
Abstract
Background
Chyle leakage, resulting in chylothorax or fistula, is a rare but potentially life-threatening complication following trauma, surgery, and thoracic and cardiac procedures (ie, coronary artery bypass grafting, neck dissection). Chylothorax is the presence of chyle, or lymphatic fluid, in the pleural space due to leakage from the thoracic duct or one of its main tributaries.1-3 Chylothorax is an uncommon sequela of thoracic trauma and surgery with a reported incidence of 0.2-9%, depending on the cause.4-10 Mortality rates associated with chylothorax have been reported between 15.5% and 75% due to complications of dehydration, malnutrition, and immunologic compromise.1,7,11
Conservative management is often used as first-line therapy which includes chest tube drainage, low-fat, medium chain fatty acids (MCFA) nutrition with possible bowel rest and total parental nutrition (TPN), adequate fluid replacement, and octreotide.1,5,10 Surgical management via thoracic duct band ligation can be employed when chest tube drainage exceeds 1 L per day; however, surgical re-exploration may be a high risk option.1,3-5,10,12
Octreotide, a long-acting somatostatin analog, binds to vascular somatostatin receptors reducing lymphatic fluid excretion. Additionally, octreotide increases splanchnic arteriolar resistance, decreases gastrointestinal blood flow, and reduces intestinal fat absorption.1,5,10,12 Octreotide is integral in the conservative management of chyle leak to help prevent surgical intervention, reduce treatment costs, and prevent morbidity and mortality. Commonly reported adverse effects include nausea, diarrhea, and abdominal distress; however, the incidence of serious adverse effects with octreotide therapy is low. 12 Several case reports and small studies have described the role of octreotide in the successful management of chyle leaks; however, there are no comparative reports evaluating octreotide dosing for this indication.1,4-6,9-15 The purpose of this study was to evaluate octreotide dosing in the medical management of chyle leak in patients with otolaryngologic, thoracic, and trauma surgeries.
Methods
Study Design and Data Collection
This was a retrospective, single center, cohort study performed at an urban, academic, quaternary referral, American College of Surgeons verified Level 1 trauma center. The institution has 724 licensed beds and had approximated 20 000 surgical encounters annually with 9000 for inpatients and 11 000 for outpatients in 2019. The study was approved by the local Institutional Review Board.
Patients were identified via a report from the electronic medical record (Epic, Epic Systems Corporation, Madison, WI) for octreotide administration and an ICD-9 or -10 diagnosis code for chyle leak. Diagnosis for chyle leak was confirmed through manual progress note documentation during chart review. Patients aged 18 years and older admitted to the trauma, cardiothoracic, or otolaryngology services between January 1, 2012 and June 30, 2021 were eligible for inclusion. Additionally, at least one dose of octreotide administered as an intravenous (IV) push, subcutaneous (SC) injection, or continuous IV infusion was required. Patients were excluded if they were pregnant or if octreotide was administered for diagnoses other than chyle leak. Institutional guidance for the management of chyle leak did not exist during the study period, and octreotide initiation and dosing was at the discretion of the treatment team.
Data was either extracted manually or from a report via the electronic medical record (EMR). Patient demographics including age, sex, height, weight, admitting team, and patient location at time of first octreotide order (eg, intensive care unit or floor/ward) were extracted from the EMR report. Hospital length of stay was provided by the EMR report. All other data was extracted manually including cause of the chyle leak; location of chyle leak and drainage catheter placement in the neck, chest, or abdomen; time in days from admission to chyle leak diagnosis and octreotide initiation; the need for any surgical procedure for definitive chyle leak management; time in days from chyle leak diagnosis to definitive surgical management; serum triglyceride concentrations; serum albumin concentration; in-hospital mortality; drain output, and octreotide and nutrition parameters described herein. The serum albumin drawn closest to octreotide initiation day was used for analysis.
Study Definitions and Outcomes
Patients were grouped and classified as medical management success or failure. Success was defined as resolution of chyle leak documented in a progress note with octreotide-based medical management without the need for surgical intervention. Failure was the need for surgical intervention for definitive management of chyle leak after the initiation of octreotide. Octreotide use following definitive surgical management was described, as appropriate. Subgroups based on chyle leak location were evaluated: (1) patients with chylothorax (ie, chest) due to acute injury or surgical complication, and (2) patients with head and neck procedures complicated by chyle leak.
