
Abstract
Introduction
Chronic Obstructive Pulmonary Disease (COPD) affects an estimated 15 million people 1 and is the fourth leading cause of death in the United States. It accounts for nearly $50 billion in healthcare expenditures annually, of which $13.2 billion are related to hospitalizations for acute exacerbations. 2 In 2012, the Centers for Medicare and Medicaid Services (CMS) implemented the Hospital Readmissions Reduction Program, which decreases the amount reimbursed for hospitals with excess rates of 30-day readmissions for certain disease states, and COPD exacerbation is among those conditions. 3 Since that time, CMS has also initiated the Bundled Payments for Care Improvements (BCPI) program, which combines payments for the physician, hospital, and other health care provider services into a single bundled payment amount per episode, which often is intended to care for a patient for 90 days after that episode. This provides incentive for health care providers to improve quality of care through efficient use of health care resources and coordination of care. 4 If an institution chooses to participate in this program for COPD, it will be held to standards for Hospital-Wide All-Cause Unplanned Readmissions within 30 days and any additional readmissions will further reduce the amount of the bundled payment kept by the institution as revenue. These initiatives intend to decrease costs and improve quality of healthcare, creating a financial incentive to implement new programs to improve outcomes for those disease states, but do not provide specific guidance as to what initiatives to consider. Current data estimates that as much as 30% of patients hospitalized for COPD exacerbation are readmitted within 30 days. 5 These early readmissions contribute both to the economic cost of the disease as well its impact on patients. 2 Of these readmissions, 10-55% may be preventable. One area that has the potential to reduce readmission rates is transitions of care (TOC). The Joint Commission refers to TOC as a patient’s movement through different healthcare settings as their condition and care needs change. 6 Post discharge periods can often be high-risk times for patients and can be complicated by changes to medication regimens and poor communication to the patient and their provider(s). TOC interventions can reduce errors and confusion during this period and can involve a variety of services including medication reconciliation, resolving medication barriers, and counseling.
Pharmacy services such as medication management during TOC have demonstrated positive impacts on clinical outcomes previously, 7 however there remains uncertainty about what specific interventions may benefit COPD as there is heterogeneity in the current literature. Furthermore, many of the studies were done in urban areas or within the Veteran’s Affairs system. There is a lack of data looking at the utility of TOC services in community hospitals serving rural regions specifically. This is critical because rural residence has been independently associated with higher incidence of COPD exacerbations. 8 Managing inhaler therapy after an exacerbation is often done in the outpatient setting, but this is challenging in rural regions. These communities usually have fewer primary care providers and even fewer pulmonary specialists. 9 Additionally, rural residents often face significant transportation barriers to accessing healthcare, which complicates follow-up care. 10 These challenges highlight the need for an all-hands on deck approach to COPD as well as the potential benefit of managing more aspects of this disease in the inpatient setting. This study aimed to address some of these challenges by packaging several different services for optimizing COPD medication management in a comprehensive TOC program.
Objective
In this study, we evaluate the effect of a pharmacy-driven COPD TOC service on 30 day re-presentation rate in patients admitted with COPD exacerbation in a large tertiary hospital serving a rural and geographically wide region. Re-presentation is defined as any encounter with the health system – emergency department visit, observation status hospital stay, or full admission as opposed to readmission which would include only a formal admission to the health system. The authors chose to target re-presentation rate rather than readmission rate to get a true picture of whether we were preventing un-planned utilization of health care as a whole, not just the type of presentation that would impact reimbursement. Secondary outcomes include re-presentation rate at 90 days, volume of interventions made by the pharmacy team, and description of the service.
Methods
Setting
This study was carried out at Mission Hospital, which is an 815-bed tertiary care community hospital in Asheville, NC that is the flagship of a 6-hospital health system serving an 18-county region in Western North Carolina. The main campus has more than 100,000 emergency department (ED) visits and 40,000 inpatient discharges per year.
