
Abstract
Introduction
Community pharmacies are often the first point of contact for patients and may be the only interaction that a patient has with the healthcare system.1–3 Recent years have seen a tremendous growth and significant changes in the services provided by pharmacists both locally and internationally. From retailing and sourcing, manufacturing and supplying of medicines (dispensers and store-keepers) pharmacists have evolved as healthcare professionals having active involvement in team-based patient care and performing more clinically orientated activities. 4
The education of pharmacists has traditionally focussed on manufacture and supply but in recent years the focus has shifted solidly to patient-centred care. 5 Approximately 75% of pharmacists in New Zealand (NZ) practice as community pharmacists. 3 Community pharmacies primarily service their local communities by ensuring appropriate medicine supply and offering a range of other services such as advice on medicines use, health consultations, INR/warfarin monitoring, emergency contraceptive prescribing, blood pressure checks, and vaccinations, to name a few. 6
Pharmacy services and practices in NZ are expanding as the landscape in community pharmacy continues to change with policy-directives calling for pharmacists to be more accessible for patient care and consultations and free up their time from the medicine supply function. Pharmacists are taking on more clinical roles in community pharmacies with wider scopes of practice.7–9 Being accessible, and as a first point of contact with patients, pharmacists can make a huge difference in health outcomes through optimizing medicines use, especially in collaboration with other health professions. 3 Some examples where pharmacists in NZ are helping improve outcomes are in reducing medication related adverse effects and hospital admissions by undertaking comprehensive medicines reviews.10–13
Considering the changing face of the pharmacy profession in NZ and the need to increase public awareness of advanced pharmacy services, the Pharmaceutical Society of New Zealand (PSNZ) created a video entitled ‘Get to know your local pharmacist’ and released it on Youtube® in September 2018. The aim of the video was to promote the full range of services provided by pharmacists and to increase community awareness of these. The video was uploaded in 3 different versions with version 1 aimed at a Māori (indigenous people of NZ) audience, and versions 2 and 3 with female and male voiceovers respectively. However, none of the versions appear to have attracted a large number of viewers on YouTube and up until April 2020 when this study was conducted, the total number of views across all the versions was 512 with 291 as the highest number for a single version (the Māori version).
As a result of this low engagement there was concern about the effectiveness of these videos in raising public awareness about pharmacy services. This could be attributed to the unsuitability of Youtube® as a sharing platform, especially in the absence of focused promotion, the public being aware of pharmacy services through other means, or because the public is somewhat apathetic about knowing the services offered by their local pharmacy. Therefore, an evaluation needed to be performed to determine what the impact of promotional videos about pharmacist services has on the public’s perception of pharmacy and their intended uptake of these services.
Patient satisfaction has long been considered an important factor in determining the quality of patient care delivered. 14 It is critical that healthcare consumers have a better awareness of the roles and responsibilities of pharmacists in order to improve the pharmacist-patient relationship and patients’ satisfaction with pharmacy services. 15 Despite the fact that the pharmacy profession is steadily transitioning from product-focused to patient-centred care in a multi-disciplinary environment, the international literature suggests that patient and public awareness and subsequent uptake of pharmacy services has been limited.16–24 This study aims to explore whether the PSNZ promotional videos were an effective intervention for educating New Zealanders about the range of pharmacy services available and whether they were likely to enact any behavioural change in consumers around pharmacy engagement.
Methods
A ‘before-after’ study design was employed. 25 The PSNZ video was used as an intervention and participants’ knowledge and awareness of the range of pharmacy services available was assessed before and after watching the video. In addition, participants were asked about the impact of the videos on their intended future use of pharmacy.
Study Participants
Participants were members of the public aged 18 years or older with access to the internet and a computer, tablet, or smart mobile phone with the ability to fill out the survey.
Questionnaire
A self-administered online questionnaire was used for data collection. The questionnaire contained 24 questions. The first 6 questions gathered relevant demographic information. The following 4 questions assessed participants’ awareness and utilisation of a range of pharmacy services. The next 3 questions were on participants’ awareness about PSNZ and the promotional video followed by a link to the video which they were asked to watch. The final eleven questions asked participants to report whether the video had changed their knowledge and perception of pharmacy services, likely future use of services, and requested feedback on the video. The questionnaire used both open and close-ended questions.
Data Collection
Following ethical approval (ref: D19/379) from the University’s Human Ethics Committee (Anon University), the survey was piloted with 30 participants who were expected to be similar to the respondents. Minor amendments to improve the clarity of the questions were made following the pilot. The finalized survey was then sent out to 1 127 randomly selected members of the public with the help of a survey company (SurveyEngine®) who also assisted in the piloting phase.
Data Analysis
Quantitative demographic data was summarised using descriptive statistics and reported as frequencies and percentages.
In analyzing and reporting the “pre and post” behaviours, due to the paired, nominal nature of the data, McNemar’s test 26 was used to analyse the significance of differences between visiting a pharmacy for health concerns before and after the intervention. A P value <.05 was considered statistically significant.
Qualitative analysis of responses to open-ended free text questions were analysed using content analysis. Content analysis represents a formal approach to qualitative data analysis when faced with a mass of open-ended material to make sense of. 27 Data was coded to build overarching themes and sub-themes within the questions asked; supported by quotations linking interpretation to data. In line with the positivistic content analytic process, themes and sub-themes emerged from the analysis and were presented in a table. Their attribution was outlined in the form of frequencies and percentages of the respondents whose responses included a particular theme. 28
Results
Participant Demographics
Demographic characteristics (n = 329).
