
Abstract
In 2021, North Carolina (NC) authorized pharmacists to initiate hormonal contraceptives. The objectives of this pilot study were to: (1) determine where hormonal contraception (HC) services were provided; (2) evaluate patient characteristics; and (3) describe pharmacist interventions. Pharmacists who completed training and prescribed HC between April 2022 and December 2023 were invited to participate. Participants completed an online survey about pharmacy demographics and descriptive statistics were used to summarize characteristics. De-identified patient encounters were uploaded into a secure website and data was analyzed using descriptive statistics. 1309 pharmacists completed HC training. Seventeen pharmacists (1.3%) participated in the study and completed demographic surveys. Four pharmacists (24%) saw 34 patients during the study period and provided intervention data for 21 patients. Seventy percent of pharmacists worked in independent pharmacies, and 47% of pharmacies were in rural communities. Seventy percent of patients had commercial insurance (50%) or NC Medicaid (20%). Fifty-three percent of patients reported that they had a primary care provider (PCP). Pharmacists prescribed a hormonal contraceptive in 95% of patient encounters, most frequently the combined HC pill (70%). One patient was referred to a primary care clinic due to elevated blood pressure. All pharmacists in this early-adopter pilot study of contraception pharmacists practiced in independent pharmacies. Seventy percent of patients who sought care from a pharmacist were insured, approximately half did not have a primary care provider, and pharmacists initiated HC for 95% of patients. The most common HC prescribed was the combined HC pill.
Introduction
The Pregnancy Risk Assessment Monitoring System (PRAMS) dataset for North Carolina (NC) reported that 46% of pregnancies were unintended in 2020 which aligns with national statistics. 1 Women who experience an unintended pregnancy often seek prenatal care later than women with an intended pregnancy and are at risk for negative maternal infant outcomes including depression, interpersonal violence, and low birth weight.2,3 The United States has the highest rate of maternal mortality compared to other high-income countries (22 maternal deaths per 100 000 live births) and Black women are at highest risk of death. 4 In 2018-2019, 76 maternal deaths occurred in NC, and 85.5% of these were considered preventable. 5 Healthy pregnancies and access to contraception are important public health goals that are impacted by closure of rural hospitals, the primary care shortage, social drivers of health, and healthcare policy. 6 Over 650 000 women in NC live in contraception deserts, meaning they lack access to a health center that offers a full range of contraceptive methods. 7 These statistics highlight the significant need to improve access to reproductive health services.
Seeing a pharmacist for hormonal contraception (HC) eliminates some access barriers for patients who prefer self-administered hormonal contraception because they can see a provider and receive their contraceptive during the same visit. 8 Pharmacists are considered the most accessible health care professional and many pharmacies offer evening and weekend hours when clinics are typically closed. According to the Guttmacher Institute, 30 states and the District of Columbia currently allow pharmacists to initiate hormonal contraception under collaborative practice agreement, standing order or statewide protocol. 9 Pharmacist-prescribed contraception is supported by pharmacists, professional organizations and policy groups,10-12 and decreases healthcare costs. 13 A survey of pharmacists in NC prior to legislation authorizing pharmacists to initiate hormonal contraception indicated that 83% of community pharmacists would provide contraception services if legislation was passed and a payment model was developed. 12 Ninety-seven percent of patients who received contraception services from a pharmacist in California and completed a survey (n = 160) indicated that they were satisfied with the care they received, and 96% of patients indicated that they would recommend the service to a friend. 14
NC passed House Bill (HB) 96 in 2021, authorizing pharmacists to initiate hormonal contraception, glucagon, prenatal vitamins, nicotine replacement therapy, and post-exposure prophylaxis for HIV, and to administer long-acting injections. 15 The new law went into effect on February 1, 2022. The National Academy of State Health Policy published a case study highlighting NC’s approach to pharmacist-prescribed contraception. 16 In order to prescribe contraception in NC under statewide protocol, pharmacists must be an immunizing pharmacist who completed a five-hour training offered by the state pharmacy association. Minors in NC must have parental or guardian consent to see a pharmacist for HC. Pharmacists are required to counsel patients about the importance of having a primary care provider (PCP) if the patient does not have one and support them with local resources such as primary care clinics, health departments, and federally qualified health centers. A referral to a PCP is completed for patients who prefer a contraceptive method that is not in the pharmacist’s scope, who have elevated blood pressure, or have a comorbidity considered category 3 or 4 in the Centers for Disease Control and Prevention United States Medical Eligibility Criteria for Contraceptive Use (US MEC).16,17
Objectives
This study evaluated pharmacy characteristics, patient characteristics, and pharmacists’ interventions during the first year and a half of pharmacist-prescribed contraception in NC.
