
Abstract
Introduction
Chronic alcohol consumers are at high risk for malnutrition and thus vitamin deficiencies, namely cyanocobalamin, folate, and thiamine. These deficiencies can lead to significant diseases including chronic anemia and Wernicke-Korsakoff syndrome.1,2 In attempts to replenish these vitamin deficits and prevent disease, some providers prefer the use of intravenous (IV) vitamin administration to chronic alcohol consumers presenting to the emergency department (ED). However, the benefit of empiric IV multivitamin supplementation, outside of thiamine, when the serum levels are unknown has not been clinically proven to prevent subsequent disease.3,4 Giving empiric IV multivitamins also comes with several concerns that may include potential vitamin toxicities or allergic reactions, additional costs, unnecessary IV access, and risk of infection at the IV site.3-6
To implement evidence-based medicine in the ED regarding the utilization of vitamin therapies in an alcohol-related diagnosis, a group of researchers employed an intervention at our institution in 2009 to change practice. 7 This intervention consisted of changes to the default order entry settings in our hospital’s electronic medical record (EMR) as well as education to the emergency providers. These EMR changes consisted of adding an option for an enteral multivitamin which replaced the intravenous multivitamin infusion (MVI) option that had 1 L of fluid including 10 mL of parenteral multivitamin, 100 mg of thiamine, and 1 mg of folic acid given over 30-60 minutes. IV thiamine was still an option on the orderset as the parenteral route of thiamine is preferred; however, intramuscular and enteral thiamine selections were also added to the orderset in the event that the patient did not have IV access. Folic acid was not addressed with this intervention. The purpose of this intervention was to most importantly decrease parenteral multivitamins and to encourage the use of enteral multivitamins instead, if still warranted. The intervention was not supporting a decrease in the use of thiamine overall, rather to encourage alternate routes for thiamine administration including enteral and intramuscular if IV access were not available. Data were collected for 1 year after the intervention and showed success with a significant decrease of 8.7% (95% CI 6.8, 11) in the overall percentage per month of patients receiving intravenous MVIs in the ED before and after the intervention. Alternative vitamin treatments, which included any route of thiamine and enteral multivitamin increased from zero to an average of 17 (95% CI 13.7, 19.5) treatments per month after the intervention. 7
We sought to perform a follow up study to the previously mentioned intervention with a purpose being to illustrate that implementing an intervention in the ED can subsequently impact hospital-wide practice. The ED may be an optimal place to make an impactful intervention because therapeutic momentum, defined as the reluctance to initiate/step down/withdraw therapy when further prescription is not needed or supported by evidence, starts in the ED and is often continued throughout the patient’s admission.8-10 There have been multiple studies that show that the decisions made in the ED guide subsequent inpatient care.9,10 This presents a significant responsibility to emergency providers to initiate the appropriate therapy early in the patient’s course of treatment as it may not be changed once the patient is admitted to an inpatient unit. Therefore, providing education to emergency providers and executing a targeted intervention in the ED optimizes time and efforts, while still allowing benefits to be seen outside of the ED.
The objective of this study was to determine whether the impact of a historical intervention implemented in the ED led to changes in hospital prescribing practices of vitamin therapies. The secondary objective was to evaluate the sustainability of the effect of the previous intervention made in 2009 within the ED over time measured by having the same or fewer MVIs ordered in the ED from 2009 to the end of this study period.
Methods
ICD-9 and ICD-10 Codes That Were Used to Identify Records and Medication Administrations for Patients With an Alcohol-Related Illness.
