
Abstract
Background
Heart disease is the number one cause of death in the world. Globally, 80% of deaths from coronary heart disease occur in developing countries (Benjamin et al., 2017). Cardiac surgery as a form of heart disease intervention was 6.7% of all interventions performed (Bonow et al., 2011). Coronary Artery Bypass Graft (CABG) is the most common surgical procedure in cardiac surgery, with an incidence of more than 72.2% compared to other types of surgery in cardiac surgery (Sun et al., 2021). Each perioperative stage has specific physical and psychological problems (Awaludin et al., 2022).
Anxiety is a problem that most often occurs in the pre-operative stage of cardiac surgery, including CABG. Eighty percent have pre-operative CABG anxiety, and the level of anxiety will continue to increase when entering the early intra-operative phase (Rahimianfar et al., 2013). Patients feel anxiety because they do not know for sure what will happen during cardiac surgery and fear of death. Intense anxiety risks causing non-adaptive behavior change responses (Ramesh et al., 2015). Anxiety is an uncomfortable feeling caused by unknown events, including the upcoming CABG surgery that can cause discomfort in the intervention and interfere with the subsequent recovery process, so intervention must be carried out (Prado-Olivares & Chover-Sierra, 2019). One of intervention that nurses can carry out is combined complementary therapy. The American Holistic Nurses Association (AHNA) recommends that nurses promote nonpharmacological interventions for anxiety.
Prayer can provide positive emotions that can affect the modulation process so that it stimulates endorphins that cause relaxation it can reduce pain and anxiety (Awaludin et al., 2022, 2020; Bartkowski et al., 2017; Sadati et al., 2021). The prayer that is read is a request for a smooth operation and healing.
Data show that patients who received pre-operative education had less emotional distress, improved physical and psychological recovery, and experienced fewer episodes of post-operative hypertension (Hardin & Kaplow, 2019). Education before surgery can reduce major pre-operative anxiety (Ng et al., 2022). The combination of prayer therapy and education is expected to synergize in reducing pre-operative coronary bypass graft anxiety. This study aimed to investigate the effect of combination prayer therapy and education on anxiety in patient pre-operative coronary bypass graft.
Methods
Study Design
A true-experimental design was carried out with pre- and post-intervention measurements of two groups namely the intervention group and the control group. The intervention group received a combination of prayer therapy and education, while the control group received standard therapy that is usually done in hospitals, the control group received a combination of prayer therapy and education after the second measurement as a standard post-intervention.
Participants
Consecutive sampling was used. This sampling technique is the best technique of the non-probability sampling method in controlling sampling bias because it includes all available subjects. In this research, consecutive sampling provides insight into the number of patients who are eligible (allows calculation of response rates) and allows use of clinical information, in addition this sampling technique provides insight into the number of patients who may be willing to use POIs, allows calculation of accurate response rates, and provide an opportunity for health professionals to support interventions that can increase credibility (Thewes et al., 2018). In this study, the consecutive sampling technique was very suitable, the stages were carried out by selecting samples that met the inclusion criteria and had been randomly allocated as a condition for true experimental research, so the respondents could be taken sequentially until the expected sample size was met. This sampling technique includes all respondents who meet the inclusion criteria. Respondents were recruited as a sample when the respondent had entered the preoperative ward. The sample size is 50 respondents. Twenty-five patients were allocated to each group. (See Figure 1 for a consort flow diagram of the two groups). The inclusion criteria for this study were respondents aged 20–75 years, willing to be respondents, good hearing function, able to read and write, did not have surgery complicating factors, while the exclusion criteria were patients experiencing the worsening condition.
