
Abstract
Keywords
Introduction
Cancer-related symptoms and side effects of chemotherapy, immunotherapy, and radiation therapy can negatively impact quality of life, due to fatigue, pain, nausea, anxiety, and distress (Buxton et al., 2014; Danhauer et al., 2016; Polivich et al., 2014; Sohl et al., 2016; VanHoose et al., 2015). Approximately 35–49% of cancer patients report distress at some point during their cancer journey (Carlson et al., 2010; O’Connor et al., 2017). Multiple factors contributing to distress in cancer patients, include physical, psychological, social, spiritual, and practical challenges which can interfere with the ability to effectively cope with cancer, and its associated physical symptoms and treatments (Carlson et al., 2013; National Comprehensive Cancer Network [NCCN], 2022a; O’Connor et al., 2017).
According to the National Center for Complementary and Integrative Health (2019), more than a quarter of all cancer patients visit complementary and alternative medicine (CAM) providers during treatment as a means of managing distress and common cancer-related symptoms and treatment side effects (NCCIH, 2019). Results of a meta-analysis suggest 40% use of CAM across 18 countries with the highest use in North America (46%). Findings from this study indicate an increase in CAM use from an estimated 25% in the 1970s to 1980s, to more than 32% in 1990s, and 49% after 2000 (Horneber et al., 2012).
Distinct differences exist between complementary and alternative therapies. Alternative therapies are non-traditional practices used in place of conventional medicine. One example of non-traditional practice is a calorie-restricted ketogenic diet which might be used as an alternative therapy for malignant brain cancer (Zhou et al., 2007). Complementary therapies incorporate non-traditional practices along with conventional medicine. For example, a cancer patient may also use natural products concurrently while receiving radiation (e.g., herbs, vitamins, minerals, probiotics) (NCCIH, 2019).
Integrative Health Care and Holistic Nursing
Integrative healthcare is a broad term used to describe practices which combine conventional and complementary therapies in a coordinated way (NCCIH, 2019). An example of integrative healthcare includes conventional medicine, such as chemotherapy, enhanced with a mind–body practice, such as yoga (NCCIH, 2019). Integrative health care “emphasizes a holistic, patient-focused approach to healthcare and wellness—often including mental, emotional, spiritual, social, and community aspects—and treating the whole person rather than, for example, one organ system” (NCCIH, 2019, para. 6).
The holistic nursing approach to healthcare culminates from humanistic philosophies which acknowledge the whole person, and the interdependence of the mind, body, and spirit (Jasemi et al., 2017). An integrative review of 94 published papers resulted in a summative definition of the holistic nurse as one who is “self-aware; has an understanding of intuition, subjectivity, spirituality, and empathy; possesses the ability to conceptualize nursing work; understands conditions and experiences from the patient's perspective; and acts with creativity, compassion, and expertise” (Frisch & Rabinowitsch, 2019, p. 263).
The standards guiding the provision and scope of holistic nursing care have been outlined by the American Holistic Nurses Association (AHNA) and the American Nurses Association (2013). These Standards of Practice describe not only the core values of holistic nursing care, but also specifically define the competencies necessary to ensure the provision of quality, person-centered nursing care (Cowling, 2015). Incorporating a program of yoga therapy tailored to the unique needs of the oncology patient population offers numerous opportunities to further expand upon what is known within the realm of holistic nursing practice by exploring new applications of non-traditional methods of holistic care (Dossey et al., 2005; Helming et al., 2022).
Yoga Therapy
Yoga is a mind–body practice which traditionally involves breathing techniques, deep relaxation, meditation, guided imagery, and physical postures focused on movement and stretching (Khalsa et al., 2016). Yoga therapy is defined as “the process of empowering individuals to progress toward improved health and well-being through the application of the teachings and practices of yoga” (International Association of Yoga Therapists [IAYT], 2019, para. 1). While some techniques are used in both yoga and yoga therapy, distinctive differences exist. Yoga is often taught in a class environment with goals of decreasing stress and improving flexibility, stamina, strength, and mental calmness (Kraftsow, 2019; IAYT, 2019). Alternatively, yoga therapy reaches beyond the standard class environment with a focus on healing the whole person. A Yoga Therapist (YT) guides yoga practice (such as breathing techniques, postures, gentle stretches, meditation/relaxation techniques, and more) in a manner that works best for an individual's unique needs. Goals of yoga therapy may include improving health and wellness, decreasing disease-related symptoms, and promoting rehabilitation (Khalsa et al., 2016; Kraftsow, 2019; McCall et al., 2016).
Consistent with a holistic approach to health, nurses can effectively integrate yoga as primary liaisons and coordinators of patient care (Van Puymbroeck et al., 2015). Nurses and interprofessional teams (comprised of members such as Yoga Therapists and Social Workers) play an important role in integrative health care, which aims for the delivery of well-coordinated care between both providers and healthcare institutions (Long et al., 2003; NCCIH, 2019).
Yoga Therapy for Cancer Patients
Chairside yoga is provided to cancer patients in the comfort of a chemotherapy or immunotherapy infusion treatment chair. Convenience has been described as an important benefit of chairside yoga (Sohl et al., 2016). This mode of practice allows the oncology patient population the opportunity to overcome barriers likely encountered in a traditional yoga setting. Barriers which may prevent cancer patients from attending group yoga therapy classes include fatigue, symptom burden, transportation, and scheduling (Sohl et al., 2016).
