
Abstract
Introduction
Appendectomy has been the gold standard for treating acute appendicitis for over 120 years (Lee et al., 2021; Writing Group for the CODA Collaborative, 2022). Acute appendicitis is the most prevalent cause of acute emergency abdomen, potentially causing 7% to 10% of patients to undergo appendectomy (Gazerani et al., 2021; Obsa et al., 2020). Approximately 17.7 million individuals were diagnosed with acute appendicitis in 2019 (Wickramasinghe et al., 2021). Appendectomy significantly increases postoperative pain (Taheri et al., 2019). In the postoperative phase, pain is inevitable, making it a terrible and distressing experience. Even with painkillers and sedatives, postoperative pain remains a global problem that is yet to be completely resolved (Hoogervorst-Schilp et al., 2016; Kapikiran et al., 2022).
Health professionals play a crucial role in the management of individualized and cultural pain to improve patient physiology (Herr et al., 2019; Rosa, 2018) and ameliorate pain severity (Moon et al., 2021). Previous studies have indicated that 30%, 30%, and 40% of patients experience mild, moderate, and severe postoperative pain severity, respectively (Adib-Hajbaghery et al., 2012). Typically, postoperative pain persists for approximately 24 to 48 hr (Garimella & Cellini, 2013). Pain examinations were conducted concurrently with vital signs, including pulse, respiratory rate, and oxygen saturation (Mularski et al., 2006). Continuous measurement and monitoring of vital signs have been suggested as possible methods to ensure the consistent and early detection of deterioration (Douglas, 1999; Downey et al., 2018). Therefore, identifying postoperative pain, vital signs, and their functions after appendectomy is necessary for a better understanding of transcultural pain management.
Dhikr therapy is a noninvasive spiritual relaxation treatment that manifests as an individual's religious commitment (Nasiri et al., 2015). Dhikr refers to the practice of remembering Allah, which is based on meditation and can be performed individually or collectively (Saniotis, 2018). Previous studies have revealed that dhikr significantly reduces pain severity in women in labor (Mualimah et al., 2020) and acute coronary syndrome (Pangestika et al., 2020). Previous randomized controlled trials have demonstrated that dhikr significantly improves pulse, respiratory rate, and oxygen saturation in patients after coronary artery bypass graft surgery (Nasiri et al., 2015). However, the effects of dhikr on pain and vital signs in patients undergoing appendectomies have not been widely explored.
In line with dhikr, prayer is a cognitive and behavioral method based on finding meaning in life and overcoming obstacles, especially health-related problems (Simão et al., 2016). A systematic review suggested that prayer, as spiritual therapy, should be utilized in holistic nursing patient care to reduce psychological problems and escalate physical functioning (Simão et al., 2016). Interestingly, patients who experience pain often use different cognitive and behavioral methods to deal with their pain, such as praying and looking for spiritual support (Dedeli & Kaptan, 2013). This highlights the fact that dhikr, together with prayer, may have a positive effect on reducing pain and improving vital signs in patients undergoing an appendectomy. However, an explanation of these interactions is required.
Therefore, we conducted a quasi-experimental study to investigate the effects of dhikr combined with prayer, which may positively reduce pain and improve vital signs in patients undergoing appendectomy. This study aimed to assess whether dhikr, together with prayer, could positively reduce pain as a primary outcome and improve pulse, respiratory rate, and oxygen saturation as secondary outcomes in appendectomy patients.
Method
Study Design
A quasi-experimental design was used in this study. The experimental design utilized an equivalent control group pretest and posttest design with repeated measures.
Participants
Participants were recruited using convenience sampling from an educational hospital in Purwokerto, Central Java, Indonesia, from June 11, 2022, to October 29, 2022. Patients diagnosed with appendicitis who underwent appendectomy with acetylsalicylic acid I or II, who were Muslim, aged 21 to 60 years, and without a history of drug addiction, whose surgeries lasted less than an hour, and who exhibited no evidence of nasogastric tube were considered eligible to participate. The exclusion criteria were participants who had auditory deficiencies and other chronic or acute diseases and who refused to participate in the study.
