
Abstract
Background and Significance
Burnout among healthcare workers has been recognized for many years, but there is a scarcity of research on how to combat the problem in nursing. Burnout can be defined as the physical, emotional, and mental enervation caused by stressful work environments (Hassanzade Daloee et al., 2020). Importantly, the U.S. Bureau of Labor and Statistics estimates that there is a great shortage in the nursing workforce, with a need for approximately 275,000 nurses between 2020 and 2030 (Haddad & Toney-Butler, 2022). Stressful work environments with the COVID-19 pandemic compounded with the shortage of nurses in the US have likely made the situation even more critical. Therefore, it is important to understand ways to mitigate the impact of burnout on healthcare providers, especially in the acute care setting and improve the well-being of the nursing workforce.
Burnout is increasing at an alarming rate among all healthcare professionals, but especially in nursing (Reith, 2018). In a sample of 1,688 nurses from the National Academies of Medicine, 54% of the sample reported experiencing some degree of burnout with 28% experiencing high levels (Kelly et al., 2020). Burnout has been directly linked to mental health problems (including anxiety and posttraumatic stress disorder), medication errors, poor patient outcomes, and higher rates of turnover in the acute care setting (Moss et al., 2016; Pastores et al., 2019). Furthermore, increased burnout among nurses is associated with an increased intention to leave the profession (Van der Heijden et al., 2019). National rates of nursing turnover range from 8.8% to 37.0%, depending on location and specialty (Haddad & Toney-Butler, 2022). In areas such as oncology and critical care (emergency medicine and Intensive Care [ICU] settings), nursing providers are at an increased risk for burnout (Duarte & Pinto-Gouveia, 2017; Kerlin et al., 2020). Importantly, high levels of burnout syndrome are commonplace among nurse practitioners working as intensivists in the ICU (Pastores et al., 2019). In a cross-sectional study of nurses in Belgium, researchers found that ICU and emergency department nurses had increased rates of reported burnout prior to the pandemic (69.8% and 51.2%, respectively; Butera et al., 2021). In the same study, emergency nurse's reported burnout stayed relatively stable during the first peak of the pandemic, reaching 70.7%. However, ICU nurses reported burnout increased dramatically to 66.7% (Butera et al., 2021).
Resilience, or the ability of an individual to “bounce back” in the face of adversity, stress, or trauma, is an important factor in understanding burnout (APA, 2004). Resilience may help individuals cope with many of the negative attributes of burnout. Resilience is a skill that can be fostered through practicing self-care and promoting personal well-being (Bender & Ingram, 2018). However, nurses may neglect taking care of their own well-being (Ross et al., 2017). Furthermore, without first taking care of themselves, providers may be less equipped to properly care for their patients (Hofmeyer et al., 2020).
Several strategies can improve the well-being of healthcare workers including mindfulness-based stress reduction (MBSR), cognitive behavioral therapy (CBT), and mindfulness (Fadaei et al., 2020; Ghawadra et al., 2019; Pender, 1987; Penque, 2019). Meditation, and specifically practices of mindfulness, focus on teaching patience, openness, and acceptance with a unique appreciation for the present moment (Gilmartin et al., 2017). Practices of intentional self-care, such as mindfulness, are key components of holistic nursing care (ANA & AHNA, 2019). Practices of mindfulness have been shown to improve levels of anxiety and depression among nurses (Ghawadra et al., 2019). In a nonrandomized experimental study of 48 oncology nurses, researchers found that an intervention group receiving abbreviated MBSR showed marked decreases in burnout and stress and increases in mindfulness, satisfaction with life, and self-compassion (Duarte & Pinto-Gouveia, 2016). In a RCT of 110 nurses in a general hospital, a MBSR intervention group showed decreases in stress and negative affect, and an increase in resilience and positive affect (Lin et al., 2019). Similarly, researchers have found that an eight-week MBSR program significantly reduced perceived stress and increased mindfulness among critical care nursing staff (Anderson, 2021). MBSR interventions also provide benefits to patient outcomes (Daigle et al., 2018). Given these positive findings, a mindfulness-based intervention could be beneficial for acute care nursing settings.
Recent technology teaches mindfulness using smartphone applications (e.g. Headspace, Insight Timer, and Calm). This specific delivery method often requires minimal amounts of time to practice mindfulness, which may be more amenable to nursing staff compared to traditional MBSR or CBT programs (Gilmartin et al., 2017). A brief intervention, such as Headspace or Insight Timer (a mindfulness-based smartphone application), can take as little as 5 minutes a day. In fact, among a sample of pediatric acute care nurses, researchers found that a meditation smartphone application was superior to traditional mindfulness exercises (in-person MBSR program) in reducing burnout (Morrison Wylde et al., 2017). However, there are few studies on brief mindfulness interventions (e.g. 5 minutes a day for 30 days) for nursing staff (Van der Riet et al., 2018). Therefore, smartphone-based mindfulness applications may further enhance a nurse's ability to improve their mindfulness and resilience, potentially resulting in decreasing levels of stress and burnout.