Yoga Therapists are trained and certified to adapt and adjust yoga instruction based on the type of illness/limitations, and the patient's own description of their personal experience with cancer. Yoga Therapy in Cancer and Chronic Illness (YCat) is a program specifically created for people with a variety of chronic conditions, including cancer, heart disease, and autoimmune diseases (Chapman, 2018; Chapman & Ashram, 2015; Danhauer et al., 2016; Hart, 2013). The YCat curriculum is used to train YTs individualized yoga practice techniques in a manner which addresses the specific goals of the patient in relation to the side effects and symptoms of their disease. The YCat interventions include specific breathing practices, gentle movements, deep relaxation (e.g., Yoga Nidra), meditation, and guided imagery, all of which may be modified to compensate for cancer-related treatment limitations or enhanced to meet the individual's personal goals (Chapman & Ashram, 2015).
Review of the Literature
Yoga Therapy for Symptom Management
Multiple benefits of yoga therapy for cancer patients and cancer survivors have been described in meta-analyses and other systematic reviews of literature. These research studies support yoga therapy as an option for reducing physical and psychosocial symptoms in cancer patients, including cancer-related fatigue (CRF), anxiety, pain, nausea, and distress (Buffart et al., 2012; Cramer et al., 2012; Danhauer et al., 2016; Harder et al., 2012; Lin et al., 2011; Mishra et al., 2014; Sisk & Fonteyn, 2016; Smith & Pukall, 2009; Zhang et al., 2012). These five common symptoms are described in detail in the following paragraphs.
Cancer-Related Fatigue (CRF)
Numerous studies support the use of yoga therapy to decrease cancer patients’ experience of fatigue (Chadwani et al., 2014; Cramer et al., 2015; Danhauer et al., 2009; Dhruva et al., 2012; Taso et al., 2014; Vadiraja et al., 2009). National Comprehensive Cancer Network (NCCN) describes CRF as a “distressing, persistent, subjective sense of physical, emotional, and/or cognitive tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and interferes with usual functioning” (NCCN, 2022b, pg. FT-1).
Anxiety
The experience of anxiety in response to a cancer diagnosis is considered a normal reaction to a potentially life-threatening illness. Cancer-related anxiety is frequently influenced by disease stage, medications, and difficulties in managing and coping with the disease and its treatments (Economou, 2017a). Numerous studies suggest that anxiety in cancer patients can be decreased after yoga therapy interventions (Dhruva et al., 2012; Raghavendra et al., 2007; Rao et al., 2009; Kovačič et al., 2013; Taso et al., 2014; Vadiraja et al., 2009).
Pain
The experience of pain is commonly associated with the disease of cancer and its treatments. One-third of patients actively receiving cancer treatment and two-thirds with end-stage cancer experience some form of significant pain (Economou, 2017b). Empirical evidence suggests that yoga therapy offers promise as an intervention to minimize the experience of pain among cancer patients (Carson et al., 2007, 2009).
Nausea and Vomiting
The experience of nausea and vomiting occurs with up to 80% of patients with cancer and can be the most distressing side effect of cancer treatment. With advances in modern anti-emetic therapy, chemotherapy-induced nausea and vomiting can be reduced to 13–35%, even among patients receiving moderately or highly emetogenic chemotherapy (Olsen et al., 2019). Yoga therapy has also been shown to help minimize the experience of nausea among cancer patients (Rezaei et al., 2017; Raghavendra et al., 2007).
Distress
The experience of distress is common among cancer patients. Distress is defined by NCCN as: A multi-factorial unpleasant experience of a psychological (i.e., cognitive, behavioral, emotional), social, spiritual, or physical nature that may interfere with one's ability to cope effectively with cancer, its physical symptoms, and/or its treatment. Distress extends along a continuum, ranging from common normal feelings of vulnerability, sadness, and fears to problems that can become disabling, such as depression, anxiety, panic, social isolation, and existential and spiritual crisis (NCCN, 2022a, p. DIS-1).
The experience of distress is so prevalent among cancer patients that NCCN developed “Clinical Practice Guidelines in Oncology for Distress Management” (NCCN, 2022a). These guidelines acknowledge that distress is “recognized, monitored, documented and treated promptly at all stages of disease and in all settings” (NCCN, 2022a, p. DIS-2). These guidelines also recommend a variety of distress-related interventions for healthcare providers to incorporate into cancer care, including complementary and integrative therapies (NCCN, 2022a). Results from multiple studies support the positive effect of yoga therapy as an intervention to decrease distress levels among cancer patients (Bower et al., 2012; Danhauer et al., 2009; Kovačič & Kovačič, 2011; Moadel et al., 2007; Raghavendra et al., 2007; Rao et al., 2009; Vadiraja et al., 2009).
While the previous summary of literature clearly supports the use of yoga as an adjunct therapy in the oncology patient population, unique challenges exist when attempting to offer this therapy in the clinical setting. Research findings can be difficult to generalize or apply in practice due to the high degree of variability in research designs, types of yoga therapy, and myriad of cancer diagnoses.