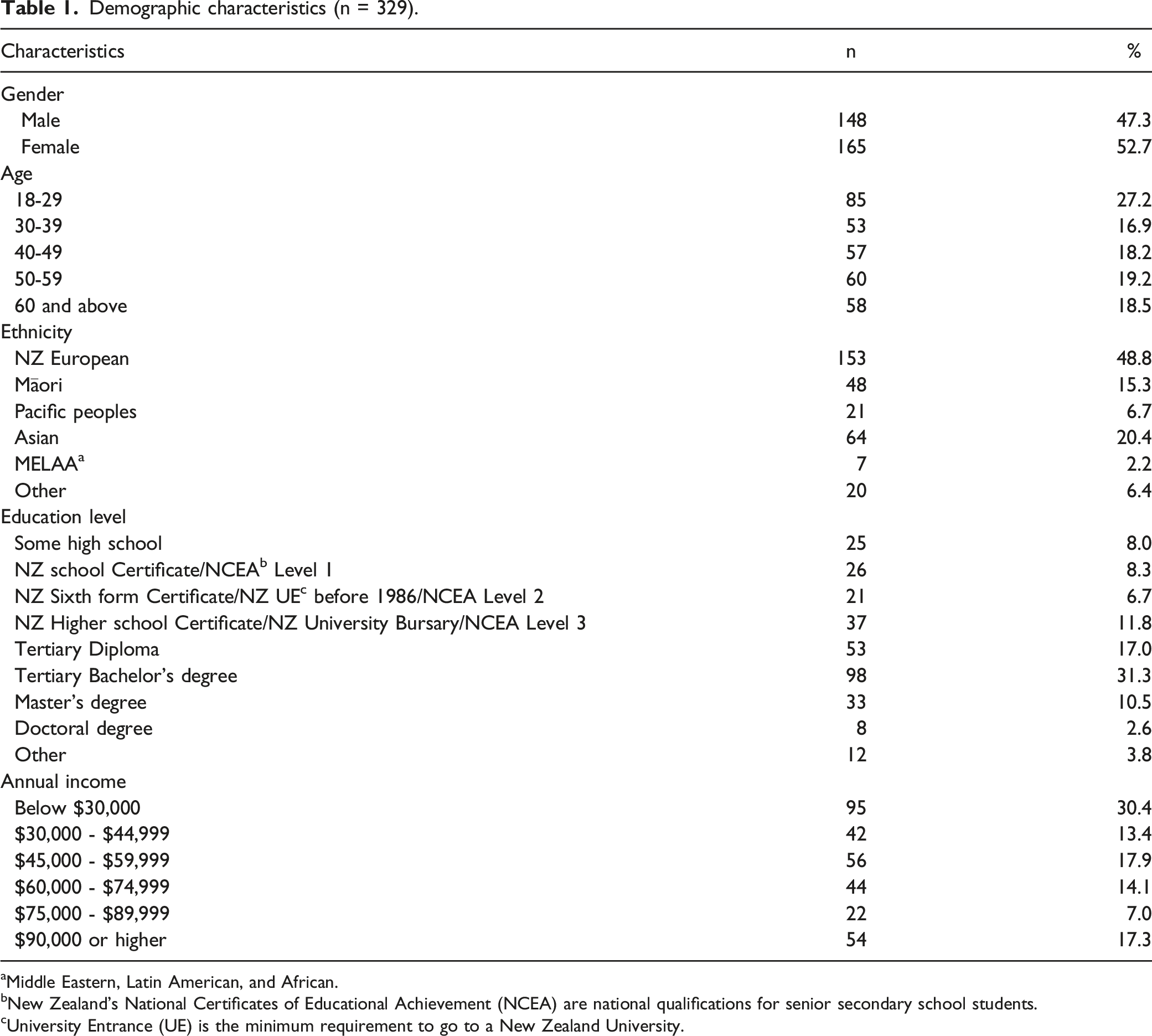
aMiddle Eastern, Latin American, and African.
bNew Zealand’s National Certificates of Educational Achievement (NCEA) are national qualifications for senior secondary school students.
cUniversity Entrance (UE) is the minimum requirement to go to a New Zealand University.
Just over two thirds (67.7%) of the participants regularly visited a pharmacy and of these over half (51.4%) visted for prescription filling. The remainder visited for purchasing OTC medicines, supplements, personal care products and cosmetics, and for consulting with pharmacists about their medications.
Awareness and Pharmacy Service Utilisation
Awareness and use of pharmacy services.
