
Abstract
Introduction
The prevalence of chronic pain increases with age. According to the US National Health Interview Survey (NHIS), in 2019, 25.8% of individuals age 45-64 and 30.8% of those age 65+ reported chronic pain in the past 3 months, and 10.3% of those age 45-64 and 11.8% of those age 65+ reported high-impact chronic pain (ie, pain that frequently limited life activities). 1 NHIS data also showed that in 2019, the proportions of those with chronic pain who used an opioid in the past 3 months were 25.9% of the 45-64 age group and 21.8% of the 65+ age group. 2 Of concern is opioid misuse and poisoning among late-middle aged and older-adult opioid users. The US National Poison Data System (NPDS), 2006-2014, showed that rates of prescription opioid misuse and serious medical outcomes among those age 60+ increased each year, especially among those with suicidal intent.3,4 In the 2011-2018 NPDS, those age 50+ comprised 23.4% of all opioid exposure cases but 29.6% of the opioid exposure cases with serious outcomes. 5 The study found that in all opioid exposure cases, exposures to 3+ medicines/substances increased the risk of a serious outcome by 250%. 5
Polypharmacy, most commonly defined as the co-use of multiple (eg, ≥5) medications, is widespread in older adults with multi-morbidity and complex drug regimens.6,7 Polypharmacy has been associated with inappropriate prescribing/use and adverse outcomes including frailty, falls, emergency department (ED) visits, hospitalization, and death.8-12 The risk of adverse effects and harms from polypharmacy in late life is due to multiple factors including drug-drug interactions, drug-disease interactions, decreased renal and hepatic function, lower lean body mass, reduced hearing and vision, and impaired cognition and mobility. 13 Among frail older adults, decreased hepatic phase II metabolism may also result in increased risk of gastrointestinal toxicity and renal insufficiency from concurrent use of multiple pain medications including prescription opioids, acetaminophen, and nonsteroidal anti-inflammatory drugs (NSAIDs). 14
Adverse effects of polypharmacy including opioids have been well-documented. A study of US adults age 65+ with 1-year continuous medical and drug plan enrollment and ≥15 days’ supply of ≥2 opioid prescriptions found that concurrent use of 2+ medications increased injurious falls/fractures by 18% and ≥3 ED visits by 21%. 15 The study also found that benzodiazepines and gabapentinoids were most often used concurrently with opioids. 15 The English Longitudinal Study of Aging (of a representative sample of those age 50+) also found that those with polypharmacy including opioids, benzodiazepines, antidepressants, antipsychotics, and muscle relaxants were at higher risk of all-cause and cardiovascular mortality compared with those who did not take these types of medications. 16 A study of privately insured adults age 18-64 found that concurrent opioid and a benzodiazepine use doubled the risk of an ED visit or inpatient admission for opioid overdose. 17 Other studies showed that prescription opioid overdose and related deaths among adults were significantly associated with co-use of benzodiazepines, other z drugs, gabapentinoids, nonopioid analgesics, muscle relaxants, and cocaine, methamphetamine and other psychostimulants.18-22
Harms of opioid misuse and poisoning are also likely to be higher among those who co-use/misuse alcohol and illicit substances. The 2015-2016 National Survey on Drug Use and Health showed that 6.6% of past-year prescription opioid users age 50+ reported misuse; however, the misuse rates were significantly higher among those who had alcohol use disorder, used other substances (ie, tobacco, marijuana, cocaine), and/or misused prescription sedatives, stimulants, and tranquilizers. 23 Alcohol use disorder among those with prescription opioid misuse is associated with progression to opioid use disorder and increased risk of opioid overdose.24,25 Illicit drug use among those age 40-55 with prescription opioid misuse was also found to be associated with higher odds of nonfatal opioid overdose. 26
Despite the high rates of prescription and over-the-counter medication and other substance use among older adults27-30 and potential adverse effects of co-using these medicines/substances, previous NPDS-based studies of older-adult opioid poisoning cases did not examine the types of other medicines/substances that may be associated with increased risk of healthcare use. In the present study of prescription opioid exposure cases age 50+ in the 2015-2020 NPDS, we examined associations between other types of medicines/substances involved and the level of healthcare service use. Based on previous studies of medicines/substances that were commonly co-used by older-adult opioid users, the study hypotheses were that higher levels of healthcare service use would be associated with (H1) medications for cardiovascular diseases (CVD), benzodiazepines, other sedatives/hypnotics, antipsychotics, muscle relaxants, other pain relievers, gabapentin, alcohol, and illicit drugs; and (H2) higher numbers of these medicines/substances. The control variables included demographic factors, exposure reasons, and medical outcomes (severity of exposure). The findings may further elucidate serious adverse outcomes and risks for higher levels of health care among older adults who used/misused prescription opioids along with other medications and licit and illicit substances.
