
Abstract
Keywords
Members of the Two Spirit, lesbian, gay, bisexual, trans, and queer (2SLGBTQ) 1 community experience poorer mental and physical health outcomes compared to their heterosexual, cisgender counterparts due to the impacts of heteronormativity- and cisnormativity-based discrimination (Fredericks et al., 2017; Medina-Martínez et al., 2021; Rainbow Health Ontario, 2020). In Canada, the term Two Spirit was formalized by Elder Myra Laramee in 1990 and reflects the roles and acceptance of gender-diverse peoples within Indigenous communities pre-contact (Dykhuizen et al., 2022; Two-Spirited People of Manitoba, 2019). Two Spirit is increasingly, though not exclusively, used by Indigenous communities across North America to recognize the unique and complex expressions of gender and sexuality within Indigenous culture (Dykhuizen et al., 2022).
Heteronormativity is the belief that being heterosexual is the most desirable and normal sexual identity (Beagan et al., 2012), while cisnormativity is the belief that the most normal gender identity is cisgender—meaning that a person's lived gender matches the sex they were assigned at birth based on physical sex characteristics (James-Abra et al., 2015). These normative ideologies overlap with the gender binary, a dominant Western cultural ideology and practice that conflates sex and gender in order to uphold only two genders, male and female, within an oppositional hierarchy (Beasley, 2005). As dominant societal beliefs, the gender binary, heteronormativity, and cisnormativity create barriers for the 2SLGBTQ community (Lim & Hsu, 2016), particularly in health care environments where normative ideologies tend to prevail.
Although many health care needs of the 2SLGBTQ community are no different than those who identify as heterosexual and cisgender (Manzer et al., 2018), in highly gendered areas of care—such as family planning 2 —2SLGBTQ people may face additional barriers. These barriers can be due to the impacts of the gender binary and normative beliefs about sex and gender, which are reinforced through policies, practices, and language as many health care environments fail to provide inclusive resources and spaces (Klein et al., 2018; Richardson et al., 2019). The lack of inclusion contributes to further discrimination, poorer health outcomes, and marginalization of those within the 2SLGBTQ community (Elertson & McNiel, 2020; Fredericks et al., 2017; Richardson et al., 2019; Utamsingh et al., 2016).
Health care providers (providers) have the power to reduce barriers and improve access to services but may lack awareness of 2SLGBTQ community needs. Many providers believe that to treat everyone equally, they must treat everyone the same (Beagan et al., 2012; Dorsen & Van Devanter, 2016; Manzer et al., 2018; Rider et al., 2019; Stewart & O'Reilly, 2017). Because of this belief, providers report that they simply avoid discussing gender and sexuality so as not to “offend” their patients (Rider et al., 2019). However, due to normative ideologies, a lack of acknowledgment—or remaining neutral—assumes everyone is heterosexual and cisgender (Fredericks et al., 2017). Therefore, ignoring gender and sexuality reinforces the insidious cycle that perpetuates normative ideologies and can inadvertently render the 2SLGBTQ community invisible (Dorsen & Van Devanter, 2016; Eliason et al., 2010; Lindroth, 2016; Stewart & O'Reilly, 2017).
In practice, both providers and members of the 2SLGBTQ community indicate overlapping deficiencies related to the care of 2SLGBTQ community members. Providers recognize that they lack specific education, experience, and resources to provide care that is sensitive to gender and sexuality for members of the 2SLGBTQ community (Angelino et al., 2020; Elertson & McNiel, 2020; Manzer et al., 2018; Richardson et al., 2019; Rider et al., 2019). Similarly, 2SLGBTQ patients recognize that providers require more knowledge to treat them appropriately (Clark et al., 2018; Lindroth, 2016). Furthermore, a lack of relevant education causes providers to rely on their patients to teach them about gender diversity and sexual health (Manzer et al., 2018). Members of the 2SLGBTQ community acknowledge this, reporting having to take time out of their appointments to teach providers about their gender or sexuality (Fredericks et al., 2017; James-Abra et al., 2015). Ultimately, these deficiencies pose a problem where (1) both provider and patient feel as though they are unable to help or be helped and (2) both parties acknowledge that providers lack education, along with meaningful action to address educational gaps. These intersecting deficiencies create barriers to fully addressing the 2SLGBTQ community's health care needs. Acknowledging gender and sexuality is an essential component to providing holistic, whole person care.