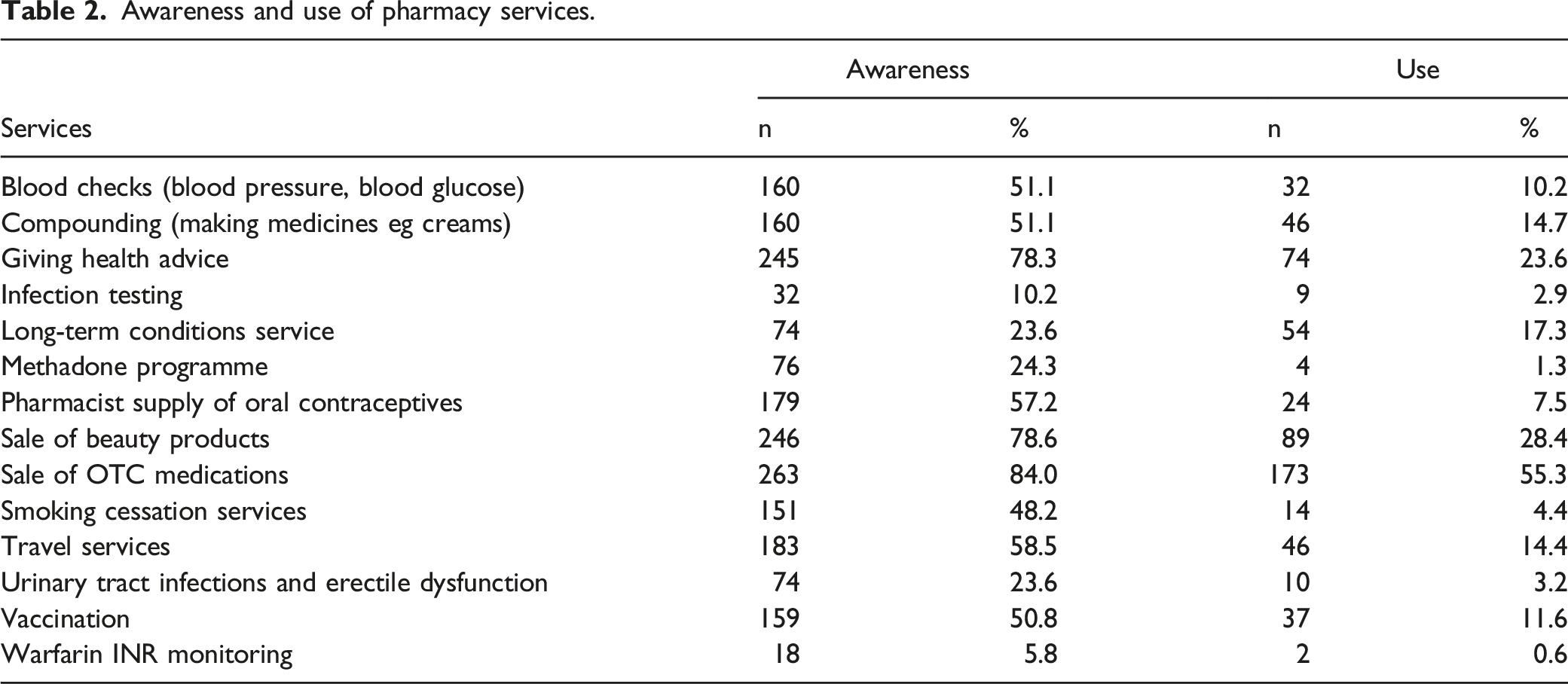
Similar patterns but with lower percentages were observed in terms of actual use of services with sale of OTC medicines (55.3%), sale of beauty products (28.4%), and giving health advice (23.6%) as the most frequent reasons, and warfarin INR monitoring (.6%), methadone programme (1.3%), infection testing (2.9%), and treating UTI and erectile dysfunction (3.2%) as the least commonly used services.
Of the 313 respondents only 13 (4.2%) reported an awareness of the PSNZ promotional videos but no respondents had watched them. However, after watching the video nearly three-quarters (74.1%) reported a change in their perception of pharmacy services. Figure 1 highlights that out of those who reported a change in perception, the majority (n = 210; 90.5%) reported an increased awareness of pharmacy services and greater than one-third (n = 94; 40.5%) reported an increase in their trust for the pharmacy profession. Perceptions of the pharmacy profession.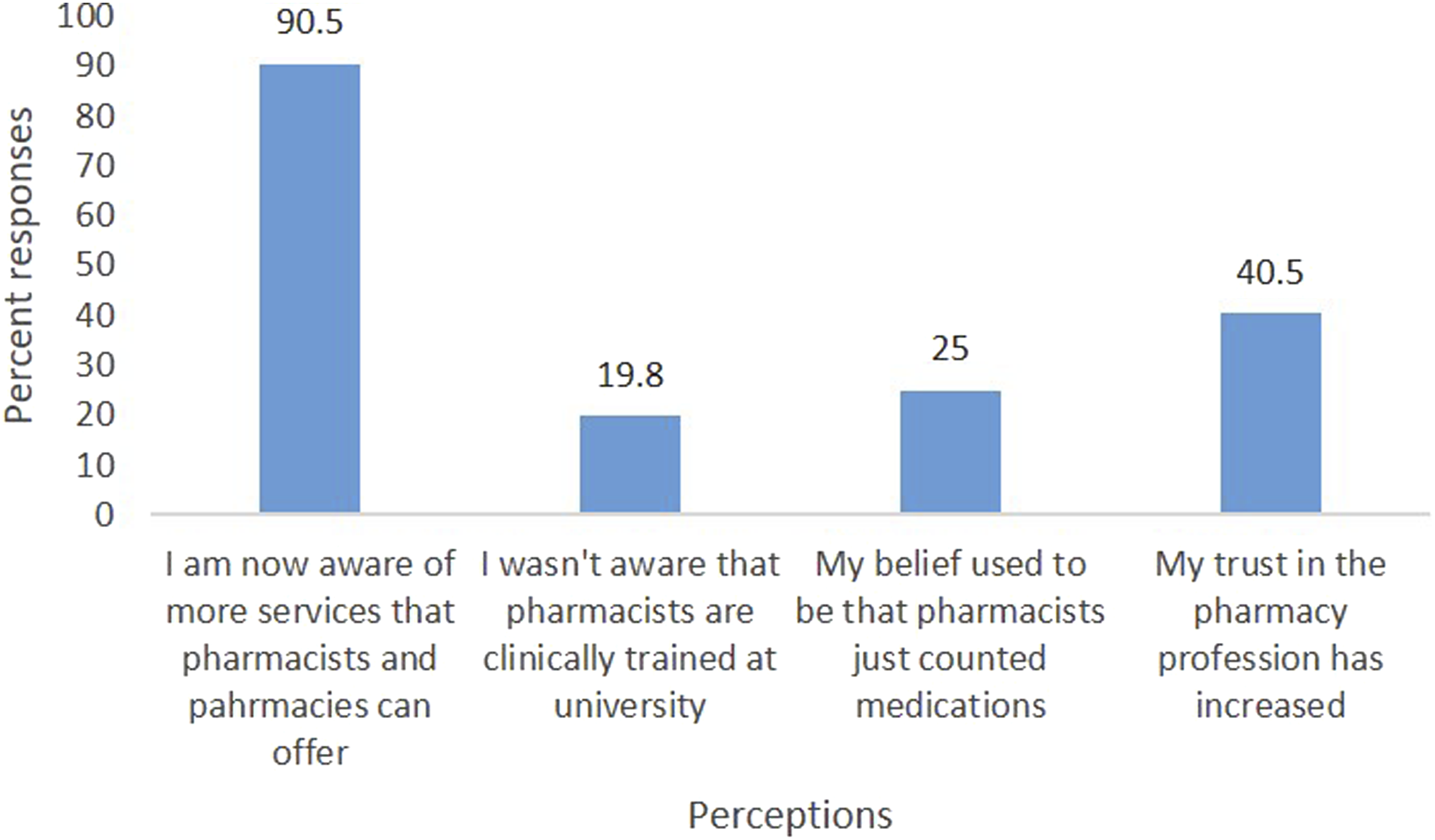
No Change in Perceptions Following the Video
For the half of respondents who reported no change in perception of pharmacy after watching the video, the most common reason cited was that they were already aware of or had positive opinion about the services highlighted in the video (n = 46; 56.8%). This can be inferred from the following quotes: “I already had a positive opinion, this just reinforced my thoughts.” (Participant 211) “Nothing would change my perception as I already know what pharmacies offer.” (Participant 300)