Interventions that can promote well-being by decreasing stress and burnout should be incorporated as integral to holistic nursing practice. Holistic nursing is a practice that focuses on “healing the whole person” (AHNA, 1998). This type of healing is focused on improving the relationship with the individual instead of focusing on the cures of specific diseases (ANA & AHNA, 2019). Mindfulness practices, which may promote self-care and may reduce many of the negative mental health attributes seen in acute care nurses, should continue to be an essential component of holistic nursing.
Theoretical Framework
The Mindfulness to Meaning Theory (Garland et al., 2015) is a relatively new theory that describes the impact of mindfulness training on psychological well-being. Importantly, practices of mindfulness are a key component of holistic nursing (ANA & AHNA, 2019). According to this theory, the utilization of mindfulness may promote mental well-being in the face of stress and trauma. Furthermore, when individuals can detach themselves from stressful situations (by practicing mindfulness), they are able to see alternative information that they may have overlooked previously. Individuals will then be able to reframe their thoughts, which will help reduce their overall distress and increase positive emotions (Garland et al., 2015). Mindfulness practices have been shown to improve positive emotions in everyday life by developing an awareness and acceptance of the present moment (Lindsay et al., 2018). Additionally, an increase in positive emotion may help to overcome and alleviate burnout (Sexton & Adair, 2019). An intervention that may increase these positive psychological states may be useful to fields, such as nursing, which are facing increasing rates of stress and burnout.
Given that the Mindfulness to Meaning Theory is a relatively new theoretical framework, another theory was used to help guide this research study. Pender's Health Promotional Model is a theoretical framework that focuses on factors that determine if individuals will participate in health promoting activities (Pender, 1987). Pender (1987) defined health as a positive state of well-being; not just being free from disease. Factors that influence whether individuals will take part in an intervention that improves their health and well-being include intrinsic factors (personal factors, perceived barriers, or self-efficacy), extrinsic factors (situational or interpersonal influences), and health-promoting behaviors (Pender, 1987). This model also makes clear that individuals are more likely to engage in health-promoting behaviors if they believe they will benefit from the behavior (Pender, 1987). For this project, the introductory educational session prior to the intervention was important in showing participants how this specific health-promoting behavior could improve their mental health and well-being. Additionally, the utilization of a mindfulness-based intervention is one way to support well-being through health-promoting behaviors. Mindfulness is a behavior that can be learned, and mindfulness may help promote self-care. According to Pender (1987), self-care is a core principle in creating holistic health and well-being. Therefore, an intervention that focuses on mindfulness meditation for individuals, especially those in high-stress environments, may be beneficial in improving the overall mental health and well-being of participants.
Purpose and Objectives
Given the limited studies utilizing mindfulness-based smartphone applications to combat burnout among nursing staff, the purpose of this study was to determine if a brief mindfulness-based smartphone application (5 minutes/day via Headspace or Insight Timer) could be used to address burnout among nursing staff in an acute care setting. Specifically, among acute care nursing staff, the aims of this study were to determine the effect of a brief mindfulness-based smartphone application on:
Burnout and stress scores and Resilience and mindfulness scores.
Methods
Design and Setting
This pilot project utilized a pre–post quasi-experimental design, with a midpoint evaluation. The participants consisted of nursing staff from cardiac progressive/acute care and cardiac ICUs from an academic medical center.
Sample
A convenient sample was obtained from the cardiovascular service line at a large academic medical center (ICU/Progressive/Acute). Nurses, nursing care technicians, nurse managers and advanced practice providers were eligible for inclusion in the study.
Intervention and Ethical Considerations
The entire intervention was delivered from October 2021 to January 2022. Participants were informed that their responses would not be shared and would remain anonymous. Institutional Review Board (IRB) approval was obtained through the University and the Hospital Nursing Research Council. Prior to providing informed consent and beginning the pre-survey, study subjects were sent a brief prerecorded online seminar via a YouTube link. The seminar covered information on the importance of meditation, how it relates to their practice, data from previous research on meditation, and information on how mindfulness can benefit their patients and their own well-being. An example of a meditation practice was demonstrated during this prerecorded seminar. Study subjects were informed that they could drop out or choose not to participate at any time. Participants agreeing to take part in the study then filled out a consent form and pre-survey. Although participants were invited to participate via email, their responses were de-identified within a Qualtrics survey software program to maintain confidentiality.
At the end of the pre-survey, participants were prompted to download the free version of Headspace or Insight Timer. Those who downloaded Headspace used the “Basics” module, which has 10 meditations in each course. Once they reached the 10th session in the 1st course, they would restart with day one, then complete the same course two more times. Participants who downloaded Insight Timer chose between two 5-minute guided meditations: “5 Minute Presence” by Felix New or “5 Minute Grounding Awareness” by Natalie Bondine. To increase compliance, daily notifications from Headspace/Insight Timer were sent to participants via the application.
