated participants to “continue exercising,” “see how much further I could reach the next time without straining” and get out of bed. Individual participants planned to continue performing the exercises and indicated that some exercises had been incorporated into the facility's regular exercise program.
Several experiences were identified as the favorite part of the program. One exercise, “when you got to rub your back” was the favorite part for one person. Others appreciated the “socialization,” “meeting new people,” “helping each other” and “knowing there were other people to help us.” Shared feelings and problems were perceived as valuable. These findings highlight social connectedness among participants and instructors. Setting goals was recognized as the favorite part for another person. One person reflected that stretching promoted a sense of “energy coming into my body” and therefore was the favorite part. Having something to do and “seeing (the facilitator)” were other contributions to the discussion about favorites.
Participants described things they would change about the program. “One exercise where we go like that and one leg up to another and go up to the other leg” (punching the shoulders with phoenix fist) offered one participant. Another person “can’t really get down here” when doing the (punching the calves with tiger fist). The coordination required was challenging and participants “had trouble differentiating right from left” and “got confused.” One participant wished the audio portion of the video was in English and another that felt the routine was not too repetitive. While exercises were challenging, participants recognized improvements and indicated that they “did what they could.”
Facilitators were recognized as an important contributor to the program. Instructors were “very patient – we appreciated it” and “a great instructor” reflected a participant. Explaining in the beginning that they would learn two to three moves each session and would learn the entire routine over time was valued. The instructor's smile made one person feel happy.
Discussion
The VA program integrated concepts of holism into a physical activity program for aging individuals in LTC. While participants were generally unfamiliar with TCM practices prior to the start of the study, many participants exhibited positive physical and psychosocial outcomes through participation in the program.
Physical
The first study hypothesis, which predicted residents in the VA exercise group would have significantly higher scores for muscle mass, muscle strength and endurance, and functional fitness, was not supported. However, there were some improvements in muscle strength and endurance and some components of functional fitness, even though they were not significant. Only handgrip strength and range of motion significantly differed for the control and intervention groups. While quantitative findings did not support significant improvements in strength or functional fitness, qualitative data indicated that participants perceived increased strength, range of motion, and flexibility. People residing in long-term care facilities are expected to decline in their physical fitness and function over time due to the aging process and living conditions. Thus, while it is not surprising that there was not a significant increase in primary outcomes, it is interesting that the scores were maintained or improved for most outcomes over the sixmonth intervention. It should be noted that residents in both groups continued to engage in normal activities, including physical therapy in some cases. It was surprising to find a significant decrease in the range of motion for the intervention group, which could be explained by events unrelated to the study that occurred during the six months. Despite the decrease, individual participants reported improvement in the range of motion in qualitative interviews, especially concerning their shoulders and arms. The VA exercise program includes stretching exercises that facilitate shoulder flexibility. This finding, though not significant, is supported in the literature for similar studies (Chou et al., 2022; Tung et al., 2020).
Psychosocial
The second study hypothesis, which predicted residents would have significantly higher scores for sleep quality, ADL, and QoL, was not supported. While not significant, there were improvements in sleep quality and QoL for the intervention group. Qualitative data suggested that the program promoted motivation to exercise and socialization. Participant's reported positive feelings related to the social aspect of the study, including socialization with their instructor. During qualitative interviews, participants indicated they continued to perform the exercises after the study was over. Participants commented that learning a new physical activity kept them mentally engaged. Notably, ADL decreased over time for the intervention group and increased for the control group. Standard of care differences between facilities may account for the unexpected outcomes. Specifically, physical therapy was a regular part of care for residents in the control group.
Limitations and Strengths
This pilot study had some limitations. First, the study had a small sample size and a predominately female participant population. Additionally, the study took place in a specific region of the southern United States, and participants were recruited through convenience sampling. Due to the sample and location, results may not be generalizable to the greater older adult long-term care population or other populations or regions of the US. Even though the facilities were randomized, the limited locations of facilities may have resulted in sampling bias. The study was statistically underpowered, possibly contributing to some insignificant findings.
There were several challenges that were unique to this population. In the post-Covid-19 era of long-term care, residents are subject to various procedures including masking based on facility counts, isolating after exposure, and the overall health impacts that Covid-19 has on the older adult population. This population is also at high risk for injury. Residents that became injured (broken wrist, broken hip, etc.) from activities outside of the program were no longer able to participate in the program. In some cases, residents moved to new facilities to be closer to family. Physical challenges including poor eyesight and age-related hearing impairment may have impacted the qualitative focus groups and interview.
While limitations existed, there are also strengths of this pilot study. The study personnel were trained and certified by the founders of the VA program, consistent with the training received for the VA program in Taiwan. The personnel also attended a twohour workshop to ensure consistency in data collection measures. Due to the mixed methods approach, there was a unique opportunity to better understand the lived experience of individuals participating in the program, as this was the first VA exercise program to take place in the US.
Implications
Studies conducted outside the US have shown that the VA exercise program is an effective intervention in older adult populations (Chou et al., 2022; Tung et al., 2020). However, it is essential to explore further the potential impact of cultural and other unique population differences on the outcomes of such studies. For example, this is the first known implementation of the VA exercise program among a U.S. population of older adults, suggesting that the participants may have been unfamiliar with this type of program and its potential benefits. TCM, with its Chinese philosophy, is rooted in a holistic view of the person, considering physical health and the balance of the body as influenced by the environment (Chien, 2022). Examining contextual factors, such as trust in unfamiliar exercise programs and programs rooted in different philosophies, such as TCM, may shed light on why this intervention has been more successful in cultures familiar with TCM beliefs. As a profession, nurses view the patient holistically and are therefore in a great position to integrate complementary and integrative health approaches such as VA as part of holistic nursing care.
While most outcome measures did not result in significant statistical differences, several increased throughout the study. Therefore, it may be valuable to investigate further the effectiveness of the VA program in enhancing functional outcomes among older adults. Moreover, as indicated by their qualitative remarks, the favorable feedback given by participants and the positive influence on their daily activities lends additional credence to the need for ongoing exploration. Future research should consider exploring the VA exercise program across various populations in an extended appropriately powered study approach. Additionally, comparing outcomes across populations that are familiar with TCM practices and those that are not familiar with TCM would add understanding to the overall impact of VA across diverse populations.
Conclusion
This pilot project aimed to test the effects of a VA exercise program on various physical and psychosocial health outcomes of older adults in LTC facilities with probable sarcopenia, while aiming to better understand the experiences of residents who participated in the VA program. The study findings indicated that the VA program was a manageable and enjoyable exercise program for older adults living in long-term care facilities. While there were statistically significant improvements in muscle strength, self-reports of participants also acknowledged enhancements in physical fitness and flexibility. Residents that participated in the VA program reported positive social experiences, achievement, and accomplishment through the completion of the program. The VA exercise program offers a holistic and evidence-based exercise program for older adults with probable sarcopenia living in LTC facilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sigma Theta Tau International-Iota Nu Chapter. The funding source supported this study financially and was not involved in the study design, data collection, analysis and interpretation of data, report writing, and decision to submit the paper for publication.