Another reason for no perception change reported by nearly 10% (n = 8) of participants’ was ‘resistance to acknowledge the pharmacist as an essential member of the health‐care team’ as described in the following quotes: “Too used to seeing the doctor beforehand.” (Participant 269) “They are not doctors or nurses.” (Participant 136)
A total of 6.1% of the responses were categorized as related to the video quality and content that weren’t effective enough to change the perception, as described in the following quotes: “The video never really grabbed my attention as the visuals weren’t filmed video.” (Participant 318) “It seemed to give relatively general information.” (Participant 224) “Not very clear.” (Participant 218)
The remaining 27.1% of the respondents whose perception did not change after watching the video did not cite any reason.
Before After Results
In response to the question whether respondents (or one of their family members) would be more likely to visit a pharmacy in the future after watching the video, nearly two thirds (63.2%) selected ‘yes.’
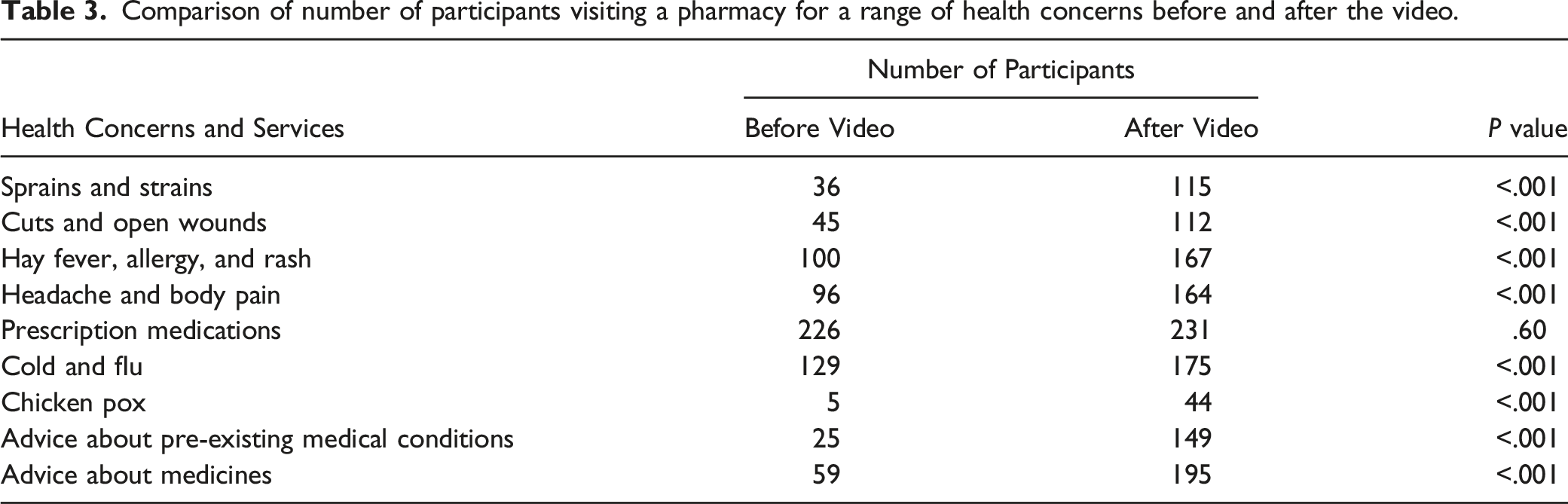
Comparison of number of participants visiting a pharmacy for a range of health concerns before and after the video.
