
Abstract
Introduction
Chronic kidney disease (CKD) has emerged as one of the leading causes of mortality worldwide, with a global estimated prevalence of 13.4% (11.7-15.1%) or approximately 850 million people. 1 According to the Centers for Disease Control and Prevention (CDC), in 2021, approximately 37 million people were estimated to have CKD in the United States, which accounted for 15% of the US adult population. 2 Type 2 diabetes is the most common cause of CKD and end-stage kidney disease (ESKD). 3 The prevalence of CKD in patients with type 2 diabetes (T2D) is currently 40% and continues to increase. 4 Approximately 90% of patients with CKD lack awareness of their diagnosis, including 2 out of 5 adults being unaware of having severe kidney disease. 5
According to the Kidney Disease: Improving Global Outcomes (KDIGO), a combination of estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) is used to assess the overall kidney function and the presence of kidney damage. Reduced eGFR (<60 mL/min/1.73 m2) for at least three months and/or persistently elevated albuminuria (UACR; ≥30 mg/g Cr) are measured to diagnose and determine the severity of CKD.6,7
Prior to 2019, the standard of care for patients with diabetes and chronic kidney disease (CKD) consisted mainly of achieving optimal glycemic and blood pressure levels and prescribing angiotensin-converting enzyme inhibitors (ACE) or angiotensin receptor blockers (ARBs). These interventions aimed to slow down the progression of kidney damage and reduce the risk of cardiovascular complications, mainly by preventing the progression of albuminuria, especially when applied to patients with early CKD stages.
In 2019, due to robust CV, HF, and CKD outcome data, the ADA added SGLT2is as recommended in their treatment algorithm to all patients with T2D and stage 3 CKD or higher independent of glycemic control. 8 Most recently, in July 2021, the FDA approved finerenone to reduce the risk of sustained eGFR decline, end-stage kidney disease, cardiovascular death, non-fatal myocardial infarction, and hospitalization of heart failure in patients intolerant to SGLT2is. It was added to the ADA Standard of Medical Care in Diabetes in 2022. 9
Finerenone is a non-steroidal mineralocorticoid receptor antagonist (nsMRA) that has been shown to have a high selectivity toward the mineralocorticoid receptor along with a low affinity for steroid hormone receptors. It blocks the effects of aldosterone, a hormone that can cause damage to the heart and kidneys by promoting inflammation, fibrosis, and oxidative stress. 10 The FIDELIO-DKD and FIGARO-DKD trials were two large clinical trials that studied the effects of finerenone in patients with chronic kidney disease (CKD) and type 2 diabetes (T2D). Both studies provided supporting evidence of finerenone significantly reducing the risk of primary outcome events by 18% and 13% in FIDELIO-DKD and FIGARO-DKD, respectively.11,12 Moreover, finerenone has been found to be more efficacious than sMRAs in reducing albuminuria, with a significant reduction in uACR ranging from 21% to 38% among patients with CKD and T2DM. 13 Furthermore, finerenone can reduce the risk of cardiovascular death, myocardial infarction, stroke, and hospitalization due to heart failure in these patients, regardless of their previous history of cardiovascular disease.
Pharmacists have an important role in optimizing finerenone therapy for patients with CKD and type 2 diabetes. They may contribute by: (1) identifying patients who may benefit from finerenone, (2) finerenone initiation, dose adjustment, or discontinuation, (3) assessing and monitoring the appropriateness of finerenone therapy for each patient based on their clinical characteristics, comorbidities, and medication profile and (4) educating and counseling patients on the benefits and rational of finerenone. Moreover, pharmacist-led programs showed increased medication knowledge, a significant decrease in medication adherence from 67.8% to 43.1%, a significant reduction in CKD stage, lower proteinuria, and an overall improvement in the quality of life of patients receiving dialysis.14,15
This review aims to emphasize the role of pharmacists in multidisciplinary kidney care teams during the early detection process of CKD patients, to optimize finerenone therapy by identifying eligible patients, monitoring renal function and potassium levels, providing patient education, and managing drug interactions. It is important for pharmacists to understand finerenone’s place in therapy as well as its mechanism of action and dosing.