In this research, our aim was to explore normative ideologies of heteronormativity and cisnormativity as they affect the experiences of the 2SLGBTQ community during family planning, specifically in relation to their fertility intentions. The purpose of this research was then to better understand how providers can provide appropriate, safe, and comprehensive care to 2SLGBTQ people engaging in family planning processes.
Methods
Critical Social Justice, Emancipatory Nursing Praxis, and Holistic Nursing
Although nursing draws from multiple disciplines and paradigms to inform nursing science (Younas & Parsons, 2019), it has core values that make the discipline unique. These values include a social justice mandate and an orientation toward critical questions, which require deeply nuanced answers that intersect with the complexity of the human experience. We view social justice as a multi-faceted theory and practice focused on promoting equity among all individuals by redistributing power and resources necessary to address the root causes of systemic injustices such as racism, sexism, homophobia, and ableism (Buettner-Schmidt & Lobo, 2012; Canadian Nurses Association [CNA], 2010; Walter, 2017). With these values, nursing as a discipline can address inequities existing at individual, organizational, and structural levels. Considering equity is a primary aim of social justice (Browne et al., 2015), nursing as a discipline is ideally situated to promote health equity. Furthermore, McGibbon and Lukeman (2019) add a critical lens to social justice, adding features that include analysis of hegemonic power structures and acts of resistance toward oppressive policies, with the overall goal of social change. With this perspective, McGibbon and Lukeman (2019) highlight the political nature of nursing research, education, and practice.
Emancipatory nursing praxis exemplifies critical social justice as foundational to the nursing discipline, offering a theoretical description for how nurses undergo transformational learning moving toward social justice–oriented nursing praxis (Walter, 2017). With this theory, not only are nurses aware of critical social justice, but also engage in social justice, undergoing four learning processes of becoming (unconscious awareness of injustice), awakening (recognizing the role they play in structural factors impacting health and wellness), engaging (exploration of the role of an ally in doing social justice), and transforming (expansion of consciousness; Walter, 2017). These learnings occur within relational and reflexive contexts as nurses move into social justice–oriented practice (Walter, 2017).
Considering that holistic nursing involves care of the whole person, it remains imperative to approach holistic nursing from a lens of critical social justice that acknowledges the structural and political factors that create inequities and contribute to the health of individuals and groups. In taking on a social justice–oriented holistic lens within this paper, we are creating opportunities to acknowledge the whole person within the social, political, and environmental contexts that influence health.
Research Design
As fertility intentions within the 2SLGBTQ community vary greatly depending on individual preferences, our study was designed to explore different participant perspectives without reducing them to a common theory. Our design aligns closely with case study methodology (Stake, 1995). As described by Stake (1995), case study methodology is constructivist in nature and allows for an in-depth exploration of an individual's experience within their specific context.
Considering that case study methodology centers the researcher as an interpreter and acknowledges that each researcher will bring a unique perspective to the case (Stake, 1995), it is imperative to acknowledge the researchers’ lenses that inform and shape the subsequent analysis. The primary investigator, KM, is a White settler, cisgender, woman, with no disabilities, who does not define her sexuality. A member of the larger team is a member of the 2SLGBTQ community and provided guidance. This research is also framed by national and international societal events that contributed to data collection and analysis. The COVID-19 pandemic, the murder of George Floyd and its instigation of a renewed Black Lives Matter movement, increasing incidences of trans people being killed international and nationally, and the polarizing 2020 US presidential election all highlight racial, sexual, and gender disparities affecting all aspects of health. We consider these events as influences on the research process.
Population and Sampling
The study population was comprised of individuals self-identifying with the 2SLGBTQ community. Inclusion criteria included participants who were child-free, English-speaking, and between the ages of 18–45 (reproductive age). Participants were recruited through purposive and snowball sampling that included posting an announcement on an internal university webpage and word of mouth. See Table 1 for demographics.
