
Abstract
Keywords
Introduction
In the U.S., Medication Therapy Management (MTM) was first recognized as a service provided to selected Medicare beneficiaries which was based on the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA 2003). Medicare Part D Prescription Drug Benefit was first available to the Medicare beneficiaries starting on January 1, 2006. Benefit was provided to its beneficiaries either through a Medicare Advantage prescription drug plan or a stand-alone prescription drug plan. Besides providing prescription drug coverage, Medicare Part D sponsors were also required to offer a MTM service to eligible Medicare Part D beneficiaries. The goals of MTM were to provide education and counseling to improve Medicare beneficiaries’ understanding of their medications, to improve medication adherence, to decrease the risks of adverse drug events and to detect patterns of improper prescription medication use. These MTM services were developed in cooperation with licensed pharmacists and physicians; and there was no consensus on the recommended mode of delivery for MTM, such as by face-to-face, tele-health or by telephone.1-3
In 2004, a joint initiative of American Pharmacists Association (APhA) and National Association of Chain Drug Stores (NACDS) developed a consensus definition of MTM for the community pharmacy setting. The consensus definition of MTM was “a distinct service or group of services that optimize therapeutic outcomes for individual patients that are independent of, but can occur in conjunction with, the provision of a drug product.” This definition emphasized an additional key feature of MTM, that is, by providing documentation of the progress and serving as a liaison to the patient’s other healthcare providers. The framework of the MTM included five features, which were medication therapy review, personal medication record, mediation action plan, intervention and/or referral, and documentation and follow-up. Some of the pharmacist-provided MTM services or programs available were Project Improve Persistence and Compliance with Therapy (IMPACT), the Asheville Project, and other employer- or commercially sponsored programs.3-6 Similarly, other MTM administrative service companies such as Outcomes MTM and Mirixa were formed and able to build a comprehensive system to enable pharmacist-led MTM services.1,7-10
The MTM services were provided through the community pharmacy setting with features that involved a comprehensive medication review and an action plan. The action plan has proven to be effective in managing and monitoring various chronic disease states such as diabetes mellitus, hypertension, and dyslipidemia among elderly patients. Studies also demonstrated that such comprehensive MTM services could improve clinical outcomes, improved patient adherence, reduced hospitalization, decreased emergency room visits, and reduced healthcare cost.11-19
On April 10, 2012, U.S. Department of Health & Human Services Centers for Medicare & Medicaid Services (CMS) issued a memorandum with the guidance to Part D sponsors and organizations who were interested to offer a MTM program. A Part D sponsor or administrator was typically defined as a designated party or organization tasked with the responsibility of running a benefit plan. The memorandum suggested that a Part D sponsor must have established a MTM program based on the following criteria: 1. To ensure that covered Part D drugs were prescribed to targeted beneficiaries, 2. To reduce the risk of adverse events for targeted beneficiaries, 3. The program may be furnished by a pharmacist or other qualified provider, 4. The program may distinguish between services in ambulatory and institutional settings, and 5. The program must be developed in cooperation with licensed and practicing pharmacists and physicians. 20 In general, each developed program should include prescriber interventions to promote coordinated care, an interactive comprehensive medication review with beneficiaries to assess their medication therapies and creation of a medication action plan, and frequent monitoring and follow-up of the beneficiaries’ medication therapies. In this MTM approach, the eligible beneficiaries must have multiple chronic conditions with three chronic diseases being the maximum number, and who took multiple covered Part D drugs, with eight Part D drugs being the maximum number of drugs and who incurred annual costs for those drugs above a threshold set by the CMS. A pharmacist or other qualified provider would undertake the medication review directly with the Part D beneficiaries in an interactive person-to-person or conduct it by using telehealth technologies in a real-time basis. The Medicare Part D beneficiaries must receive a written or printed summary of the results of the review. 20 In the required MTM program, the Plan D sponsors must offer a minimum level of MTM services to each beneficiary enrolled in the program that included all of the following: 1. Interventions for both beneficiaries and prescribers, 2. An Annual CMR with written summaries in CMS’ standardized format, and 3.Quarterly targeted medication review (Quarterly TMR) with follow-up interventions when necessary. Thus, starting in 2013, the MTM program offered by sponsors of Part D Prescription Drug plans must include an Annual CMR and to accompany with follow-up interventions as needed.