Theoretical Framework: Biopsychosocial Model and Yoga Therapy
The provision of holistic care is characterized by the treatment of the whole person and acknowledgement of mental and social factors, rather than just the symptoms of an illness. The World Health Organization encourages this holistic perspective and defines health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” (WHO, 2022).
The biopsychosocial model of health, first proposed by Engel in 1977, provides a comprehensive framework for understanding health and disease when managing patient health (Engel, 1977; Bryan et al., 2012). According to this model, health is viewed as a complex, dynamic process that involves the interplay of three aspects, including biological, psychological, and social (Molina, 1984). These holistic aspects are interconnected and interdependent and affect health outcomes in either a positive or negative way (Bryan et al., 2012; Hoffman & Driscoll, 2000; Suls & Rothman, 2004). Factors within each of these aspects include:
Biological factors—age, race/ethnicity, gender, and preexisting health conditions. Psychological factors—emotional status, including depression, anxiety, reactions towards stress, and psychological and emotional well-being. Social factors—socioeconomic status and social interactions, including friends, family, and ties to one's community and society (Ross et al., 2014).
The yoga perspective parallels Engel's biopsychosocial model of health (Engel, 1977). Yoga, which is an age-old practice and literally means “union,” refers to the union of the mind, body, and spirit (Diab, 2001). Because yoga has been associated with physical and mental well-being, the authors adapted Engel's (1977) model and Ross et al.'s (2014) model to create a biopsychosocial model of yoga therapy and health. In this adapted biopsychosocial model, health is defined as well-being and increased quality of life, including decreased symptoms. Total health can be achieved with balance and stability in all three aspects.
Numerous randomized clinical trials have been performed, which have examined the benefits of yoga therapy on mental and physical health of cancer patients (Danhauer et al., 2016). Based on the evidence, the research team structured this pilot study to determine if one or more yoga therapy interventions (e.g., gentle movement, breathing practices, meditation, awareness practices, yoga nidra, and/or guided imagery) will decrease physical and emotional symptoms in cancer patients who are receiving chairside infusions.
Purpose
Few studies exist describing the role of chairside yoga therapy used in an outpatient infusion setting for the relief of cancer patient symptoms as part of hemotherapy/immunotherapy administration (Buffart et al., 2012; Sohl et al., 2016). The purpose of this feasibility study was to examine the potential effect of a yoga therapy intervention on perceptions of fatigue, pain, nausea, anxiety, and distress among oncology patients. This study examined oncology patients while concurrently receiving outpatient cancer therapy infusions. Qualitative data was also examined to determine participants’ overall experience with the yoga therapy intervention.
Methods
Setting
This study was conducted in an outpatient cancer center at a 550-bed, academic, healthcare network located in the mid-west. The Cancer Center's Oncology Service Line, accredited by the American College of Surgeons Commission on Cancer, prioritized integration of a holistic approach into oncology care with a focus on yoga therapy. An interprofessional team collaborated to plan and develop a feasibility study, which was designed to determine the effectiveness of a yoga therapy program. The team consisted of an Oncology Clinical Nurse Specialist, Director of Nursing Research, Oncology Social Worker, staff nurses, and a YT.
Study Population
A single convenience sample of patients participating in an individually-guided, chairside yoga session was used for this study. All eligible patients were adults (over the age of 18), English speaking, of any gender, mentally competent, and capable of verbally consenting and physically participating in basic yoga therapy. In addition, all eligible patients were able to understand the study and rating of study variables (fatigue, pain, nausea, anxiety, and distress).
Eligible oncology patients were referred to the YT in collaboration with nursing and social work. These health care providers identified patients who were experiencing high levels of symptoms, especially pain, anxiety, fatigue, nausea, and distress.
Instrument
A comprehensive review of the literature revealed several lengthy instruments, but no concise instruments, which could efficiently measure the effect of yoga on cancer-related symptoms among patients receiving infusion therapy in a busy outpatient treatment center. The tools revealed in this literature review are included in this discussion for completeness, but none were selected for use in this study due to their excessive length which would have been impractical for a brief intervention in an outpatient setting. Cleeland et al. (2000) developed the MD Anderson Symptom Inventory, which measured 26 cancer-related symptoms (Cleeland et al., 2000). Rosenthal et al. (2007) modified the MD Anderson Symptom Inventory, Head and Neck Module, which included 19 questions (Rosenthal et al., 2007). Also, Sikorskii et al. (2007) assessed 17 cancer-related symptoms in their tool (Sikorskii et al., 2007).
Due to the lack of a concise instrument, the interprofessional team leading this study developed a succinct, easy-to-use tool called the Outpatient Cancer Symptom Assessment Scale (OCSAS) to assess the five most common symptoms in oncology outpatients, as supported by the literature (Buffart et al., 2012; Cramer et al., 2012; Danhauer et al., 2016; Harder et al., 2012; Lin et al., 2011; Mishra et al., 2014; Sisk & Fonteyn, 2016; Robison et al., 2019; Smith & Pukall, 2009; Zetzl et al., 2021; Zhang et al., 2012). The OCSAS was derived from a tool called the Symptom Assessment Scale (SAS), which was developed and used in a study of hand/foot massage to measure the effect of the massage intervention on pain, fatigue, anxiety, and nausea among oncology patients receiving a cancer infusion treatment (Robison & Smith, 2016).