To determine the sample size, a power analysis was conducted using G*Power Version 3.1.2, with a power sample of 0.95, an effect size of 0.50, and a significance level of 5% (Faul et al., 2007). According to these calculations, a sample size of 73 patients was determined, with 37 patients in each group. We calculated an attrition rate of 20% and increased the sample size of each group to 44 participants.
Intervention and Control Groups
A 2-min introduction to the dhikr and prayer therapy, a 10-min dhikr treatment, and an 8-min prayer were provided in three cycles within 1 hr of the trial period. The dhikr and prayer treatments were performed using an MP3 player with headphones (Sonic Gear Airphone 5). Respondents received an MP3 player with headphones, instructions on how to implement the dhikr and prayer treatment, and a recorded dhikr and prayer (du'a) for their usual pain management regimen.
The procedure for dhikr therapy is as follows: (a) The patient believes that dhikr can calm the heart, thus improving their health by, for example, alleviating pain; (b) the body position of the patient: the patient lies in accordance with the situation; (c) the researchers encourage respondents to close their eyes and breathe deeply. The patient takes a slow, deep breath to fill their lungs with air, holds their breath for approximately 5 s, then exhales slowly; (d) As the patient gently relaxes their breath, the patient utters the word “Allah” and visualizes all the diseases and negative emotions leaving their body and mind; (e) Patients recite different dhikr words using the same method, such as “Astaghfirullahal'adzim,” “Subhanallah,” “Laailaaha illallah,” and “Laa hawala walaa kuwwat illa billah” (three times). Patients say dhikr according to their expectations and ask for health from God by saying: “Yaa Syaafi,” “Yaa Salaam,” “Yaa Rohman,” “Yaa Rohiim,” “Astagfirullah,” “Alhamdulillah”; “Bismillahi” (three times); and “A'uudzubillahi wa qudrotihi min syarrimaa ajidu wa uhadziruu” (seven times).
The prayers (du’a) of the patients are done by listening to the Quran and Surah, including “Ta'awudz,” “Basmallah,” “Hamdallah,” and “Syahadat.” Moreover, the patient listens to Du'a and asks for the good of life (consequently reducing their pain) by saying (translated to English): (a) “Allah set my religion right for me, which is the safeguard of my affairs. Set the experiences of my world where I live right for me. Put my future right for me, on which depends my after-life. Make my life (a source) abundant for all good and make my death a source of comfort for me, protecting me against every evil”; (b) “In the name of Allah, the Almighty. I seek comfort in Allah the Highest from wounds and the spectacle of hell's fire”; and (c) “Glory be to Allah, and all praise is due to Allah; I confidently say that there is no god other than Allah; I seek Your pardon and repentance alone”.
For the control group, the researchers encouraged the respondents to close their eyes and breathe deeply. Subsequently, the patient takes a slow, deep breath to fill their lungs with air, holds their breath for approximately 5 s, and then exhales slowly.
Data Collection
The researcher and research assistant conducted face-to-face data collection with the participants. Once a patient agreed to participate in the study, the research assistant reported their information to a clinical nurse, who subsequently allocated the patients to the aforementioned groups based on an opaque and sealed envelope containing the identifiers assigned to each participant in the order of their entry into the trial. Given the nature of the intervention, it was impossible to blind the individuals. Data containing questions regarding the demographic characteristics of the participants were collected at baseline and included their age, sex, marital status, job, income, and educational level. We primarily measured pain, pulse rate, respiratory rate, and oxygen saturation. Data were collected three times: immediately after leaving the recovery room, and 1 and 2 hr after surgery for both the experimental and control groups.