Outcome data was assessed from octreotide initiation up to day 7 of use or drug discontinuation, whichever came first, unless otherwise specified. The primary outcome was the octreotide total daily dose compared between groups. Secondary outcomes included, weight-based dose per day, route(s) of administration, total cumulative dose, and treatment duration. Cumulative octreotide dose was calculated from EMR report of all administrations during treatment of chyle leak. Proportion of patients with octreotide 100 µg every 8 hours or 250 µg every 8 hours ordered at any time through the first 7 days of therapy was reported. Additional secondary endpoints were daily drain output, change in drain output, and nutrition management. Proportion of patients with complete and any bowel rest defined as no enteral intake and nil per os (NPO) orders, received any MCFA or low-fat diet and/or tube feeds, received any dietary intake with or without fat restriction, and received any TPN were reported. Duration of bowel rest in days and time to initiation of enteral intake in days was also evaluated.
Statistical Analyses
Descriptive statistics were used to summarize demographic data and clinical outcomes. Categorical data were analyzed using Chi-square or Fisher’s exact tests and reported as number (percent), as appropriate. Continuous data were analyzed using Student’s t-test or Wilcoxon Rank Sum and reported as mean (standard deviation [SD]) or median (interquartile range [IQR]), respectively, as appropriate. A P-value ≤ 0.05 was used to define statistically significant differences between groups. Independent risk factors associated with failure of medical management were evaluated with a multivariate logistic regression using variables identified with a P-value < 0.2 on univariate analysis. Daily octreotide dose was identified a priori for inclusion in the model if no other dose parameter had a P-value < 0.2. Statistical analyses were performed using SigmaPlot® 14.0 (Systat Software, Inc. San Jose, California).