Decentralized pharmacists are responsible for verifying orders, participating in multidisciplinary rounds, providing clinical services, participating in emergency code responses, and precepting pharmacy residents and students from the University of North Carolina Eshelman School of Pharmacy, for which the hospital is contracted with the school to provide 150 student-months annually.
Pharmacy technicians obtain admission medication histories for patients admitted into the hospital through the ED. Nurses, physicians, and pharmacy students obtain admission medication histories for patients not admitted through the ED.
Design
This single-center, retrospective, chart review study was conducted from January 1, 2019 through December 31, 2019. Patients were identified using an electronic health record (EHR) and were included in the study if admitted to the pulmonary unit of the hospital with an International Classification of Disease-10 (ICD-10) code of J44.0 or J44.1 documented anywhere in the chart. There were no exclusion criteria. The intervention group was comprised of 756 patients that received any part of the pharmacy-driven COPD TOC intervention. The control group was comprised of 1666 patients that did not receive any part of the pharmacy-driven COPD TOC intervention. This study was approved by the Institutional Review Board (IRB), HCA Healthcare, and Mission Health-System’s Research Institute.
Chart review was utilized to determine what aspect of TOC services the patient received, including whether they had a medication history conducted by pharmacy personnel (pharmacist, pharmacy tech, or pharmacy student), utilization of medication bedside delivery service, and whether they received medication education. Documented pharmacy TOC consults were utilized to assess medication barriers upon admission and suggested changes made by pharmacists.
Intervention
Patients admitted to the hospital’s pulmonary unit with a qualifying ICD10 code had an automatic pharmacy consult populate the unit pharmacist’s task list. The TOC services were carried out by a team comprised of early immersion (student inn years 1-3 of their PharmD program) and advanced immersion (students in their 4th and final year) student pharmacists and an attending pharmacist. The pharmacy-driven COPD TOC intervention is described in Figure 1, including which