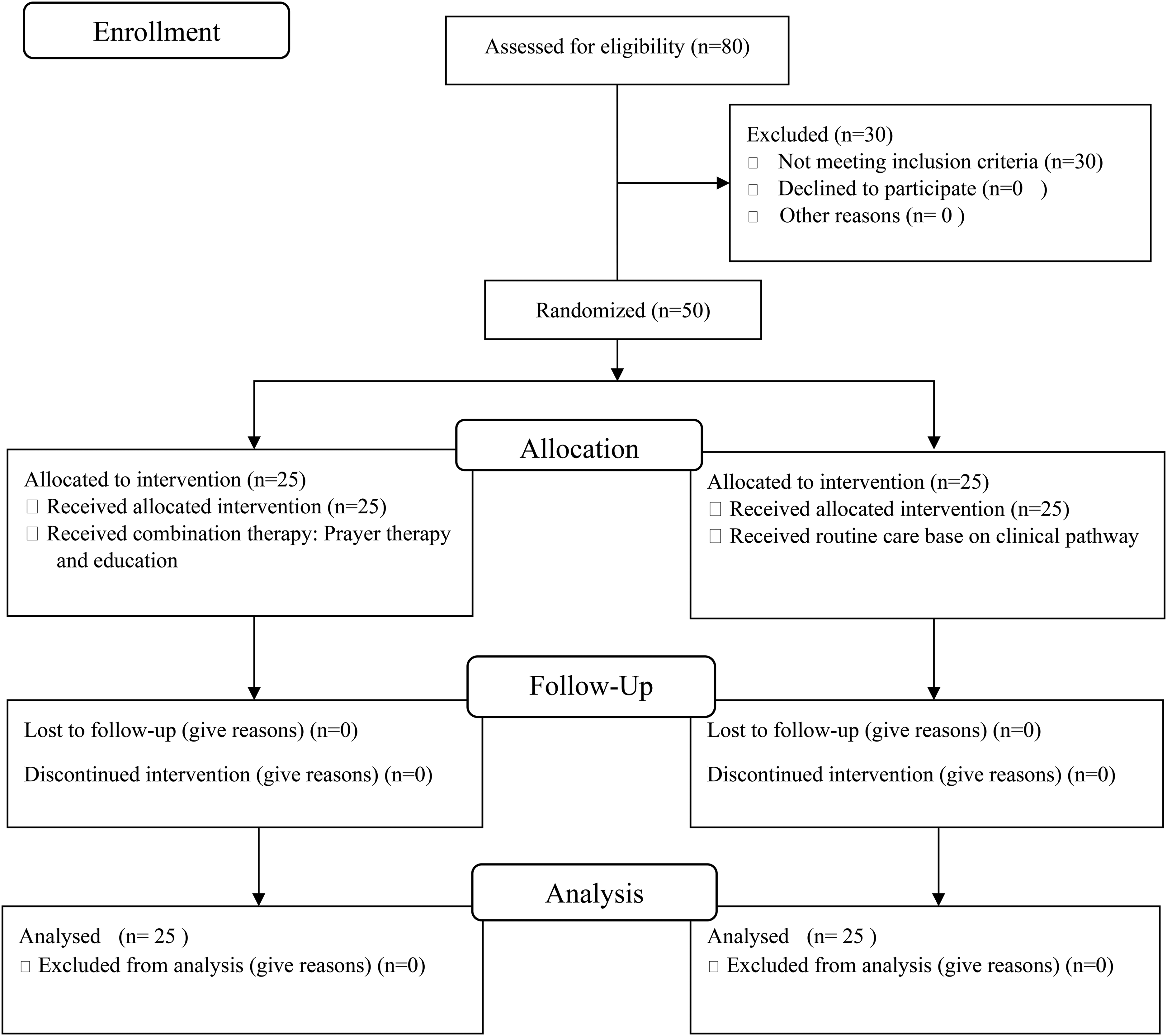
CONSORT Flow Diagram.