As plan sponsors were required to establish Annual CMR, they were given the flexibility by CMS for designing programs that best suited their landscape. Various strategies for conducting Annual CMR had been implemented to include an outreach telephone call, face-to-face visitation, utilization of various quality of care indicators, and also various pharmacist-led MTM programs.
The goal of this study was to evaluate the impact of pharmacist’s interventions in Annual CMR for Medicare Part D beneficiaries by using a web-based technology that can incorporate all the necessary electronic records information of the patients for meaningful and effective medication review.
Methods
Brand New Day (BND), a Part D benefit sponsor, started with a unique goal of improving the quality of life for its members and physicians, and has been doing business for more than thirty-five years in Long Beach, California. 21 The Brand New Day model of care was designed with a focus on its members, members’ families, caregivers, and physicians in supporting each member’s healthcare needs through its comprehensive benefit program. This personalized benefit program helped to keep its members healthy and had care plans for those who had ongoing medical conditions such as diabetes, cardiovascular disease, dementia, or mental illness. Available to residents in California, individuals with Medicare and Medi-Cal or those who lived in long-term care facilities were enrolled with the Brand New Day HMO plan.
In compliance with the CMS requirement of Annual CMR regarding the covered Medicare beneficiaries for contract year 2013, Brand New Day had implemented a new web-based process to actively collect the patient’s health and medication information, to perform a comprehensive review of the medication, and provide an action plan to beneficiaries and their physicians. This documented action plan was to ensure that appropriate actions were implemented to improve the proper use and effectiveness of the medication. Collaborating with American University of Health Sciences (AUHS) School of Pharmacy, Brand New Day was able to develop a process by conducting Annual CMR for its Medicare beneficiaries.
Patients who participated in contract year 2012-2013 with Brand New Day HMO plans had met the criteria for Annual CMR and were enrolled in this program. The initial Annual CMR was conducted in October 2013 by a pharmacist and follow-up measures were performed until 2015 for a period of fifteen months. Patients who were considered eligible to participate in this Annual CMR were Medicare Part D beneficiaries who met all the following criteria: 20 1. Enrollees had multiple chronic diseases, with three chronic diseases being the maximum number required for targeted enrollment. If the enrollees did not have the minimum number of chronic diseases to be eligible for the MTM program, the minimum threshold for each beneficiary may set at two or three. 20 In addition, target enrollees or beneficiaries with any or specific chronic diseases may apply to this review program. However, those with specific chronic diseases must have at least five of the nine core chronic conditions, such as Alzheimer’s Disease, chronic heart failure (CHF), diabetes, dyslipidemia, end-stage renal disease (ESRD), hypertension, respiratory disease (such as asthma, chronic obstructive pulmonary disease, or chronic lung disorders), bone disease - arthritis (such as osteoporosis, osteoarthritis, or rheumatoid arthritis), or mental health (such as depression, schizophrenia, bipolar disorder, or chronic and disabling disorders). 20 2. Enrollees were taking multiple Part D drugs, with eight Part D drugs being the maximum number of drugs that may be required for targeted enrollment. However, the minimum threshold may set at a number equal to or between two and eight. 3. Enrollees were likely to incur the following annual Part D drug cost: for contract year 2013, the cost for covered Part D drugs were greater than or equal to $3144. 20
The Web-based Electronic Health Record.
aCerecons is now part of Medecision.
Data were collected at the first day of their comprehensive medication review by the pharmacist as a baseline data followed by the end of 3-month, 6-month, and 12-month intervals after the Annual CMR. Based on the recommendations by the pharmacist, data on pharmacist’s interventions were collected, analyzed and compared. Nominal and continuous data were analyzed by using appropriate statistical tests. A P value
Results
Patient Demographic Data, Medical Conditions & Multimorbidity.