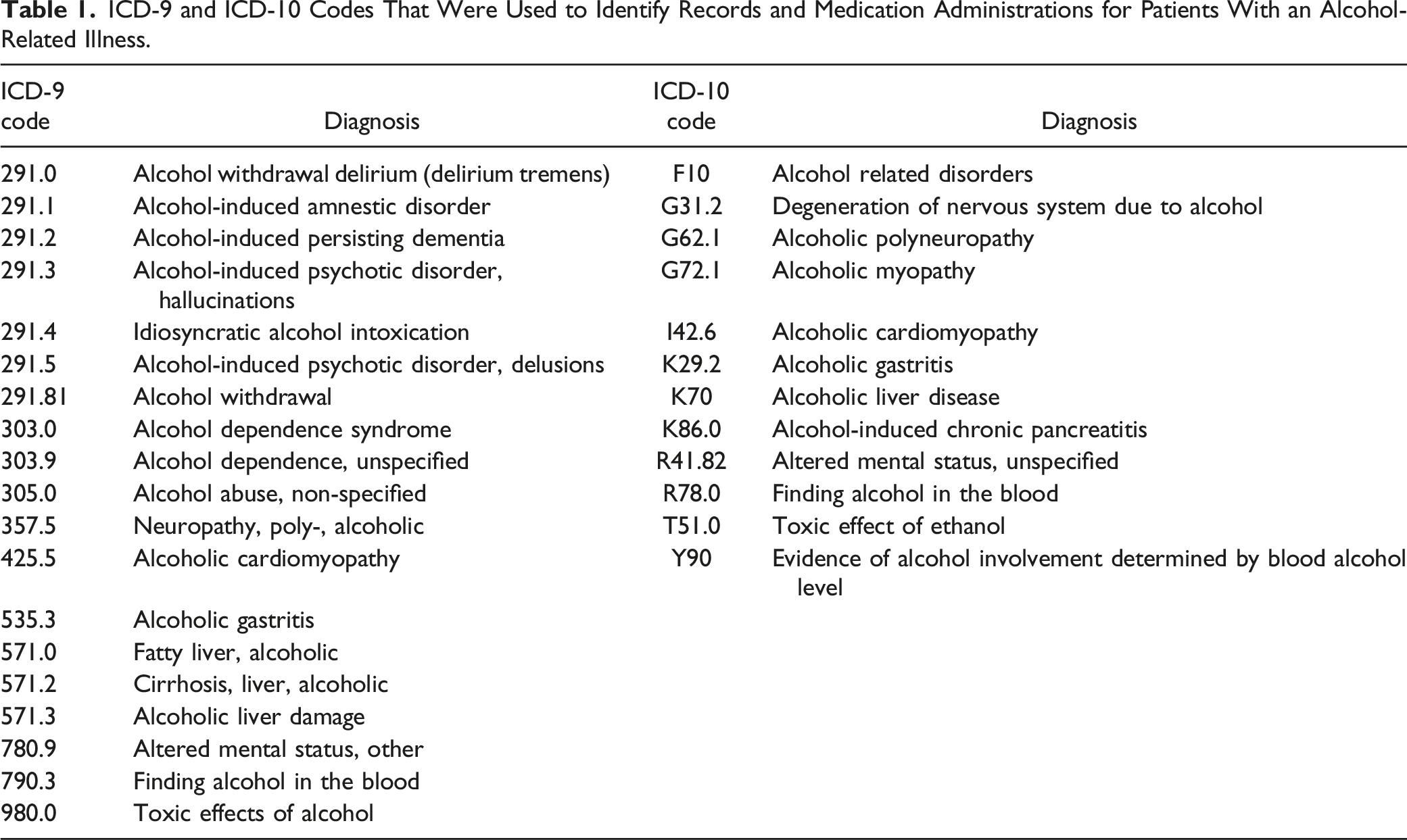
The primary outcome was the change in the monthly average of MVIs ordered inpatient within the first four months compared to the last four months of the study period. Secondary outcomes included the percentage of patients who received any form of thiamine in the ED, any form of thiamine in the inpatient setting, as well as intravenous MVIs in the ED. Enteral was defined as given orally or via gastrointestinal tube, while parenteral was defined as given intravenously or intramuscularly.
