
Abstract
Introduction
Sickle Cell Disease (SCD) is a common heritable hematological disorder affecting more than 100 000 individuals in the United States. 1 Approximately, 1 out of every 365 births occurs in Blacks or African Americans.1SCD is an umbrella term that is used to refer to all genotypes that cause the characteristic clinical syndrome. 2 Sickle cell anemia is the most common subset of SCD and refers specifically to the βS allele for homozygosity. 2 It is a genetic disorder often characterized by hemolytic anemia, end organ damage and vaso-occlusive crises (VOCs). 3 A VOC, the most common complication of SCD, is defined as an acute episode of severe pain resulting from tissue ischemia due to vaso-occlusion typically in the bones and bone marrow. 4 VOC is also one of the main reasons that patients are hospitalized at high rates and is often linked to early mortality rates.3,5,6 Additionally, patients suffering from SCD often experience chronic pain. 7
The primary method of management for a VOC is with analgesics, most commonly with opioids. 4 In addition to opioids, chronic therapies for pain management may include NSAIDs, anticonvulsants such as gabapentin for neuropathic pain and use of diazepam for anxiety related pain. 8 For acute treatment of pain related to a VOC, rapid treatment with parenteral opioids is recommended due to their fast onset. Outpatient treatment of chronic pain is adequately treated with oral analgesics. 9 It is important to determine the incidence of opioid misuse amongst patients with SCD since the United States is currently experiencing an opioid epidemic.10,11 In a study investigating pain management in adults with SCD, patients were asked to self-report on the pain medications they were using at home. The most reported opioid analgesics being used in this study were oxycodone and codeine. 12 However, a study by Han and colleagues 7 purported that the most utilized analgesics for pain in their adult patients with SCD contained hydrocodone and oxycodone. Although the results of these studies provide insight on the most used analgesics reported by patients, the type of opioids can vary by institution and determined by a participant’s insurance.
A study by the Medical University of South Carolina showed that in the United States, providers are more likely to prescribe stronger, longer-acting opioids for chronic pain management than non-US providers. 9 However, US prescribers are also more inclined to perform urine drug tests and to utilize databases that track prescriptions. 9 Still, data show the results of these urine drug screens are hard to come by or inconsistently reported. 9 The information elucidated from these databases include urine drug screens which can be very useful in highlighting patient characteristics associated with prescription misuse. Additionally, it can help identify patients who need treatment modification if prescriptions are consistently being used inappropriately. Studies have shown that of all prescriptions filled for pain medications, those filled for opioids have the strongest rates of misuse.10,11 This is quite a concern as chronic pain medications are a necessary way of life for those living with SCD. 9
There are some studies that show that patients with SCD require opioid dose escalation for chronic pain due to tolerance and continuous pain potentially equating to high morphine milligram equivalent (MME) doses.13-15 A study by Karafin and colleagues 15 showed that patients on 90 MMEs or higher had worse mental health, higher somatic symptom burden and worse health related quality of life (HRQOL). However, no data has been published on the impact of MMEs on the rate of opioid misuse particularly in SCD. Other studies have highlighted the use of marijuana as a treatment for pain in patients with SCD.16,17 However, the impact of marijuana as a predictor of misuse is lacking. Nevertheless, distinction should be made between the use of medical marijuana for treatment of acute pain in comparison to the use of illicit marijuana. The lack of information on the rates of misuse and/or predictors in this population presents an opportunity for investigation with the primary focus of the study being based on illicit marijuana. Therefore, the primary objective of this study is to determine the rates of opioid misuse of participants with SCD in an urban setting by assessing the rate of unexpected drug screening results in a SCD clinic.
Methods
Study Design
This was a retrospective chart review study conducted at the outpatient SCD clinic at Howard University Hospital (HUH). Approximately 100 participants with SCD diagnosis were identified for chart review. However, only 71 participants were included in the analysis with 29 participants not meeting the inclusion criteria or missing information. Participants were included if they had frequented the clinic within the previous 3 months of data collection, were 18 years or older, had received either a buccal swab or urine drug sample and prescribed at least one opioid. Participants were excluded if they were 17 years or younger or had not received either a buccal swab or urine drug sample or prescribed an opioid. The researchers in this study defined the word “misuse” as when a patient had an opioid metabolite present in their urine or buccal sample when it should not be present, or when an opioid metabolite was missing in their sample when it should be present. The study was approved by the Howard University IRB on October 12, 2020.