Instruments
Data were collected using a State-Trait Anxiety Inventory (STAI) questionnaire from Spielberger to assess patient anxiety one hour before the CABG procedure. The demographic reliability of the questionnaire has been verified by content validity and expert test methods. The STAI is usually used as a measure of the nature and state of anxiety. The most popular version of the inventory form has 20 items to assess trait anxiety and 20 items to assess state anxiety. Anxiety experienced by preoperative patients can be assessed with a questionnaire. The most frequently used questionnaire to assess the anxiety of surgical patients is the State-Trait Anxiety Inventory (STAI). STAI can assess A-State and A-Trait. The scale for the A-state consists of 20 item questions to measure one's feelings about certain events. The score obtained can indicate a temporary level of anxiety. Temporary anxiety has characteristics including tension, anxiety, worry, and fear. Meanwhile, the A-Trait scale consists of 20 items that have been designed to measure persistent, stable anxiety to assess the situation as a danger or a threatening condition. This study used the State Anxiety Inventory questionnaire because anxiety about heart surgery is a temporary anxiety. The internal consistency coefficient for the scale ranges from 0.86 to 0.95, while the retest-test reliability coefficient ranges from 0.65 to 0.75 (Shahpari et al., 2021; Spielberger et al., 1983).
Data Collection
After the respondents were grouped, the researcher gave informed consent. Data collection to measure anxiety was carried out using the STAI instrument. The data collection process was carried out by the researchers directly by providing questionnaires to be filled in by the respondents after an explanation regarding the technicalities of filling in by the researchers was carried out. The researcher accompanied the respondent when filling out the questionnaire directly. After filling out the questionnaire, the questionnaire sheet was handed over to the researcher. Filling out the questionnaire was carried out in the preoperative ward. Filling in the questionnaire in the intervention group was carried out 2 times, namely before the intervention and after the intervention. While the control group was also carried out 2 times, namely the first measurement as a pre-intervention and the second measurement after standard intervention from the hospital. The standard forms of intervention carried out at the hospital are education carried out as a group of heart surgery patients, room orientation and prayer performed by clergy. The intervention in the intervention group was in the form of prayer therapy in the form of a video which lasted 2.57 min. Prayer therapy is carried out according to prayer scripts that can be used by every believer of any religion because of his prayers in general, while education is in the form of preoperative teaching and orientation of the surgical process using a 10-min video so that the information provided is standardized for each respondent. The duration and sequence of interventions carried out by researchers follow the research that has been conducted by previous researchers in providing education and prayer therapy whose intervention results are very effective in dealing with patient anxiety problems.
Statistical Analysis
This study uses univariate and bivariate data analysis. The reseacher conducted a descriptive analysis of the response frequency for each categorical item as in the variables of age, gender, and level of education. The researcher calculated the mean and standard deviation (mean ± SD) for the continuous variables such as an anxiety score (Zhang, 2016). Normality of parametric continuous variables was tested using the Kolmogorov-Smirnov test. The difference test in groups uses the Wilcoxon test and dependent t-test, while the difference test between groups uses the independent t-test (Gerald, 2018).
Results
The data of the study result were presented below:
Characteristics of Respondent
The characteristics of the respondents in the treatment group, most of the respondents are elderly (52%), male (84%). The majority of respondents graduated from senior high school (40%). The majority of respondents in the control group are elderly (64%), male (80%), and have higher education (Bachelor) (44%). The population was homogeneous in terms of demographic characteristics (See Table 1).