A convenience sample over the 9-year period was used to capture the required population within the specified inclusion and exclusion criteria. An exploratory a priori power analysis was performed to determine daily dose difference between success and failure of medical management groups. This indicated that 58 patients were required to achieve 80% power at an alpha of .05 to find a mean daily octreotide dose difference of 75 ± 100 µg.
Results
Demographics
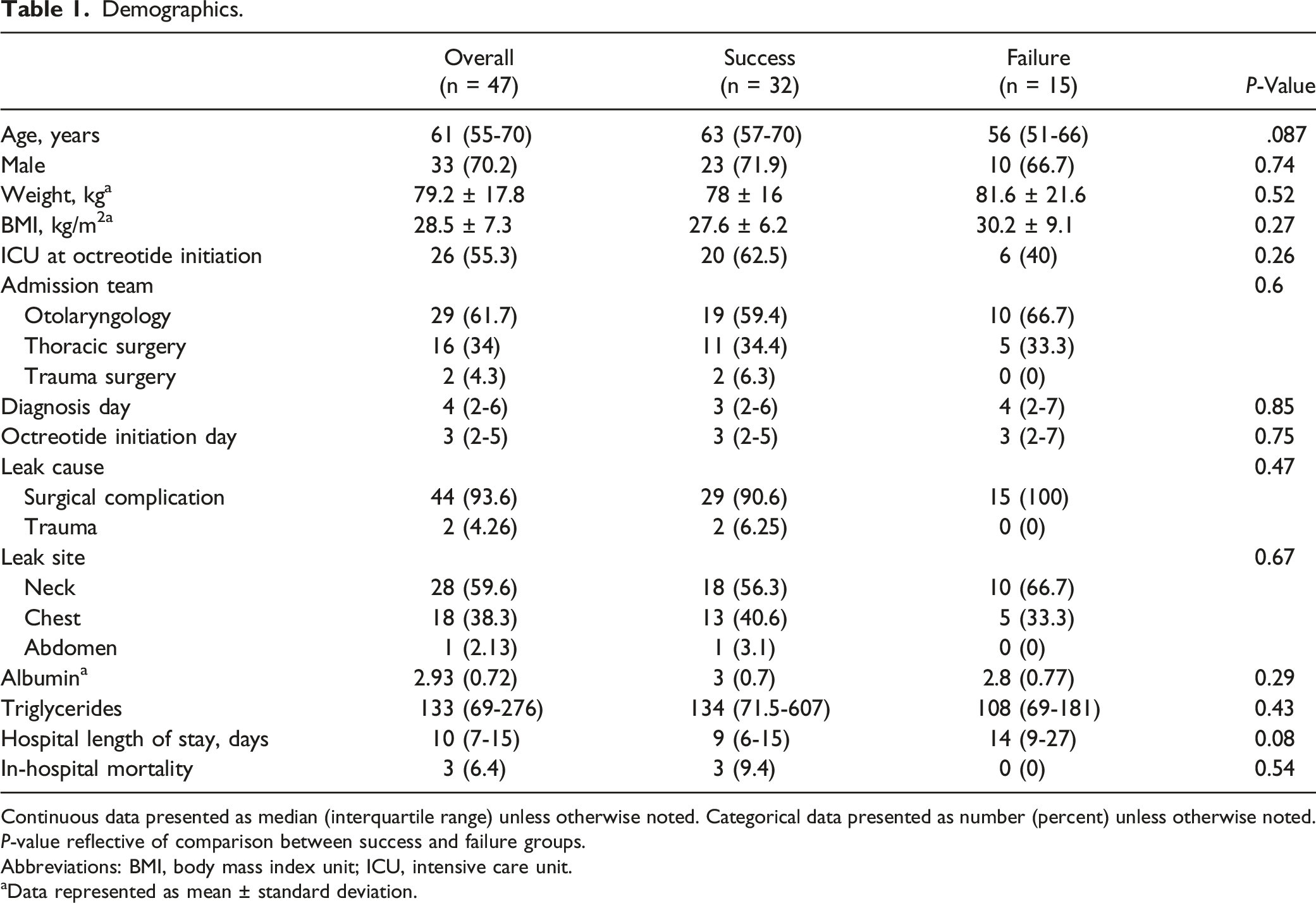
A total of 108 patients were identified from the EMR, and 47 met inclusion criteria (Figure 1). The study population had the following characteristics: 33 (70.2%) male, 61 (55-70) years of age, and 29 (61.7%) admitted to the otolaryngology service. Patients were diagnosed with chyle leak on hospital day 4 (IQR, 2-6) due primarily to surgical complications (44 [93.6%]) with octreotide initiation in the ICU (26 [55.3%]). Daily dose was 250 (IQR, 200-282) µg per day, and SC injection was the most common route of administration (34 [72.3%]); no patients received a continuous infusion of octreotide. Median length of stay was 10 (IQR, 7-15) days. Thirty-two (68.1%) patients had successful medical management of