Data Collection
The participant profiles that were used in this study were extracted from the electronic medical records database. Information about the urine and drug swab testing of metabolites was found in the drug screening toxicity database. The electronic medical record database was used to extract information on prescribed opioid medications. This information was retrospectively collected from participants during the time period of July 1, 2018, to June 30, 2020.
The primary independent variables were the opioid medications that were prescribed to the participants. The primary dependent variable was the metabolite that was obtained from the urine or buccal sample. Several covariates were collected as a part of this study. Additional information collected from respondents included demographic data such as age, gender, race, ethnicity, insurance, date of visits, names of SCD management drugs prescribed, names of pain management drugs prescribed from the electronic medical records database and opioid metabolites present in buccal swab or urine sample. The SCD management drugs included hydroxyurea, L-glutamine and voxelotor.
Statistical Analyses
The statistical analysis was conducted using SPSS version 24. The variables were examined by the software to determine whether or not they were normally distributed. Descriptive statistics were utilized to characterize the population in terms of sociodemographic characteristics and their rates of opioid misuse based on gender, age, and SCD genotype. The rates of misuse between age groups with regards to opioids were assessed with a student t-test. Linear regression was conducted to compare the effect of each of the demographic variables, SCD genotype, types of opioids, number of pain medications and MMEs on the rates of opioid abuse. In our multivariate logistic regression, we adjusted for genotypes, gender, MMEs, marijuana and NSAIDs use. The significance level for all statistical analysis was set a priori at alpha <.05.
Results
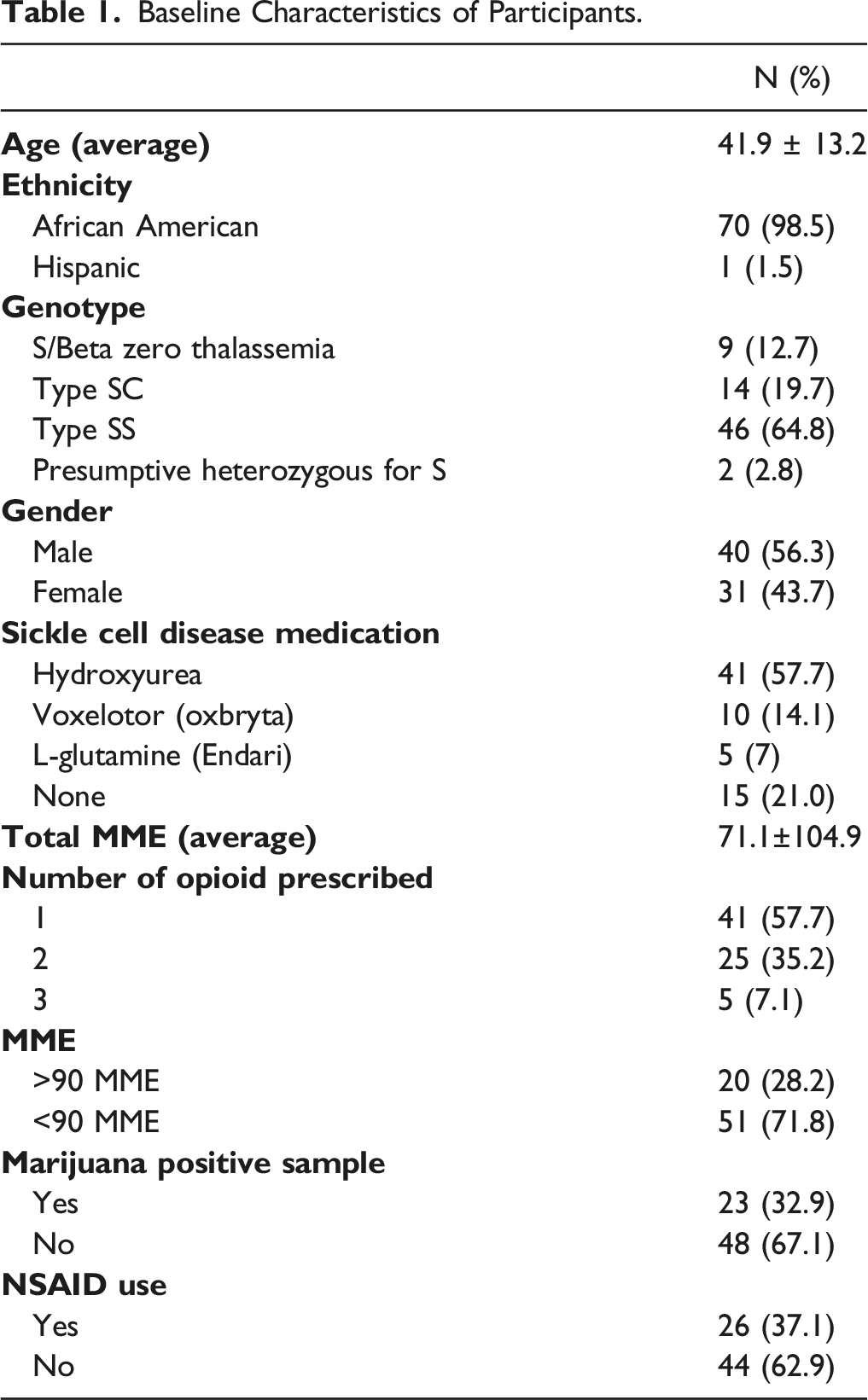
Baseline Characteristic of Participants
Baseline Characteristics of Participants.
Predictors for Opioid Misuse Among Patients With Sickle Cell Disease
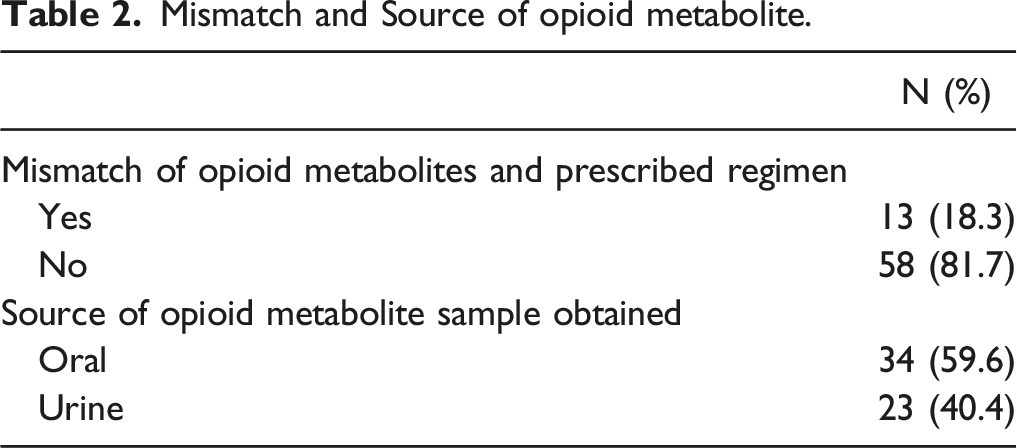
Mismatch and Source of opioid metabolite.
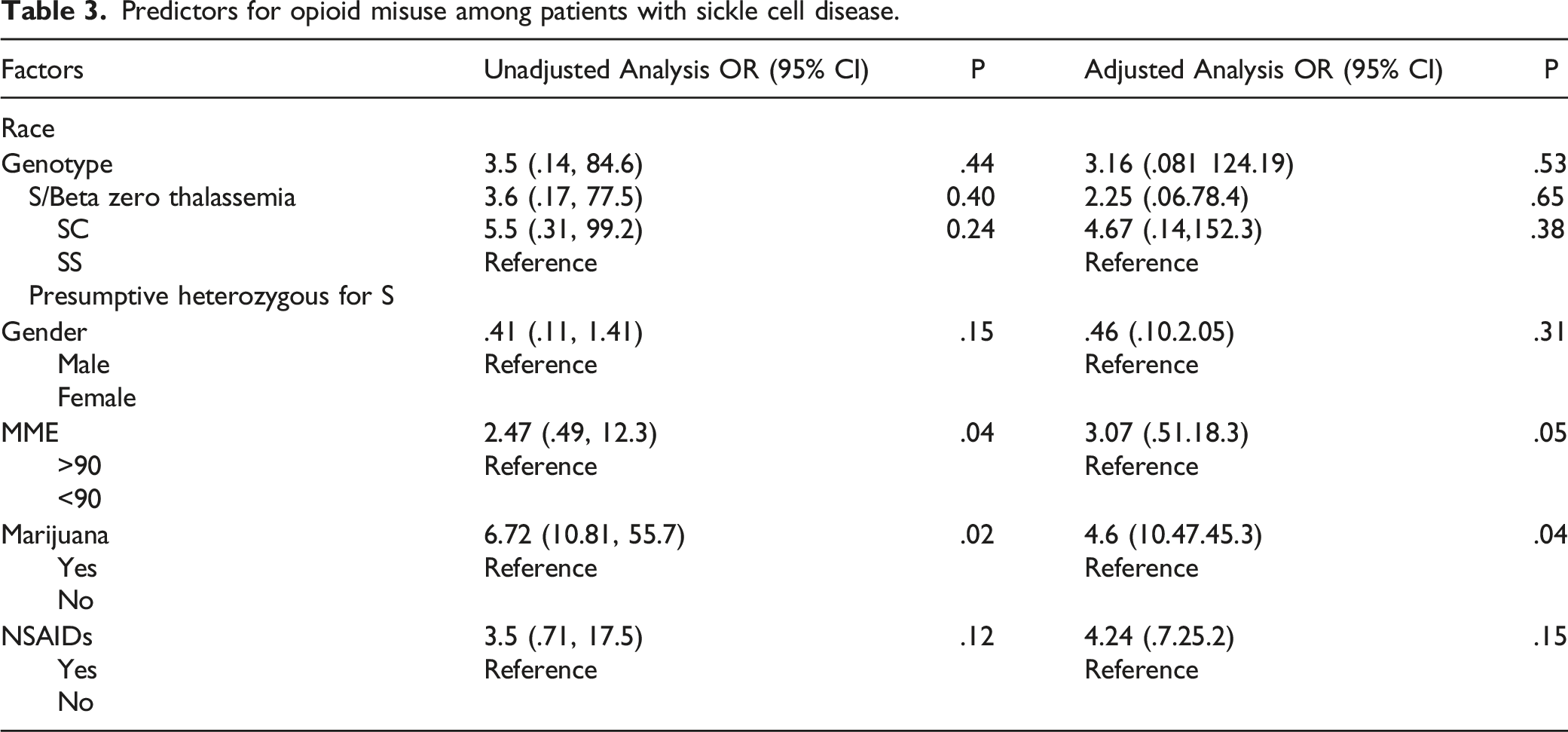
Predictors for opioid misuse among patients with sickle cell disease.
Discussion
Results of this study identify that many participants did not have an expected outcome as per the drug toxicity screening database (81.7%) and electronic medical records (69%) systems due to a mismatch between the pain management medications prescribed and the metabolites present in the urine or buccal sample. This study contributes to the literature by identifying factors that can be used to predict opioid misuse among participants with SCD. As per the results, the odds of misusing an opioid were 2.47 times higher if the participant was prescribed an opioid daily dose greater than 90 MME as opposed to a daily dose less than 90 MME. This is consistent with the study that showed that participants who had an opioid daily dose of >90 MME has a worse HRQOL outcome. 15 The study by Roberts and colleagues also showed that 83% of participants with an opioid daily dose of >90 MME had a higher prevalence of unemployment, 96% reported chronic pain and higher rates of hospital admissions (P<.0001). 15 Based on our study, there are additional concerns associated with surpassing the daily dose threshold of 90 MME among participants with SCD including greater risk of opioid misuse. With this information, prescribers and other care providers can provide targeted counseling and resources to those highest at risk of experiencing adverse consequences with chronic opioid use.