Comparison of Demographic Characteristics of Patients in the Intervention and Control Groups (N = 50)
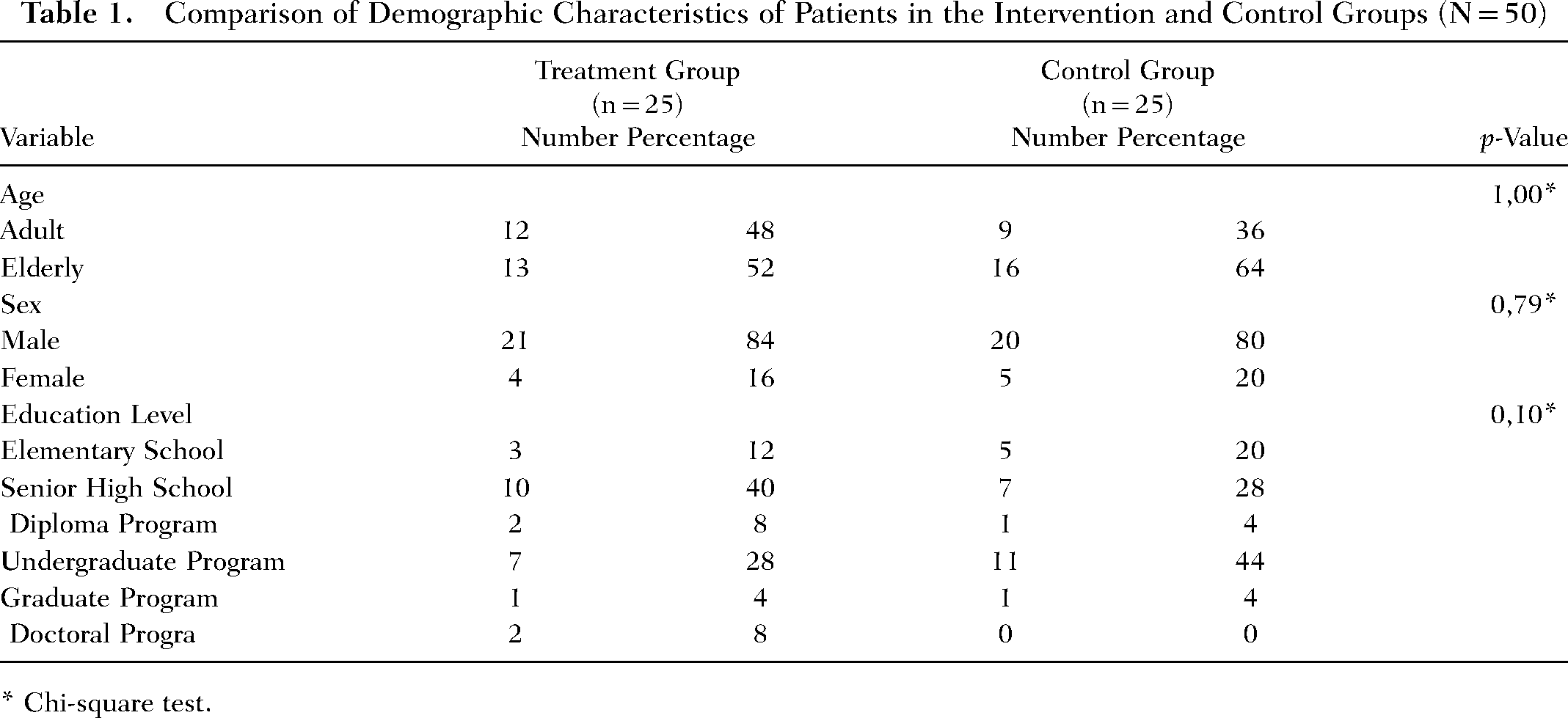
* Chi-square test.
Anxiety Score Description Before and After Treatment
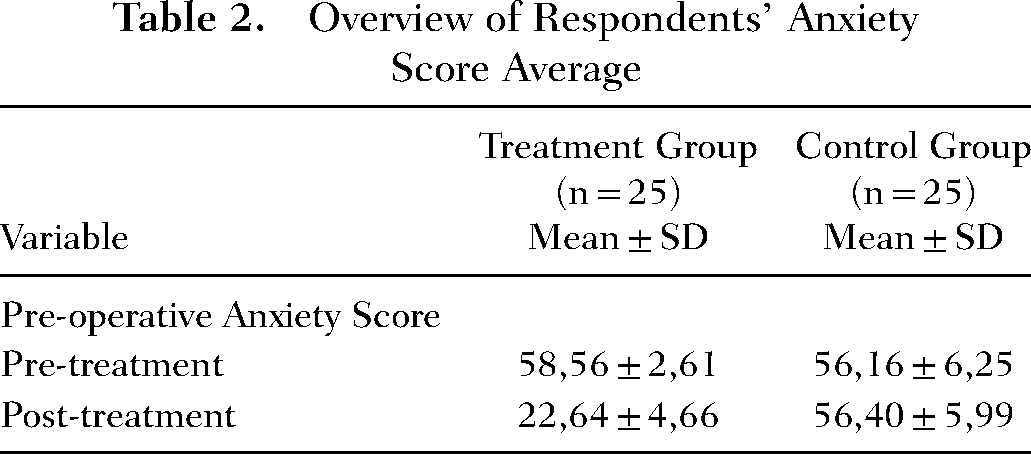
Table 2 describes the average anxiety score based on the results of measuring anxiety using the STAI questionnaire, in the treatment group, there was a decrease in the average score from 58.56 to 22.64, while in the control group there was an increase in the average anxiety score from 56.16 to 56.40.