Methods
Data Source
We used NPDS from January 2015 through December 2020, which included cases from 55 U.S. poison control centers. NPDS is the data warehouse for the American Association of Poison Control Centers (AAPCC) and the only near-real time poisoning surveillance data base in the US that tracks and monitors adverse events. See NPDS’s website (https://aapcc.org/data-system) or Gummin et al. 31 for detailed NPDS descriptions. AAPCC granted the authors access to NPDS after reviewing our study proposal pertaining to prescription and illicit opioid exposure cases age 50+. In this paper, we focused on cases involving prescription opioids (with or without illicit opioids). Cases that only involved illicit opioids (heroin, non-prescription fentanyl, and other illicit opioids; N = 5207) were excluded from the present study. We followed the NPDS variable labels and attributes. Although NPDS lists cases, not individuals, the extent to which these cases include duplicate individuals is minimal as poison center specialists are trained to identify duplication and correct it as soon as it is discovered. Based on the authors’ institutional IRB guidelines, IRB exemption was assumed for analysis of these de-identified, existing data.
Measures
Prescription Opioids
The NPDS includes 23 types of prescription opioids (eg, tramadol, oxycodone and hydrocodone alone or combination products [other than with acetaminophen or acetylsalicylic acid], morphine, methadone, buprenorphine, prescription fentanyl) as well as acetaminophen and acetylsalicylic acid combined with opioids.
Other Medicines
In this study, we included the following: (1) CVD drugs (angiotensin converting enzyme inhibitors, angiotensin receptor blockers, antihyperlipidemics, antihypertensives, beta blockers, calcium antagonists, and other miscellaneous CVD drugs); (2) antidepressants; (3) benzodiazepines; (4) other types of sedatives/hypnotics; (5) antipsychotics; (6) muscle relaxants; (7) acetaminophen alone or combined with nonopioids; (8) NSAIDs, including acetylsalicylic acid alone or with nonopioid combinations); and (9) gabapentin. We included CVD drugs given the significant increase in their use over the past decade 27 and previous study findings showing increased cardiovascular mortality in older prescription opioid users.16,32 We included gabapentin as it is one of the most commonly added adjunctive analgesic medications for older adults.33,34 The NPDS annual report also shows that after analgesics, CVD drugs, muscle relaxants, and psychotropic medications were the most frequently involved pharmaceuticals in adult exposures. 31 We did not include other medications as they were involved in a small proportion (<3%) of cases (eg, hypoglycemic medications involved in 1.1% of cases).
Other Substances
These were (1) alcoholic beverages, (2) cannabis, (3) illicit opioids (heroin, non-prescription fentanyl, and other synthetic, nonpharmaceutical opioids), and (4) psychostimulants (cocaine, methamphetamines or amphetamines). We did not include other illicit substances (eg, hallucinogens [psilocybin, psilocin, hallucinogenic amphetamines]) as only small numbers of prescription opioid exposure cases age 50+ involved them.
Management Site and Level of Healthcare Facility Care
The NPDS lists the following management/care sites: managed outside a healthcare facility (HCF) (mostly at the initial call site); treated/evaluated and released; admission to a psychiatric facility (mostly for evaluation); admission to noncritical care; admission to critical care; and refusal of PCC referral to a HCF, no show, or leaving HCF against medical advice (AMA). We first grouped these into 3 categories: (1) managed outside a HCF; (2) managed at a HCF; and (3) no follow-up (ie refused referral/no show/left AMA) for descriptive analysis. Then, among those managed at a HCF, level of HCF care (dependent variable in the multivariable analysis) was categorized as (1) treated/evaluated and released or admission to psychiatric care (treated/evaluated and released hereafter); (2) admission to noncritical care; and (3) admission to critical care unit.