Assessment of Outcomes
The data collection tool consisted of a three-part questionnaire that contained demographic data, a visual analog scale (VAS) for pain, and a form to collect information on physiological parameters. A 10-point VAS was used to assess pain as a standard self-report instrument. The possible pain intensity scores ranged from 0 to 10 (no pain to extreme pain and the worst pain). The reliability and validity of the VAS have been demonstrated for acute pain (Bijur et al., 2001) and implemented in appendectomy patients (Kim et al., 2021; Taheri et al., 2019). Heart rate, respiratory rate, and blood oxygen percentage were evaluated as physiological parameters using a portable fingertip pulse oximeter (LED CE 0413; OXIMETER).
Study Fidelity and Measurements of Incidence of Adverse Events
Study fidelity was established through meetings with investigators, enumerators, and physicians to review protocols, check proficiency measurements, and equalize perceptions during the intervention. During the intervention, the enumerators monitored the participants’ use of the MP3s containing dhikr and prayer. The incidence of adverse events in the intervention group was assessed during the study period. Potential adverse events, such as hearing problems, were monitored every 30 min and documented by clinical nurses. In the event of side effects, physicians and investigators immediately discontinued the intervention. No adverse events were observed during the intervention period.
Statistical Analyses
SPSS (version 25.0; Chicago, IL, USA) was employed for statistical analysis, and a p-value of .05 was evaluated as statistically significant. Mean (standard deviation) and n (%) were calculated to identify continuous and categorical data, respectively. Chi-square and one-way analyses of variance were used to compare the sociodemographic and baseline characteristics of the groups, respectively. Adjustments were made for potential confounding