Demographics
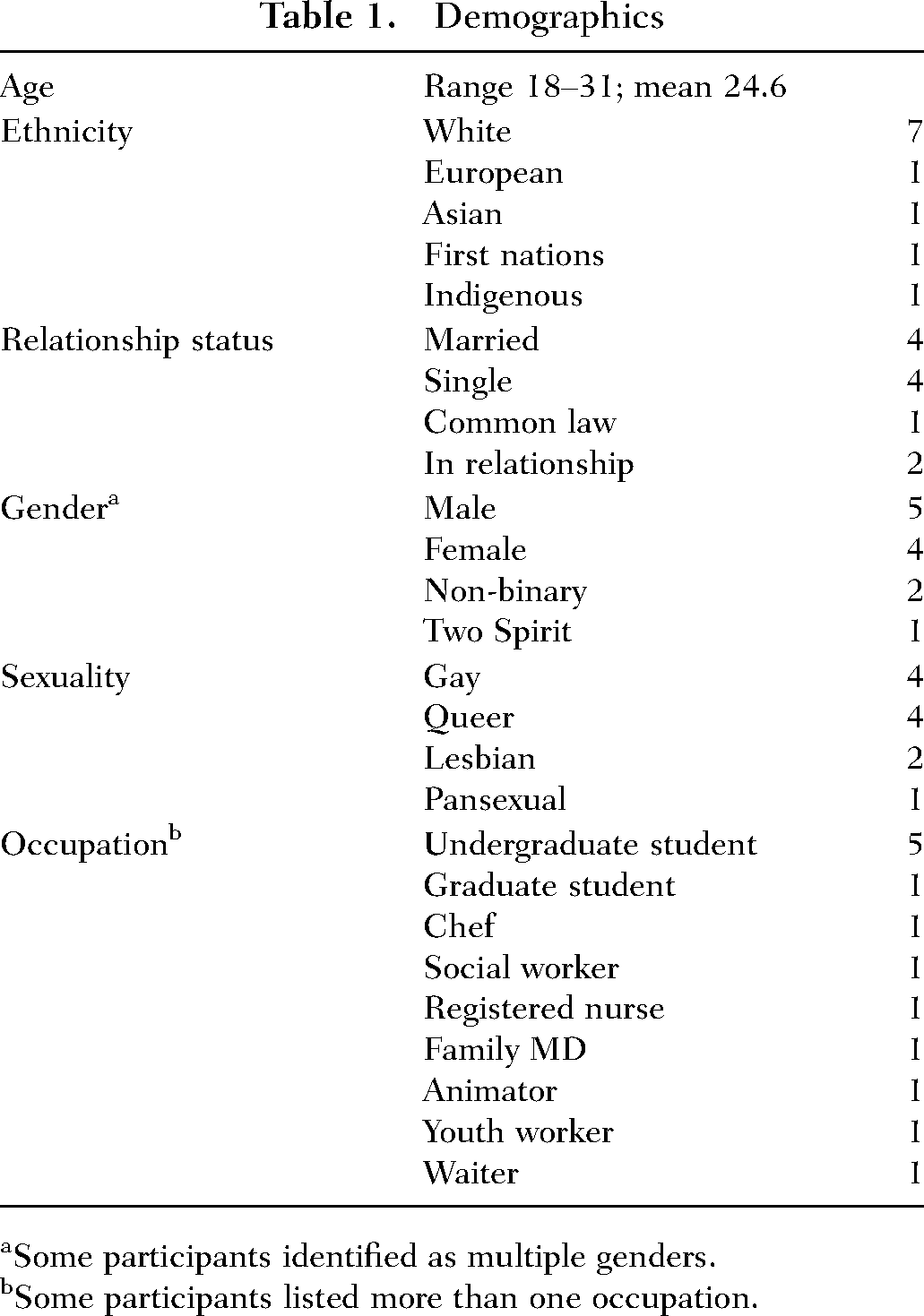
Some participants identified as multiple genders.
Some participants listed more than one occupation.
Data Collection
Data collection occurred virtually due to the COVID-19 pandemic from October 2020 to January 2021. KM completed nine semi-structured interviews with 11 participants (two group interviews), which is commensurate with the methodological framework. KM developed the interview questions that were approved by the research team. There was no participant attrition, and no participant requested that their data be removed. Interviews lasted 1 hour and 6 minutes on average. Six participants were in relationships with other participants (three couples, two couples interviewed together). Participants lived in two Canadian provinces and consisted of various genders, sexualities, relationship statuses, and ethnicities. Participants were given the option to use their name, choose a pseudonym, or contribute anonymously in order to provide opportunity for personal expression and comfort.