pharmacy team member completed each step and percent of patients that received each step. Generally, one early immersion student and one advanced immersion student were dedicated to the COPD TOC workflow per day. The attending pharmacist was responsible for the unit’s inpatient and general TOC needs and oversight of the remaining students on the TOC service in addition to the COPD TOC workflow. Medication access and adherence was assessed using the Medication Access and Adherence Tool (MAAT) developed at the University of Pittsburgh Medical Center.
11
Decisions regarding alternative inhaler choices were made based on shared decision making with the patient and included cost of alternative choices. Common reasons a patient did not receive any part of the pharmacy COPD TOC service were inadequate staff to provide the service on weekends and holidays, and patient being cared for on a unit other than the pulmonary unit. Intervention. Pt = patient; PTOC = Pharmacy TOC Team; EI = Early Immersion student, 2nd or 3rd year in pharmacy school; MAAT = medication access and adherence tool; AI = Advanced Immersion student, 4th year in pharmacy school; AMR = admission medication reconciliation; RPh = Attending pharmacist, TOC and pulmonary specialist; M2B = Meds To Beds, discharge medication bedside delivery service; Orange shading = opportunities for improvement in process.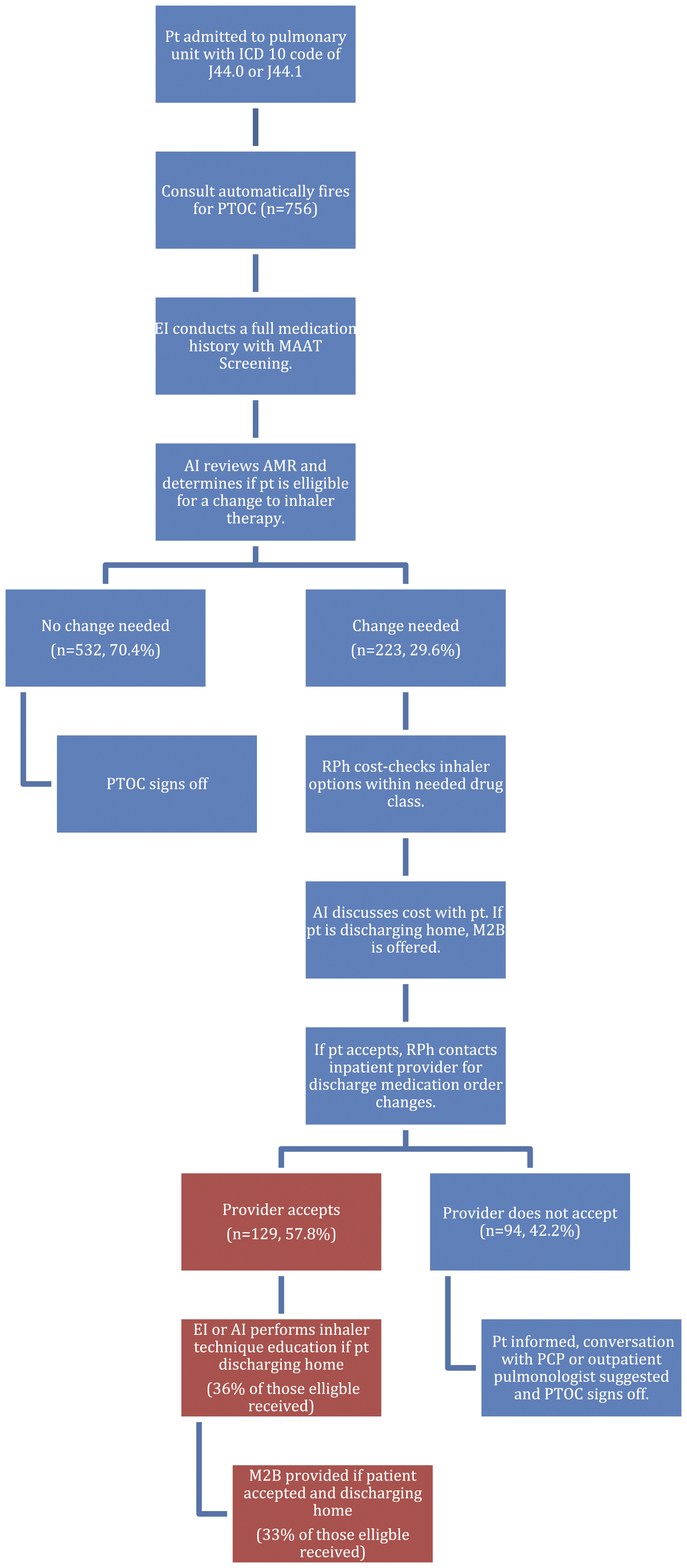
Study Outcomes
The primary outcome of the study was re-presentation rate at 30 days, defined above as any encounter with the health system. Secondary end points were re-presentation rate at 90 days, pharmacy intervention rates, and description of the service. Subgroup analyses were performed to determine re-presentation rates between 0-30 days, 31-60 days, or 61-90 days after discharge, re-presentation rates for those same time points for rural zip codes, 12 and for various discharge dispositions. Types of interventions were described and categorized.
Statistical Analysis
Re-presentation rates were expressed in percent. Mean difference along with confidence intervals and P values were calculated for primary and secondary outcomes. Chi square tests were performed for qualitative data and t-tests were performed for quantitative data. P values less than .05 were considered significant.
Results
Baseline Characteristics.