The historical ED intervention took place in June of 2009. When comparing monthly medication administration rates, we assessed the first four months following the 2009 ED intervention (June 2009 to September 2009) and the last four months of the study period (February 2019 to May 2019). This methodology was pre-specified prior to data abstraction. We chose these time periods to allow us to capture an average medication administration rate in both the first and last quarter of the study to then compare these values. We also assessed the specific administration setting, characterized as the ED or inpatient, where the medications (multivitamin or thiamine) were administered. An inpatient administration was defined as a medication given to a patient on a unit in the hospital, not including the ED and ambulatory care clinics. Patients assessed in the inpatient setting included only those who were admitted through the ED. We report the mean difference (MD) in binomial risk proportions and 95% confidence intervals (CI). All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
Results
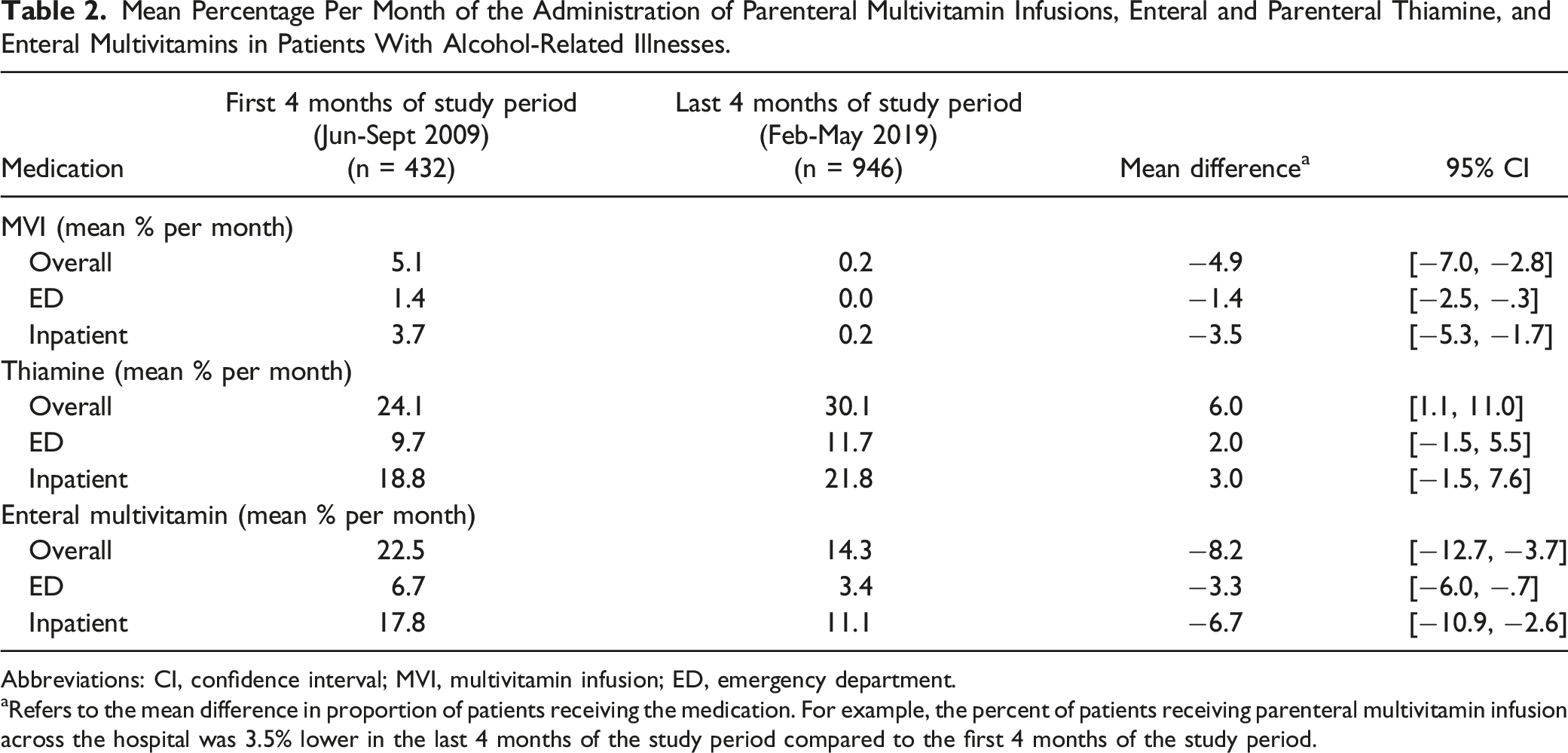
Throughout the study period, there was an average of 200 patients per month that presented to the ED with an alcohol-related illness, with 432 patients comprising the first 4 months and 946 patients included in the last 4 months of the study period. The trends in administrations by medication and by setting are presented in Figure 1. We found that average administrations of MVIs remained low over time in the ED as well as inpatient setting (Figure 1(A)). Overall, we found a 4.9% (95% CI −7.0, −2.8) decrease in the mean difference of MVI administrations in both the ED and inpatient combined from the first four months of the study period to the last four months of the study period. The mean average of MVIs ordered in the ED in the first four months was 1.4% with zero ordered in the last four months (MD −1.4%; 95% CI −2.5, −.3). MVIs were ordered inpatient on an average of 3.7% in the first four months as compared to .2% in the last