For 30 consecutive days, participants were asked to spend 5 minutes per day using the mindfulness-based smartphone application while at work or at home. Participants were emailed the midpoint evaluation survey at the 15-day mark, and the post-survey at 30 days. Participants entered a code prior to each survey to allow for linking the surveys over time, while maintaining participant anonymity. At each testing point, participants completed an online survey via Qualtrics that included rating scales to assess our main outcomes. Descriptive data collected post-intervention included perceived barriers and facilitators of the 5-minute meditation, average time spent meditating each day, total time spent meditating during the study, and total number of days spent meditating (these data were collected by participants from the Apple Health application or the Headspace/Insight Timer application). After completion of the final survey, they could follow a link to another anonymous Qualtrics survey for a chance to win a $50 gift card.
Measures
Demographics
The Qualtrics survey asked respondents to self-report their age, years of nursing experience, sex, race, previous meditation experience, job title, and unit.
Scales
The Copenhagen Burnout Inventory is a 19-item tool that measures personal, work-related, and client-related burnout. Each subscale is calculated as the mean score of the items within, with potential ranges of 1 (Always/To a very high degree) to 5 (Never/To a very low degree); with higher scores reflecting lower degrees of burnout. It is important to note that the last four items on the work-related CBI were reverse-scored.
The Perceived Stress Scale-4 is a brief scale that measures stress. This assessment tool utilizes a Likert scale of 0–4 per item (Never to Very often). A summary score was calculated ranging from 0 to 16, with higher scores reflecting increased stress levels.