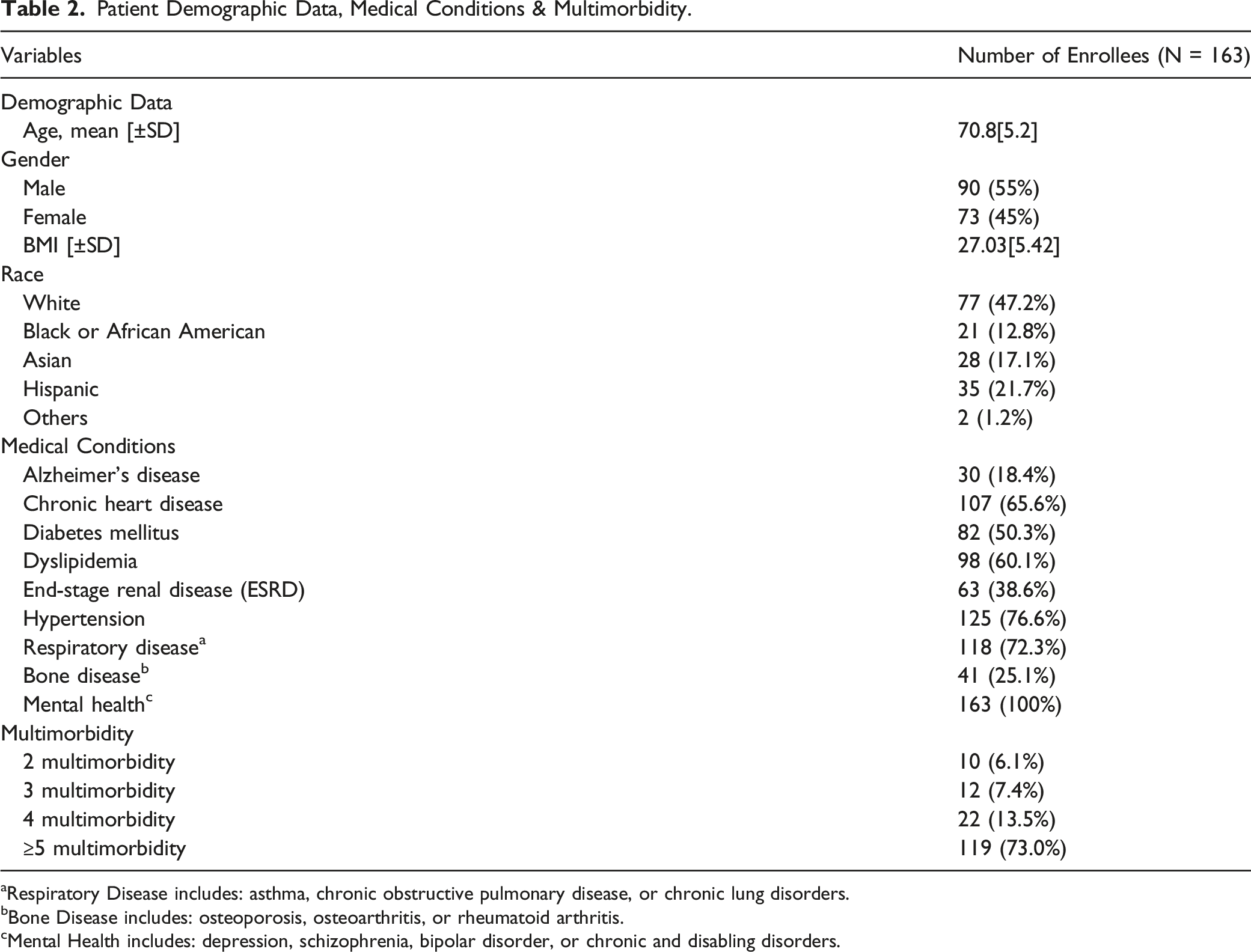
aRespiratory Disease includes: asthma, chronic obstructive pulmonary disease, or chronic lung disorders.
bBone Disease includes: osteoporosis, osteoarthritis, or rheumatoid arthritis.
cMental Health includes: depression, schizophrenia, bipolar disorder, or chronic and disabling disorders.