Identifying Patients Who May Benefit From Finerenone
Pharmacists can play a valuable role in identifying patients with CKD by ordering eGFR and urine albumin-creatinine ratio (UACR) screening tests for early detection of kidney damage. Pharmacists may also utilize their access to a patient’s medication profile to assess the need for intervention. For instance, the specific drugs prescribed for hypertension and diabetes, in combination with the patient’s eGFR, can detect early-stage CKD and propose pharmacist-intervention required in cases of renal impairment. 16
Given finerenone’s novelty, initially, specialists like endocrinologists, nephrologists, or cardiologists could take the lead on initiating finerenone therapy for appropriate patients. This allows for addressing any initial uncertainties regarding finerenone’s use, such as potential side effects or drug interactions. Also, specialists can refine best practices for using finerenone, including appropriate managing of potassium levels, which can be impacted by the medication
Following this, a gradual transition to broader use in primary care can be considered. As primary care providers become more familiar with finerenone’s profile and established best practices are disseminated, they can confidently integrate finerenone into their treatment plans for suitable patients. 17
Pharmacists may use the following indicators to identify potential candidates for finerenone therapy in CKD patients with T2D: 1. eGFR: Finerenone is recommended for patients with an eGFR of 25 to 90 mL/min/1.73 m2.
18
2. Albuminuria level: Finerenone can be given to patients with moderate albuminuria (UACR of 30 to less than 300 mg/g) or severely increased albuminuria (UACR of 300 to 5000 mg/g). There is limited evidence that supports patients with UACR of less than 30 mg/g as candidates for finerenone therapy.18,19 3. Serum potassium concentration: Finerenone can increase the risk of hyperkalemia, a potentially serious condition. Patients with normal serum potassium concentration (3.5 to 5.0 mmol/L) are recommended for finerenone therapy, while patients with high serum potassium concentration (more than 5.0 mmol/L) are not candidates for finerenone therapy.
20
4. Use of renin-angiotensin-aldosterone system (RAAS) inhibitors: Patients who are already receiving optimal therapy with a RAAS inhibitor, such as an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) may be recommended for finerenone therapy. Finerenone is recommended for patients with persistent albuminuria despite receiving RAAS inhibitors at the maximum tolerated dose.
21
Dose Initiation, Adjustment, or Discontinuation
Finerenone Dose Initial and Maintenance: Renal and Potassium Adjustment.
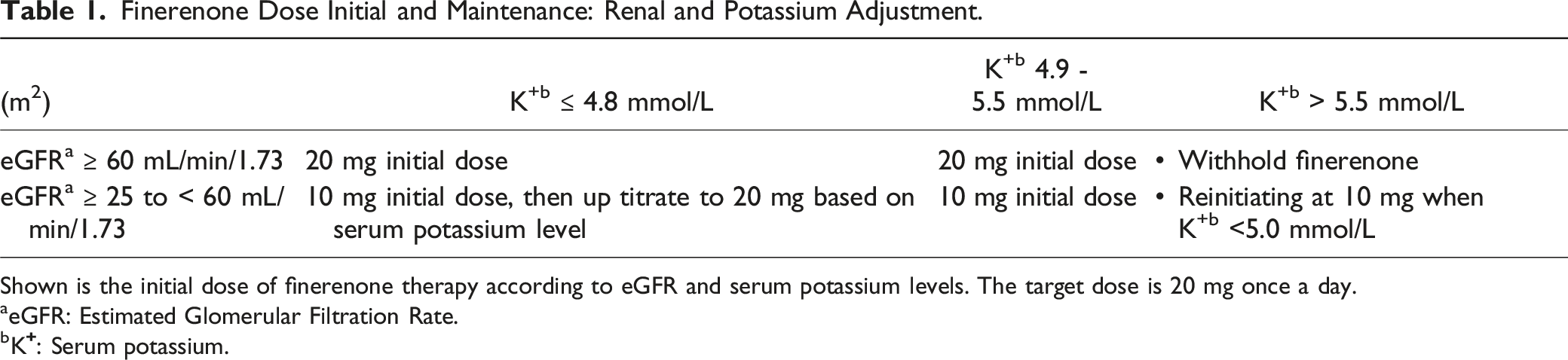
Shown is the initial dose of finerenone therapy according to eGFR and serum potassium levels. The target dose is 20 mg once a day.
aeGFR: Estimated Glomerular Filtration Rate.
bK
Finerenone can be continued upon patient admission, except in case the patient is unable to tolerate the drug due to adverse events such as, hyperkalemia that are not manageable (e.g., dietary changes and/or diuretic use with ACE or ARBs) or such as hypotension. In emergency situations, decisions regarding medication discontinuation should be made based on individual patient assessment and clinical judgment.