Data Analysis
The interviews were audio recorded and transcribed verbatim, and NVivo was used to code the transcripts inductively. KM analyzed the data using Braun and Clarke's (2006) six phase approach that includes becoming familiar with the data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and producing the report. After completing the first stage of data analysis, an interview summary was sent to each participant to review and provide feedback. Member checking was completed, and all participants responded that the summaries reflected the interview, their thoughts, and experiences. 3 Participants were able to provide additional information or clarify the summary in more depth at that time; two participants took the opportunity to expand on thoughts stemming from the summary.
Ethical Considerations
This study was granted ethical approval from the University of Saskatchewan before participant recruitment. All participants gave consent prior to the initiation of the interviews.
Results
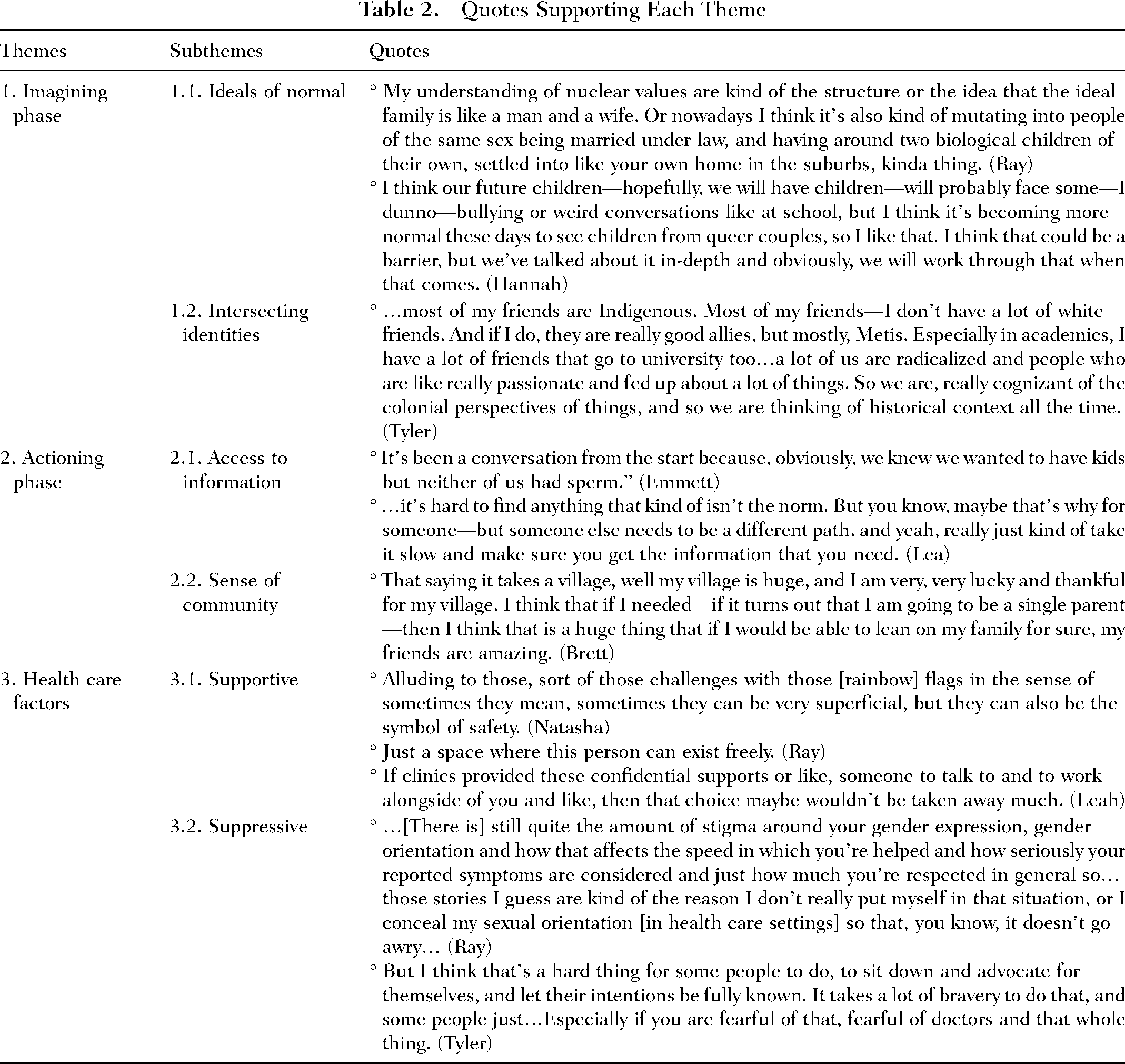
Participants discussed two phases of fertility intentions: (1) imagining fertility intentions (the hypothetical) and (2) actioning fertility intentions (the concrete). Within each phase, two themes arose, representing influential factors related to fertility intentions. In the imagining phase, fertility intentions were influenced by ideals of “normal” and intersections of identity, while in the actioning phase, participants identified that they were impacted by their access to information and community influence. During both phases, participants experienced suppressive and supportive factors within health care settings (Theme 3) that affected the intentionality of their decisions and increased their emotional labor. Regardless of their experiences, all participants expressed feeling hope for the future. See Table 2 for quotes supporting each theme.