In this feasibility study, OCSAS is a modified version of the SAS tool and consists of the same common cancer and treatment-related symptoms as contained within the original massage therapy instrument (pain, fatigue, anxiety, nausea) (Robison & Smith, 2016). The OCSAS was modified by adding the symptom “distress” and by expanding the Likert scale from 5 points to 10 points to reflect the NCCN Distress Thermometer (NCCN, 2022a). Both words and numbers were used with symptom ratings to increase understanding for patients. For example, the pain rating included: 0 = no pain; 1-3 = mild pain; 4-6 = moderate pain; 7-9 = severe pain; and 10 = the worst pain ever. The psychometric properties of the OCSAS have not yet been performed, and this will be examined and described in a future paper.
Demographic questions (age, gender, diagnosis, and treatment) were also included on the OCSAS and then compiled into a survey which asked patients to identify their yoga treatment goals, including stress reduction, relaxation, increased feelings of peace/quiet, symptom relief, and the opportunity to learn yoga techniques which could be practiced at home. Qualitative data collected on the survey helped inform the YT's overall assessment of the patient and guided the final selection of the type of yoga therapy which could yield the most therapeutic experience for the patient (selection of therapy is described in the next section). In the post-yoga survey, symptoms were re-assessed (using the same symptom assessment instrument), and patient comments about their experience with yoga therapy were recorded. Definitions for each study variable (pain, anxiety, fatigue, nausea, and distress) were based on patients’ own subjective experience. No attempt was made by researchers to define or influence any patient's perception of their symptom experience.
Data Collection
Using the OCSAS tool, data were collected before and after the yoga intervention. The YT guided patients to rate the intensity of the five symptoms frequently caused by cancer or cancer-related therapies (e.g., pain, nausea, fatigue, anxiety, and distress) on the 0–10 Likert rating scale. In the post-yoga survey, patients were encouraged to provide any qualitative feedback regarding other benefits derived from the yoga therapy intervention.