Participant Feedback on Videos
The results of the survey question asking the participants to rate the promotional videos on a scale of 5 are presented in Figure 2. The largest proportion (n = 132; 42.2%) rated the video as a 4 suggesting that they enjoyed the video but it wasn’t the best, followed by 92 (29.4%) who really liked the video and rated it as a 5. Perceptions of PSNZ promotional videos.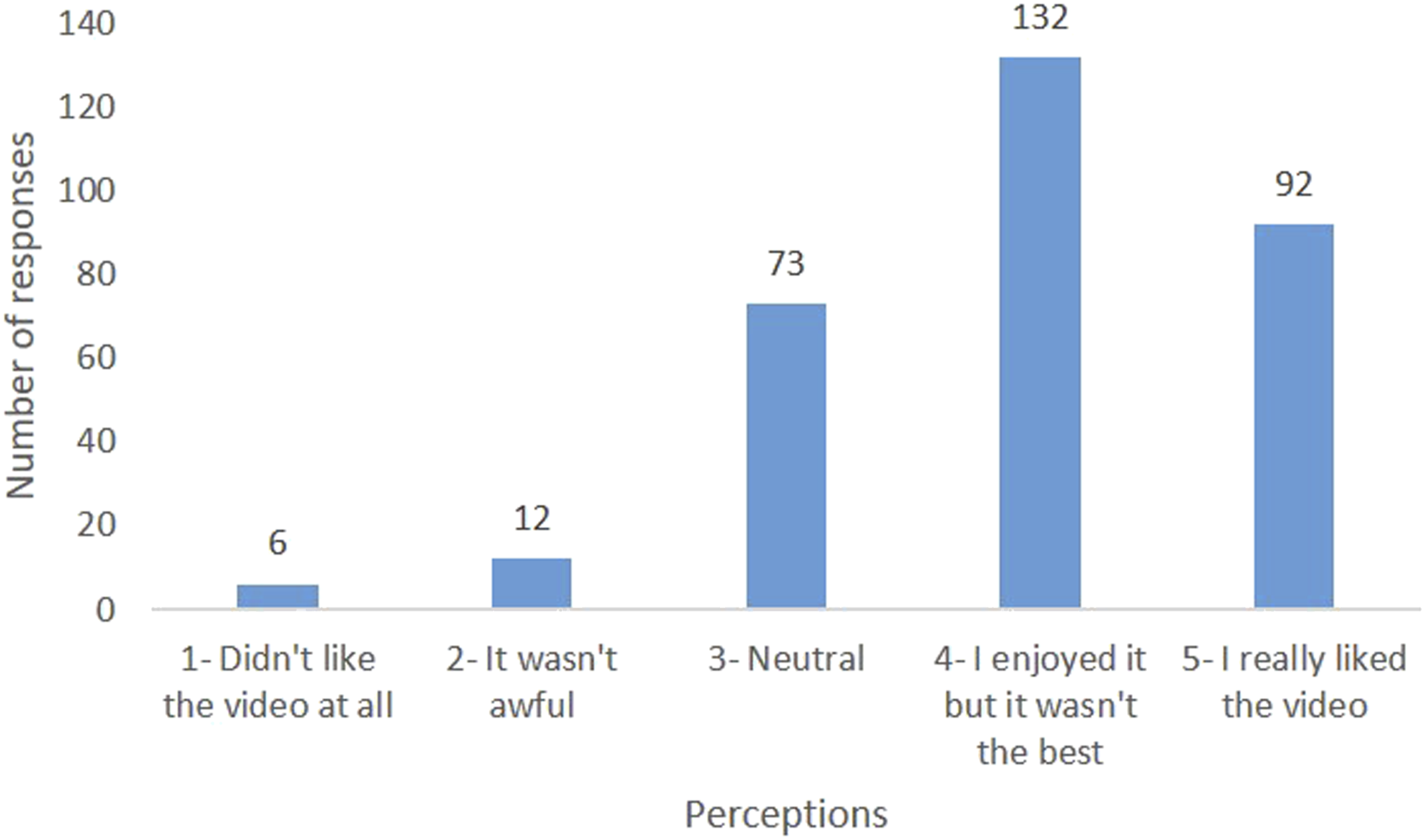
When asked whether they had any positive feedback about the video intervention, 264 (84.3%) thought that the video was informative and only