Control Variables
These were year of exposure (2015-2020), age group, gender, census region of residence, exposure reason, exposure site (own or others residence and all other locations), and medical outcomes (ie, severity of exposure). We collapsed exposure reasons into 4 categories: unintentional poisoning (adverse reaction or unintentional therapeutic error, misuse, general, occupational, environmental, or unintentional but unknown reason); intentional misuse/abuse without suicidal intent (intentional misuse/abuse hereafter); suspected suicide; and unknown or other reasons (including withdrawal and malice). See Gummin et al. 31 for detailed description/scenarios of each exposure reason. We also collapsed medical outcomes into 4 categories: no or minor effects (ie, exposure not resulting in any symptoms or minimally bothersome effects that resolved rapidly); moderate (ie, exposure resulting in effects more pronounced, more prolonged, or more systemic in nature than minor symptoms); major effects or judged as a potentially toxic exposure in cases not followed; and death. Moderate or major outcomes or death are considered serious outcomes in PCC annual reports. 31
Analysis
All analyses were conducted with Stata 17/MP (Stata Corp, College Station, TX). First, we described the types of prescription opioids involved. Second, we used χ2 tests for descriptive examination of demographic factors, exposure reasons, medical outcomes, and other substance use by management site and level of HCF care. Third, to analyze associations of level of HCF care and other substance use, we fit 2 multinomial logistic regression models with HCF level as the dependent variable. In Model 1, 13 different types of medicines/substances were entered as the independent variables. In Model 2, the number of these other co-used medicines/substances was the independent variable. Results are reported as relative risk ratios (RRRs) with 95% confidence intervals (CIs). Statistical significance was set at P < .05.
Results
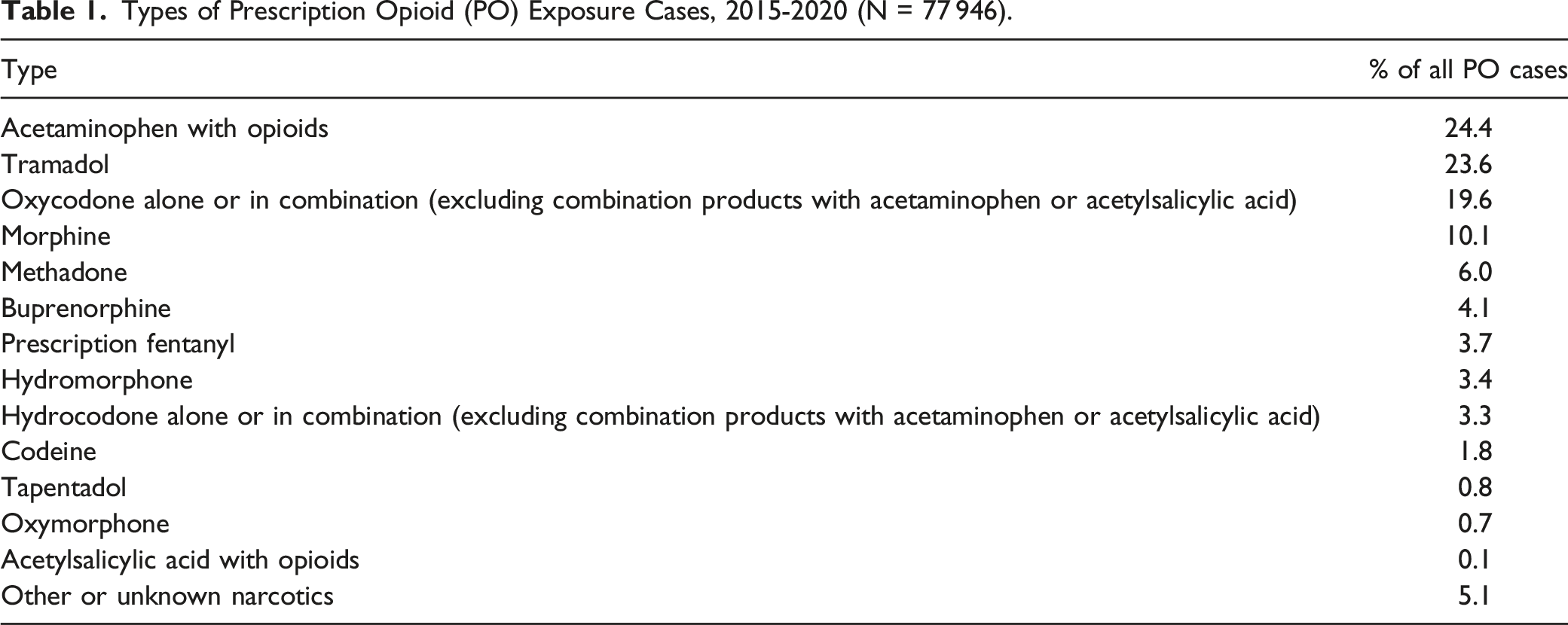
Types of Prescription Opioids Involved
Types of Prescription Opioid (PO) Exposure Cases, 2015-2020 (N = 77 946).