variables using generalized estimating equation models with appropriate link functions and distribution assumptions to assess differential changes in outcomes over time and between groups. At follow-up T2, missing data (n = 1; patient refused to participate in the intervention group) were presumed to be randomly missing, and the data were analyzed using the intention-to-treat approach.
Ethical Considerations
This study was approved by the Institutional Review Board of Prof. Dr. Margono Soekarjo Hospital (IRB Number 420/06031/2022). All participants provided written informed consent and the confidentiality of their information was ensured. Participant agreement forms were collected after the researcher described the goals of the study and ensured data confidentiality. The suppressed encoding of the name of each participant ensured anonymity.
Results
The baseline sociodemographic characteristics of the participants are presented in Table 1. The mean ages were 50.64 years for the study group and 53.86 years for the control group. No statistically significant differences (p > .05) were noted between the two groups in sociodemographic or clinical characteristics including age, sex, marital status, education, income, and employment status.
Comparisons of the Sociodemographic and Clinical Data of the Participants According to Their Group
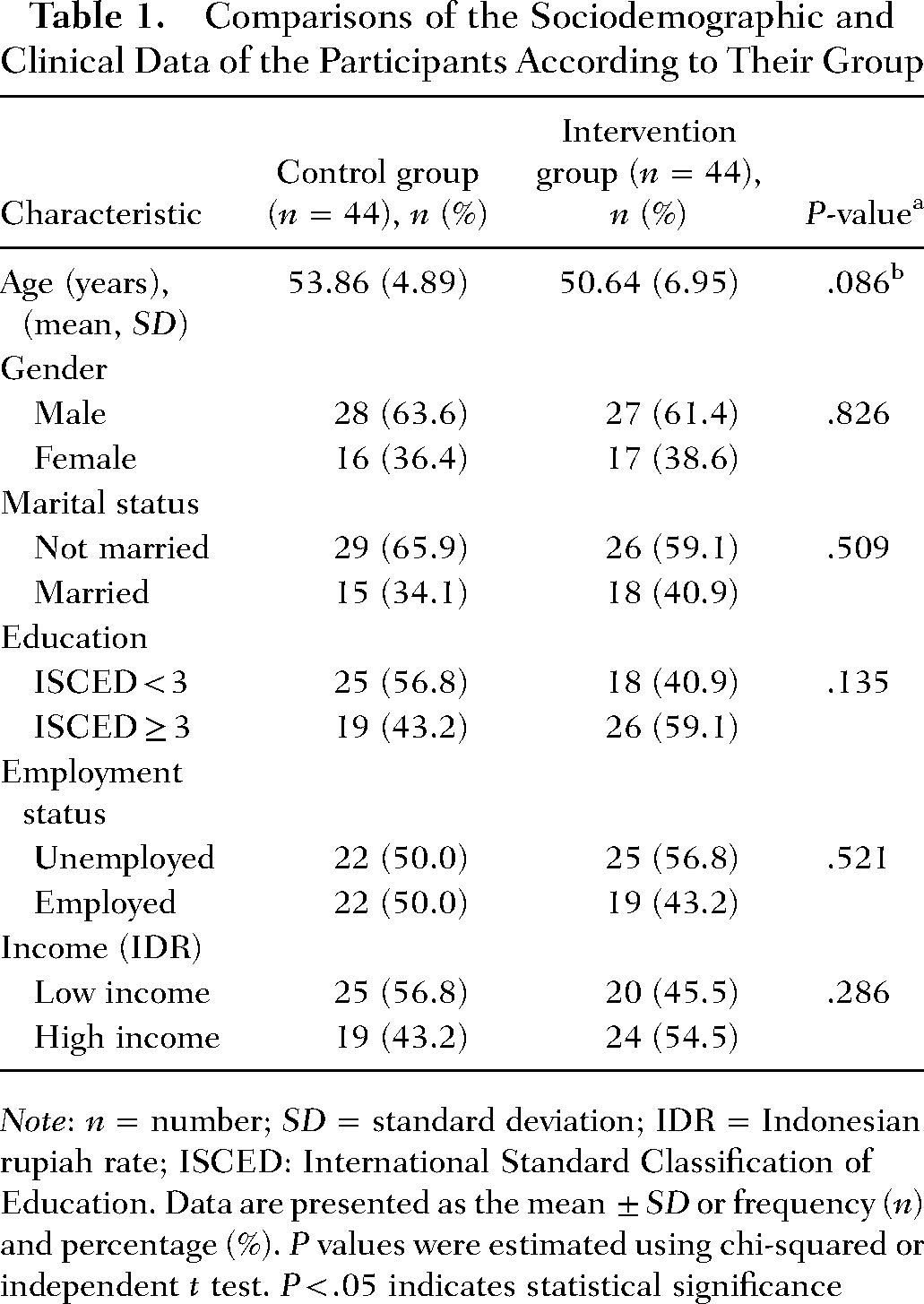
Note: n = number; SD = standard deviation; IDR = Indonesian rupiah rate; ISCED: International Standard Classification of Education. Data are presented as the mean ± SD or frequency (n) and percentage (%). P values were estimated using chi-squared or independent t test. P < .05 indicates statistical significance
The pain, pulse, respiratory rate, and oxygen saturation scores before and after the intervention are presented in Table 2. Participants in the control and intervention groups had lower pain, pulse, and respiratory rate scores, and an increased oxygen saturation score.