chyle leak while 15 (31.9%) failed and required surgical intervention. Baseline characteristics were similar between groups except the failure group had a significantly longer hospital length of stay (Table 1). In the failure group, surgery occurred a median of 4 (IQR, 2-9) days after octreotide initiation and 10 (66.7%) patients continued octreotide post-operatively. Patient inclusion. Demographics. Continuous data presented as median (interquartile range) unless otherwise noted. Categorical data presented as number (percent) unless otherwise noted. P-value reflective of comparison between success and failure groups. Abbreviations: BMI, body mass index unit; ICU, intensive care unit. aData represented as mean ± standard deviation.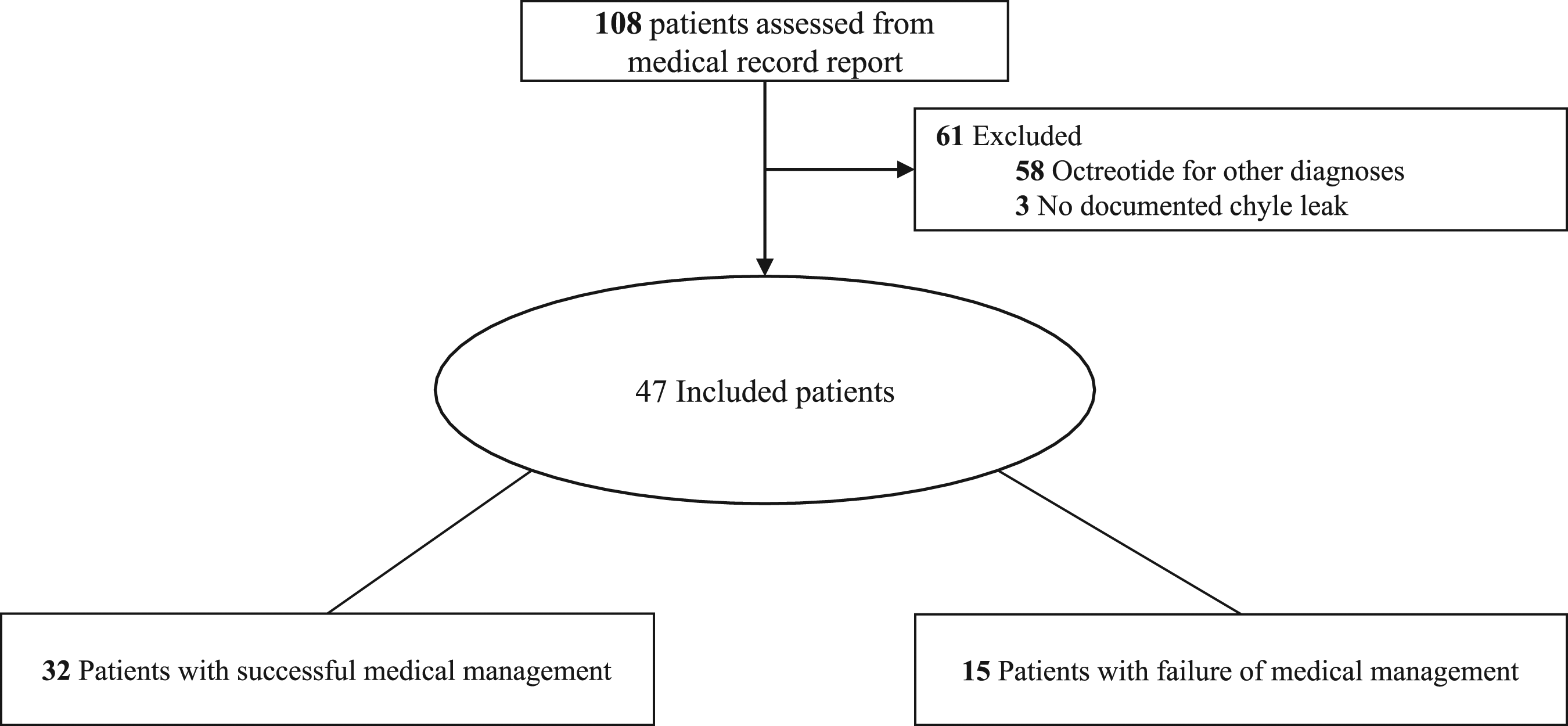
Outcomes
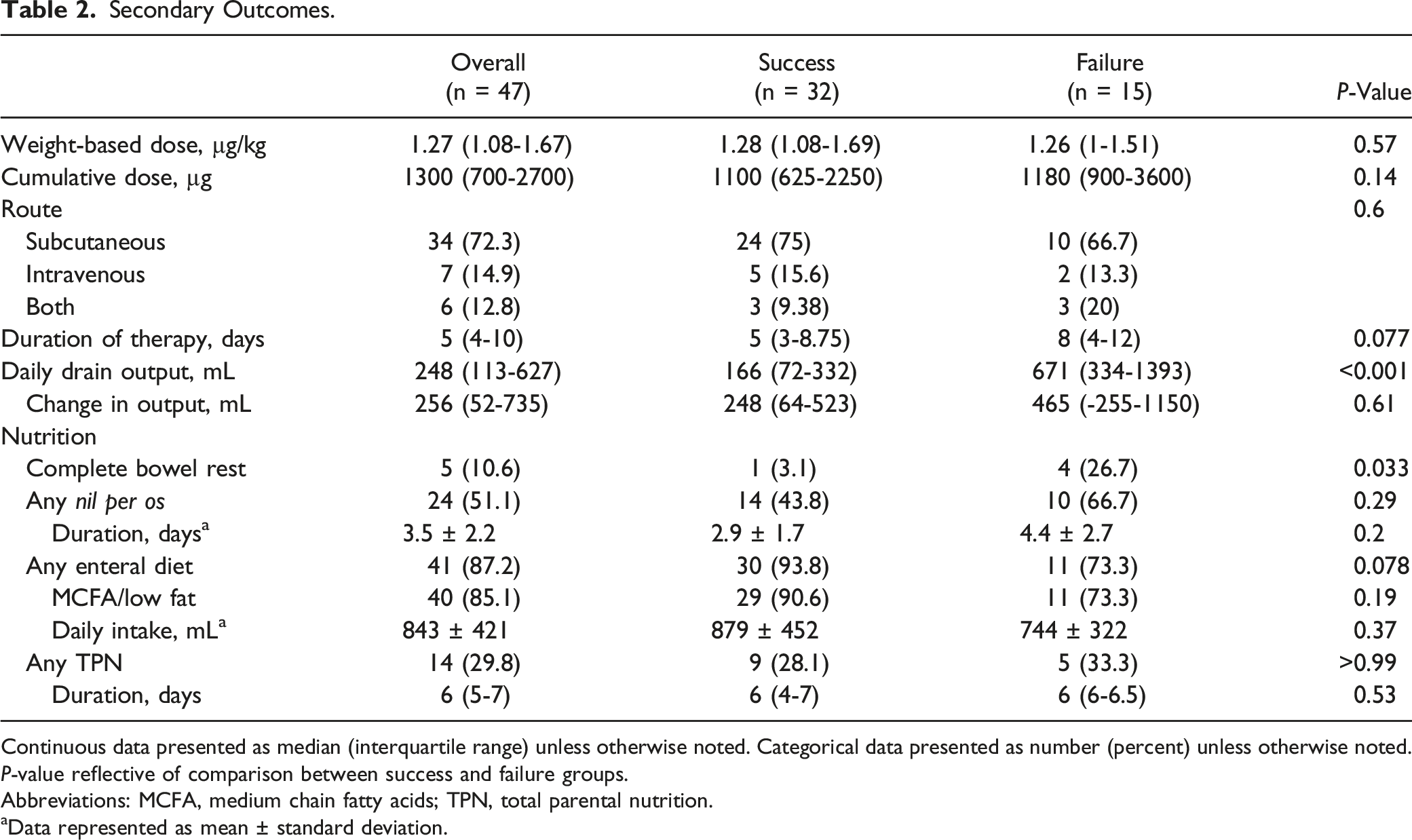
Daily dose of octreotide was similar between the success and failure groups (250 [IQR, 170-288] µg vs 253 [IQR, 200-282] µg, P = 0.9) (Figure 2). Proportion of patients ordered total daily dose of 300 µg (eg, 100 µg every 8 hours) or less was 29 (90.6%) vs. 15 (100%) per group, respectively (P = 0.54). Four (12.5%) patients in the success group received a total daily dose of 750 µg or more vs only 1 (6.7%) in the failure group (P > 0.99). Median daily weight-based dose was similar between groups and routes of administration were not different. Cumulative dose and duration of therapy were not statistically different but were numerically greater in the failure group (Table 2). Daily octreotide dose between patients with success and failure of medical management of chyle leak. Secondary Outcomes. Continuous data presented as median (interquartile range) unless otherwise noted. Categorical data presented as number (percent) unless otherwise noted. P-value reflective of comparison between success and failure groups. Abbreviations: MCFA, medium chain fatty acids; TPN, total parental nutrition. aData represented as mean ± standard deviation.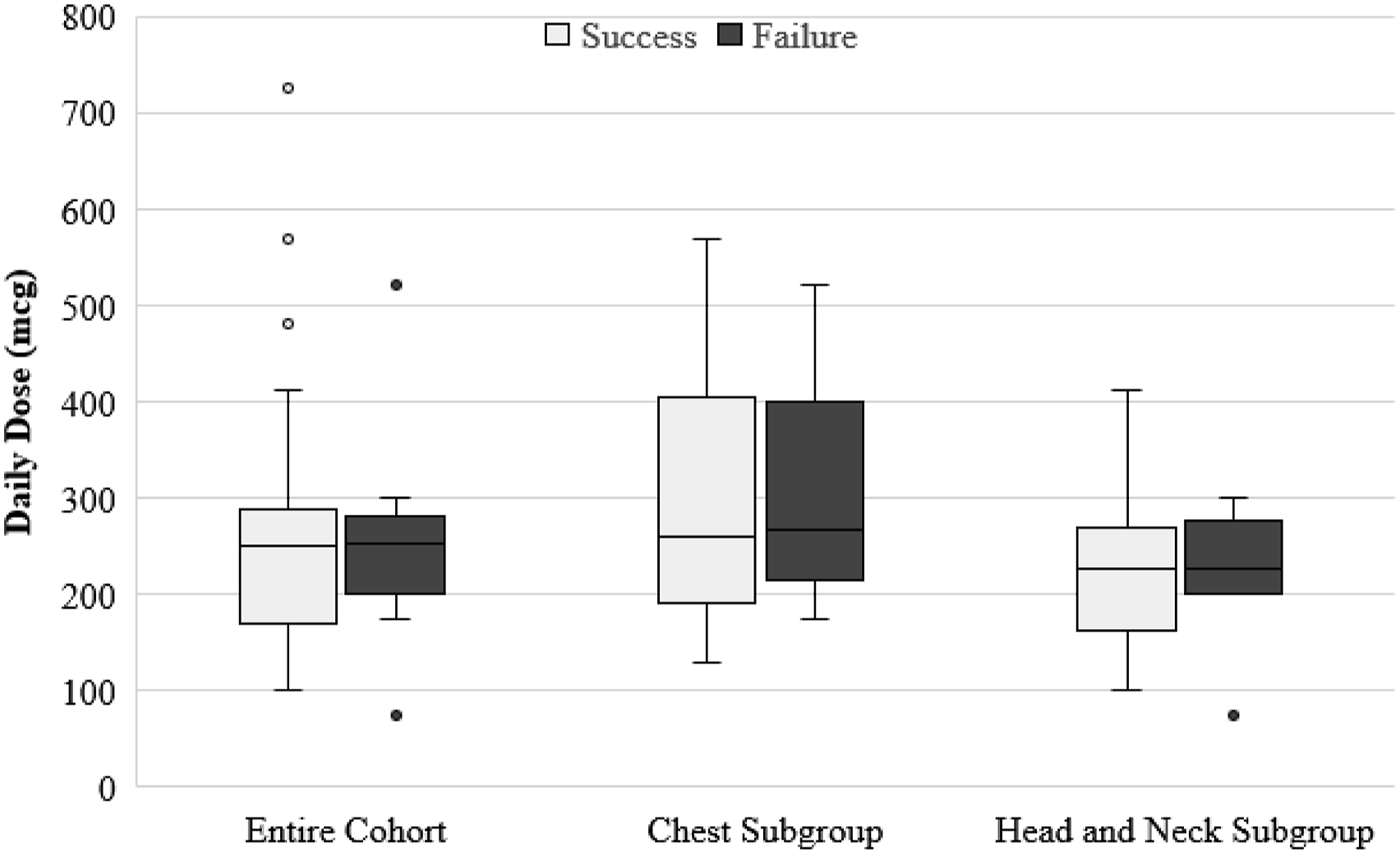
Risk Factors for Requiring Surgical Intervention.
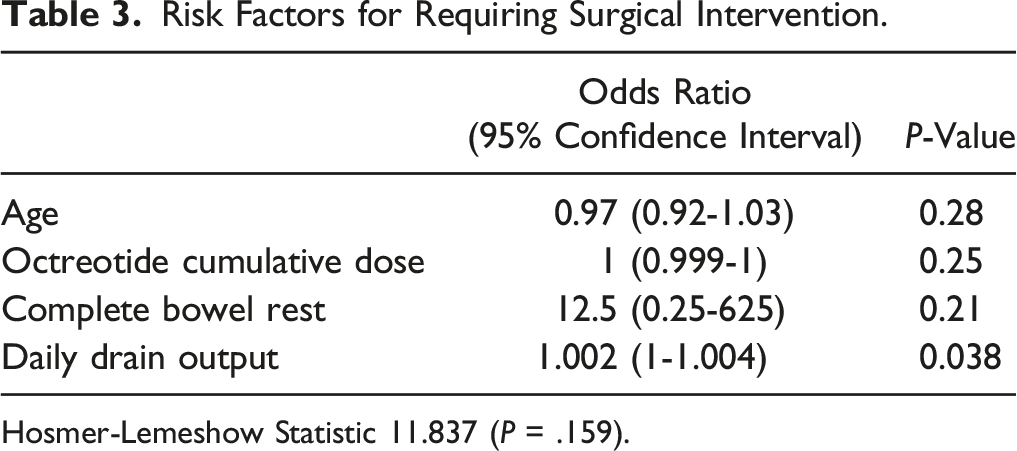
Hosmer-Lemeshow Statistic 11.837 (P = .159).