one-third 104 (33.2%) found it relatable. This is presented in Figure 3. Positive feedback on PSNZ promotional videos.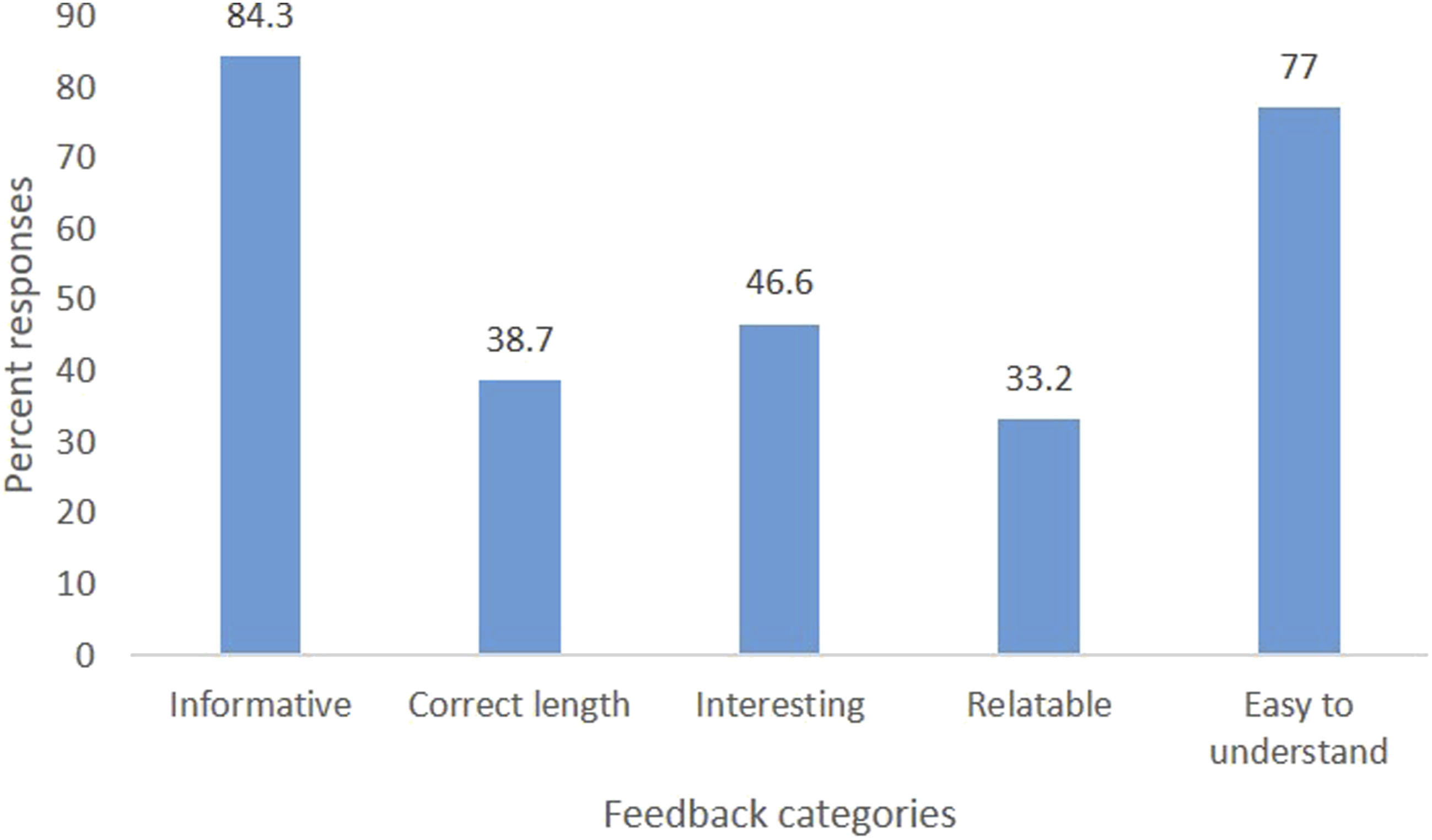
Figure 4 summarises the negative feedback about the videos. A total of 125 (40.0%) participants thought that the video was ‘too long’ followed by 36 (11.5%) who found it ‘boring.’ However, only a small proportion 5 (1.6%) had difficulty in understanding the content of the video. Negative feedback on PSNZ promotional videos.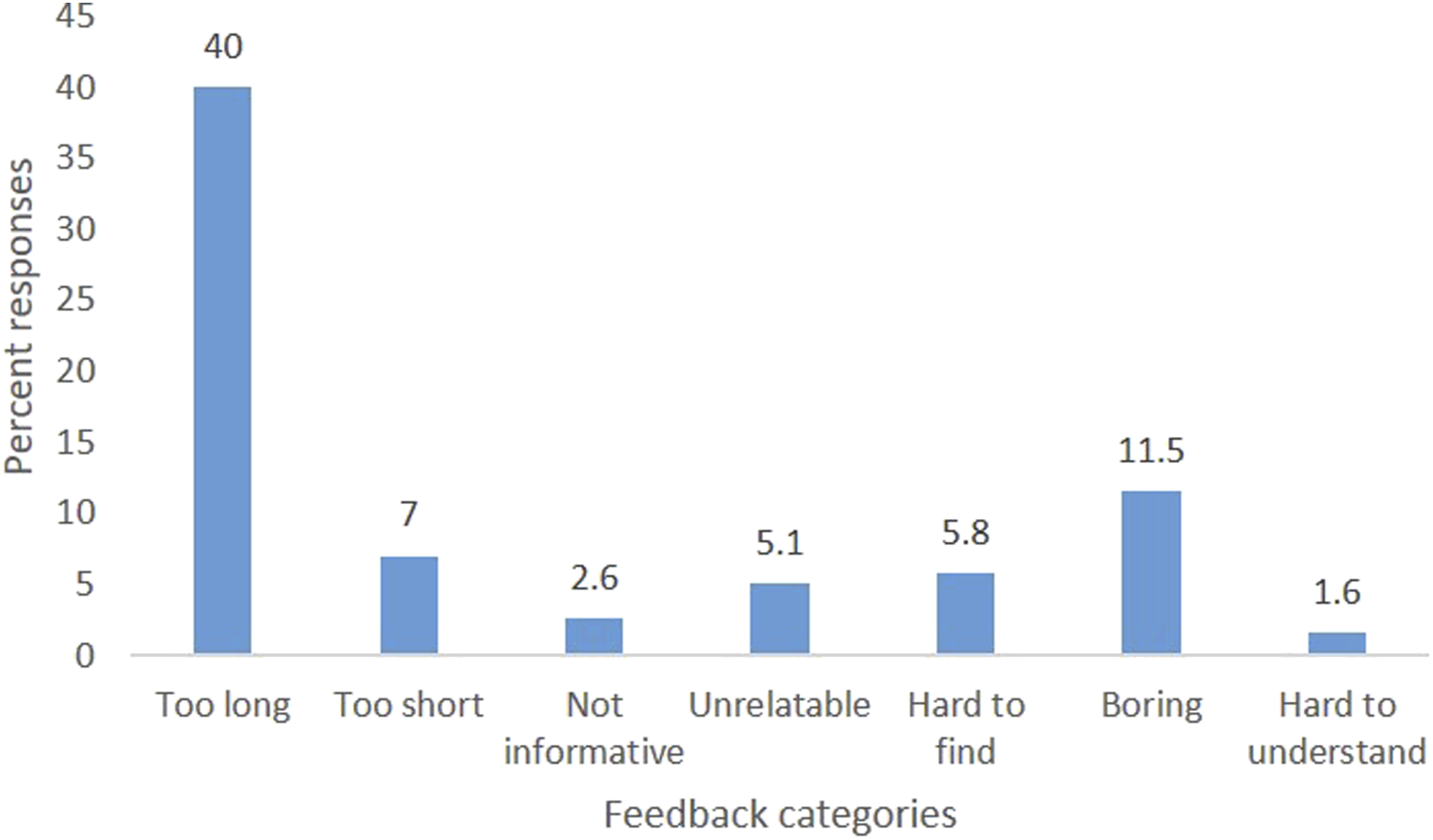
Free-Text Content Analysis
Free text thematic analysis.