Pain, Pulse, Respiratory Rate, and Oxygen Saturation Before and After the Intervention
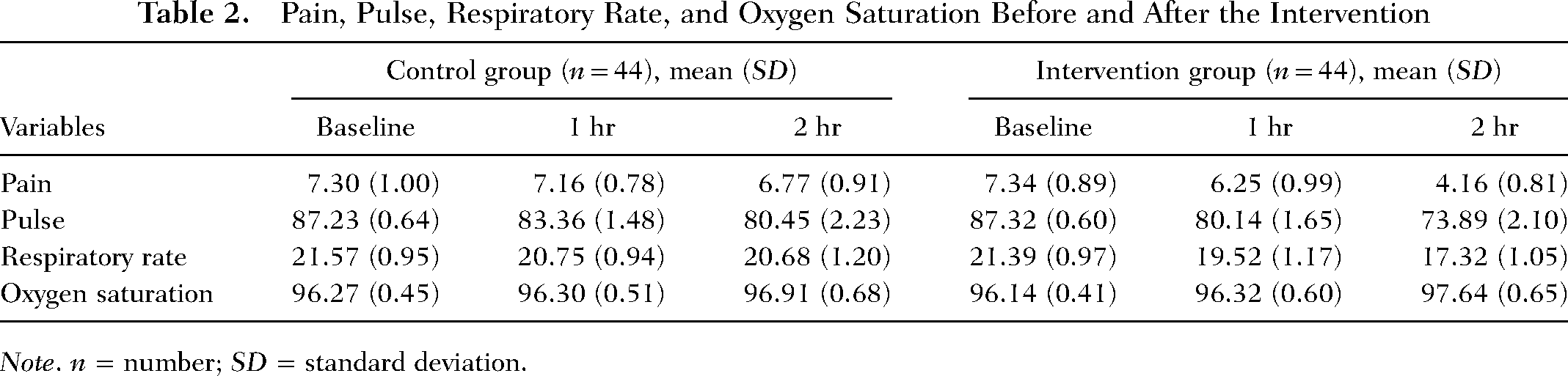
Note. n = number; SD = standard deviation.
A comparison of the measured outcomes, such as pain, pulse, respiratory rate, and oxygen saturation between the groups is shown in Table 3. The differences in pain (p = .820), pulse rate (p = .488), respiratory rate (p = .369), and oxygen saturation (p = .133) between the groups at baseline were not statistically significant. In the control group, there was a substantial decline in pulse and respiratory rates after 1 and 2 hr, respectively. However, no significant decrease in pain was observed after 1 ht. Interestingly, respondents showed a significant interaction between the group and time to escalated oxygen saturation, except for pain within 1 hr. The intervention had a significant effect on pain, pulse, and respiratory rate, indicating that the decline in the intervention group was significantly higher than that in the control group. Pain scores decreased significantly over time in both the control and intervention groups. Moreover, a significant difference was observed between the groups after 2 hr of oxygen saturation.
Effect of the Combination of Dhikr and Prayer Therapy on Pain, Pulse, Respiratory Rate, and Oxygen Saturation
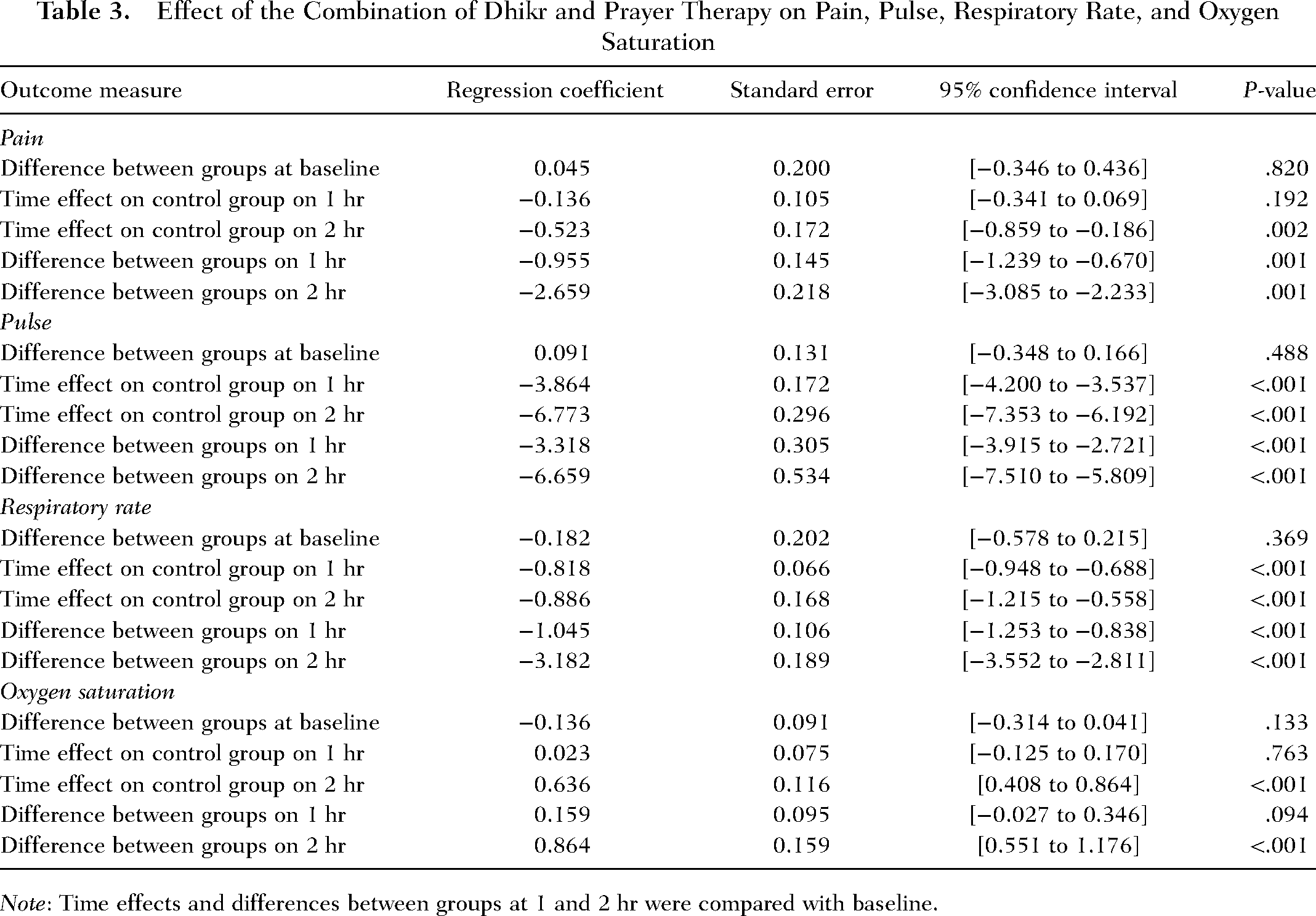
Note: Time effects and differences between groups at 1 and 2 hr were compared with baseline.
Discussion
This finding revealed that a novel treatment involving a combination of listening to the recitation of the dhikr and prayer therapy decreased pain and improved vital signs in patients undergoing appendectomy after 1 and 2 hr.