All quantitative and qualitative survey responses were provided verbally to the YT before, during and after the yoga intervention. The ability for patients to complete surveys in writing was often not feasible due to multiple reasons, including their reclined position, concurrent administration of infusion therapy, experience of symptoms (e.g., fatigue, nausea), or inconvenience. The YT carefully recorded each participant's survey response and clarified answers, as needed.
Intervention
The yoga therapy intervention was provided by a YT, certified in oncology yoga therapy. This certification qualified her to provide safe, effective methods of adaptive yoga specific to the particular needs of cancer patients. The YT personally approached eligible cancer patients who were receiving, or scheduled to receive, chairside infusion (e.g., chemotherapy, immunotherapy, hydration fluids, and other infusion services) within the outpatient Cancer Center.
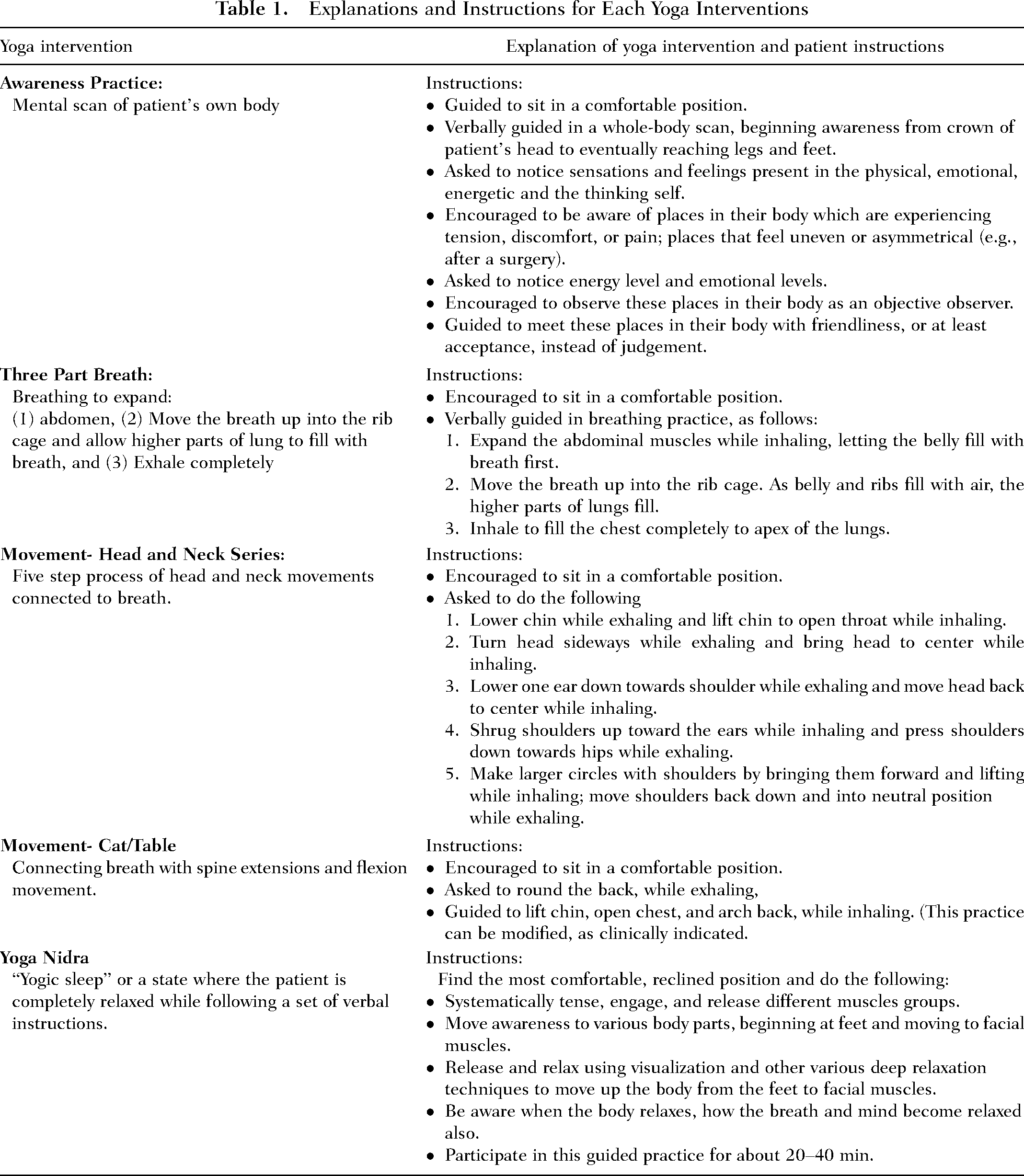
The yoga therapy intervention used in this feasibility study consisted of five primary yoga techniques. The YT selected one or more of these techniques (awareness practice, three-part breath, movement, head and neck movement series, and yoga nidra) for each patient. General explanations and instructions, which were provided to patients for each type of yoga intervention used in this study, are described in Table 1.
Explanations and Instructions for Each Yoga Interventions
The most appropriate yoga therapy intervention was selected by the YT based on patient assessment, using the OCSAS, guided by the empirical literature (Chapman & Ashram, 2015; Danhauer et al., 2016, 2017). The yoga therapy was customized for each individual patient and adapted as needed. The selection for each type of yoga based on assessment of patient symptom is described in Table 2.
Guidelines to Select Yoga Therapy Interventions Based on Symptom Assessment Using the Outpatient Cancer Symptom Assessment Scale (OCSAS)
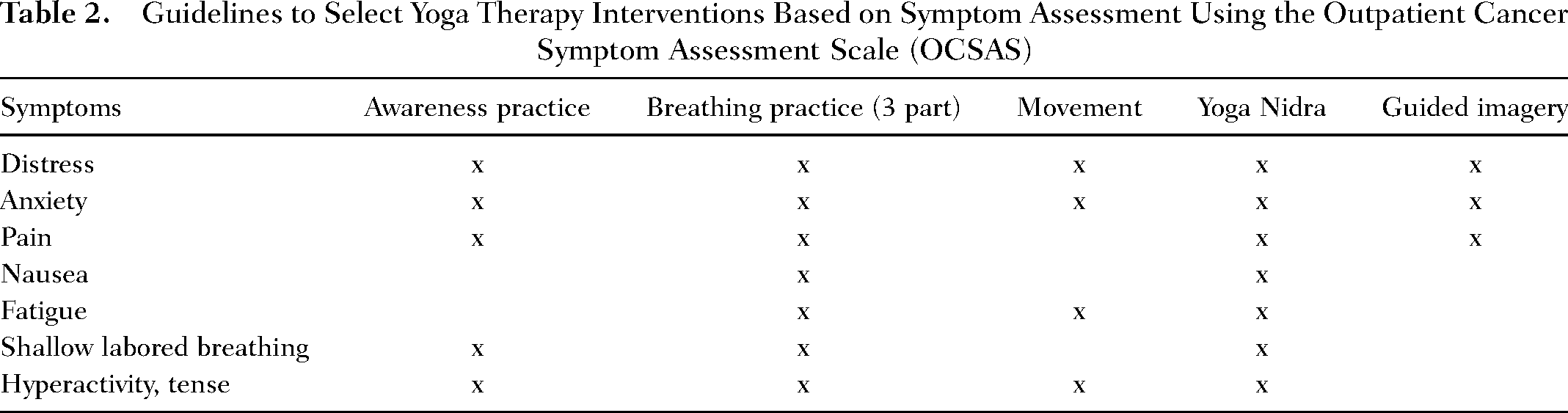
Patients received 15–25 min of individualized, chairside yoga therapy interventions using standard YCat yoga curriculum (Chapman & Ashram, 2015). After assessing the patient's symptoms and personal goals/preferences, the YT selected the appropriate yoga intervention(s). For example, the YT may have selected three-part breath techniques for persons with low energy levels, or awareness practice for those experiencing distress. For patients experiencing multiple symptoms, the YT prioritized and combined yoga therapy interventions. For example, the YT may offer a breathing practice which incorporates meditation techniques to a patient who was experiencing high levels of anxiety and fatigue.