The objectives of this study were to: (1) determine the types and location of pharmacies that provided HC services during the first year and a half of implementation (eg, early adopters) in NC; (2) evaluate the characteristics of patients who received birth control services from pharmacists; and (3) describe interventions provided by pharmacists during a contraception visit.
Methods
Pharmacists who completed the NC training are termed “contraception pharmacists” in this study. Contraception pharmacists and their email addresses were identified through a query of the North Carolina Association of Pharmacists (NCAP) HC training database. NCAP oversees HC training and maintains a registry of all pharmacists who have completed a required, five-hour, self-paced, online training. Association newsletters advertised the study and invitations to participate were distributed to contraception pharmacists via email. Two follow-up emails were sent in 2-week intervals. Inclusion criteria included completion of the required NCAP HC training, implementation of contraception services, and provision of HC during the study period which approximated the first year and half after prescribing authority was granted (April 2022 – December 2023). Pharmacists who had completed contraception training but did not provide services during the study period were excluded.
Pharmacists interested in participating in the study contacted the research assistant via email to obtain more information. The research assistant explained the study, verified that the pharmacist met inclusion criteria, and scheduled a virtual meeting for those who agreed to participate. During the virtual meeting pharmacists were consented to the study, completed an online demographic survey in Qualtrics® about their pharmacy, and created a login and password for a secure website where they were asked to upload de-identified HC encounter documentation. Specific pharmacy characteristics collected included pharmacy type (chain, independent, grocery store, other), pharmacy location (rural, suburban, urban), and NC county and region (western, central, eastern). Definition of rurality was based upon county classification from the NC Rural Center 18 and NC regions were defined by state classification. 19 Demographic data about the pharmacists and where they provided HC services was summarized using descriptive statistics from the Qualtrics® survey.
During in-person patient encounters, pharmacists utilized standardized, NC Board of Pharmacy (NCBOP)-approved screening and encounter forms that all NC contraception pharmacists are required to use to determine medical eligibility for contraception, document interventions, and make referrals. Patients completed a history form that included demographic information (eg, age, primary care provider, insurance), previous experiences with HC, goals and preferences for contraception, and an assessment of eligibility for contraceptive methods based upon the US MEC. The pharmacists reviewed the forms, completed a blood pressure measurement, discussed contraception options, selected, prescribed and counseled about HC, educated the patient about smoking cessation and folic acid use (when applicable), advised about primary care (for those patients without a provider), and made referrals when necessary. After the visit, pharmacists completed encounter documentation forms which are stored in the pharmacy and sent to primary care providers as required by the NCBOP. Participants were asked to upload de-identified screening and encounter forms to a secure, password-protected Sharepoint® site. A contraception education kit from Birth Control Pharmacist valued at $300 was provided to pharmacists as an incentive for uploading intervention data. Quantitative data including patient demographics, pharmacist interventions, and patient referrals were collected from the de-identified forms, entered into Excel®, and analyzed using descriptive statistics. This study was considered exempt by the University of North Carolina – Chapel Hill Institutional Review Board.
Results
According to the North Carolina Association of Pharmacists, 1309 pharmacists had previously completed the required HC training at the time of the study; however, it was unknown whether all pharmacists had implemented HC services. Seventeen pharmacists volunteered for the study, met the inclusion criteria, enrolled in this study and completed the demographic survey about their pharmacy. Pharmacy types represented in the study included: twelve independent pharmacies (70.6%), 1 free clinic (5.9%), 1 ambulatory care clinic, (5.9%), and 3 “other”. No chain pharmacies were represented. Eight pharmacies were located in rural communities (47.1%), 5 in suburban areas (29.4%), and 4 in urban areas (23.5%). Pharmacy locations represented all 3 geographic regions of NC including western, central, and eastern NC.