Enrollees with Interventions being Implemented.
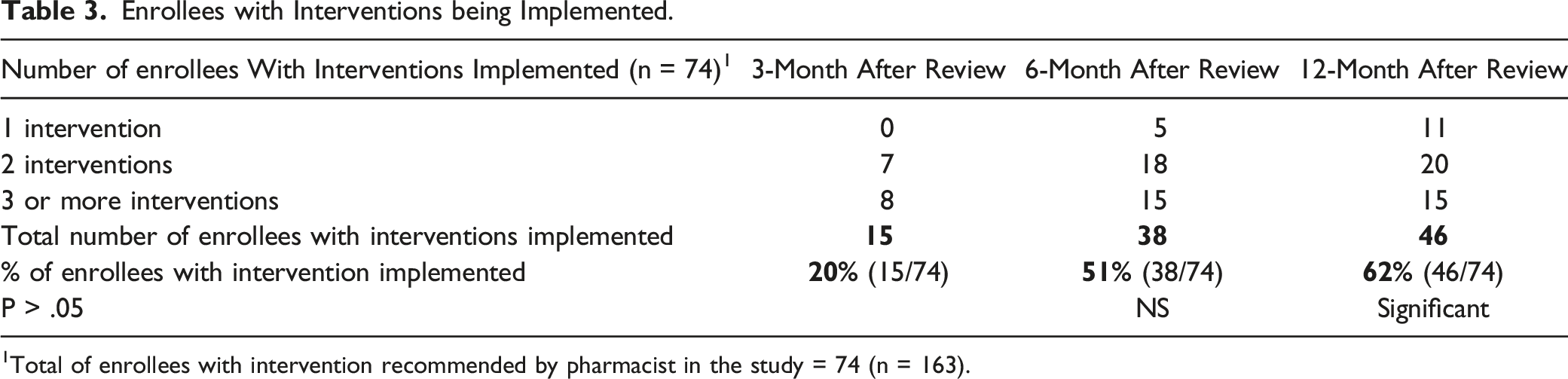
1Total of enrollees with intervention recommended by pharmacist in the study = 74 (n = 163).
Number of Pharmacist Interventions Implemented Over the Various Time Points.
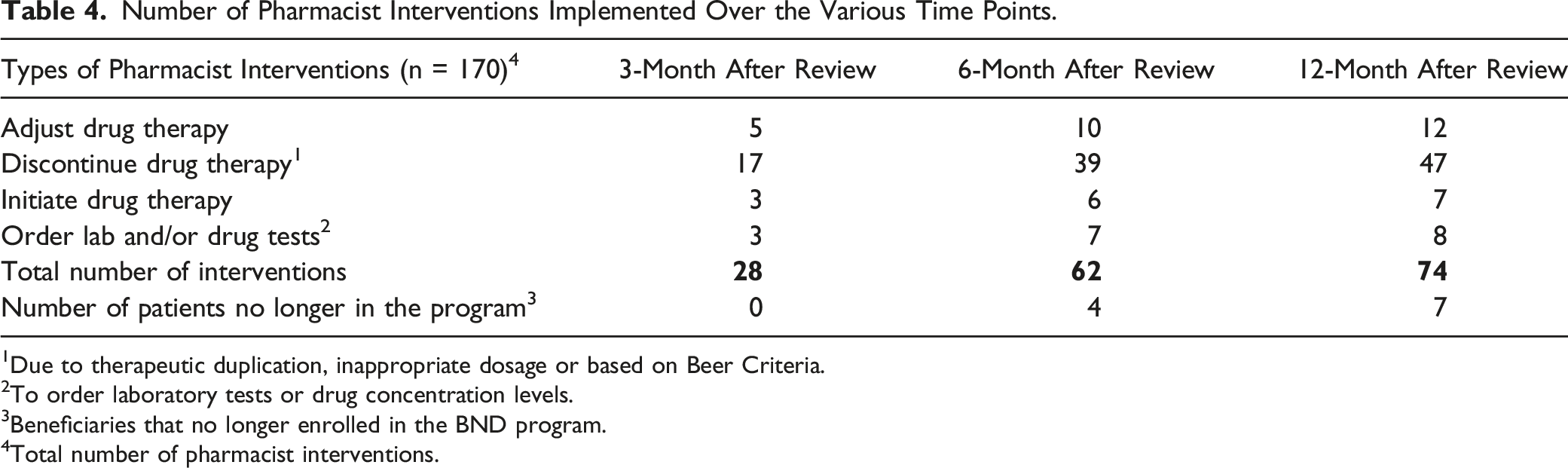
1Due to therapeutic duplication, inappropriate dosage or based on Beer Criteria.
