
Abstract
Keywords
Introduction
Community pharmacists in Australia play an integral role in diagnosing and providing symptomatic relief of nausea and/or vomiting (N/V). 1 Supply of anti-emetics by pharmacists is currently limited by scheduling of medications by the Therapeutic Goods Administration (TGA). In Australia, serotonin (5-HT3) antagonists, such as ondansetron (administered orally or via injection) and granisetron (administered orally or via injection) are prescription-only-medications (Schedule 4, S4).2,3 Dopamine (D2) antagonists, such as prochlorperazine (administered orally) are pharmacist-only-medications (Schedule 3, S3) and may be supplied over the counter (OTC) specifically for the treatment of nausea associated with migraine 2 (Supplementary material S1).
Down-scheduling 5-HT3 antagonists to S3 pharmacist-only-medications may provide additional options for pharmacists to consider when treating N/V. Presently, the perceptions of pharmacists on the down-scheduling of 5-HT3 antagonists is limited. This study aimed to gather community pharmacists’ perceptions on the down-scheduling of oral 5-HT3 antagonists to S3, specifically regarding their opinions on their efficacy and safety and to determine if they possess the knowledge and training to safely provide them.
Methods
An anonymous survey (developed using Qualtrics and accessible via QR code) was disseminated via social media and the research team’s personal network (including direct email to 51 pharmacies in South Australia) during April and May of 2023. Participants were required to be (i) at least 18 years old, (ii) a pharmacist registered with the Australian Health Practitioner Regulation Agency, and (iii) practicing as a community pharmacist.
Participants responded to short-answer and Likert scale multiple-choice questions regarding the safety and efficacy of D2 antagonists and 5-HT3 antagonists. The pharmacists’ level of training and their clinical skills in providing these medications safely were also explored. Results were exported to Microsoft Excel for analysis. Short answer questions were thematically analysed using Delve 2023. The study was approved by the UniSA Human Research Ethics Committee (ID 205449).
Results
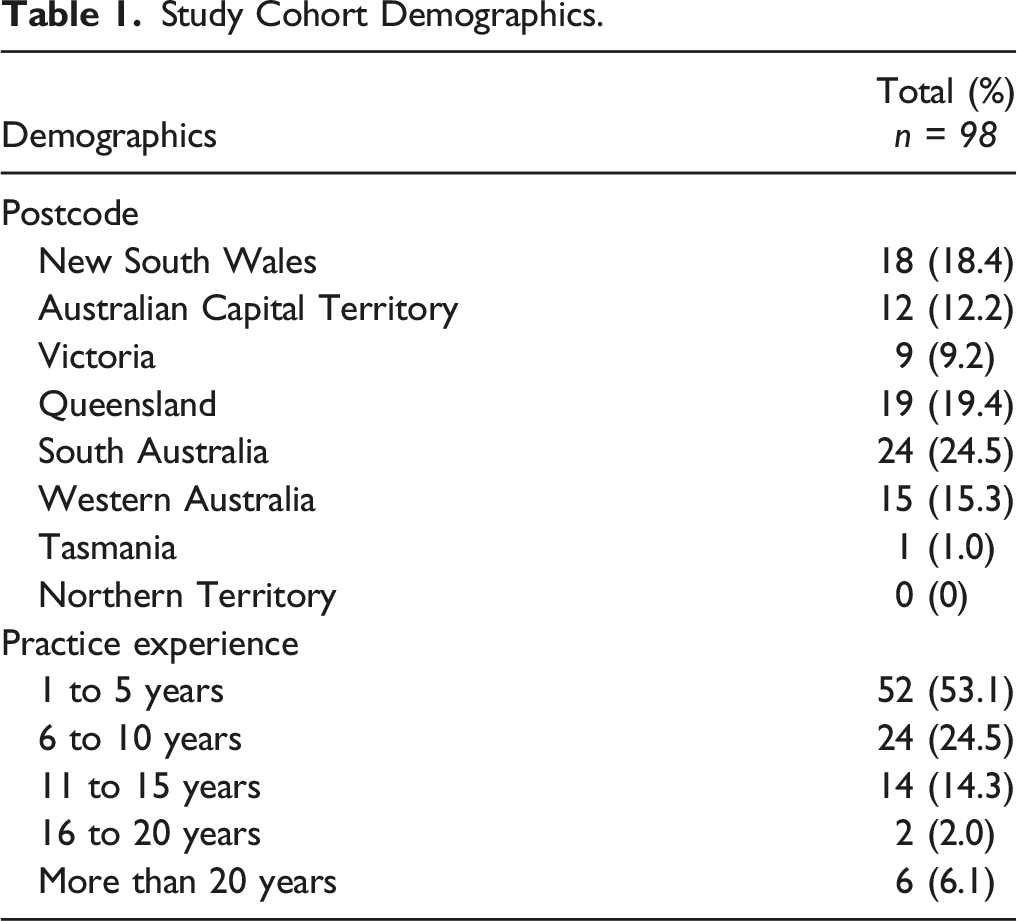
Study Cohort Demographics.