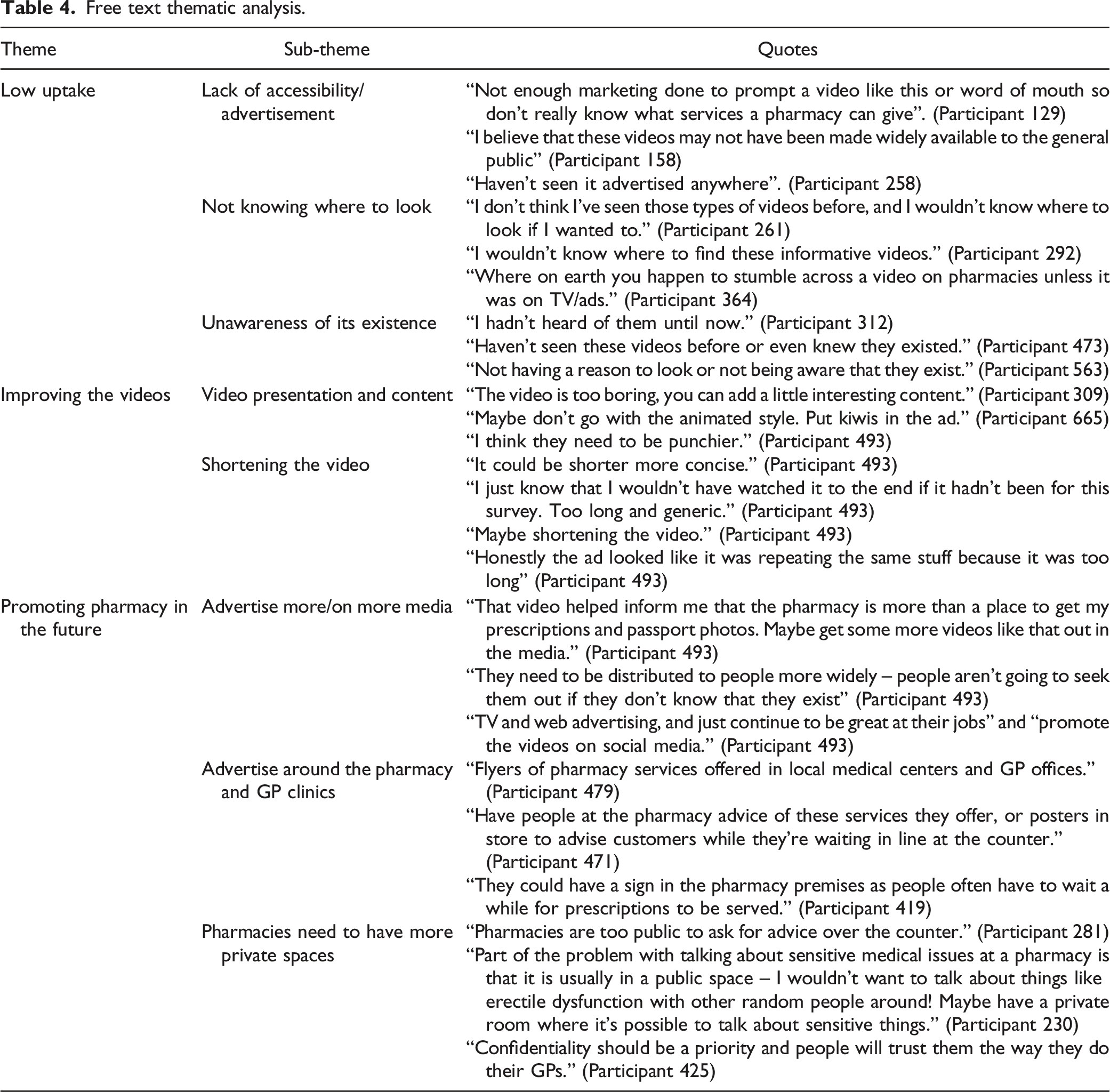
Low Uptake
Three prominent sub-themes were identified from the free-text responses to the question on reasons for low uptake of the PSNZ videos. These included ‘Lack of accessibility/advertisement’ (25.4%), ‘Not knowing where to look’ (23.7%), and ‘unawareness of its existence’ (16.6%).