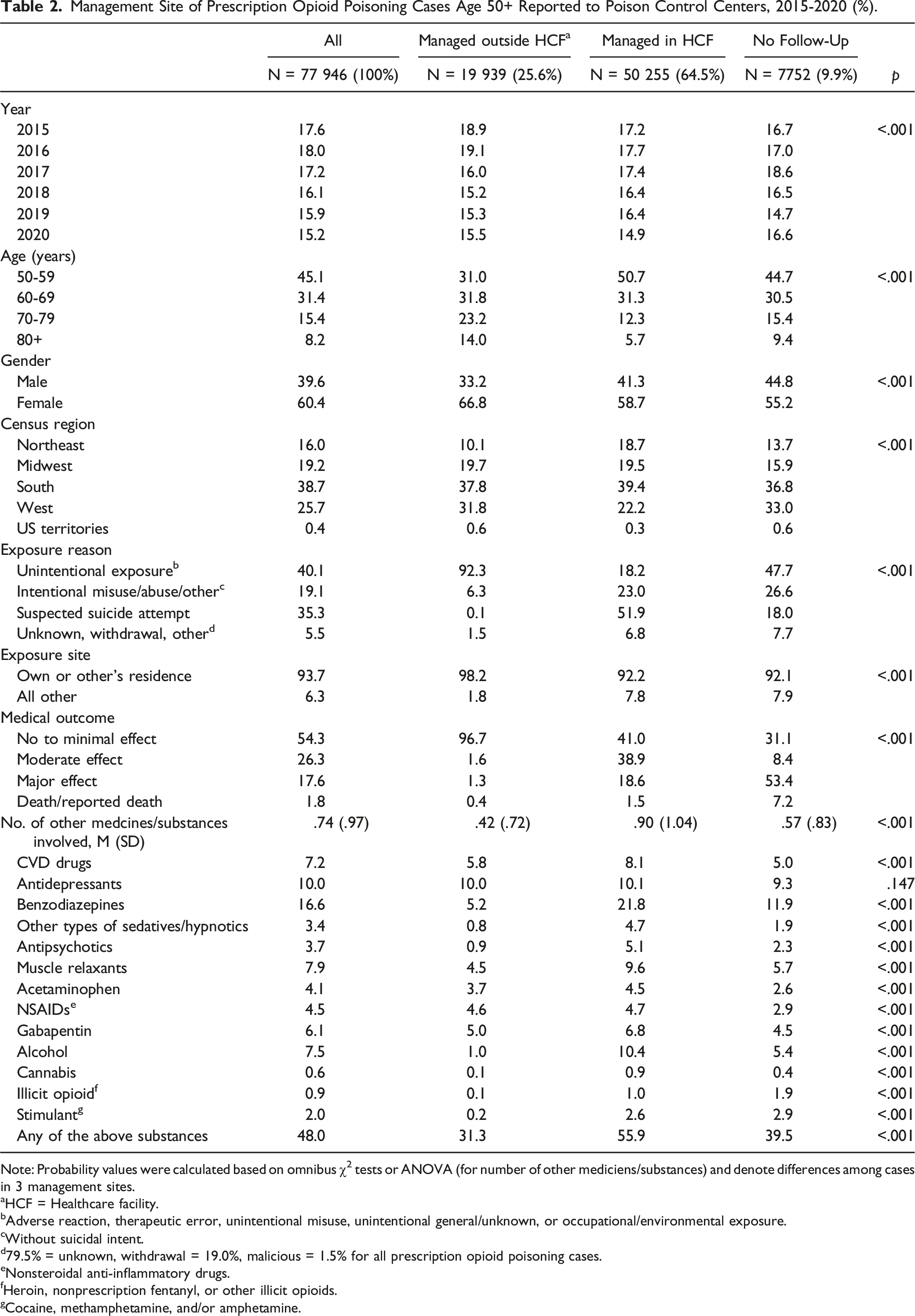
Case Characteristics by Management Site
Management Site of Prescription Opioid Poisoning Cases Age 50+ Reported to Poison Control Centers, 2015-2020 (%).