Overview of Respondents’ Anxiety Score Average
Differences in State Anxiety Scores Between Before and After Treatment
Table 3 shows that there is a significant difference in state anxiety scores before and after being given a combination therapy of prayer and education in the treatment group (p-value <.001), there is no difference in state anxiety scores in the first and second measurements in the control group (p-value .425).
The Result of Anxiety Score Difference Between Pre and Post Treatment

Wilcoxon test. bPaired t-test.
Differences in Mean After Treatment Anxiety Scores of Respondents Between Groups
Table 4 shows significant differences in post-treatment anxiety scores between the treatment group and the control group (p-value <.001).
Test Results Differences in Mean Anxiety Scores of Respondents Between Groups
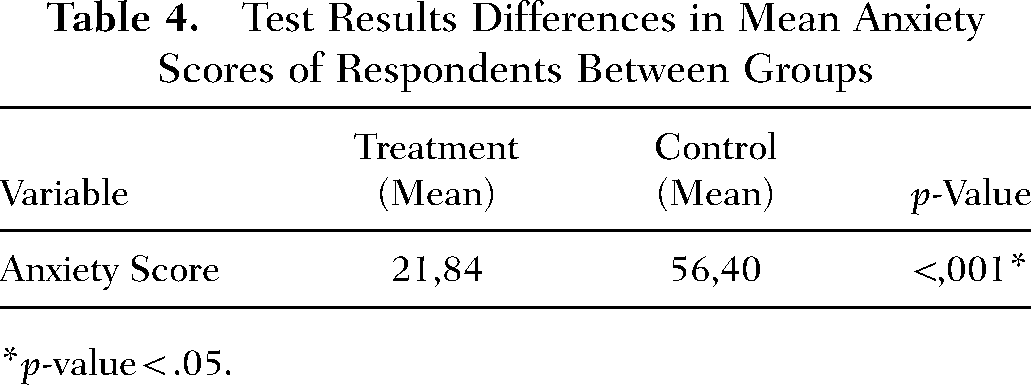
*p-value < .05.
The researcher conducted a data normality test to determine the parametric and non-parametric tests. The after treatment difference test between the intervention and control groups was chosen by the researcher because based on the results of the anxiety score homogeneity test before the intervention, the anxiety score was homogeneous, so it was sufficient to do a after treatment different test. Researchers also carried out random allocations so that data homogeneity between groups could be maintained. In addition, researchers also controlled for bias, so that the difference in post-treatment anxiety scores obtained was purely due to the intervention given (Table 5).
The Great Effect of Prayer Therapy and Education on Anxiety
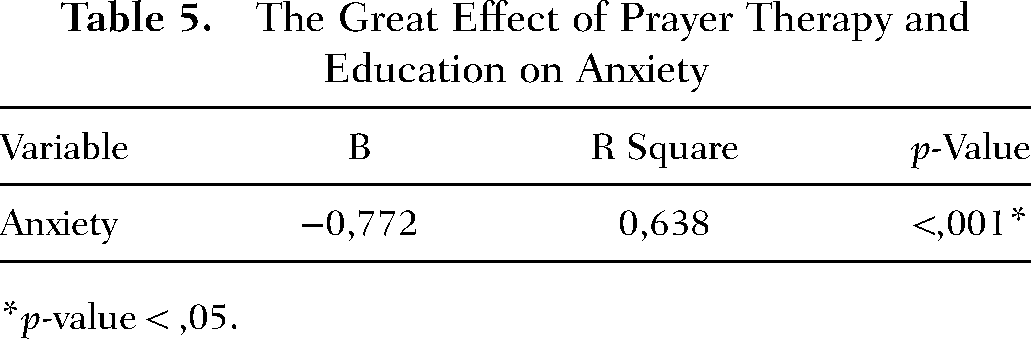
*p-value < ,05.