The YT was flexible in the time frame provided for yoga therapy due to the typical interruptions of a busy infusion center (medication administration, IV maintenance, treatments, family visits, etc.) (Chapman & Ashram, 2015; Robison et al., 2019). For example, if the RN entered the patient's room/bay during a yoga intervention and needed time with the patient, then the YT returned to the patient after the required nursing tasks were completed.
Data Analysis
Survey data were entered into Microsoft® Excel and imported into SPSS®, version 17.0, for statistical analysis. Demographic characteristics (e.g., cancer diagnosis, age, gender) were analyzed using descriptive statistics. Mean, standard deviation, and paired sample t-tests were performed to determine if significant differences existed between pre-and post-test scores for pain, fatigue, nausea, anxiety, and distress. Content analysis was used to analyze patients’ comments regarding the overall benefit of the yoga intervention. Qualitative data were coded according to common themes by the Principal Investigator (PI) and YT, and coded themes were then reviewed by the hospital's Director of Nursing Research. Number of comments in each category were calculated, and sample comments for each theme were summarized in a table. A research assistant entered qualitative data into an electronic spreadsheet.
Ethical Considerations
Approval was obtained from the hospital's Institutional Review Board prior to the initiation of this study. Eligible patients invited to participate in the research were assured their participation was voluntary and could be withdrawn without penalty at any time. The YT introduced the chairside yoga therapy program to qualifying participants receiving chemotherapy/immunotherapy in the infusion treatment area. Following verbal consent, the YT described the potential benefits of yoga therapy, explained the basic physiology of yoga, and demonstrated the techniques to be used. Only those patients who verbally consented were included in this study.
Results
Over a 12-month period, this feasibility study enrolled 82 patients (54.95% female, 42.7% male, 2.4% no response) with a mean age of 58.5 years (SD = 12.44). Participants were simultaneously receiving chemotherapy/immunotherapy in an outpatient setting for the following cancer diagnoses: Breast cancer (26.8%), leukemia/lymphoma/multiple myeloma (17.1%), lung cancer (16.4%), colorectal (11.0%), and 11 other solid cancers (28.7%).
Participants receiving a yoga therapy session concurrently with infusion reported statistically less pain (p < 0.001), fatigue (p < 0.001), anxiety (p < 0.001), and distress (p < 0.001) compared to pre-yoga baseline scores (Table 3). No significant change was noted in the symptom of nausea compared to baseline (p = .062). Mean differences from pre-yoga to post-yoga ranged from 1.16 points (pain) to 1.87 points (distress), for all symptoms, except nausea. Mean pain score decreased from 2.10 (SD = 2.93) to 0.94 (SD = 1.98). Mean fatigue score decreased from 3.69 (SD = 3.27) to 1.90 (SD = 2.34). Mean anxiety score decreased from 2.59 (SD = 2.45) to 1.17 (SD = 1.50). Mean distress score decreased from 3.84 (SD 3.00) to 1.97 (SD = 1.85) (See Table 3). Patients infrequently described “other” cancer symptoms which were not included as options on the survey (e.g., back pain, vertigo, and insomnia). However, these findings were insufficient in number to warrant thematic coding and analysis.
Repeated Measures t-Tests: Pre and Post-Yoga Scores

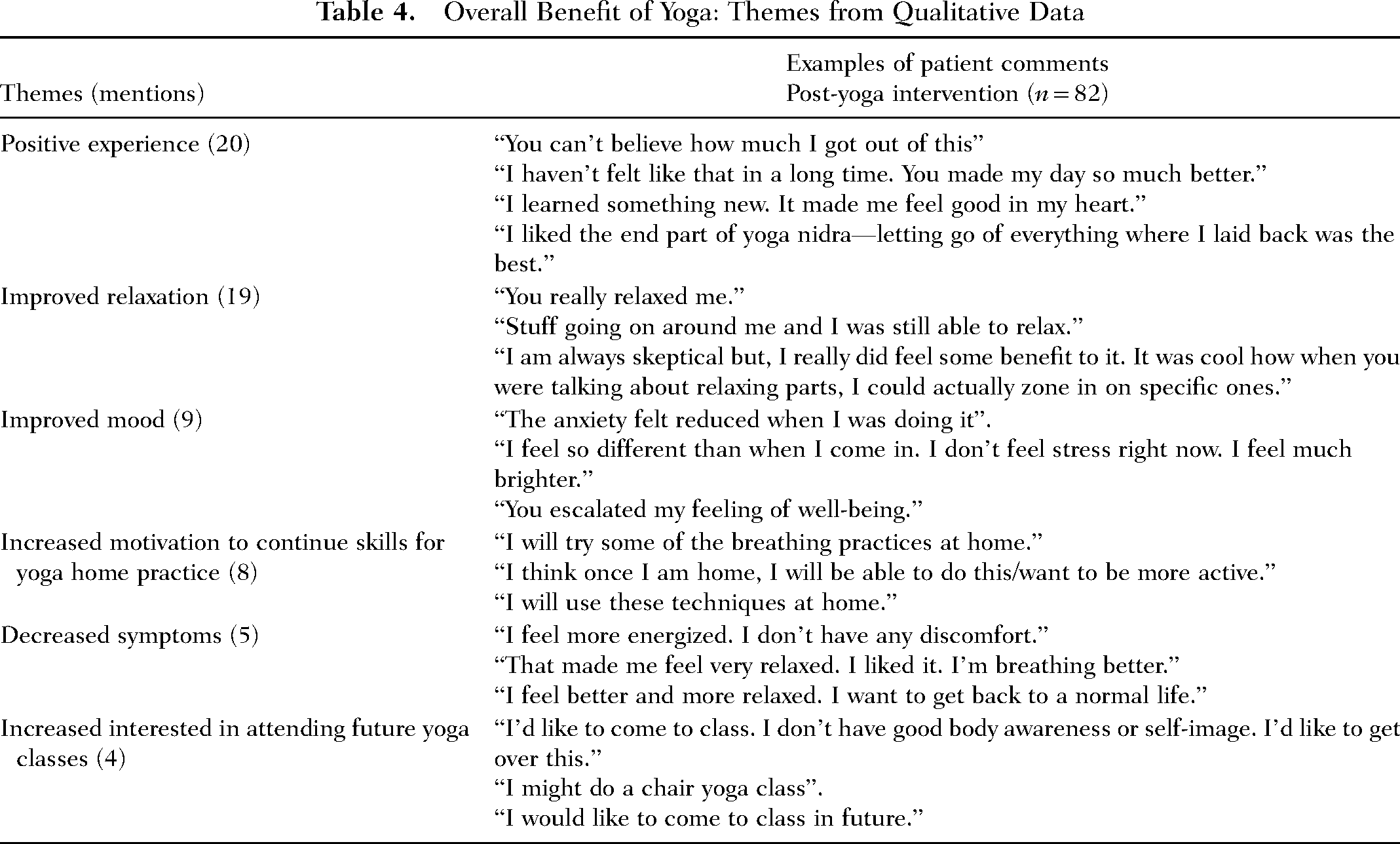
Qualitative feedback provided to the YT revealed themes describing the yoga therapy intervention as a positive experience. Some of the key themes included increased relaxation, improved mood, diminished symptoms, increased motivation to continue skills for home yoga practice, and increased interest in pursuing yoga therapy in the future. (See Table 4.)