Patient Demographics and Pharmacist Interventions
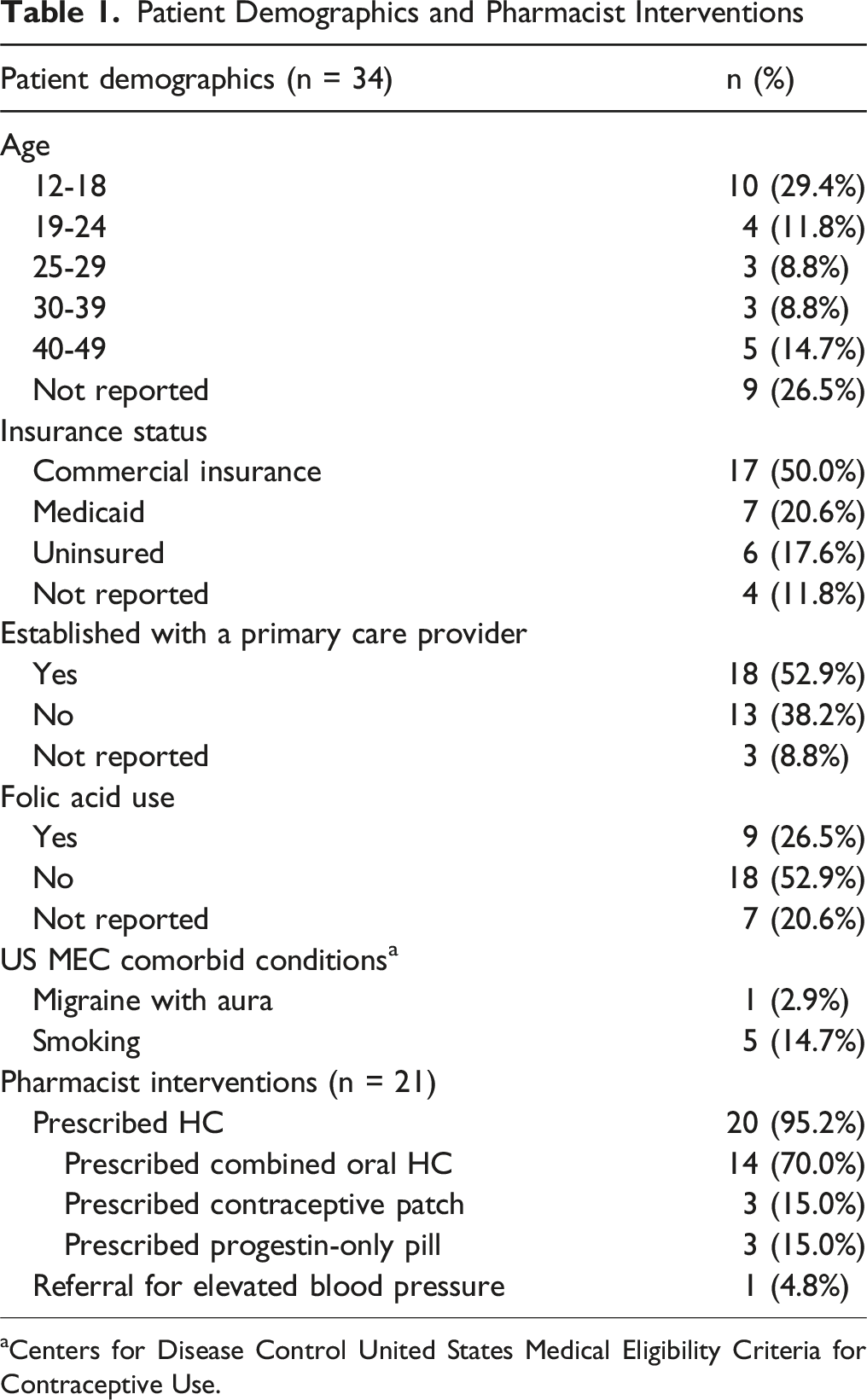
aCenters for Disease Control United States Medical Eligibility Criteria for Contraceptive Use.
Patients reported that they had previously used combined HC pills (76.5%), condoms (26.5%), and depot medroxyprogesterone injection (11.8%) for contraception. One patient reported a history of migraine with aura (2.9%) and was not eligible for an estrogen-containing produce per the US MEC. Fourteen percent of patients were current smokers, and 26.5% were taking folic acid.
Complete pharmacist intervention data was provided for 21 patients. A hormonal contraceptive was initiated in 20 patients (95.2%), and 1 patient was referred to primary care due to elevated blood pressure. Of those patients prescribed HC, contraceptives included the combined HC pill (70%), the progestin only pill (15%), and the contraceptive patch (15%).
Discussion
This study determined that early adopters of pharmacist-prescribed HC in NC practiced in independent pharmacies. Pharmacists served women ranging from adolescents to those in their 40s, and it is encouraging to note that almost 1 in 3 patients were age 18 or under, indicating that pharmacists did prescribe contraceptives for adolescents with parental or guardian consent. The most common comorbidities pertinent to the CDC US MEC included smoking and migraine with aura, and 1 patient had elevated blood pressure during the visit, requiring a referral to a primary care provider. In this pilot study, most of the patients who presented to community pharmacies for contraception services did not have contraindications to HC and were eligible for contraceptives within the pharmacists’ scope of practice. Because 1 referral was required, development of relationships with primary care practices is an important element to incorporate into workflow.