four months (MD -3.5%; 95% CI −5.3, −1.7) (Table 2). There was also a significant decrease in enteral multivitamin use overall as shown in Figure 1(B) (MD −8.2%; 95% CI −12.7, −3.7), though this was largely due to a decrease in its utilization in the inpatient setting (MD −6.7%; 95% CI −10.9, −2.6) (Table 2). Enteral and parenteral thiamine administrations increased during the study period (Figure 1(C)). In the ED and inpatient combined, we observed a 6.0% (95% CI 1.1, 11.0) increase in thiamine administrations per month. Trends in administrations by medication (parenteral multivitamin infusion (A), enteral multivitamin (B), and thiamine (C)) and setting (emergency department and hospital). Mean Percentage Per Month of the Administration of Parenteral Multivitamin Infusions, Enteral and Parenteral Thiamine, and Enteral Multivitamins in Patients With Alcohol-Related Illnesses. Abbreviations: CI, confidence interval; MVI, multivitamin infusion; ED, emergency department. aRefers to the mean difference in proportion of patients receiving the medication. For example, the percent of patients receiving parenteral multivitamin infusion across the hospital was 3.5% lower in the last 4 months of the study period compared to the first 4 months of the study period.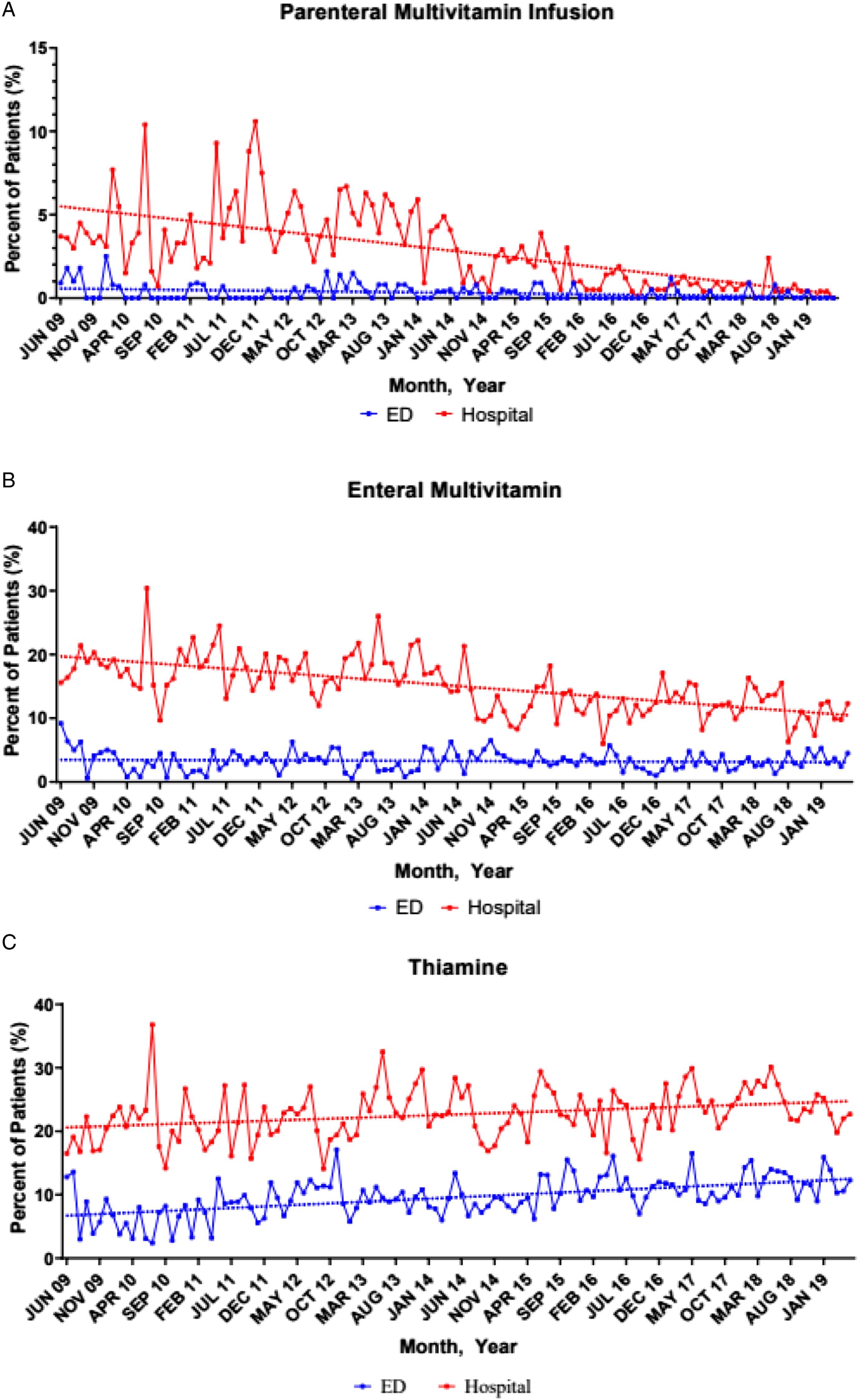
Discussion
Emergency practitioners are uniquely positioned to implement initiatives and affect change for the entire institution due to therapeutic momentum starting in the ED. The ED serves as an interface between the inpatient and community settings, and is the first place where patients present for emergency care. Early therapeutic decisions made in the ED have been shown to influence subsequent care for patients admitted to the hospital.9,10 Two studies specifically looked at the impact of antibiotic choices in the ED and found that greater than 80% of antibiotics initiated in the ED were ordered unchanged upon admission.9,10 For these reasons, an intervention made in the ED can have an exceptional influence on care throughout the entire institution.