Discussion
Both respondents in the treatment and control groups are mostly elderly (Table 1). The results of this study are in line with the research of Wan et al. (2021) which stated that the average age of respondents who experienced heart disease was 67 years old (interquartile range, 62–72 years). Factors that cause heart disease in the elderly are having a significantly longer duration of diabetes, having higher albumin to creatinine ratio (ACR) and urinary triglycerides, having an estimated Glomerular Filtration Rate (eGFR) and high-density lipoprotein (HDL) were lower, and having a higher prevalence of smoking, and unilateral and bilateral Common Carotid Arteries (CCA) plaques (Wan et al., 2021). The elderly also have increased low-grade chronic inflammation and oxidative stress as active participants in the pathological mechanism of cardiovascular disease (CVD) (Milanesi et al., 2021). The elderly vary significantly in their future risk for CVD and decreased life expectancy. This variance in CVD risk and mortality is mainly dependent on the underlying comorbidities and degree of frailty. The elderly need to discuss the risk factors for CVD with health professionals, the complexity of the concomitant disease, quality of life considerations, and cost issues associated with polypharmacy (Bays et al., 2021).
The characteristics of the respondents in the treatment and control groups according to gender in this study were mostly male (Table 1). These results are consistent with the literature that men have a higher risk of developing heart disease. However, heart disease also remains a major cause of death in women, especially after menopause (Gao et al., 2019). Men are at risk for heart disease due to unhealthy lifestyles such as smoking, alcohol consumption, and unhealthy diets (Khalili et al., 2014; Tsao et al., 2022). However, the hormonal effect is believed to have a strong contribution to the incidence of coronary heart disease in women. The hormones that play a role are estrogen and progesterone which affect the cycles of menstrual and menopausal. In addition, hormonal contraception is thought to contribute to the incidence of coronary heart disease (De Marvao et al., 2021; Perrino et al., 2021).
The results of this study indicate that the characteristics of the respondents in the treatment and control groups according to education. In the treatment group, the majority of them are senior high school or equivalent, while the control group is mostly undergraduate education (Table 1). These results support that the higher the education, the more knowledge will increase, affecting a person's health attitudes and behavior. Education is part of a person's socioeconomic status, socioeconomic status is a predictor of a person's morbidity and mortality for all health problems. Lower levels of education are a proxy for a lack of knowledge about prevention. In addition, lower levels of education tend to be correlated with lower incomes. Thus, any mechanism through which lower family income leads to a higher risk of CHD can also be applied to education indicators. Education affects the occurrence of risk factors for cardiovascular disease, the higher the education, the more understanding of the causes of disease and the importance of taking steps to help if disease occurs (Miao et al., 2021). The level of education also affects a person's anxiety, the lower the level of education the higher the anxiety (Chen et al., 2019).
The results of the study shown in Table 3 related to the average initial anxiety score before treatment in the treatment group and the control group showed that there was in the moderate anxiety range (score 40–59). However, after treatment, the treatment group showed a decrease in the range of mild anxiety, while in the control group it tended to increase. Cardiac surgery decisions conveyed by doctors to patients create emotional shocks, including anxiety for the patient himself and his family members. Anxiety is negative or threatening emotions that are felt in general, in the long term (trait anxiety), or in certain situations that fluctuate over time (state anxiety) (Kumar et al., 2019). Anxiety in patients can be caused by unusual situations, including; being temporarily separated from the family for surgery, having limited knowledge of medical interventions, diagnoses, or therapeutic methods, and the high costs of surgery, hospitalization, induction of anesthesia, post-operative pain, possible future disability, lack of confidence, lack of help and death (Verulava et al., 2021). The prevalence of anxiety in elective cardiac surgery is reported at 80%. Anxiety during surgery can affect the outcome of surgical treatment. Moreover, long-term anxiety increases metabolism, oxygen consumption, and emotional conception of pain which will lead to a poor mobilization process (Awaludin et al., 2022).