The Brief Resilience Scale is a five-question assessment tool that measures resilience. This questionnaire utilizes a Likert scale with values ranging from 1 to 5 (strongly disagree to strongly agree). Responses are summed and the total is divided by the number of questions answered. Total scores can range from 6 to 30, with higher scores representing greater resilience.
The Cognitive and Affective Mindfulness Scale-Revised is a 10-item scale that measures trait and/or dispositional mindfulness. A summary score was calculated. The fifth item is reverse scored. Each question uses a Likert scale with potential ranges from 1 to 4 (Rarely/not at all to Almost always). Total scores can range from 13 to 36, with a higher value representing greater mindfulness qualities.
Each of these scales was utilized for the pre–post and midpoint survey, via Qualtrics. All scales have demonstrated validity and reliability in prior studies (Feldman et al., 2006; Fung, 2020; Karam et al., 2012; Riley et al., 2018).
Data Analysis
Of 33 individuals initially enrolled in the study, 31 fully completed the pre-survey. However, only 16 individuals completed the midpoint evaluation, and eight completed the entire study. Descriptive statistics (mean and standard deviation or frequency distribution) were used to summarize participant characteristics. Repeated measures analysis of variance was used to assess changes over time for the main outcomes. Both groups in the study (Headspace and Insight Timer) were combined in the data analysis. All analysis was completed using SPSS, version 28 with an alpha of .05 used to determine significant findings.
Results
Sample Description
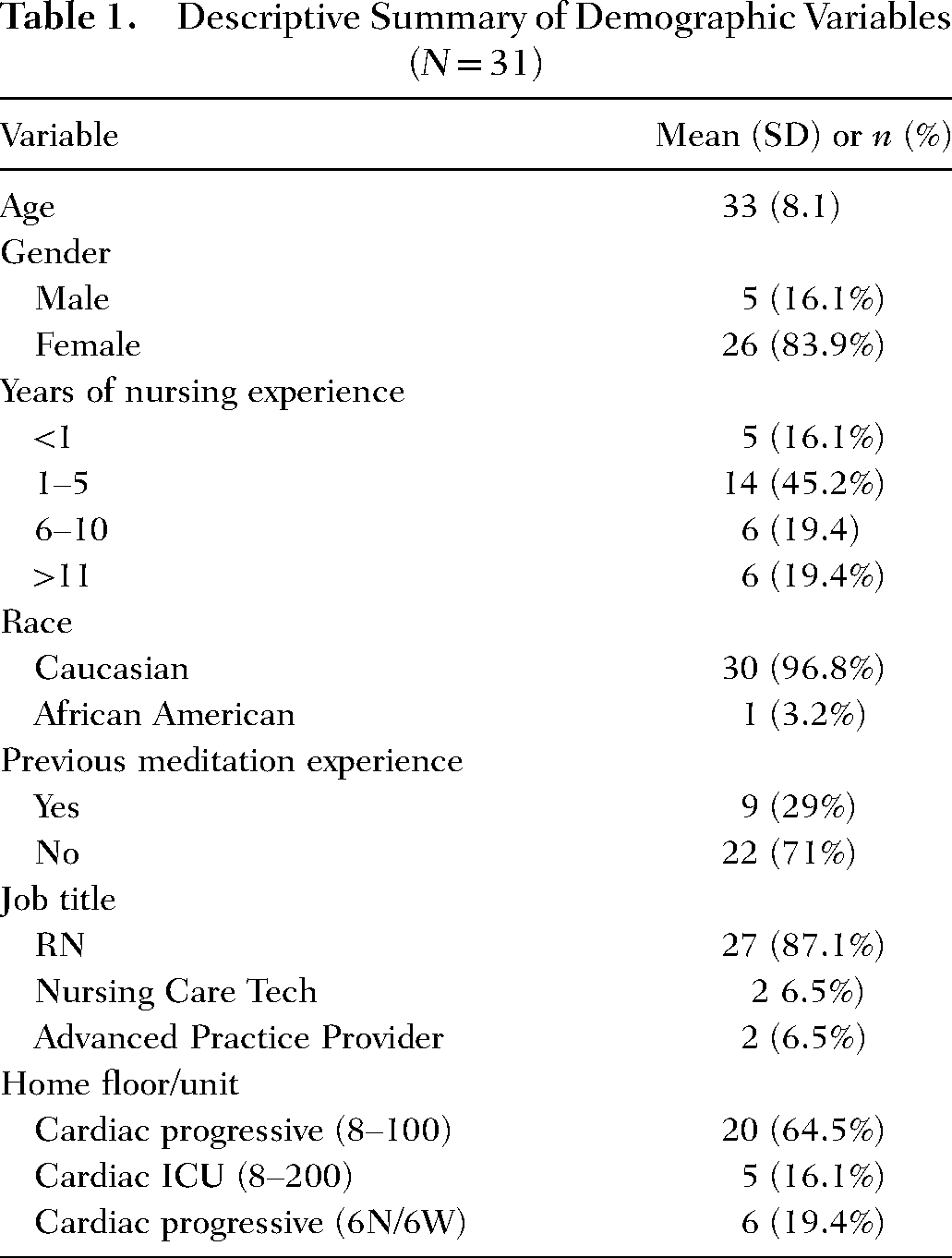
The average age of participants was 33 years (SD = 8.1) and ranged from 22 to 49 years. A majority of the sample was female (83.9%) and Caucasian (96.8%). More than half of the sample (61.3%) had less than five years of nursing experience. Nearly three-quarters of participants had no previous meditation