Overall Benefit of Yoga: Themes from Qualitative Data
Discussion
The purpose of this feasibility study was to examine the potential effect of a yoga therapy intervention on perceptions of fatigue, pain, nausea, anxiety, and distress among oncology patients. concurrently receiving outpatient cancer therapy infusions. Qualitative data was also examined to determine participants’ overall experience with the yoga therapy intervention. This study represents a significant step towards the implementation of yoga therapy in an outpatient oncology setting where cancer patients routinely receive chemotherapy and immunotherapy infusions while seated/reclined in chairs. Chairside yoga therapy was selected as an intervention due to the frequent barriers experienced among cancer patients’ attempting to participate in group yoga therapy classes (Sohl et al., 2016). A chairside yoga program allows the YT to bring the intervention directly to the patient during the time of their infusion therapy, which offers potential to alleviate both cancer- and disease-related symptoms.
Since this was a feasibility study, many practical lessons were learned and are included in the comprehensive discussion section that follows. As noted previously, sparse studies exist describing the role of chairside yoga therapy when used in an outpatient infusion setting for the relief of cancer patient symptoms as part of hemotherapy/immunotherapy administration. Therefore, researchers felt it important for the YT to take advantage of the unique opportunity to capture comments that were voluntarily shared by patients during or following their yoga session. These supplemental data points were not formally analyzed but were included for the YT's information and to guide decisions about yoga therapy practice.
Notations made by the YT on the data collection tool allowed for the capture of supplemental qualitative data that could serve to inform the direction of future research and provide opportunities for programmatic improvements on the little known topic of chairside yoga (to be described in a future paper). Supplemental information captured by the YT included: The presence of family members (∼80% of the time), and “other symptoms,” such as headache which were reported by the patient but excluded from data analysis (this information could be used to inform future revisions of the instrument). Finally, a “patient comment” section was added so the YT could capture the comments voluntarily provided by patients for future qualitative analysis and programmatic improvements. Supplemental additions to the data collection tool (but not included in analysis) were made to help guide more rigorous research in the future and were reported to, and approved by, the institution's IRB, as appropriate.
Several practical lessons were learned during the implementation of the yoga therapy program. Some patients had difficulty independently completing the Likert scale for symptom assessment, which may have been related to their experience of high levels of fatigue, pain, or other symptoms. Therefore, during this study, the YT interviewed patients before and after the yoga intervention to obtain the symptom ratings and assess for visible clues which might suggest distress and physical limitations. Visible clues of distress included: altered breathing patterns (shallow or labored breathing), decreased level of motivation, and altered emotional state. Visible signs of physical challenges could include low energy and postural limitations. While this ongoing assessment was completed informally during the therapy session, future studies might formalize and document this assessment process. An incidental finding was that patients often rated their anxiety as a “0” before the yoga therapy intervention, but then commented that their anxiety and/or the tension in their shoulders diminished with the relaxing effects of the yoga intervention.