Quotes Supporting Each Theme
Imagining Phase
Fertility intentions ranged broadly and included having biological children (either with gametes from them and their partner or from only one partner), adopting children, using donor gametes (known donor sperm or anonymous donor sperm), carrying the pregnancy themselves, using a surrogate, adopting, or step-parenting. Participants were open to different numbers of children—ranging from not wanting to birth their own children and adopting children to having one set of twins, to three or more. No participant had a set number of children they desired.
Participants made intentional decisions when it came to their family plans. Intentional decision-making ranged from why they chose specific ways to become parents, how they would want to raise their children, how society and their community would view their decisions, and making life decisions based on the possibility of being single parents: I guess maybe we will be more intentional in the way that we raise our kid knowing about queer people and thinking about gender and thinking about sexuality and thinking about race and racism and…I dunno I think we might be more intentional about that than maybe folks that aren’t in our position might be. (Sophie)
Ideals of Normal
Ideals of normal included what participants believe to be “normal” (overt or not) based on societal understandings and practices of the norm. Throughout the interviews, all participants casually languaged “normal,” while locating themselves outside of what is considered normal. Participants directly or indirectly referred to “the normal” people as those who were White, heterosexual, monogamous, and cisgender. All participants discussed the ways that the specter of “normal” impacts their individual and social experiences and further how this influences the 2SLGBTQ community's own expectations of normalcy: I guess I think that telling people about it, [my sexuality] they’re really weirded out because it's not what they expect—it's not the normal way for people to go, but I’m like I’m not going to be with a guy—I can’t go the normal way you guys want me to go. (Natasha)
The specter of “normal” affected the ways in which participants explored their fertility, as participants often saw themselves distinctly outside of the norm and compared themselves to people whom they considered normal, including their monosexual (attracted to only one gender), heterosexual, or cisgender peers. Alternatively, normative beliefs are internalized and can create challenges and barriers for participants to wholly participate in their fertility intentions: So, for the longest time, I was accustomed to think that “normal” was always part a male and a female, so, it was very hard to—even now I have to sometimes say normal—and that's like, but, no no no no no no. (Mason)
There was also discussion that some members of the 2SLGBTQ community were continually striving to fit within society's definition of normal. Participants explored that being a same-sex couple was accepted, celebrated, and normalized only if they lived the “normal” life—White, married, monogamous, and reproducing: …this is something that I have seen too, not in Two Spirit people but in gay people—especially White, gay males—they want to get married, and they want to like adopt a baby and everything, they wanna have—it's kind of like the gay ideal family structure. (Tyler)
Intersecting Identities
Participants explored intersecting parts of their identities that influenced their ideals of normal. These intersecting identities affected what they believed to be normal and how they experienced normal within the greater society. Most often, intersecting identities involved sexuality, gender, race, and culture. For most participants, intersections of identities influenced their fertility intentions through how they were raised, what they wanted to replicate, what had previously been represented, and what their capacity was. Some participants that already considered themselves outside of normal felt that having children may continually draw unwanted attention and lack of safety for being different: I don’t often hold hands out in public because we are afraid we are going to get attacked from some homophobia—we are just going to get insults thrown at us, and we wouldn’t have to deal with that if we were a straight couple. Even though it is a [straight] interracial couple it wouldn’t make as much of a difference as compared with two guys holding hands or gently kissing each other in public it [being in a gay and interracial relationship] is a bigger deal than it would be if it was a straight couple for sure. (Aaron) I think I’ve grappled [with] and I’ve seen other queer people or non-binary people and people like that and all sorts of people, and it [carrying a pregnancy] doesn’t have to be such a feminine thing. (Leah)
Actioning phase
Access to Information
Although all participants sought information from online sources, they discussed that finding trusted and accurate information specific to their specific needs based on location and intersecting identities was challenging: “…it's hard to find anything that kind of isn’t the norm” (Lea).