Note: Probability values were calculated based on omnibus χ2 tests or ANOVA (for number of other mediciens/substances) and denote differences among cases in 3 management sites.
aHCF = Healthcare facility.
bAdverse reaction, therapeutic error, unintentional misuse, unintentional general/unknown, or occupational/environmental exposure.
cWithout suicidal intent.
d79.5% = unknown, withdrawal = 19.0%, malicious = 1.5% for all prescription opioid poisoning cases.
eNonsteroidal anti-inflammatory drugs.
fHeroin, nonprescription fentanyl, or other illicit opioids.
gCocaine, methamphetamine, and/or amphetamine.
As for exposure reasons, 40.1% of all cases were unintentional, 19.1% intentional misuse/abuse, and 35.3% suicidal intent; however, these distributions varied significantly by management site. Of those managed outside a HCF, an absolute majority were unintentional exposure cases, and of those managed at a HCF, the largest proportion (51.9%) was suicidal intent cases. Of medical outcomes, 69% of cases managed at a HCF and almost 70% of those not followed-up had serious outcomes.
Of all cases, 48.0% involved one or more (range 1-8) of the 13 other medicines/substances, and the cases managed at a HCF and not followed-up had greater numbers than the cases managed outside a HCF. Benzodiazepines (16.6%), antidepressants (10.0%), muscle relaxants (7.9%), and alcohol (7.5%) were most common. Additional analysis showed that 91.9% of all cases used only one type of prescription opioid and the remainder used 2-5 types.
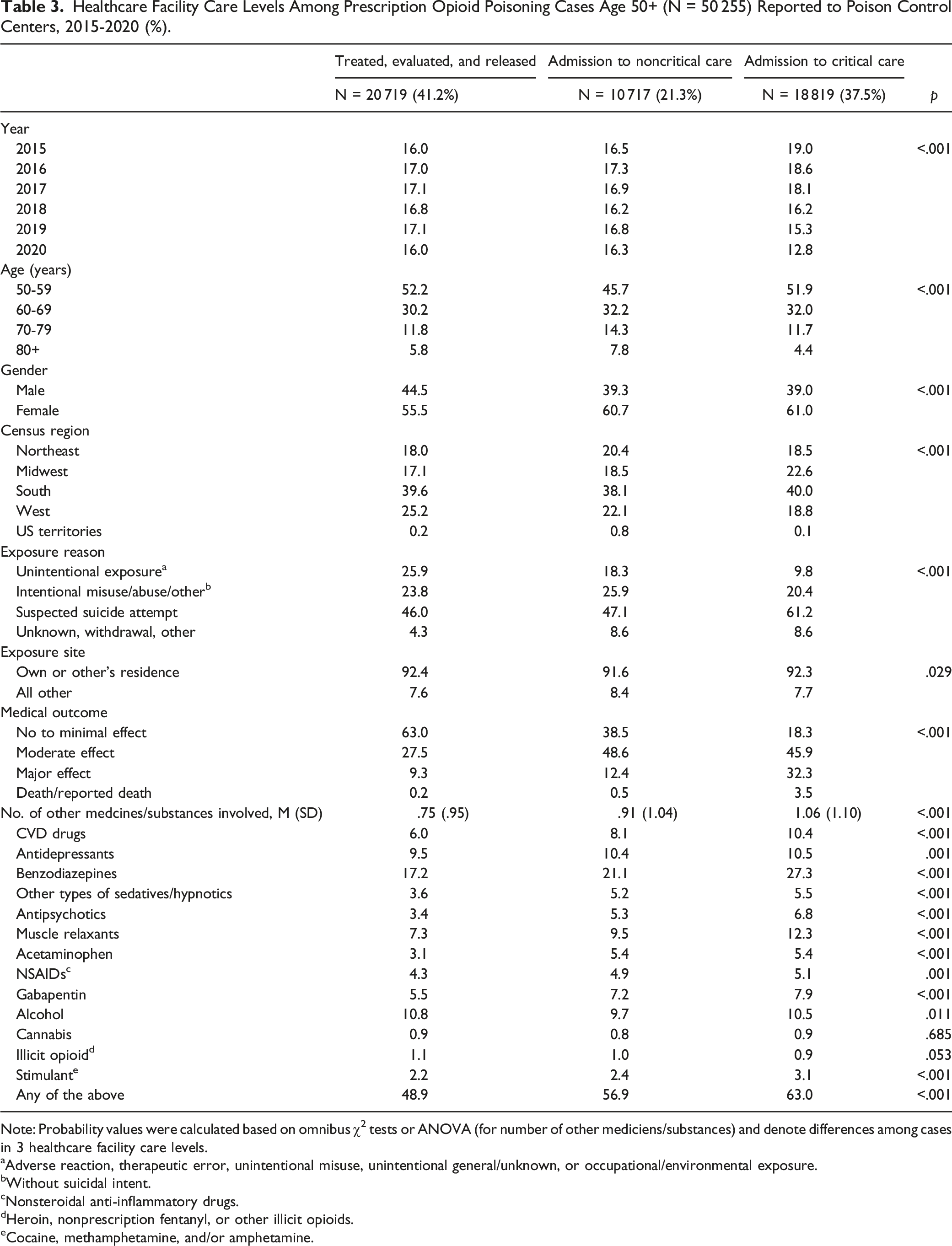
Case Characteristics by Level of HCF Care
Healthcare Facility Care Levels Among Prescription Opioid Poisoning Cases Age 50+ (N = 50 255) Reported to Poison Control Centers, 2015-2020 (%).