experience (71%). The majority were nurses (87.1%) followed by nursing care technicians (6.5%), and advanced practice providers (6.5%). Most of the nursing staff worked on cardiac progressive/acute floors (83.9%) while the rest worked in the cardiac ICU (16.1%; see Table 1). On average, participants reported practicing the intervention for 18 days, with a range of 4–28 days. Additionally, participants reported their total time practicing meditation, which ranged from 20 to 360 min for the entire study period, with an average of 149 min.
Descriptive Summary of Demographic Variables (N = 31)
Changes in Burnout Scores
For personal burnout, there were statistically significant changes over time (F = 11.80, df = 1.10, p = .007), with higher scores representing lower burnout. There was a statistically significant decrease in personal burnout from baseline (M = 2.43, SE = 0.18) to both midpoint (M = 3.15, SE = 0.19, p < .001) and follow-up (M = 3.46, SE = 0.27, p = .004; see Figure 1). Scores did not differ from midpoint to follow-up. However, there were no statistically significant changes among work- (F = 2.69, df = 1.30, p = .126) or client-related (F = 3.83, df = 1.40, p = .067) burnout scores across the three timeframes (see Table 2).
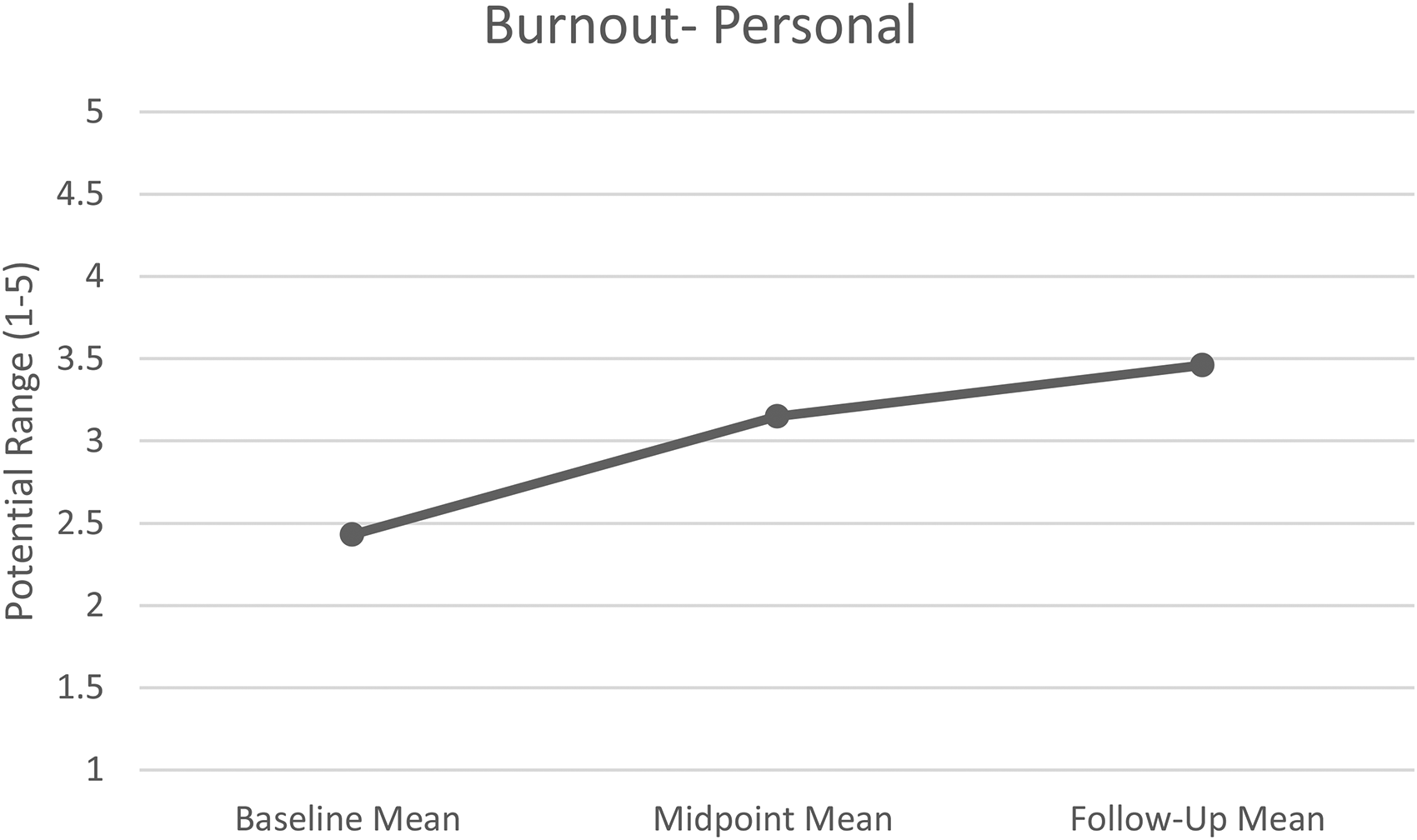
Repeated measures analysis of personal burnout scores over time.
Repeated Measures Analysis of Outcomes Over Time
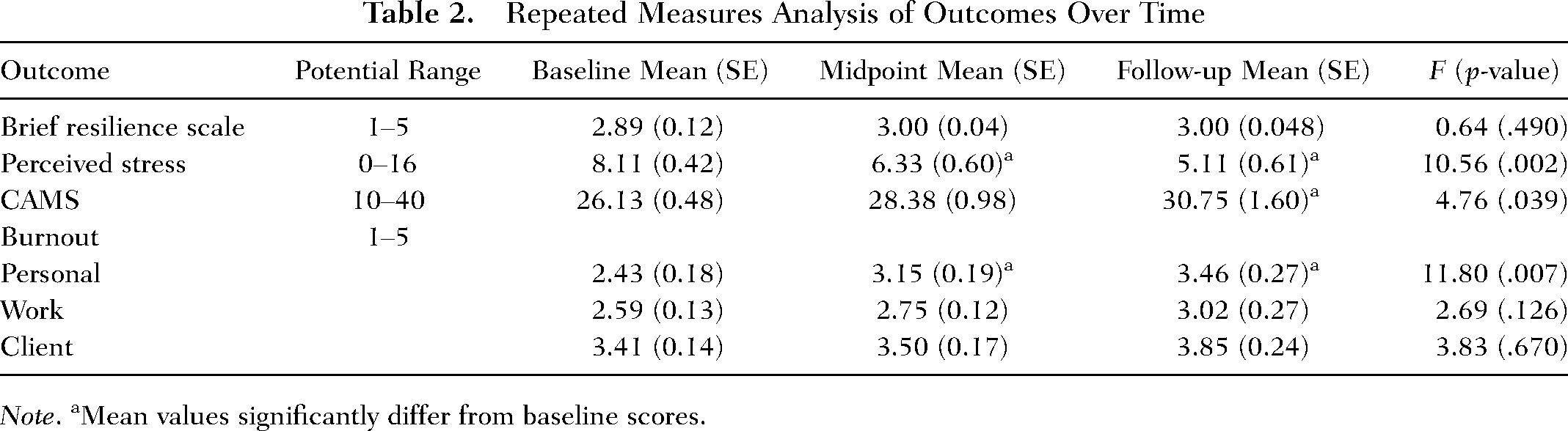
Note. aMean values significantly differ from baseline scores.
Changes in Perceived Stress Scores
For the PSS-4, there were statistically significant changes over time (F = 10.56, df = 1.74, p = .002). There was a statistically significant decrease in stress from baseline (M = 8.11, SE = 0.42) to the midpoint (M = 6.33, SE = 0.60, p = .009) and follow-up evaluation (M = 5.11, SE = 0.61, p = .002; see Figure 2). Scores for stress did not significantly differ from midpoint to follow-up assessments (see Table 2).