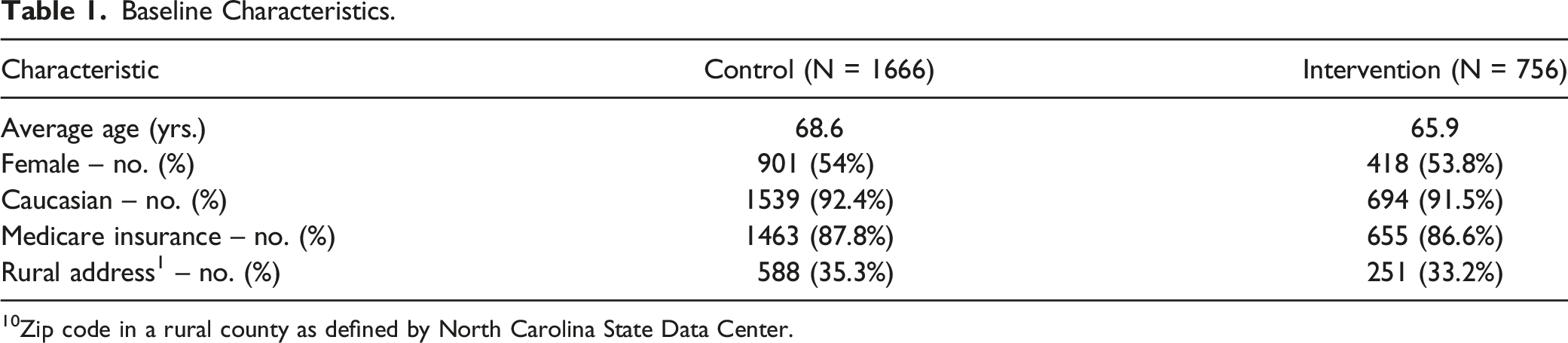
10Zip code in a rural county as defined by North Carolina State Data Center.
Thirty day re-presentation rate was 28.5% in the intervention group compared to 25.5% in the control group (P = .12). The subgroup analysis for rural zip codes revealed a 30-day re-presentation rate of 22.8% in the intervention group and 24.1% in the control group but this trend was not sustained at 90 days with re-presentation rates of 41.2% in the intervention group and 40% in the control group. No time points or subgroup analyses were associated with statistically significant differences.
Inhaler changes were suggested to the provider for 223 patients (29.6%), with 168 recommendations (75%) for escalation in therapy and 55 recommendations (24.7%) for resolving barriers to access and/or adherence. Volume of pharmacist recommendations accepted by the provider, volume of patients that received inhaler technique education, and volume of patients that received bedside discharge medication delivery can be found in Figure 1.
Screening for barriers found 55 patients with reported barriers with the most common being difficulty understanding how to use their inhaler. Twenty-eight (50.9%) had difficulty understanding their medications, 18 (32.7%) experienced cost issues, 7 (12.7%) were not honest about compliance, 5 (9.1%) expressed physical limitations to use of their inhaler, and 7 (12.7%) communicated other barriers that included needing nebulizer equipment, unwillingness to adhere to maintenance inhaler, or unable to remember inhaler regimen.
Discussion
While COPD exacerbations are known to be associated with high morbidity, mortality, and cost, they continue to prove difficult to prevent. Health care providers are incentivized to develop innovative services to increase the quality of care for these patients by CMS’s HRRP and BCPI initiatives, but so far literature on these innovative services show conflicting results. One systematic review found that post-discharge support and interventions provided by pharmacy did reduce 30-day readmission rates, but the authors noted that they could not identify a specific set of interventions as the 10 studies in the review included different interventions. 5 Another study conducted in the Veteran’s Affairs system found that including a clinical pharmacy specialist to perform medication reconciliation, medication management, and counseling services post discharge in patients with heart failure (HF) or COPD reduced both COPD and HF and all-cause readmission rates. 13 This study included two post-discharge visits with a clinical pharmacist, however, which may be difficult to achieve in a rural setting where patients must travel significant distances to reach the pharmacy specialist. In another review, Prieto-Centurion et al. 14 remarked that it is challenging to compare strategies due to lack of standard approaches to defining patient populations, interventions, and outcomes. Until more standardized approaches emerge, it may be necessary to consider potential TOC interventions individually and consider the patient populations and settings that have benefited from them when looking to design or evaluate new programs.