Note: Probability values were calculated based on omnibus χ2 tests or ANOVA (for number of other mediciens/substances) and denote differences among cases in 3 healthcare facility care levels.
aAdverse reaction, therapeutic error, unintentional misuse, unintentional general/unknown, or occupational/environmental exposure.
bWithout suicidal intent.
cNonsteroidal anti-inflammatory drugs.
dHeroin, nonprescription fentanyl, or other illicit opioids.
eCocaine, methamphetamine, and/or amphetamine.
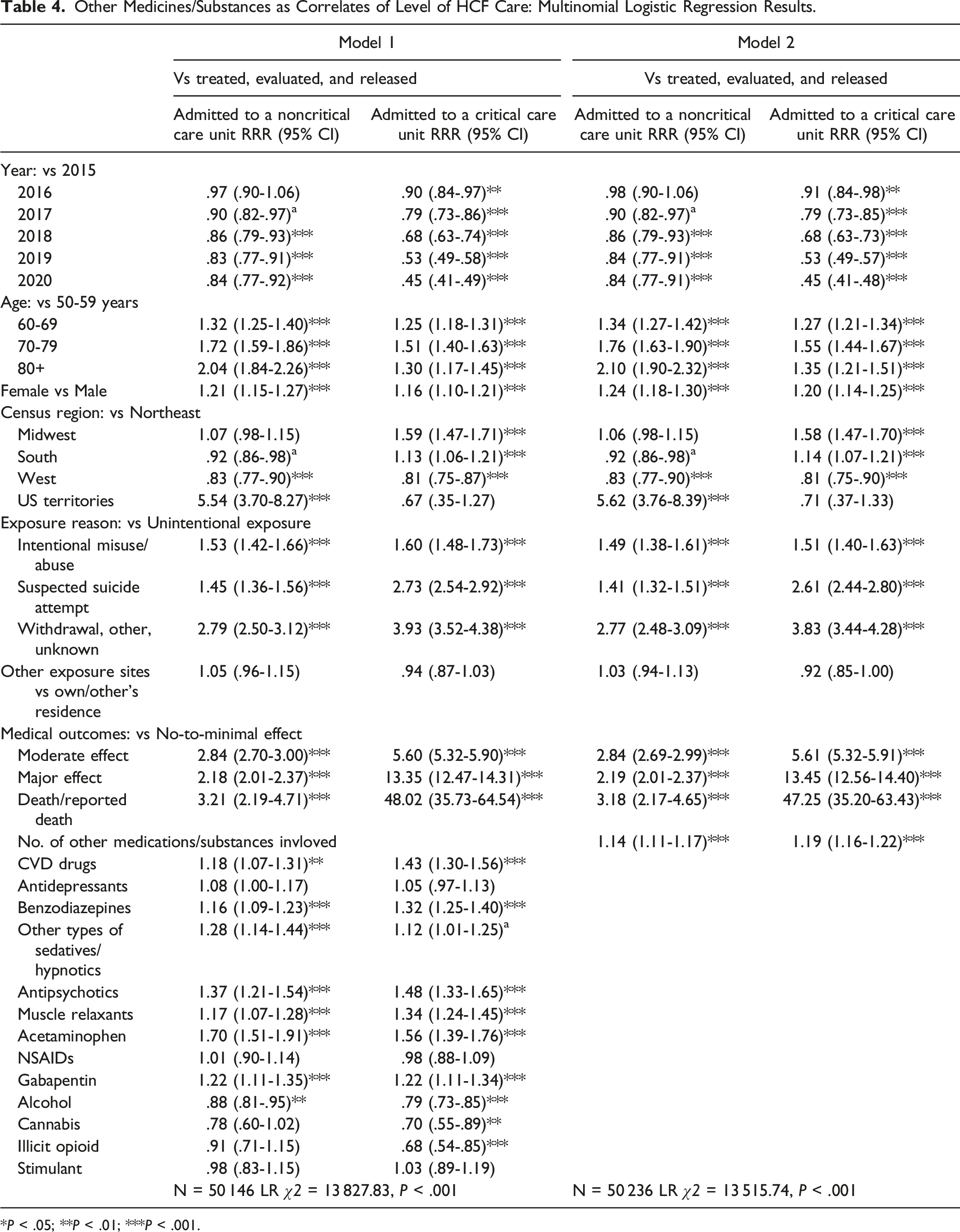
Associations of Level of HCF Care With Other Medications/Substances
Other Medicines/Substances as Correlates of Level of HCF Care: Multinomial Logistic Regression Results.