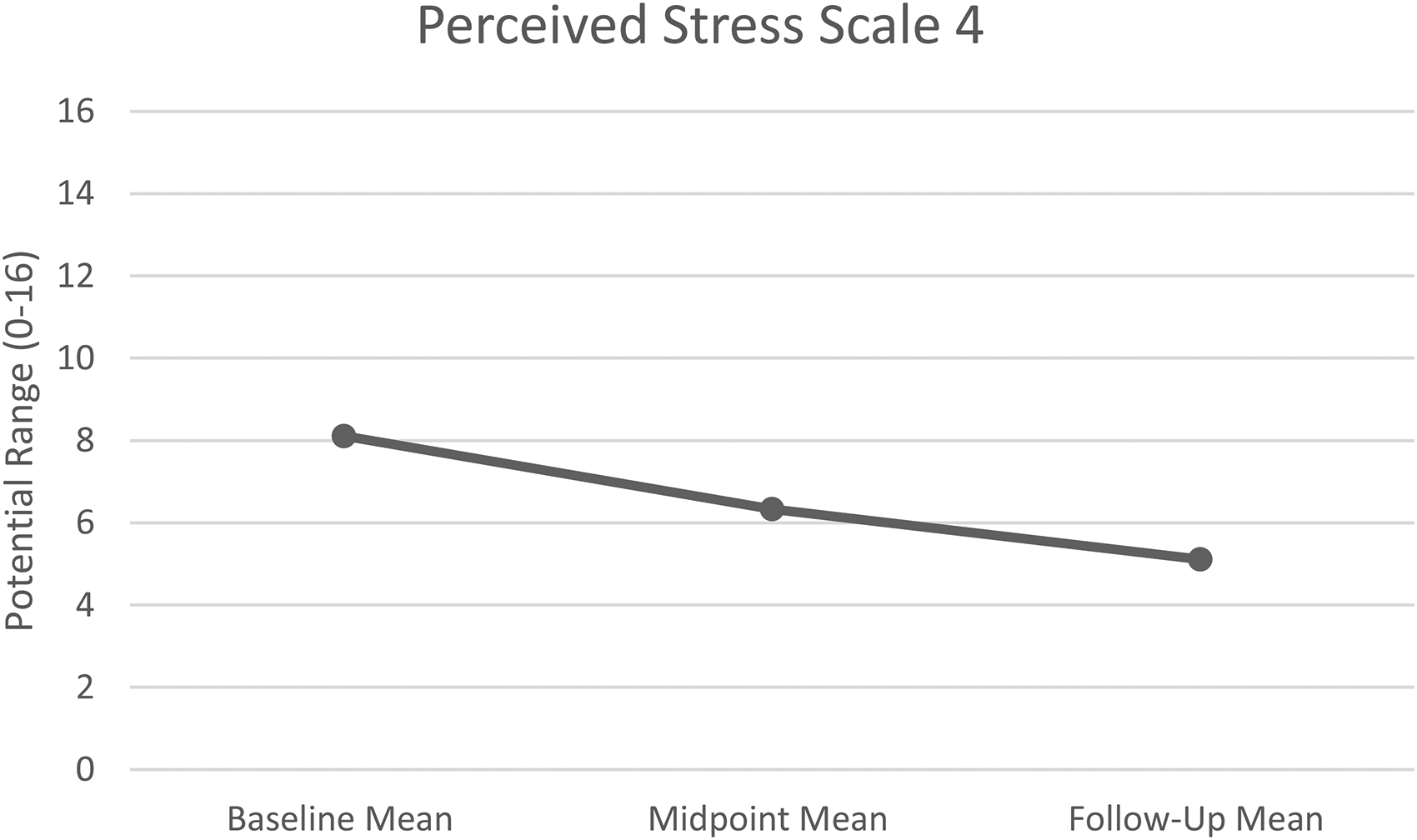
Repeated measures analysis of perceived stress scores over time.
Changes in Resilience Scores
In the repeated measures analysis, there were no significant changes in scores from the BRS across the three timeframes (F = 0.64, df = 1.42, p = .490) (see Table 2).
Changes in Mindfulness Scores
There was a statistically significant change in mindfulness scores across time (F = 4.76, df = 1.57, p = .039). Scores significantly increased from baseline (M = 26.13, SE = 0.48) to follow-up (M = 30.75, SE = 1.60, p = .039; see Figure 3). Mindfulness scores did not differ between baseline to midpoint or midpoint to follow-up assessments (see Table 2).