Our study was unique in that it utilized a comprehensive set of admission-to-discharge TOC services, including medication reconciliation reviews, barrier screening, pharmacotherapy management, medication education, and bedside medication delivery all while the patient was still in the hospital for an exacerbation, which may be preferred when caring for a rural population. The patients in the intervention group in this study did not experience a reduction in the primary outcome of re-presentation rate at 30 days. Of note, the was a large portion of patients identified that qualified for a change to their inhaler regimen, either to resolve an access barrier or to bring their therapy more in line with current guidelines, indicating a need for medication management in this patient population. These types of comprehensive interventions are time consuming for pharmacists, suggesting a need to consider using pharmacy extenders. To our knowledge this was the first TOC study focused on COPD that utilized both early and advanced immersion pharmacy students in a layered-learning model demonstrating that pharmacy students are able to play integral roles in delivering comprehensive TOC services as well as effectively identifying medication related problems and communicating them to providers.
No data were collected on what recommendations were made concerning outpatient follow-up. Several of the previously mentioned studies that did decrease readmissions involved post-discharge follow-up so it may be that this is a key component of effective COPD management. Access to specialists as well as transportation barriers can make such follow-up challenging in rural communities, which is in part what some of the interventions in this study hoped to address such as making inhaler changes while patients were still in the hospital. It may be necessary, however, to package these interventions with post-discharge follow-up to see a significant impact. The study hospital considered pursuing a Clinical Pharmacist Practitioner agreement with inpatient physicians in order to make needed inhaler adjustments per a collaborative practice agreement, which would have brought this study more in line with others such as the VA study that found a benefit. 13
Ideally, a COPD-specific TOC program would benefit patients as well as generate cost savings that cover the expense of running the program through reducing readmissions. Our study did not show this reduction so we cannot estimate any cost savings, however there is significant potential for this as hospitals with excessive readmissions of patients with COPD face the loss of up to 3% of total Medicare reimnursement per year as of 2015.15,16 A previous TOC study at this same hospital estimated the average direct cost per readmission in 2013-2014 was $4306. 17 Further work is needed to identify what specific interventions are effective at reducing readmissions, however the financial potential is there and this study did find significant opportunities to optimize medication therapy for these patients.
Limitations to consider for this study are the retrospective design, the majority Caucasian study population, and lack of investigation of comorbidities, smoking status or eosinophil levels. In addition, there were concomitant efforts at the study hospital focused on an increase in appropriate influenza and pneumococcal vaccination rates and smoking cessation, but there was not data collected on these potential confounders. Most importantly, there were opportunities for improvement on provider acceptance rates of the pharmacist’s suggested changes, provision of inhaler technique education, and utilization of bedside discharge medication delivery. The study hospital also moved the transitions of care specialist and associated students to the pulmonary unit after this first year in an effort to improve the capture rate for inhaler technique education. The transitions of care specialist continued to work closely with the bedside discharge medication delivery team to improve rate of utilization of this service. The study authors feel strongly that improvement in these three aspects could greatly improve outcomes associated with this service and deserves further study.
Conclusion
COPD is a disease with a high burden on patients and healthcare systems due to high re-presentation rates following exacerbations. To further complicate the treatment of this disease state, transitioning between care settings increases the risk for adverse events due to potential miscommunication. 18 While guidelines do not necessarily recommend changing therapy during an exacerbation, many patients live in an isolated rural setting and are far from care. While this comprehensive admission-to-discharge service did not demonstrate a reduction in re-presentations, a bigger focus on provider acceptance rates, ensuring the patients have the drug in hand before discharge through bedside delivery, and provision of education on appropriate inhaler technique may have potential for improved results, particularly in a rural setting. Utilization of student pharmacists should also be heavily considered in an effort to reach more patients with these important yet time-consuming interventions.
Footnotes
Acknowledgments
Authors Notes: Austin Bently, PharmD and Hope Ball, PharmD were student pharmacists at UNC Chapel Hill ESOP during the data collection and analysis of this project.
Disclosures
The authors have no financial conflicts or other competing interests to disclose. This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.