2To order laboratory tests or drug concentration levels.
3Beneficiaries that no longer enrolled in the BND program.
4Total number of pharmacist interventions.
Number of Pharmacist Interventions Implemented on Drug Groups.
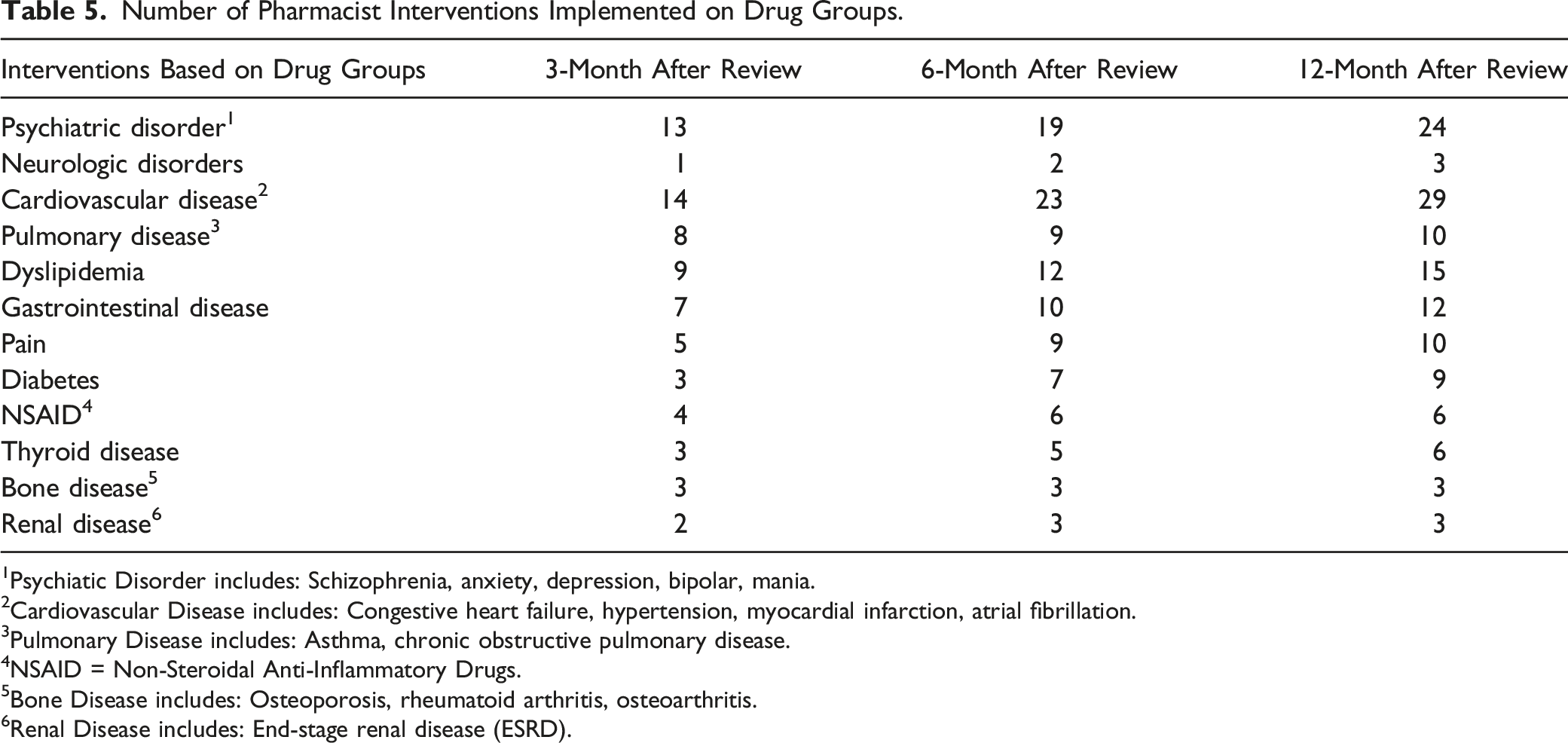
1Psychiatic Disorder includes: Schizophrenia, anxiety, depression, bipolar, mania.