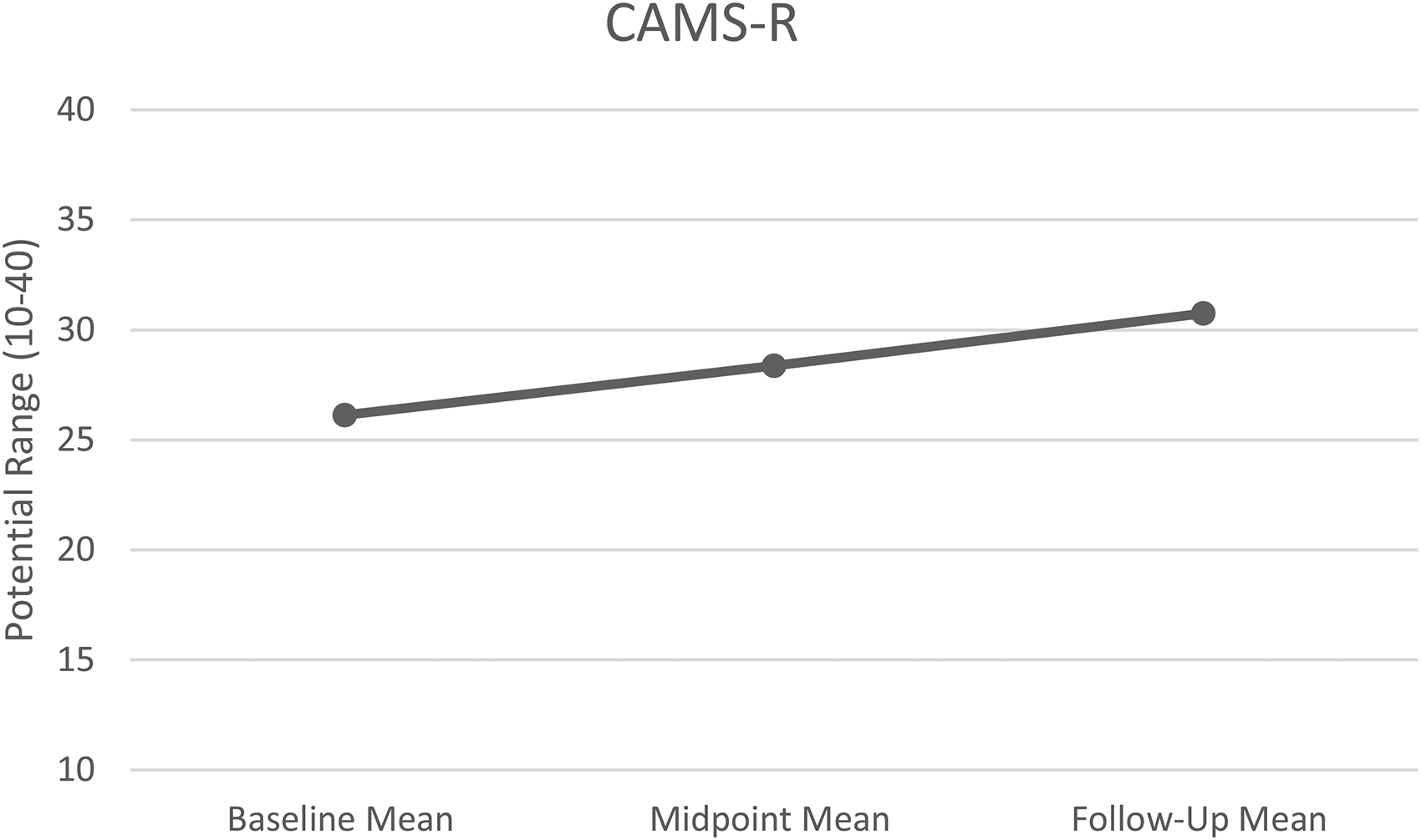
Repeated measures analysis of mindfulness scores over time.
Discussion
The purpose of this study was to determine the impact of a brief mindfulness-based smartphone application on burnout, stress, resilience, and mindfulness in acute care nursing staff. Individuals who participated in the intervention had significantly decreased levels of reported personal burnout and stress compared to pre-intervention levels. Additionally, those who participated in the intervention reported increased levels of mindfulness from pre- to post-intervention. But no differences were observed in resilience. These findings have important implications for future studies on the impact of mindfulness-based stress reduction techniques for nursing staff.
Similar to our current findings, previous research has demonstrated that brief mindfulness interventions can positively impact perceived stress, mindfulness, and well-being (Champion et al., 2019; Wen et al., 2017; Yang et al., 2018). While there were no significant changes in resilience scores from the intervention in our current study, previous findings have shown that mindfulness-based applications can improve perceived stress and resilience in the general population (Champion et al., 2019). Future studies may be needed to determine how mindfulness-based applications may be adapted to improve resilience in nurses. It may be beneficial for nurses to develop these types of self-care practices on a regular basis, and not only in times of crisis. Additionally, we should consider training our nursing students early in their education on ways to utilize holistic practices of self-care, such as mindfulness and meditation. Initiating practices of self-care earlier in one's career could potentially reduce their risk of developing burnout after entering the workforce.