Monitoring
Pharmacists in all practice areas have a key role in taking a comprehensive medication history for patients, especially those with chronic or complicated conditions. A summary of all the medications that a patient is currently taking or has recently taken, including prescribed, over the counter (OTC), herbal, and complementary and alternative medicine (CAM) products. 25 It also includes information about adherence, intolerances, allergies, adverse drug reactions, drug interactions, and preferences.
A key benefit of the involvement of a pharmacist as part of the care team is preventing drug-related problems (DRP) and consequential risks to patients. DRPs are common and can occur at any stage of the medication use process, such as prescribing, administering, or monitoring. A recent study found the most common type of DPR for community pharmacists was dosage issues and contraindications/non-conformity to guidelines, 74% and 26%, respectively.26,27 Some common causes of medication errors are attributable to incomplete or inaccurate medication histories, lack of pharmacist-physician communication, and/or lack of patient involvement in the treatment plan. 15
Pharmacists can improve the efficacy and safety of pharmacotherapy, enhance patient adherence and self-management, and prevent complications or hospitalizations by monitoring the patient’s response to therapy. They can also adjust the medications and doses, educate and counsel the patient on their medications, and coordinate with other healthcare providers to provide comprehensive care. Furthermore, they can help detect and manage any adverse effects such as hyperkalemia or hypotension and educate patients about the signs and symptoms of hypotension, 28 which can include dizziness, lightheadedness, fatigue, blurred vision, and fainting (syncope). Some patients may be at a higher risk of hypotension and might require closer monitoring due to existing low blood pressure, dehydration, or severe electrolyte imbalances (particularly potassium depletion).
Pharmacists can help evaluate how well the patient is following the prescribed regimen, how effective the therapy is improving their kidney and cardiovascular function, how well the patient tolerates the therapy without adverse effects, and how the therapy impacts their overall well-being and satisfaction.
Adherence to finerenone therapy can impact effectiveness and safety, in addition to the patient’s risk of complications or hospitalizations. The tolerability of finerenone therapy can be evaluated by identifying any adverse effects or drug interactions that may affect the patient’s comfort or well-being. Pharmacists should monitor these factors periodically and use various methods and tools to measure them, such as questionnaires, scales, interviews, or devices.
Pharmacists should identify any drugs that may interact with finerenone, assess their potential impact on finerenone pharmacokinetics or pharmacodynamics, and avoid or minimize the use of drugs that may increase the risk of hyperkalemia with finerenone. Finerenone is a CYP3A4 substrate. Therefore, it is contraindicated with potent CYP3A4 inhibitors, such as some antibiotics, antivirals, or antifungals. 23 These drugs can increase plasma concentration and exposure to finerenone, which may increase the risk of hyperkalemia or other adverse effects. Similarly, grapefruit and grapefruit juice should be avoided. Caution and monitoring should be considered with moderate and weak CYP3A4 inhibitors and inducers. Finerenone should not be given concomitantly with potassium-sparing diuretics (such as amiloride and triamterene) and mineralocorticoid receptor antagonists (such as eplerenone and spironolactone). These drugs increase the risk of hyperkalemia as they have similar mechanisms of action.
In contrast, finerenone is not contraindicated but should be used with caution and close monitoring with drugs such as ACE, angiotensin receptor blockers (ARBs), direct renin inhibitors (DRIs), nonsteroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase-2 inhibitors (COX-2 inhibitors), heparinoids (such as enoxaparin), trimethoprim-sulfamethoxazole, tacrolimus, cyclosporine A, potassium supplements, salt substitutes containing potassium chloride, or other drugs that may affect potassium balance. These drugs can also increase the risk of hyperkalemia with finerenone, as they can alter the renal excretion or reabsorption of potassium. 29 Additionally, finerenone interacts with lithium by increasing the renal clearance of lithium, which may decrease its serum concentration and efficacy. Finerenone may also interact with drugs that are substrates of certain transporters, such as Breast Cancer Resistance Protein (BCRP), Organic Anion Transporting Polypeptides (OATP1B1, or OATP1B3). 30
Additionally, the impact of finerenone on UACR can serve as an important parameter to evaluate the drug’s efficacy and a patient’s adherence to the prescribed dosage regimen. As finerenone significantly reduces UACR, 13 a key indicator of kidney damage. This reduction in UACR holds additional value. By closely monitoring UACR, pharmacists can gain valuable insights into the effectiveness of finerenone treatment, assess a patient’s response to the medication, and identify non-adherence to the drug regimen, if any.