*P < .05; **P < .01; ***P < .001.
Of the control variables, compared to 2015, exposure years 2016 to 2020 were associated with a lower risk of admission to noncritical and critical care units. Age groups older than 50-59 and women than men had a higher risk of admission to noncritical and critical care units. Compared to Northeastern residents, residents of the South and West had a lower risk of admission to noncritical care units while residents of US territories had a higher risk; and residents of the Midwest and South had a higher risk of admission to critical care units while residents of the West had a lower risk. Compared to unintentional exposure, all other exposure reasons were associated with a higher risk of admission to noncritical and critical care units. Suicidal intent and other exposure reasons and major medical outcomes and deaths had the highest associations with critical care admissions.
Discussion
This study shows that of prescription opioid poisoning cases age 50+ that were reported to PCCs between 2015 and 2020, about two-thirds were managed at a HCF, about a quarter were managed outside a HCF, and one-tenth were not followed-up. Compared to 2019, the proportion of cases managed at a HCF was slightly lower and the proportion with no follow-up was slightly higher in 2020; however, it is not clear if reluctance to access a HCF during the COVID-19 pandemic played a role in these changes. Among cases managed at a HCF, 41.2% were treated/evaluated and released, 21.1% were admitted to noncritical care units, and 37.5% were admitted to critical care units. The study also shows a high rate of multi-drug use among these opioid poisoning cases, with benzodiazepines, antidepressants, muscle relaxants, CVD drugs, and gabapentin being the most common other prescription medications involved. A small proportion also co-used alcohol and illicit substances with prescription opioids.
Co-use of other medicines/substances was significantly more common among cases managed at a HCF, with the highest rate among cases admitted to critical care, which included high proportions of suspected suicides and intentional misuse/abuse cases. Cases involving unintentional opioid poisoning may have been prescribed these other medications due to multi-morbidity. However, a majority of critical care admittants appear to have misused other medications along with prescription opioids for intentional self-harm. A study found that among those with opioid overdose history, active/passive suicidal intent was associated with use of ≥5 substances, including illicit drugs, especially cocaine/crack. 35 Research posits links among chronic pain, opioid overdose/opioid use disorder, worsening depressive symptoms and other life stressors, and vulnerability to suicide. 36 However, discerning unintentional from intentional misuse/abuse and suicide attempts may be difficult as the intentionality of overdose tends to be dimensional rather than categorical with shared risk factors.36,37
Multivariable analyses showed that all co-used medications except antidepressants and NSAIDs were associated with significantly increased risks of noncritical and critical care admissions, and each additional medication increased such risks substantially. These findings largely support our hypotheses. The significant association between CVD drugs and increased risks of noncritical and critical care admissions is not surprising as individuals with underlying CVD may be at increased risk for adverse health consequences from opioid poisoning. The increased risk associated with acetaminophen is also not surprising as research shows its association with adverse gastrointestinal, cardiovascular, hepatic, and renal events, and there is evidence that frail older adults may have impaired acetaminophen clearance. 38 Our findings for benzodiazepines, muscle relaxants, and gabapentin are similar to previous study findings of increased likelihood of opioid overdose, ED visits, and hospitalizations among people who concurrently used these medications with opioids.16,20 Despite increased risks for overdose and healthcare use, research has shown rapid increases in co-prescribing of opioids with benzodiazepines, other sedatives, and gabapentin over the past decade.17,39-41
The increased risk of healthcare service use associated with increased number of medicines/substances is not surprising, either. Older-adult PCC cases with prescription opioid exposure and complex medication regimens likely had multiple medical conditions and associated chronic pain contributing to their elevated need for healthcare services. Previous studies found strong bidirectional relationships between polypharmacy and frailty, functional and cognitive impairments, falls, ED visits, hospitalizations, and death.11,12,42,43 The association between polypharmacy and hospitalization was shown for any hospitalization, unplanned hospitalization, and re-hospitalization.12,44 These studies also found more serious outcomes for excessive polypharmacy (eg, 6-9 drugs).