Limitations
There are clear limitations to this study. First, the COVID-19 pandemic continues to place a strain on the healthcare workforce. Even with a monetary incentive, participants were likely unable to add anything “extra” to their daily schedules. In post hoc qualitative responses from participants regarding the use of the mindfulness-based applications, time was the most cited barrier for not practicing the meditation intervention each day. Participants felt that even 5 minutes/day was a large amount of time to dedicate to their mental health and well-being. Other studies have mentioned adherence as a barrier, especially for mindfulness practices, such as MBSR, which require an even greater time commitment (Gilmartin et al., 2017). This suggests that retention of subjects may be a problem in studies with longer interventions.
Additionally, the study had a high attrition rate. Only 8 participants out of 33 (24.0%) completed the study. This high attrition may appear to compromise the acceptability and feasibility of the study. To reduce such attrition in future studies, it would be important to provide staff with incentives (e.g. monetary, gift cards) or other forms of contingency management to improve retention. Such incentive approaches may also encourage the participants to use the tool for the recommended durations and potentially enhance the effectiveness outcomes. Therefore, future studies employing incentives with larger sample sizes may be considered to better assess the acceptability, feasibility, and effectiveness of such a study.
Trusting that participants meditated each day and were adhering to the intervention is another clear limitation of this study. The application sent a daily notification as a way to improve compliance. Receiving a daily notification was noted to be a facilitator of the intervention in the post-survey qualitative response data.
Another limitation of this study was the use of two different mindfulness-based smartphone applications: Headspace and Insight Timer. The free version of the Headspace application unexpectedly timed out two weeks into the first cohort. A free voucher was obtained through Headspace for those in the first cohort to continue using the application for the remainder of the first study period. Therefore, participants in the second cohort had to use Insight Timer instead. This change in protocol was considered acceptable given that Insight Timer is still a mindfulness-based smartphone application, and participants could choose from two 5-minute meditations.
Having different nursing units in this study also may have been a limitation. This is really a site-specific barrier because different units may have differing patient acuities. However, this was necessary in an attempt to increase the total sample size. It is important to note that all but one of the participants who fully completed the study were from the same unit. The limited sample size (in both number and homogeneity) precludes generalizing the results of this project to other populations.
Implications for Future Nursing Research
There is a clear need for holistic interventions to reduce stress and burnout among those in the nursing workforce. As the acuity of our patients in the acute care setting continues to rise, our nursing workforce is struggling to maintain their own mental health and well-being. Given that nurses may neglect the practice of self-care, strategies to highlight the importance of holistic nursing practices need to be addressed in the research (Ross et al., 2017). Modeling intentional self-care as providers is a fundamental practice in holistic nursing (ANA & AHNA, 2019). It may also be important to assess how modeling these behaviors can benefit our patients. Research in this area may allow us to understand how our patients can integrate practices of self-care into their own lives. This could potentially have positive implications for the mental well-being of the patients that we serve.
Future research may include objective measurements from participants such as cortisol levels and blood pressure. These are more specific parameters that may provide objective assessments of the effect of brief mindfulness-based interventions on nursing staff in addition to self-report measures. It would be important for future studies to assess the impact of a brief mindfulness-based smartphone intervention on a larger sample of nursing staff. Future research in this area may include samples from across different nursing sub-specialties to improve the generalizability of findings. Additionally, focusing on other healthcare professionals, especially those in critical care settings, because they are at an increased risk for burnout (Kerlin et al., 2020). Although this study had a small sample size, we can conclude that a brief mindfulness-based smartphone intervention may have a positive impact on burnout, mindfulness, and stress among nursing staff in an acute care setting. Therefore, future studies could expand the brief mindfulness-based smartphone interventions to other healthcare professionals at risk of experiencing burnout and stress.
Given that our sample was small, it is hard to infer the specific amount of time needed for a mindfulness-based intervention to be “effective.” Seeing that participants would likely not meditate every day; it would be important to recommend that participants attempt to meditate every day. Total time meditating during the study ranged from 20 to 360 min, so this varied widely across the sample. Future research may examine the specific impact of different times (5 min vs. 10 min, etc.) on the well-being of nursing staff. This may provide direction on a specific amount of time needed for individuals to reap the benefits of practicing a mindfulness-based intervention.
Conclusion
Understanding the impact of brief mindfulness-based interventions for acute care nursing staff remains an important topic, especially given the COVID-19 pandemic. The findings of this study suggest that a brief mindfulness-based intervention may be effective in reducing burnout and perceived stress, while increasing levels of mindfulness. Addressing strategies that nursing staff can utilize to adhere to these types of interventions will be important in future studies. While mindfulness-based interventions are important to consider, this is only one of many holistic strategies that could be used to improve the well-being of the nursing workforce. Decreasing the rates of stress and burnout among nursing staff will enhance the well-being of the nursing workforce, which may have implications on nurse retention and patient outcomes.
Footnotes
Acknowledgements
Amanda Wiggins, PhD