In our study, approximately one third of the participants were found to be using marijuana. This is consistent with other studies in which patients with SCD either self-report cannabis use or test positive for cannabis through urine drug screening tests.16,17 A study by Roberts and colleagues, 16 showed that 42% of the participants had reported marijuana use and of those 18% tested positive for cannabinoids only, while 12% tested positive for cocaine and phencyclidine and 5% tested positive for the combination of cannabinoids and cocaine/phencyclidine. The study by Howard and colleagues 17 showed that 36% of participants had used marijuana in the previous 12 months and that about 52% of participants used it for treatment of pain. In our study, the odds of misusing an opioid were 6.72 times higher if the patient was using marijuana defined as the presence of marijuana detected in the urine, compared to patients who did not use marijuana. There is some evidence that patients with SCD who test positive for cannabinoids are admitted to the hospital for the treatment of VOCs significantly more often than patients who do not use cannabinoids. 18 Increased marijuana use in patients with SCD has possibly been linked to undertreatment of pain from opioids or for use in anxiety or depression.16,19 In addition, some patients opted to use non-opioid alternatives such as marijuana for pain due to restricted access to opioids further increasing likelihood of misuse of illicit drugs. 19
Notably, 21% of the participants in our study were not prescribed any sickle cell disease medication, and studies have shown that this could potentially contribute to an increased likelihood of VOC occurring in these individuals.20–24 Proposed factors for those who might not be on SCD therapy could include but are not limited to high cost of medication, toxic side effects of medications, kidney and hepatic dysfunction, inability to be adherent to the regimen, or lack of benefit of previous SCD therapy. Therefore, there are various reasons why participants may not be on a SCD medication or might potentially be receiving exchange transfusions for management of VOCs. During the time of the data collection, patients who did not tolerate hydroxyurea due to toxicity or those found to be non-adherent had the medication discontinued. Many of those participants are now prescribed newer SCD medications which include L-glutamine that was FDA approved in 2017, voxelotor and crizanlizumab which were both FDA approved in 2019. Nevertheless, during the time of this study, newer SCD medications were not as widely prescribed and may have contributed to the overall low SCD medication use rate. Additionally, this study also included patients who receive exchange transfusions that could result in less than 3 VOCs per year, and thus decreasing their need for hydroxyurea therapy. It is reasonable to expect more participants to be initiated on newer SCD agents as prescribers become more comfortable utilizing these agents.
This study had a few limitations. First and foremost, the accuracy in the presence or absence of metabolite found in a participants’ urine or buccal sample may be compromised due to any of the following reasons: patient medication non-adherence, urine sample dilution by either participant or clinic, participant sample swapping due to clinic error, and lab sample reporting error to database. Missing metabolite in the system was also considered a limitation in this study as participants were observed to have run out of medication on the day the sample was collected. Therefore, this may have been indicated from the urine or buccal sample that participants were misusing. Missing metabolites can also indicate drug diversion in some participants, but this would be much harder to predict. Second, opioids administered in the emergency room or after a hospital admission have a high probability of being mislabeled as misuse when compared to the patient’s outpatient opioid prescriptions. In order to circumvent this, an extensive workup can be completed during each patient’s appointment, including recent hospitalizations and medication reconciliation. This would capture any one-time prescriptions that the patient may have been prescribed including those given on an as needed basis. Additionally, the use of controlled substance reporting software and electronic medical records, comes with limitations as not all pharmacies update the database every time a patient comes in with a controlled substance prescription, leading to discrepancies when collecting a medication list and assessing adherence.
This study may not be generalizable to the opioid utilization habits of patients with SCD in other communities around the United States. For one, this study was conducted at an outpatient clinic in an urban setting where a large percentage of the patients are on government insurance plans. As it has been stated earlier, the odds of misusing an opioid were higher if there was a presence of marijuana detected in the urine. Patient populations in areas more affluent may have better access to medications, thus medication non-adherence due to cost might not be applicable.
Conclusion
Participants were approximately 2.5 times more likely to misuse opioids if they consumed a daily dose of greater than 90 MMEs. Participants who were utilizing marijuana for pain management were also found to be more likely to misuse opioids. Therefore, it is important for the healthcare team to evaluate whether the management of SCD drugs is optimized. The optimization of SCD drugs will allow the participants with SCD to utilize less opioids for VOCs thus potentially reducing the risk of misuse. The healthcare team may also use the cut of greater than 90 MMEs per day to screen for patients most at risk of opioid misuse. Future studies should incorporate pharmacogenomics to better quantify the exact rate of misuse based on a participant’s unique ability to metabolize the medications. Future studies should also include assessment of medication adherence and effects of medications prescribed during any hospitalization or emergency room visits which could potentially affect the metabolites detected in the urine or buccal swab sample. As this study did not investigate an association between mismatch and source of samples, future studies may also seek to include this as an endpoint of interest.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.