The two interventions that we're able to reduce pre-operative anxiety in cardiac surgery are prayer therapy and education. Prayer is shown to reduce anxiety, depression, and increase hope in cancer patients and surgery patients. The effectiveness of prayer therapy is influenced by the patient's beliefs and culture (Sadeghimoghaddam et al., 2019). The research of Breslin and Lewis (2008) has supported the results of this study and explained the effect of prayer on health through a theoretical model. According to the model, an individual receives healing prayer through possible causal physiological and psychological mechanisms, social support, and spiritual and placebo mechanisms (Breslin & Lewis, 2008). Similarly, the results of this study are in line with the results of research by Tloczynski and Fritzsch in 2002 supporting this idea which states that prayer can be viewed as a placebo or as a positive form of self-fulfilling inspiration in psychology. Factors such as relaxation, catharsis, hope, forgiveness, love, satisfaction, and empowerment play a role between prayer and health through psycho-neuroimmunological and psycho-neuroendocrinological mechanisms (Tloczynski & Fritzsch, 2002).
Pre-operative education is comprehensive information provided before surgery on a variety of topics including procedures, preparation, post-operative progress, psychological support, physical preparation, coping skills, including pain management, effective deep breathing and coughing exercises, physical exercise, and anxiety control techniques (Kalogianni et al., 2016). The media used for education can be in the form of verbal explanations or combined with media such as booklets, leaflets, flipcharts, or videos. When using videos, educational videos work effectively with a duration of 12–40 min. The results of pre-operative education can reduce anxiety (Guo, 2015; Kalogianni et al., 2016). Rahimianfar's research in 2002 using a training booklet was able to reduce patient anxiety. From the results of his research, it is recommended that nurses use this method in conjunction with other interventions to provide comfort to patients (Rahimianfar et al., 2013).
Pre-operative anxiety can continue into the postoperative period if it is not treated at this stage, so psychological problems arising from admission to the care unit should be considered. Patients with post-operative psychosis may present themselves with anxiety, depression, insomnia, or nightmares. This disorder can be intervened through pre-operative education and training, where patients are educated about the possibility of developing this mental disorder because otherwise, patients will think that they have some kind of permanent brain or memory disorder (Loghmani & Monfared, 2018). The combination of prayer therapy and education improves the ability to comprehensively reduce pre-operative anxiety.
Limitations
This study investigates the effect of combination prayer therapy and education, in this study it has not considered the level of religiosity of the respondents, so that in future research it is necessary to pay attention to the level of religiosity in the provision of prayer therapy.
Conclusion
Based on the results and discussion combination of prayer therapy and education can reduce pre-operative anxiety. The combination of prayer therapy and education can be used by nurses to overcome the anxiety of pre-operative CABG.
Implications
The findings show that the recommendation of a combination of prayer therapy and education has a positive impact on clinical practice of nurses in perioperative care units holistically. Nurses can apply these combination therapies to help with surgical anxiety because they save time in educating patients and families, have no side effects, are inexpensive, and are safe for the patient. Nurses who understand which intervention options the most effective treatment for anxiety is important for nursing because the results of anxiety during surgery will inevitably occur in the patient. Therefore, increasing the results for anxiety will also improve the quality indicators.
Footnotes
Author Contributions
Study design was performed by Sidik Awaludin, Elly Nurachmah, and Dwi Novitasari. Data collection was done by Sidik Awaludin. Data analysis was performed by Sidik Awaludin and Dwi Novitasari. Manuscript writing and revision was done by Sidik Awaludin, Elly Nurachmah, and Dwi Novitasari.
Ethical Considerations
Ethical considerations of this study have received ethical approval from the Research Ethics Committee of the National Cardiovascular Center Harapan Kita No. LB.02.01/ VII/517/KEP012/2021, as well as obtaining a written consent form from the respondent, briefing participants about the research and its objectives, and maintaining the confidentiality of patient information.