There was also a lack of clarity on accessing policies for members of the 2SLGBTQ community. For example, participants that were undergoing fertility treatments faced challenges finding specific protocols and policies for the 2SLGBTQ community and felt as though there was a lack of transparency within the clinics. This lack of transparency left participants feeling excluded, confused, and discriminated against: “I think the world is not set up for same-sex couples, I feel like there are barriers in conversation, there's barriers in policy, there's barriers, in like everything, really” (Hannah).
Sense of Community
Community was a supportive factor for all participants. Participants most frequently described other members of the 2SLGBTQ community with similar experiences as providing a supportive environment. For those who were imagining fertility intentions, supportive communities most often included those with similar intersecting identities, for example, similar sexual orientations—or the same or similar cultural backgrounds or understandings.
For participants moving toward actioning fertility intentions, supportive communities with experience of fertility action proved to be the most important. These supports included friends who had previous personal or work experience with fertility treatments, or strangers going through treatment processes. Some participants explained they had arranged Zoom meetings with friends of friends who had gone through the fertility process, or reached out to strangers through the internet, because they felt so lost: “Finding these Facebook groups where I’m just like—I’m just gonna message this random person, and I don’t care because I am so alone in this” (Hannah). Participants used these support groups to find others who were going through similar experiences and were then able to confide in them and to access support and information.
Individuals found reflective experiences of other members of the 2SLGBTQ community to be invaluable. Some participants explained that because of the information they found from others online, they would be much more likely to also share their story online, in hopes to support others, answer questions, and alleviate any undue stress: …there are a couple of like Facebook groups as well, about queer folks trying to conceive. And with some of the fertility clinics in [location] have Facebook groups which can be a bit of a nightmare but also helpful. You kind of have to weed through. (Sophie)
Health Care Factors
Suppressive Health Care
For some participants, barriers within health care made them feel discouraged and marginalized. For example, participants discussed the long wait times and intense planning related to any sort of decision around fertility: “Timing is really a choice that is taken away from us. So basically, we can start trying when we get to the top of the IVF waitlist” (Hannah). Some participants knew that the fertility journey took a long time and started almost 2 years before they wanted to conceive a child. A lack of autonomy and representation for participants often left them feeling hopeless and invisible. Of the participants who had experience within fertility-specific health care settings, four out of five felt that clinic policies did not represent any aspect of their identities and were heterosexist, transphobic, and ableist: …even though we knew that we weren’t going to use [my partners] eggs and that he didn’t have sperm to use they still made us fill out the “female” form for him that went through like menstrual history and pregnancy history and all of that. (Sophie)
For those participants who did not have fertility-specific health care experiences, accessing supportive health care services proved equally challenging. Concerns included how providers would treat participants if they knew they were in the 2SLGBTQ community, or whether they would be accidentally outed to providers. They feared that the care they received would be affected if they were outed, and this fear extended to the treatment of family, friends, and partners: …[there is] still quite the amount of stigma around your gender expression, gender orientation and how that affects the speed in which you’re helped and how seriously your reported symptoms are considered and just how much you’re respected in general. (Ray)
I think that we’ve got a long way to go in terms of being more diverse in terms of education. I don’t remember non-binary or transgender or any of those types of different identities or any other type of orientation [being touched on]. Because I’ve talked to my nursing friends about certain things, because [I am a part of the 2SLGBTQ] community I like to educate myself about that so I am usually the person to come to if you have any questions about that. (Brett)
Supportive Health Care
Only participants that had experiences with fertility-specific health care services discussed the supportive factors they experienced with providers. Most other participants did not have consistent providers or reported that their providers did not know or ask about their sexual orientation. My family doctor—she's amazing—and she really does take a holistic approach, looking at the whole person and looking at the physical side and also the mental and what really contributes to everything…and the reproductive clinic where I mean most of it will happen, they’ve been, they’ve been super inviting and friendly and super supportive and any questions I had they would answer right away. (Lea)
Hope for the Future
Participants explored having a sense of hope, even within the constraints of the health care system. This sense of hope coincided with imagining what supportive systems could look like. When asked about what contributed to feelings of safety in relation to providers and various spaces, some participants offered concrete suggestions—such as providers having 2SLGBTQ stickers or Indigenous art on the wall, or making spaces feel less sterile. Other participants described safe spaces more abstractly, indicating that it was based on an innate feeling where you “just know.”