Discharge Care & Treatment
Pharmacists who practice in acute care settings can reconcile the patient’s discharge medications with their pre-admission and inpatient medications, identify any potential issues with the discharge regimen, educate and counsel the patient on their discharge medications, provide written information or aids to facilitate adherence and self-care, arrange for follow-up care or referrals, and communicate the discharge plan to the patient’s primary care provider or community pharmacist. These additional measures of care can help ensure a smooth transition, prevent medication errors or discrepancies, improve patient understanding and satisfaction, and reduce readmissions or adverse outcomes.
Education and Counseling
The role of a pharmacist may extend to assessing the patient’s educational requirements, preferences, hopes, and objectives. The baseline knowledge, attitudes, preferences, and expectations of the patient towards their ailment and therapy can be evaluated by the pharmacist in all practice settings using a variety of techniques and tools. Pharmacy professionals can utilize this data to customize patient education and counseling to their unique needs and characteristics. 31 Some of the important aspects of education and counseling are the rationale and benefits of finerenone therapy. It involves delaying the progression of diabetic nephropathy, a condition that damages the kidneys and increases the risk of end-stage kidney disease and cardiovascular complications. 32 It also assists in reducing the risk of major adverse kidney events (MAKE) by 18% and major adverse cardiovascular events (MACE) by 14% compared with placebo in patients with CKD and type 2 diabetes. 33 Furthermore, pharmacists can educate patients on the need to regularly monitor serum potassium, eGFR, and UACR levels. They may also review recommended steps should abnormal results appear, especially hyperkalemia since it is the most common adverse effect of finerenone therapy and can cause muscle weakness, fatigue, palpitations, or arrhythmias.
Adherence to finerenone and other medications and lifestyle modification is imperative for patients with chronic kidney disease and type 2 diabetes. 30 Pharmacists can enhance adherence to finerenone by providing medication reminders, refill services, adherence aids (such as pill boxes, calendars, or apps), and follow-up calls or messages to help patients remember to take their medications as prescribed. Pharmacists may further assess patients’ adherence using different methods (i.e., self-report, refill records, pill counts, or electronic devices) and address any barriers or challenges patients may face in adhering to their medications and lifestyle modifications. They may also collaborate with other healthcare providers (i.e., physicians, nurses, dietitians, etc.) to coordinate care, improve patient outcomes, and inform any modification or problem in patients’ medication regimen or level of adherence to the rest of the healthcare team.
Pharmacists have an opportunity to explain potential barriers to patients with respect to finerenone adherence, such as the high cost of the medication and the availability and/or accessibility of the medication. They can expand and improve patient awareness and education about the benefits and risks associated with finerenone. Especially focusing on adverse effects such as hyperkalemia or hypotension and drug interactions with other medications. Finally, pharmacists should also account for emotional factors such as fear, anxiety, depression, stress, or anger that may affect the patient’s mood, attitude, and willingness to take finerenone. 34
Conclusion
The proactive involvement of pharmacists positively contributes to the care of CKD patients and reduces the gaps in current patient care. Enhancing pharmacist-led programs and interacting with patients, physicians, and other healthcare professionals can ensure optimal renal and cardiovascular patient outcomes. There are many opportunities for pharmacists to contribute to the care of CKD patients and optimize finerenone administration, including identifying potential candidates for finerenone therapy, assessing the appropriateness of dosing, and monitoring parameters, conducting regular medication reviews, including dosage adjustment, detecting adverse drug events and drug interactions, and monitoring the therapeutic drug. In addition, they can provide patient education, medication reconciliation, adherence monitoring, and lifestyle modifications for CKD patients.
Supplemental Material
Supplemental Material - Optimizing Finerenone in People With Diabetes and Chronic Kidney Disease: An Opportunity for the Pharmacist
Supplemental Material for Optimizing Finerenone in People With Diabetes and Chronic Kidney Disease: An Opportunity for the Pharmacist in Jennifer D. Goldman in Journal of Pharmacy Practice
Footnotes
Acknowledgments
The author would like to acknowledge the medical writing support provided by Sherif Shamseldein, MBBCH, MMSCI, MPH, of ILM Consulting Services, LLC, which was funded by Bayer US, LLC. The authors would also like to acknowledge the editorial support, visualizations and graphical abstract development provided by Aqsa Dar, ScM, of ILM Consulting Services, LLC, which was also funded by Bayer US, LLC. ILM’s services complied with international guidelines for Good Publication Practice (GPP 2022).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bayer US, LLC funded the article processing charge for this article. Bayer US, LLC also funded ILM Consulting Services, LLC for medical writing support and publication management.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.