Improving the Videos
In response to the question on constructive feedback to improve the videos, 2 sub-themes emerged; video presentation and content (17.1%) and shortening the video (16.1%).
Promoting Pharmacy in the Future
Three prominent themes were generated from the suggestions of the participants on promoting the pharmacy services better in the future; advertise more/on more media (46.8%), advertise around the pharmacy and GP clinics (15.3%), and pharmacies need to have more private spaces (1.7%).
Table 4 presents an account of the selected quotes for each sub-theme.
Discussion
This study aimed to evaluate the effectiveness of promotional videos on the perception and intended uptake of patient-centred pharmacy services. Globally, there is scarce literature on the impact of such interventions as promotional videos on the public perception of pharmacy services. This study strives to fill this information gap by using NZ as a case study. With pharmacies being an essential primary care service, especially in recent COVID-19 times it is important to market and advertise the full range of clinically enhanced services that pharmacists and pharmacies provide.
Overall, the findings of this study align with trends found overseas with international literature on public awareness of pharmacy services suggesting that the low awareness found in this study is not exclusive to NZ.29–34 A systematic review of patient and public perspectives of community pharmacies in the United Kingdom (UK) found an association between lack of awareness and poor utilisation of pharmacy services. 35 The widespread lack of awareness of advanced pharmacy services and pharmacist roles suggests that more needs to be done to promote the pharmacy setting as a desirable location for health‐care delivery both locally and internationally. 35
The findings of the study suggest that promotional videos are an effective tool to promote the profession and increase public awareness of pharmacy services. Although the study did not aim to identify the barriers to accessing pharmacy services, the open-ended feedback and reason for no change in perception of pharmacy upon viewing the video provides an opportunity for respondents to report factors that prevent them from utilising such services. Some of the noteworthy barriers reported by the participants included ‘resistance to acknowledge the pharmacist as an essential member of the health‐care team’ and ‘lack of privacy.’
Similar to another study, we found poor awareness of patient centred services, and pharmacies being seen mostly as a place to buy OTC and prescription medicines, and beauty products. 35 This is in line with the earlier findings reporting pharmacists being perceived as ‘behind the counter’ health care staff. 36 A general perception that physicians are superior to pharmacists in knowledge and training could be a contributing factor36,37 and so could be the pharmacists’ lack of confidence and unwillingness to take on advanced clinical roles38–41 as articulated by one of the participants “…. I have previously been advised by pharmacists to see my doctor when I have asked basic questions related to my prescriptions and medications.” (Participant 158)
Lack of privacy, the second noteworthy barrier to utilisation reported in this study, has repeatedly been reported as an issue for pharmacy.39,42–46 However, the finding suggests a low awareness of consultations rooms in most NZ community pharmacies which needs to be addressed in future promotional strategies.
Success of any product or service in today’s world depends on how extensively it has been marketed and how widely it’s been recognized by the end user. Despite the myriad of services provided by pharmacists in NZ, there is a dearth of evidence on public perception of pharmacy and how effective current marketing strategies are in promoting these services. The findings of this study provide baseline information on how well pharmacy services are being marketed currently and public opinion on how to improve these marketing tools. The results of the study inform future studies and will be beneficial to pharmacy leadership and professional bodies in developing effective and well-received promotional strategies. A possible strategy to enhance the messaging and increase awareness among the population could be, having a bullet-point handout about the services offered for over the counter and prescription sales that goes with prescriptions. Since some respondents felt the videos were too long, future investigations should consider shorter length promotional videos. Similarly, the impact of demographic characteristics on awareness as well as understanding of promotional material makes an interesting area of research in the future.
As with any study there are limitations. Having access to an electronic device to complete the survey is likely to have caused underrepresentation of people with lower socioeconomic status; resulting in a potential for selection bias. Small sample size is another limitation and part of the reason was the large dropout rate due to technology issues and expired survey links. Therefore, the findings of the study should be generalised with caution. Nevertheless, the use of a survey company and random sampling ensured a large and demographically diverse sample. Lastly, the fact that the participants were asked what services they will use in the future immediately after watching the video does not necessarily mean that the awareness and perceived action will be translated into increased commitment and utilisation of pharmacy services.
Conclusions
The public’s understanding of the role of the pharmacist and the range of pharmacy services other than the provision of dispensed prescriptions remains low in NZ. Despite this, the PSNZ videos were found to be an effective tool for educating New Zealanders on the range of pharmacy services. This study suggests improvement in terms of choosing the right content and using the right platform to increase the viewership and engagement of the public around pharmacy. Overall, the intervention resulted in an increased awareness of pharmacy suggesting that the videos could be impactful if appropriate cut through was achieved. For future practice, more work is needed to ascertain from wider sample sizes of the NZ population the true perception of the pharmacy sector.
Footnotes
Author’s Note
All the authors had complete access to the study data that support the publication.
Author Contributions
M.A., C.M., and S.S. conceptualized and designed the study. All 4 authors were involved in designing the data collection instrument. P.R. collected data. P.R., M.A., and C.M. analysed and interpreted the data. P.R. and M.A. contributed to initial manuscript drafting. C.M. and S.S. critically reviewed and revised the manuscript for important intellectual content. All authors have reviewed, revised, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grant from The New Zealand Pharmacy Education and Research Foundation (NZPERF).