Surprisingly, antidepressants and NSAIDs were not more likely to be associated with noncritical or critical care admissions compared to treatment/evaluation and release. Prior studies found links between NSAID use and elevated blood pressure and increased risk of heart failure and thrombotic events 45 and higher risk of NSAID-induced gastrointestinal toxicity and adverse renal events among older adults.17,46 Also unexpected was that alcohol and other illicit substances were associated with lower risk of noncritical and critical care admissions. It is not clear how or why co-use of these substances was associated with lower risk of HCF admissions. A recent study, based on 11 years of NHIS data, of alcohol use and healthcare use among older adults found that compared to lifetime abstainers, former alcohol users had more but current moderate users had fewer ED visits, controlling for sex, race, educational attainment, marital status, and concurrent tobacco use. 47 The study also found that those with any lifetime alcohol use, but those with current heavy use, had more recent healthcare visits than lifetime abstainers. Current alcohol users may have better health than former users as older adults tend to quit drinking in response to ill health. 48 Data on physical and mental health conditions (that NPDS does not provide) are needed to examine associations of HCF admissions with co-use of alcohol and other substances among older adults with opioid overdose.
The study’s limitations are: (1) A large proportion of missing data on substance quantity in NPDS prevented factoring in drug potency. In addition, data collection methods in the 55 poison centers may not have been uniform, which may have affected inter-center reliability of the data. (2) Because NPDS does not include data on physical and mental health conditions and pain, they could not be controlled in our analyses. (3) Since NPDS contains only exposures that are reported (usually by telephone) to poison centers, they likely do not represent all exposures among the population, limiting the findings’ generalizability.
The findings have the following clinical and research implications: First, healthcare providers should carefully monitor the medication use of older adults prescribed opioids and avoid prescribing medications that likely increase the risk of opioid poisoning, either unintentionally or intentionally. The large proportion of suspected suicide among older-adult prescription opioid exposure cases also underscore the importance of suicide risk assessments. Second, healthcare providers should also educate their patients about the risks of taking multiple medications with prescription opioids and encourage them to engage in nonpharmacological interventions for alleviating pain. Third, more research is needed to examine the associations (or lack thereof) between noncritical/critical care admissions and antidepressants and NSAIDs, as well as alcohol and illicit drug co-use. Fourth, further research is needed to examine other physical/mental health factors that may be associated with adverse outcomes from prescription opioid use and co-use of other substances.
Conclusions
The findings show that among prescription opioid poisoning cases age 50+, co-use of several commonly prescribed/used medications was associated with increased risk of admissions to both noncritical and critical care units, and each additional medication substantially increased the risk. Healthcare providers should carefully monitor older adults who take prescription opioids and other medicines and educate them about the risks of prescription opioids and polypharmacy.
Footnotes
Acknowledgments
The American Association of Poison Control Centers made the National Poison Data System (NPDS) available to the authors for this study. This study’s findings and conclusions are those of the authors alone and do not necessarily represent the official position of the American Association of Poison Control Centers or participating poison control centers.
Author Contributions
All authors contributed to conceptualization. S.D.B. applied for and obtained the de-identified NPDS data and provided overall guidance on the data system and analysis. N.G.C. conducted data analysis and drafted the paper. B.Y.C. provided review of medications and direction for their analyses. C.N.M. provided statistical consultation, and D.M.D. contributed to editing the paper and provided feedback. All authors agree to publication of the paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant, P30AG066614, awarded to the Center on Aging and Population Sciences at The University of Texas at Austin by the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.