A previous study demonstrated that dhikr significantly reduced pain in patients with the acute coronary syndrome (Pangestika et al., 2020), operation reduction, internal fixation reduction during surgery (Misnawati & Ropyanto, 2015), and abdominal surgery (Soliman & Mohamed, 2013). Dhikr is a mind–body therapy that enhances psychophysical health and stimulates the immune system (Saniotis, 2018). Furthermore, dhikr can purify the heart of negative attitudes and emotions, increase physical and spiritual energy, and stimulate the spirit of life (Soliman & Mohamed, 2013). Literally, prayer as spiritual healing means calling upon, supplicating, and asking for good life and health (Ahsan et al., 2012). Prayer appears to be an integral aspect of the transition between states of health and illness and the promotion of well-being (Esperandio & Ladd, 2015). Remarkably, prayer enables emotional compatibility with pain by transforming feelings of fear and discomfort into comfort, trust, hope, and optimism (Asadzandi, 2019). Prayer significantly reduces pain among labor women (Kocak et al., 2022) and cholecystectomy patients (Maarof et al., 2022). A possible mechanism for the synergistic effect of dhikr and prayer might be the effects of feeling relaxed on the stimulated neurotransmitters: serotonin, melatonin, and endorphins. Prayer may alter the neural control of pituitary hormone release by increasing endorphins in the hypothalamus and inhibiting glutamate-aminobutyric acid in the central nervous system by focusing on Allah and increasing serotonin and melatonin production (Elvina et al., 2020; Kongsuwan & Chatchawet, 2019). Serotonin plays a critical role in the analgesic mesolimbic pathway and is closely associated with melatonin (Haleem, 2018). Furthermore, melatonin depresses the central nervous system and mediates global regulatory changes to decrease pain (Xie et al., 2020). This mechanism may provide substantial insights into the pathways that influence pain in patients undergoing appendectomy.