The majority of participants (n = 84, 86%) had supplied an oral D2 antagonist for an OTC N/V request. A significant number (n = 96, 98%) perceived oral D2 antagonists to be effective in managing N/V as compared to oral 5-HT3 antagonists. The remaining 2% (n = 2) perceived oral D2 antagonists not to be effective compared to 5-HT3 antagonists. When asked how often patients reported experiencing side effects whilst taking oral D2 antagonists, 5% (n = 5) reported ‘regularly’, 63% (n = 62) reported ‘occasionally’ and the remaining 32% (n = 31) reported ‘patients had never reported side effects’. In comparison, 3% (n = 3) reported patients taking 5-HT3 antagonists would experience side effects ‘regularly’, 39% (n = 38) ‘occasionally’ and the remaining 58% (n = 57) reported ‘patients have never reported side effects’.
There were 87 participants (89%) who believed that oral 5-HT3 antagonists should be down-scheduled to S3 while 11% (n = 11) said they should not. When asked if pharmacists could safely supply oral 5-HT3 antagonists as OTC, 92% believed they could whilst 8% believed they could not.
Discussion
Pharmacists’ Responses.
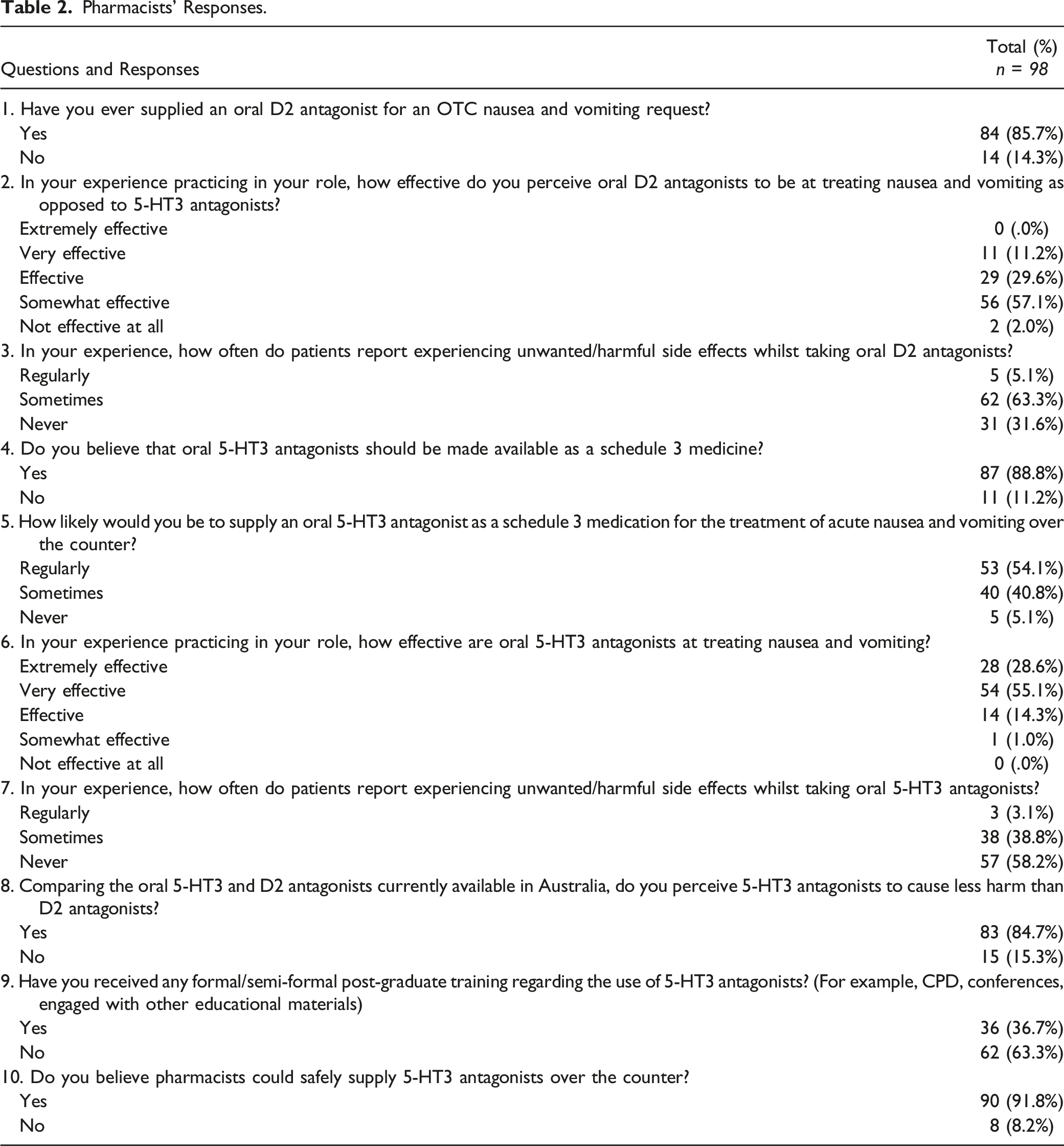
Participants (n = 83, 85%) believed that oral 5-HT3 antagonists cause less harm than oral D2 antagonists (Supplementary material S2). Prior literature has suggested that both classes of anti-emetics are equally tolerable. 6 Despite acceptable tolerability, D2 antagonists can cause extrapyramidal side effects 7 and 5-HT3 antagonists may harm the foetus during first trimester of pregnancy. 8 Pharmacists did show concern regarding 5-HT3 antagonists and pregnancy, mentioning “pregnancy is an area that should be overseen by a medical practitioner” and that down-scheduling could “decrease general practitioner involvement in pregnancy-induced nausea”. Concerns regarding constipation were raised with 5-HT3 antagonists, as one pharmacist mentioned “side effects such as constipation are common” and another mentioned there would be an “increased need for medications to treat constipation”. Pharmacists also raised concerns about QTc prolongation with 5-HT3 antagonists. This was part of the reason why the TGA decided to not down-schedule ondansetron in 2020. 4 While 5-HT3 antagonists have been reported to cause QTc prolongation, this adverse effect is mainly associated with high dose and intravenous administration in patients with risk factors for Torsades de Pointes. 9 In a primary health care setting, patients would be treated with an orally administered 5-HT3 antagonist. Furthermore, when used short term in patients without such risk factors, there is minimal risk for QTc prolongation. 9 Appropriate counselling of such risks when supplying 5-HT3 antagonists is therefore recommended to prevent patient harm.