Our findings confirm the continued impact of an ED intervention on vitamin prescribing practices for patients presenting to the ED with alcohol-related illnesses. Additionally, we found that the hospital-wide prescribing of MVIs decreased significantly and approached zero per month by the end of the study period, again suggesting that the ED is the most appropriate place to make an impactful intervention.
Regarding the importance of thiamine administrations, Wernicke-Korsakoff syndrome is an acute neuropsychiatric disorder resulting from thiamine deficiency, and is associated with significant morbidity and mortality. Due to the difficulty in distinguishing altered mental status from Wernicke-Korsakoff syndrome vs acute alcohol intoxication, it is often underdiagnosed and undertreated. 2 For this reason, it is still critical to administer empirical thiamine in patients with undifferentiated altered mental status related to acute or chronic alcohol intoxication.2,3 Therefore, the purpose of the 2009 ED intervention was not encouraging the omission of thiamine therapy, but to most importantly decrease MVI usage. Our study did in fact show that patients were still receiving thiamine given the increase in thiamine administrations from the beginning of our study period to the end in both the ED and inpatient cohort.
There are many opportunities to expand on this research that include evaluating the outcomes of patients in this study and see if a relationship exists with various vitamins therapies and routes of administration. We were unable to match medication therapies with specific diagnosis codes and follow up on patient outcomes; thus in the future, we would like to assess the appropriateness of thiamine doses and route of administration as it pertains to preventing and treating Wernicke-Korsakoff syndrome. Additionally, another study could be performed looking at the impact of an ED intervention on hospital-wide prescribing patterns at other institutions to determine the generalizability of our findings.
There were several limitations in our study. First, the nature of a retrospective study introduces the possibility of inaccurate reporting as our study heavily relied on the correct documentation of ICD-9 and ICD-10 codes. Inaccurate documentation may have led to either under- or overestimation of our outcomes. However, we selected data variables that are easily accessible from the EMR and were abstracted by a trained and blinded researcher. Our study was a single center study, which may limit its generalizability to other institutions. Additionally, there were no patient centered outcomes measured as that was not within the scope of our study, however this could be a potential area of expansion on this research as previously described. Finally, there may have been some external factors described below that potentially impacted the decline in the prescribing of MVIs at our institution. For example, there was literature published during the study period, such as a review article from 2016 suggesting the abandonment of MVI in ICU patients with chronic alcohol use disorder which could have influenced the prescribing patterns of providers at our institution. 11 Although there were no major fluctuations in MVI administrations at a single point in time, it is also possible that other specialties throughout the hospital recognized the lack of value of MVIs and changed their practice independently. However, to our knowledge, there were no other specific interventions or education provided to clinicians outside of the ED during our study period. Throughout our study, there was reeducation in the ED to the new emergency residents each year as well as continual education regarding evidence-based treatment for vitamin therapies in patients with alcohol-related illnesses provided by emergency pharmacists, which all could have potentially aided in the decrease of MVIs ordered overall. While we can’t rule out other causes for the decrease in inpatient MVI use, the steady decline in the rate of MVI use suggests that the intervention likely had an impact on overall MVI prescribing rates over time.
Conclusion
In conclusion, this study suggests that a historical ED intervention with a goal to decrease the administration of MVIs had sustained positive impact over a 10-year timeframe, and the therapeutic momentum associated with the intervention influenced hospital-wide prescribing patterns of vitamin therapies. This emphasizes the utility of and effect that an intervention in the ED can have on hospital-wide prescribing practices, suggesting that the ED is a suitable place to make an intervention yielding high impact and sustainability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.