Successful implementation of HC services has been described in a case series of chain, independent, and grocery store pharmacies. 20 Challenges to providing care were lack of public knowledge about pharmacist-prescribed HC and the need to market services and receive payment from insurance companies, whereas development of patient care workflows and integration of pharmacy technicians promoted success. 20 A study of 391 grocery store pharmacies in California and Oregon examined characteristics of patients who received contraception services from pharmacists. 21 Patient encounters were evaluated (n = 676) and indicated that 74% of patients had health insurance compared to 70% in our cohort; whereas, approximately half of patients (53%) in our study self-reported that they had a current primary care provider (PCP) compared to the majority (89%) of the California and Oregon cohort. 21 Prescribing patterns in both studies favored combined oral HC and most patients were previous pill users, aligning with national prescribing trends reported by the CDC that indicate 79.8% of US women age 15-49 have used the pill, 10.4% have used the vaginal ring and 8.2% have used the patch. 22 Patients in our study were less likely to have a primary care provider than the Oregon study and pharmacists are well-positioned to provide reproductive health services for those without a primary care home.
A retrospective cohort study in Oregon evaluated Medicaid claims data for pharmacist prescribing for 367 patients. Data were sourced from Medicaid prescription claims, and 94% of claims were submitted from chain pharmacies in urban locations, 23 indicating a higher uptake of contraception services in chain pharmacies in Oregon than was experienced during the rollout of services in NC where independent pharmacists were early adopters.
In this study 14% of patients reported that they were current smokers and only 1 in 4 women were taking folic acid; consequently, it is important for contraception pharmacists to counsel patients about smoking cessation and the benefits of a multivitamin. A national sample of nonpregnant women aged 15-44 indicated that 20% were current smokers, 24 and pharmacist interventions using pharmacotherapy and counseling positively impact quit rates. 25 NC legislation authorizing pharmacists to initiate HC also included folic acid and nicotine replacement therapy 16 which are important components of preconception care and promote healthy pregnancies. 26 Our data indicate that pharmacists should look beyond HC to incorporate other important aspects of preconception care into contraception encounters.
Since this study, pharmacist-prescribed contraception in NC has expanded so that 93% of counties have at least 1 pharmacy providing care. 27 A survey of contraception pharmacists in NC (n = 96) determined that services were provided in chain pharmacies, independent pharmacies, ambulatory care, and health system pharmacies, indicating that contraception services were available in more settings than what we found in our early adopter study. 28 However, only 15.6% of respondents had prescribed contraception, and reported multiple barriers including time constraints (53%), reimbursement (41.9%), employer/management restrictions (41.9%), patient reluctance (20.9%), professional liability concerns (17.2%), and inadequate training (6.1%). 28
Limitations to this study exist and include the small sample size of pharmacist participants and incomplete documentation of patient encounters. Given the small number of patient encounters reported, the generalizability of these findings is limited. Pharmacists reported that the workflow for uploading patient forms in the study was burdensome, leading many to complete only the pharmacy demographic survey and not report patient encounter forms that documented interventions. Data may not be generalizable to all pharmacies due to the low response rates overall, and no data was available from chain or grocery store pharmacies. The study population did not include all contraception pharmacists in NC, creating selection bias.
Conclusions
In this pilot study of NC pharmacists, early adopters of hormonal contraception services were primarily independent community pharmacists in rural and suburban communities, and the most frequently prescribed contraceptive was the combined HC pill. Few women had contraindications to estrogen-containing products per the CDC US MEC, and 1 patient required a referral to a PCP for elevated blood pressure. Approximately half of patients encountered did not have a primary care provider, indicating that pharmacists serve an important role in increasing access to HC and should develop workflows to connect patients with primary care services in their community to receive more comprehensive healthcare services. One in 7 patients were current smokers and few patients were taking folic acid, emphasizing the opportunities for pharmacists to engage in smoking cessation and folic acid counseling for women of reproductive age.
Footnotes
Ethical Considerations
This study was reviewed by the University of North Carolina – Chapel Hill IRB and was considered exempt.
Consent to Participate
Pharmacist participants completed a written informed consent.
Consent for Publication
Does not apply.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Duke Endowment.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The following authors report that they received funding from The Duke Endowment and that they received honoraria for the development and delivery of hormonal contraception training from the North Carolina Association of Pharmacists (Mollie Scott, Amanda Savage).
Data Availability Statement
Data is available in UNC Dataverse.
Previous Presentations of this Work
North Carolina Association of Pharmacists Annual Convention poster presentation – 2024.