Pharmacists were most concerned about masking the underlying cause of N/V (Supplementary material S3). Several pharmacists (n = 21, 21%) said that down-scheduling could lead to patients not seeking appropriate medical advice. If oral 5-HT3 antagonists were to be down-scheduled, guidelines for pharmacists to diagnose the specific type of N/V and supply the medication must be developed and implemented. A perceived lack of training (n = 63, 63%) was the most commonly reported barrier to down-scheduling of 5-HT3 antagonists (Supplementary material S3), reinforcing the need for guidelines and appropriate training to ensure safe supply of 5-HT3 antagonists as OTC medicine. Training may include assessment of skills related to diagnosis and treatment of N/V, professional collaboration with medical practitioners through partnered prescribing. Moreover, development and completion of continuing education modules that include real-life case studies would assist pharmacists to analyse cases and determine treatment approaches.
There are several limitations to consider. Firstly, this study included 98 participants who were mostly recruited from social media and the majority (n = 52, 53%) were early career pharmacists. This sample of pharmacists may not represent the diversity of opinions of all pharmacists as there are an estimated 21,000 community pharmacists in Australia. The study had a high exclusion rate as 48% (n = 60) of participants did not complete the entire survey. A pilot study of pharmacist-diagnosed N/V and supply of 5-HT3 antagonists as S2 medicines is required to determine safety of down-scheduling and provision of these medicines by pharmacists before another submission to amend the scheduling of 5-HT3 antagonists is made in Australia.
Conclusion
This is the first study to investigate pharmacists’ perceptions upon the down-scheduling of 5-HT3 antagonists in Australia. Pharmacists perceive 5-HT3 antagonists as safe, effective and superior compared to D2 antagonists; supporting the down-scheduling of oral 5-HT3 antagonists to S3 medications to treat acute nausea and vomiting in the community.
Supplemental Material
Supplemental Material - Understanding Australian Pharmacists’ Perceptions on the Utilisation of Oral 5-HT3 Antagonists as Pharmacist-Only Anti-Emetics in Comparison to Oral D2 Antagonists
Supplemental Material for Understanding Australian Pharmacists’ Perceptions on the Utilisation of Oral 5-HT3 Antagonists as Pharmacist-Only Anti-Emetics in Comparison to Oral D2 Antagonists by Aiden Hendry, Jack Janetzki, and Wern Chern Chai in Journal of Pharmacy Practice.
Footnotes
Acknowledgements
The authors would like to thank all community pharmacists for their support in recruiting participants for this study.
Author Contributions
AH formulated the survey questions, promoted the survey, data interpretation and wrote the article; JLJ designed the study, formulated the survey questions, promoted the survey, data interpretation and wrote the article, WCC designed the study, formulated the survey questions, promoted the survey, data interpretation and wrote the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Access Statement
The data are stored as de-identified, password protected files within the University of South Australia: Clinical and Health Sciences network drive.
Data Availability Statement
The data will be shared on reasonable request with the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.