2Cardiovascular Disease includes: Congestive heart failure, hypertension, myocardial infarction, atrial fibrillation.
3Pulmonary Disease includes: Asthma, chronic obstructive pulmonary disease.
4NSAID = Non-Steroidal Anti-Inflammatory Drugs.
5Bone Disease includes: Osteoporosis, rheumatoid arthritis, osteoarthritis.
6Renal Disease includes: End-stage renal disease (ESRD).
Discussion
The objective of this study was to evaluate the impact of pharmacist’s interventions on Annual CMR for Medicare Part D beneficiaries by using a web-based technology that can include all the necessary electronic records information of the patients for meaningful and effective medication review. The purpose of this Annual CMR was for the pharmacist to assess, review and provide feedback on proper and safe use of medications to the enrollees and to the primary care providers. At the time when CMS rolled out this Annual CMR program in 2013, there were no specific instructions to the plan sponsors or administrators regarding what method or approach to provide Annual CMR to eligible Medicare Part D beneficiaries. This study demonstrated that the pharmacist was able to effectively use a web-based electronic health record to accomplish an Annual CMR in collaboration with the primary care provider. The finding of this study revealed that such a web-based EHR system was a very useful tool in assisting pharmacists to assess and review the appropriate use of medication in the elderly Medicare Part D beneficiaries.
From the study, it was apparent that this digital device was an important tool for the pharmacist to perform effective Annual CMR. Using this EHR, the pharmacist was able to retrieve information about the patients, medical conditions, preventive assessment data, medication information and laboratory results. At the same time, enrollees and primary care providers were also able to access to this digital portal at their convenience. Thus, this EHR helped to expand the role of pharmacist to perform and in obtaining both meaningful and quality interventions for the proper and safe use of medication among these enrollees. It was shown that the acceptance rate for implementation of the pharmacist’s interventions by the primary care provider was very encouraging.22,23
An alarming finding from this study was that all eligible enrollees had at least 2 or more chronic diseases or medical conditions which were considered as multimorbidity. In fact, it showed that seventy-three percent (73%) of the enrollees had been diagnosed with five and more chronic diseases or multimorbidity. In the U.S., it was estimated that 3 in 4 adults over age 65 suffer from two or more chronic medical conditions such as diabetes mellitus, chronic kidney disease, hypertension, and chronic pain. 24 As patients developed these multiple chronic conditions or multimorbidity condition, they are likely to increase health resource utilization, requiring more complex physician’s visits and increased health expenditure. Having multiple chronic conditions, patients are vulnerable to medication nonadherence and eventually leading to unfavorable outcomes such as unnecessary emergency room (ER) visits, hospitalizations, adverse drug reactions, declining functional status, and mortality.24-26 Consistent with the finding from our study, there should be more studies focusing on pharmacist’s direct patient care role in improving proper and safe use of medication in patients with the complexity of multiple chronic conditions especially the elderly adults.