Ultimately, participants discussed positive spaces where staff were friendly, open, accepting, kind, and were supportive of their journeys. Participants expressed simply wanting a space to feel normal: “it is nice to have it just feel normal. People are just educated in basic human rights I guess” (Emmett).
Discussion
In this study, we sought to learn more about the impact of heteronormativity and cisnormativity on the experiences of the 2SLGBTQ community related to fertility intentions and family planning. Findings demonstrated that in the “imagining phase” of fertility planning, both decisions and desires were shaped by societal ideals around what identities and experiences are considered “normal” within the fertility planning process. In the “actioning phase” of fertility planning, participants were influenced by access to information and a sense of community. Participants encountered supportive and suppressive factors from health care settings and providers that shaped their family planning experiences. However, regardless of barriers or suppressive factors, 2SLGBTQ community members continue to imagine and/or action their future fertility.
The findings from this study demonstrate the influence that heteronormativity and cisnormativity have on the family planning experiences of the 2SLGBTQ community. One may expect different findings considering this research included multiple identities within the 2SLGBTQ community in two Canadian provinces; however, in line with comparable research, experiences were similar. For example, studies that looked at queer women of color in the United States (Karpman et al., 2018), lesbian mothers in Poland (Mizielińska & Stasińska, 2019), and sexual and gender minorities in India (Bowling et al., 2019) all demonstrated the impact of heteronormativity and cisnormativity on fertility planning, including the impact of an underlying referent to what or who is “normal.” Together, these analyses demonstrate the role that heteronormativity and cisnormativity play in defining and dictating what is normal in health systems, while failing to account for those who do not fit into these norms.
The dominance of heteronormative and cisnormative ideologies is shown to be the result of a lack of 2SLGBTQ-specific reproductive education for providers and reproductive treatment protocols that privilege those who are heterosexual and cisgender (Tasker & Gato, 2020). Health care systems and providers may also perpetuate heteronormative and cisnormative ideologies as shown by experiences of trans individuals exploring surgery, hormones, and treatment options (Occhino & Skewes, 2020). In these cases, providers act as gatekeepers to treatment and perpetuate normative ideologies, transphobia, homophobia, and biphobia through dictating the most normal way to be (Occhino & Skewes, 2020). These examples highlight that, although there are more inclusive policies—for example, the Diagnostic and Statistical Manual, same-sex marriage legalization, and in vitro fertilization access—for the 2SLGBTQ community, many barriers to access persist. Also, although individual providers can be supportive toward members of the 2SLGBTQ community, they still face institutional barriers that are challenging to overcome.
The findings of this study may highlight the value of an intersectional analysis when exploring the effects of heteronormativity and cisnormativity, as intersectionality highlights the importance of understanding how some are privileged over others and how deeply entangled privilege and oppression are within the human experience (Lane, 2019; Mizielińska & Stasińska, 2019). Furthermore, intersectionality allows a deeper exploration when understanding the complexities of reproductive justice for the 2SLGBTQ community (Lane, 2019) and integrates the effect that complex social and political factors have on experiences (Mizielińska & Stasińska, 2019). Previous research parallels our findings where intersections of identities and ideals of normal form fertility intentions—regardless of race, sexuality, gender, and geographical location (Bowling et al., 2019; Karpman et al., 2018).
Additional research parallels our findings regarding the intentionality behind the decisions of the 2SLGBTQ community (Lane, 2019; Mizielińska & Stasińska, 2019; Tasker & Gato, 2020). Although a comparison of fertility intentions with cisgender and heterosexual participants was outside of our study's scope, Mizielińska and Stasińska (2019) discuss that members of the 2SLGBTQ community do experience additional barriers, oppressions, and intentional decision-making due to navigating stereotypes, discrimination, and non-normative parenting relationships compared with cisgender and heterosexual couples.