Our findings also support our second hypothesis that respondents showed a significant interaction between group and time to decrease in pain, pulse, respiratory rate, and improved oxygen saturation, except for pain within 1 hr. The differences in all outcome scores between the groups after 1 and 2 hr were statistically significant, except for oxygen saturation after 1 hr. This highlights that spiritual relaxation, such as dhikr and prayer, may positively reduce clinical damage due to improved pulse rate, respiratory rate, and oxygen saturation. A qualitative study demonstrated that dhikr could effectively increase feelings of peace, happiness, and meaningfulness (Subandi et al., 2022). Moreover, a randomized control study revealed that dhikr significantly improved the pulse, respiratory rate, and oxygen saturation (Nikbakht Nasrabadi et al., 2005). In the relevant literature, an individual listening to prayer with headphones via an MP3 player significantly escalated their oxygen saturation levels and decreased pulse and respiratory rates in intensive care unit patients (Mansouri et al., 2017). Interestingly, dhikr and prayer may increase delta brainwave signals, indicating decreased breathing frequency and increased melatonin levels (Fauzan & Rahim, 2015). Melatonin can increase oxygen saturation, reduce oxidative stress (Kruk et al., 2021), and improve pulse and respiratory rates (Uchendu et al., 2022). Consequently, these mechanisms may provide significant insights into the pathways that regulate vital signs, including pulse, respiratory rate, and oxygen saturation, in appendectomy patients.
However, our study has some limitations. First, dhikr and prayer therapy can only be implemented for Muslims. Thus, it cannot be used for any other religion or belief. Second, larger sample sizes should be available for future studies considering mental health problems, such as anxiety, stress, and depression, which impact pain and vital signs. Third, the majority of enrolled participants were male; consequently, the generalizability of our results may be limited.
Conclusion
This study showed that listening to the recitation of dhikr and prayer after appendicectomy reduced pain and improved the vital signs of patients. As a result of a more comfortable and helpful postappendectomy experience, together with an increase in the use of nonpharmacological methods, it is hoped that nurses and other health professionals will have more accessible spiritual treatments and that their pharmacological demands will decrease. Spiritually supporting appendectomy patients with a combination of dhikr and prayer helped nurses implement this procedure with renewed hope and promoted essential spiritual care as part of nursing care.
Footnotes
Author contributions
Arif Imam Hidayat contributed to the conception, investigation, analysis, acquisition, interpretation, drafting, critical revision, final correction, and final approval of the manuscript. Iwan Purnawan contributed to the conception, investigation, acquisition, interpretation, drafting, critical revision, final correction, and final approval of the manuscript. Wahyudi Mulyaningrat contributed to the conception, investigation, design, analysis, and interpretation, drafted the manuscript, critically revised the manuscript, and provided final approval. Adiratna Sekar Siwi contributed to the conception, drafted the manuscript, critically revised the manuscript, and gave the final approval. Saryono Saryono contributed to the conception, interpretation, and investigation, critically revised the manuscript, and approved the final version. Yohanes Andy Rias contributed to the conception, interpretation, and analysis, critically revised the manuscript, final correction, and approved the final version. Ferry Efendi contributed to the interpretation and analysis, critically revised the manuscript, final corrections, and approved the final version. Finally, all authors agreed to be fully accountable for ensuring the integrity and accuracy of the work and have read and approved the final manuscript before submission.
Data Availability Statement
All data generated or analyzed in this study are included in the published article. The datasets of this study are not publicly available owing to confidential restraints on the information of the participants.