The YT collaborated with nurses to determine which patients might benefit from and participate in the yoga therapy. Nurses provided brief education on the yoga therapy intervention and encouraged qualifying patients to participate, when appropriate. Social workers identified patients with high distress scores (≥4) and referred them to the YT, as appropriate. The most significant steps to effectively implement a yoga therapy program in an outpatient oncology clinic were:
Use strategies to increase the patient/caregiver's acceptance of yoga therapy (e.g., establishing a therapeutic relationship, describing yoga therapy as a stress-reducing activity, and wearing facility name badge). Provide patient education about yoga therapy interventions and correct any misconceptions (e.g., they will not be asked to do difficult yoga poses; it is a stress-reducing activity). Provide nurse education related to yoga therapy to increase their understanding of the yoga therapy interventions for cancer patients. Plan logistics in implementing the yoga therapy program in the outpatient oncology clinic, including dates, times, etc. Engage the support and assistance of nurses to help identify patients for the yoga intervention and integrate the yoga session into the infusion schedule.
Limitations
This study was impacted by several limitations. Data were collected from patients in the infusion department of a single outpatient cancer center so results cannot be generalized to all cancer centers. The population included a relatively small sample size (n = 82) and participants had multiple cancer diagnoses. A variety of yoga interventions were necessarily used during the patient's yoga experience, including yoga nidra, breathing practices, movement, guided imagery. Flexibility in customizing the interventions was essential for the YT to appropriately respond to the myriad of patient diagnoses, physical abilities, and acuity levels encountered during cancer infusion therapy. However, determining the efficacy of any single yoga intervention over another was beyond the scope of this feasibility study.
Another potential limitation was the lack of a manual for standardizing the use of yoga therapy for cancer patients. The YT did use the “YCat Yoga Therapy: Yoga for People with Cancer and Chronic Illness” manual as a guideline; however, an institution-specific manual was not available. This study could help guide the development of a standardized manual for yoga therapy that could be customized to the institution.
The properties of the instrument (reliability and validity) were not investigated but will be provided in a future paper. However, this feasibility study provides valuable information that can help guide the development of more robust tools in the future. The specific amount of time for each yoga therapy intervention was not measured since it occurred during the typical infusion timeframe of 15–25 min. There was a potential for bias, since the data was collected by the YT, who also provided the intervention. Finally, family members were frequently present during the yoga intervention. Their presence and participation in the session could have enhanced or lessened the impact of the session, potentially confounding study findings.
Implications for Future Research
Study participants were commonly accompanied by family members or caregivers who also frequently participated in the yoga therapy intervention during the patient's infusion therapy encounter. Future studies could examine the impact of family/caregiver participation in the yoga therapy intervention, including the impact on the family member/caregiver's own coping strategies. Future yoga therapy studies could include formalized patient and family education on holistic approaches to health, including support for the continuation of yoga practices at home. Educational resources could include CDs, websites, group yoga classes (virtual and in person), and other forms of support which reinforce learning and provide a meaningful and practical way to practice yoga at home.
The frequent use of anti-emetics by this study population (e.g., cancer patients receiving chemotherapy and infusion therapies) likely influenced the low nausea scores. In future studies, it may be prudent to remove the nausea/vomiting variable given the confounding effect of anti-emetics since there are varying levels of emetogenicity with single agent and multiple agent chemotherapy regimens.
Future studies could include collection of additional demographic data, including cancer stage and reason for clinic visit (e.g., type of chemotherapy, infusion). Data could also include more objective measurements of visible signs of distress, physical limitations, and length of therapeutic yoga intervention.
The yoga therapy interventions used in this study were limited to one per patient. Future research could include randomized controlled studies using multiple sessions of outpatient YT. Additionally, replication of this research with larger sample sizes, using a longitudinal study design, and multiple healthcare sites could make study findings more generalizable to other populations. A longitudinal design could include implementation of a defined type of yoga intervention customized for specific symptoms or complaints, followed by a series of measures to evaluate the efficacy of the yoga therapy intervention for the identified symptom(s) over time, as well as patient satisfaction with the yoga intervention.
Definitions for each study variable (pain, anxiety, fatigue, nausea, and distress) were based on patients’ own subjective experience. Future studies could include clear definitions of symptoms which could help participants evaluate their experience of anxiety and distress more uniformly.
Conclusions
Numerous research studies support yoga as a therapeutic option for reducing the physical and psychosocial symptoms experienced by cancer patients. Yoga therapy is a mind–body practice which involves breathing techniques, deep relaxation, meditation, guided imagery, and physical postures focused on movement and stretching. More than a quarter of all cancer patients use integrative healthcare practices during treatment to help manage distress and decrease common cancer-related symptoms and treatment side effects. Cancer-related symptoms and side effects of chemotherapy, immunotherapy, and radiation therapy often include pain, fatigue, nausea, and anxiety. Consistent with a holistic approach to health, nurses can effectively integrate yoga therapy in their role as primary liaisons and coordinators of patient care. Findings from this feasibility study suggest that yoga therapy in an outpatient infusion setting can be an effective non-pharmacological method for decreasing some of the most common symptoms in cancer patients and offers significant implications for holistic oncology nursing practice.