In the ever-changing healthcare environment, the role of pharmacists has continued to evolve along with the healthcare needs of our population. Besides dispensing medications, today’s pharmacists are taking a different role in an integral part of the healthcare team as medication experts to provide direct patient care in various practice settings. In this study, the accessibility to the web-based EHR allowed pharmacists to perform more patient care activities such as medication management, preventive care screenings and direct interaction with patients to identify potential drug interactions or related issues on the proper use of medication. Such activities conducted by pharmacists had shown to improve medication adherence and clinical outcomes for patients with chronic conditions such as diabetes, hypertension and cardiovascular disease.12-15 In the study, Table 3 and Table 4 showed the number of interventions recommended by the pharmacist and the different types of pharmacist’s interventions that were recommended during the Annual CMR process. A total of one hundred seventy interventions was initiated by the pharmacist which comprised of forty-five percent (45%) of the enrollees in the study. Interventions recommended by the pharmacist could be either one intervention, two interventions, or three or more interventions based on the amount of medication that the patient was taking for chronic medical conditions. It was interesting to notice that by using this web-based EHR, the pharmacist was able to initiate, to adjust, to order lab tests, and to discontinue medication to provide comprehensive medication management. Interventions included the switching to generic drugs, changing to more effective or less side effect drugs, initiate lipid-lowering agents, low-dose aspirin, angiotensin-converting inhibitors, angiotensin-converting blocker based on evidence-based standard of care, and discontinued medication based on Beer’s Criteria.22,23 From the finding, a total of seventy-four interventions were recommended by the pharmacists; 20%, 51% and 62% of these interventions were acknowledged and implemented by the medical providers at 3-month, 6-month, and 12-month intervals after the medication review respectively over a 12-month period, which demonstrated with a significant difference (P-value <.05).
The study revealed that the most common disease groups which were considered as non-communicable diseases that required interventions were psychiatric disorder, cardiovascular disease, dyslipidemia, gastrointestinal disease, pain and diabetes as shown in Table 5. Findings from other studies showed that certain conditions had higher frequency in their occurrence or re-occurrence such as depression associated with Alzheimer’s disease, diabetes and dyslipidemia, diabetes with hypertension and others. 27 Additional research in understanding the framework of this clustering of chronic diseases may help to better enhance patient adherence, improving clinical outcomes, and advancing health and wellness through the proper and safe use of medication.
Several limitations of this study were identified. First, the sample size (n = 163) was relatively small. The demographic data could be more appropriately represented if the number of eligible enrollees were included from multiple plan sponsors. Second, a face-to-face or a collaborative ambulatory care setting will be more effective in a direct patient care approach. Third, outcomes would be different if interventions by pharmacists could be on a continuous or interval basis. Fourth, it would be more informative if cost saving and other intangible benefits could be estimated appropriately through this study. Keeping in mind with the limitations as mentioned, by using web-based tool, pharmacists were able to recommend meaningful interventions to improve optimal drug use to improve health outcomes.
Conclusion
The finding from this study revealed that the Web-based EHR approach can be used as a meaningful and effective tool in assisting pharmacists to assess the proper and safe use of medication among the Medicare Part D beneficiaries through the Annual CMR.
Footnotes
Author’s Note
A part of this work was presented at the following conferences: American Association of College of Pharmacy (AACP) Annual Meeting, Pharmacy Education at Anaheim, California, USA on July 23-27, 2016; American Association of College of Pharmacy (AACP) Annual Meeting, Pharmacy Education at Grapevine, Texas, USA on July 26-30, 2014; and American Pharmacists Association (APhA) Annual Meeting and Exposition at Los Angeles, California, USA on March 1-4, 2013.
Acknowledgments
The authors would like to thank Laura Davis-Loschiavo from Brand New Day (BND) program and Pastor Gregory Johnson, Co-Founder of American University of Health Sciences for his full support on this project. This study had been approved by American University of Health Sciences (AUHS) Institutional Review Board (IRB) committee.
Author Contributions
Dr. Mok Thoong Chong contributed to the design of the study, data collection and analysis, writing of the manuscript, and preparation of the final draft. Desiree S. Chong, Doctor of Pharmacy (Pharm.D) Candidate, (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.