Chest Subgroup
The thoracic cavity was the site of the chyle leak (ie, chylothorax) for 18 patients. Thirteen (72.2%) patients had successful medical management while 5 (27.7%) failed and required surgical intervention. In the failure group, surgery occurred a median of 8 (IQR, 3.5-12.5) days after octreotide initiation and all continued octreotide post-operatively for a median of 4 (IQR, 2.25-13) days. Demographics were similar between groups except hospital length of stay was clinically longer in the failure group (13 [IQR, 8.5-21.5] days vs 27 [IQR, 18-34.5] days, P = 0.08) (Supplementary Table 1). There was no statistical difference in daily octreotide dose between groups (260 [IQR, 192-406] µg vs 267 [IQR, 214-401] µg, P = 0.77) (Figure 2). Weight-based daily dose and route of administration were no different between groups. Cumulative dose (2769 ± 2194 µg vs 4530 ± 2808 µg, P = 0.18) and duration of therapy (8.6 ± 4 days vs 15 ± 9.8, P = 0.22) were not statistically different but were numerically greater in the failure group (Supplementary Table 2).
Daily drain output was numerically higher in the failure group (P = 0.051). There were no statistical differences in use of TPN, NPO, and MCFA/low fat enteral diet. Duration of NPO was numerically but not statistically longer in the failure group (Supplementary Table 2).
Otolaryngologic Subgroup
Chyle leak following head and neck procedures occurred in 28 patients. Eighteen (64.3%) patients had successful medical management while 10 (35.7%) failed and required surgical intervention. Surgery occurred a median of 3 (IQR, 1.5-6) days after octreotide initiation and 5 (50%) continued octreotide post-operatively for a median of 2 (IQR, 1.5-6) days in the failure group. Demographics were similar between groups except the failure group was 10 years younger (64.4 ± 10.4 years vs 54.3 ± 11, P = 0.023) and had a numerically longer length of stay (7 [IQR, 5-9.5] days vs 10 [IQR, 7.8-14] days, P = 0.08) (Supplementary Table 1). There was no statistical difference in daily octreotide dose between groups (224.6 ± 75 µg vs 226.2 ± 64.1, P = 0.96]) (Figure 2). Weight-based dose and routes of administration were similar between groups. Cumulative dose was numerically greater (850 [475-1150] µg vs 1500 [IQR, 875-2300] µg, P = 0.052) and duration of therapy was statistically longer in the failure group (4 [2-5.3] days vs 6 [4-9.3] days, P = 0.024) (Supplementary Table 2).
Daily drain output was significantly higher in the failure group (P = 0.002). There were no statistical differences in use of TPN, NPO, duration of NPO, and MCFA/low fat enteral diet (Supplementary Table 2).
Discussion
This study is the largest single report of octreotide use in the management of chyle leak in surgical patients and the first to compare octreotide dosing strategies for patients with and without successful medical management, including subgroups based on chyle leak location. There was no difference in daily octreotide dose for patients with success or failure of medical management. Patients requiring surgical management of the chyle leak had numerically higher cumulative octreotide doses and longer duration of therapy. However, this was likely a clinical consequence of medical treatment failure which is also reflected in the longer length of stay in the failure group. Daily drain output was higher in patients who failed medical management. Moreover, higher drain output was predictive of the need for surgical intervention.