Intentional decision-making leads to emotional labor. Emotional labor is the “effort, planning, and control needed to express organizationally desired emotion during interpersonal interactions” (Morris & Feldman, 1996, p. 987). Emotional labor was expended by participants as they navigate systems of oppression, are forced to educate providers and members of the public, anticipate and overcome challenges, and make choices to fit within the confines of heteronormative and cisnormative expectations.
Berenstain (2016) uses the term epistemic exploitation to describe instances where those with privilege (for example, providers, heterosexual, and cisgender people) hold power to exploit emotional labor from marginalized groups. This exploitation is accomplished by requiring the community impacted to explain the oppressions they face (Berenstain, 2016). In our study, participants explained their participation in epistemic exploitation through requirements to explain their identities and experiences to providers, friends, and family, navigating how they wanted to be seen and witnessed within health care systems and—more broadly—within society. Alongside such expectations, not only do heteronormativity and cisnormativity impact experiences within highly gendered areas of health care, but also the effect of normative ideologies also increases the emotional labor of the 2SLGBTQ community.
Considering that 2SLGBTQ-specific information on fertility planning is available but that it can be challenging to find relevant information, the lived experience of other members of the 2SLGBTQ provides a promising resource for those navigating the health system. Strong kinship patterns already exist within the 2SLGBTQ community, because of many relying on chosen family over families of origin (Jackson Levin et al., 2020). Connecting with other 2SLGBTQ people while navigating the medical system provides much needed support, mentorship, and resource sharing. The provision of peer supports or peer navigators could be a resource that clinics explore further, if they are seeking to better support 2SLGBTQ people.
Limitations
The initial literature review may be limited by the diverse labeling of the 2SLGBTQ community within research and community settings, which could mean literature was missed. This study was also limited in its diversity of participants. Although participants represented different races, cultures, genders, and sexual identities, many participants were White students, and no participant discussed having disabilities. Given the nature and goals of qualitative research, the findings are not generalizable to the greater public; however, the research does provide a valuable exploration of experiences that could prove useful to various health care settings and practitioners.
Implications for Practice
When approaching health from a holistic critical social justice lens, nursing as a discipline can challenge the normative nature of current health care practices by discussing the need for diversity and culturally appropriate nursing care. Also, nursing can advocate for more inclusive spaces to validate patient existence and experiences (Searle et al., 2017). Understanding how health is influenced by gender and sexuality, not only at the individual level, but also organizationally and structurally, is essential in providing holistic care for members of the 2SLGBTQ community.
Conclusion
The experiences of the 2SLGBTQ community related to fertility intentions and family planning are nuanced, complex, and influenced by a variety of intervening factors. Societal understandings of what is normal in relation to gender and sexuality dictate these experiences and create additional barriers for the 2SLGBTQ community. As such, barriers exist not only in highly gendered areas of health care but affect the everyday lived experiences of 2SLGBTQ people outside of health care. When it comes to family planning, the decisions made by the 2SLGBTQ community are often more intentional than those outside the community and thus require additional emotional labor in an area that is already emotionally charged. Increased awareness about the experiences of 2SLGBTQ people within family planning and fertility intervention landscapes will help to improve health care experiences and to challenge normative ideologies surrounding gender and sexuality, especially as they negatively impact 2SLGBTQ people.
Supplemental Material
sj-docx-1-jhn-10.1177_08980101231189653 - Supplemental material for Exploring the Impacts of Heteronormative and Cisnormative Ideologies on Fertility Intentions and Family Planning Experiences Within the 2SLGBTQ Community: A Qualitative Case Study
Supplemental material, sj-docx-1-jhn-10.1177_08980101231189653 for Exploring the Impacts of Heteronormative and Cisnormative Ideologies on Fertility Intentions and Family Planning Experiences Within the 2SLGBTQ Community: A Qualitative Case Study by Kerry Marshall, Wanda Martin, Rachel Loewen Walker and Helen Vandenberg in Journal of Holistic Nursing
Footnotes
Ethical Statement
Ethics was obtained by the University of Saskatchewan Research Ethics Board BEH #1862 before participant recruitment.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.