To our knowledge, this is the first retrospective study of octreotide dosing in the conservative management of chyle leak. Animal studies have shown octreotide effectiveness in thoracic duct injury through chyle drainage reduction and early fistula closure.16-18 Use of high-dose octreotide is a well-recognized treatment option in the management of chylothorax in pediatric patients and has been reported in doses up to 15 µg/hour for up to 21 days.10,19 Conservative management with octreotide has been explored in several case reports and case series in adults which reported total daily doses ranging from 150 to 750 µg.1,4-6,9,10,12-15 There are no prospective randomized trials of octreotide in adults with chyle leak secondary to surgery or trauma.
Our retrospective analysis showed no difference in octreotide dose between patients with and without successful medical management of chyle leak likely due to the majority of patients receiving no more than 300 µg per day (ie, 100 µg three times per day). It is unclear based on the undertaken chart review if different management strategies such as complete bowel rest over continued enteral intake with MCFA/low fat diet was driven by higher drain output. Future analysis of the complex association between various interventions and octreotide dose is needed. The heterogenous population of the study may also have influenced the findings given the observed higher output in the chest subgroup over the head and neck subgroup. Moreover, higher daily drain output was an independent risk factor for requiring surgical management of the chyle leak. It is unclear in this investigation if there is a specific threshold for output compared to octreotide and optimized nutrition to guide clinical practice. Larger randomized-controlled trials are necessary to determine the ideal octreotide dose in the management of chyle leak.
This study is not without limitations. The retrospective nature limited control over the data extracted from the EMR. Data collection of drain output relied on chart notes and data reported by healthcare personnel into the EMR. Nutritional management such as TPN, NPO, enteral nutrition, and MCFA/low-fat diet were evaluated through chart notes; however, reported data was not consistent. Generalizability is limited due to the inability to control for variables such as selection of specific octreotide doses. Similarly, this was a single center experience, albeit a 9-year evaluation. Our report relied on serum albumin and triglycerides as a biomarker for nutritional status without the ability to determine patient-specific caloric goals including total protein and fat intake. This may be a potential confounder since nutrition is an integral intervention in the management of chyle leaks, and controlling dietary management in future studies may better inform clinical decision making. Last, a convenience sample was employed due to the rarity of chyle leak diagnoses and the hypothesized dose differences were not observed. The relatively small sample size likely limited the ability to find statistical significance where numerical and arguably clinical difference is present for secondary outcomes such as drain output and duration of treatment.
There are several strengths presented in this investigation. It is the largest, single center investigation of octreotide dosing in the management of chyle leak and provides more extensive pilot data to guide future prospective investigations. Comparisons were able to be performed between patients with and without surgery, which has not been available in prior case studies and series. Investigation into multiple demographic and clinical endpoints provide a thorough picture to contextualize patient care for externalization. This includes weight-based octreotide dose, duration of octreotide, drain output, and nutrition management. Presented subgroups based on anatomic leak location also provides refinement around clinical application given possible pathophysiologic and surgical differences within each subpopulation.
Conclusions
Daily octreotide dose was not different between patients with and without successful medical management of chyle leak in otolaryngologic, thoracic, and trauma surgery patients. No additional difference was observed when exploring specific subpopulations based on anatomic site of the chyle leak. However, numerical differences were seen in duration of therapy and length of stay, which may be clinical consequences of requiring surgical management but deserves greater exploration. Larger studies are necessary to discern the ideal octreotide dose relative to drain output for optimized medical management of chyle leaks.
Supplemental Material
Supplemental Material - Octreotide Dosing in the Medical Management of Chyle Leak Following Otolaryngologic, Thoracic, and Trauma Surgery: A 9-Year Evaluation
Supplementary Material for Octreotide Dosing in the Medical Management of Chyle Leak Following Otolaryngologic, Thoracic, and Trauma Surgery: A 9-Year Evaluation by Kelly L. Strama, Timothy D. Rice, Jacob P. Ruff, Kristen E. Carter, Neil E. Ernst, Dalton J. Kuebel, and Molly E. Droege in Journal of Pharmacy Practice.
Footnotes
Acknowledgments
The authors would like to acknowledge Carolyn Philpott, PharmD, BCCCP for supporting this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was obtained from the University of Cincinnati.
Informed Consent
Waiver for consent was obtained from the University of Cincinnati Institutional Review Board due to the retrospective nature of the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.