
Abstract
Introduction
Transitions of care (TOC) are the points at which a patient moves to or returns from a physical location or contacts a healthcare professional for the purpose of receiving health care. 1 TOC can occur between home, acute care settings, long-term care settings, and/or within each of these systems. According to the National Coalition of Transitions of Care, there are seven elements involved in a safe transition: (1) medication management, (2) transition planning, (3) patient and family engagement and education, (4) information transfer, (5) follow-up care, (6) health care provider engagement, and (7) shared accountability across providers and organizations. 2 Pharmacists are engaged in all of these elements to differing degrees, depending on the care setting.
Due to age-related changes in physiology, disease burden, and complicated health care needs, older adults undergo frequent TOC between their residence and institutional health care settings. Unfortunately, the care during these transitions is often ineffective, leading to adverse events, higher hospital readmission rates, and increasing costs.3,4 The Centers for Medicare and Medicaid Services (CMS) formally recognized this issue and in October 2018, long-term care facilities began to receive financial incentives from CMS to reduce hospital readmissions. 5
It has been estimated that 25 to 80% of patients have at least one medication discrepancy at discharge from a healthcare facility. 6 A study by Sinvani and colleagues reviewed patient charts for medication discrepancies across three transitions of care; (1) hospital to discharge, (2) hospital to skilled nursing, and (3) skilled nursing to home or long-term care. 7 After reviewing 44 patients, they found that all of these patients experienced medication discrepancies. The average number of discrepancies per patient at each type of transition was similar, with 8.1, 7.2, and 7.6 medication discrepancies in areas 1, 2, and 3, respectively. While most discrepancies were determined to be intentional, an average of one discrepancy per patient at each level of transition was labeled as unintentional, with 86% of patients having at least one unintentional discrepancy.
One strategy to reduce medication errors is to provide effective medication reconciliation during care transitions. Those residing in long-term care facilities have a 27 to 57% risk of having at least one medication discrepancy found between their hospital discharge summary and their long-term care medication list. 4 In 2014, the Improving Medicare Post-Acute Care Transformation (IMPACT) Act was enacted to address several concerns in the long-term care setting by requiring the reporting of standardized patient assessment data to long-term care and home health agency providers with the goal of improving clinical outcomes. 8 One of the charges of the IMPACT Act was the requirement of conducting a medication reconciliation by a healthcare professional. 9 Pharmacists and pharmacy staff are well positioned to provide effective medication reconciliation due to their expertise in medication management. Research has shown that when pharmacists are involved in medication reconciliation, accuracy and efficiency is improved. 10 As such, the World Health Organization (WHO) along with several key international organizations have recommended that pharmacists be involved in medication reconciliation at these care transitions.4,8
Most of the literature regarding pharmacist involvement in TOC services is centered around transitions in and out of the hospital. 11 While the hospital is an important area for intervention, an additional area identified as having poor transitions of care with a need for effective TOC services is long-term care settings. For this review, long-term care settings will be termed patient care centers (PCC) and will include acute rehabilitation, residential care, care homes, skilled nursing, and assisted living facilities.
A 2012 systematic review analyzed medication reconciliation specifically during the transition to and from long-term care settings and found only seven studies to include in the analysis. 12 Although these studies showed improvements in process and measured outcomes, none were able to determine long-term clinical effectiveness of the interventions. Therefore, they identified a need for well-designed studies that use appropriate methods to assess the clinical effectiveness of medication reconciliation. In all seven studies included in this review, clinical pharmacists were identified as playing a key role in TOC services as the medication expert providing medication reconciliation. The objective of this review is to build upon the 2012 systematic review, expanding to all TOC interventions including the involvement of pharmacists, to determine which services are most effective when patients transition in and out of PCC.
Methods
A review of the literature was conducted to identify studies where a pharmacist was involved in an intervention to assist with the TOC for older adults in and out of PCC. The procedure and reporting of this scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 13
Articles Meeting Inclusion Criteria and Descriptions.

SD, standard deviation; IQR, interquartile range; PCC, patient care center; OR, odds ratio; RR, relative risk; CI, confidence interval; ADR, adverse drug reaction; IRR, incidence risk ratio; ED, emergency department; TOC, transitions of care.
aPCC included nursing home and community home care (defined as living in the community with assistance, similar to an assisted living facility).
Medication Discrepancies.
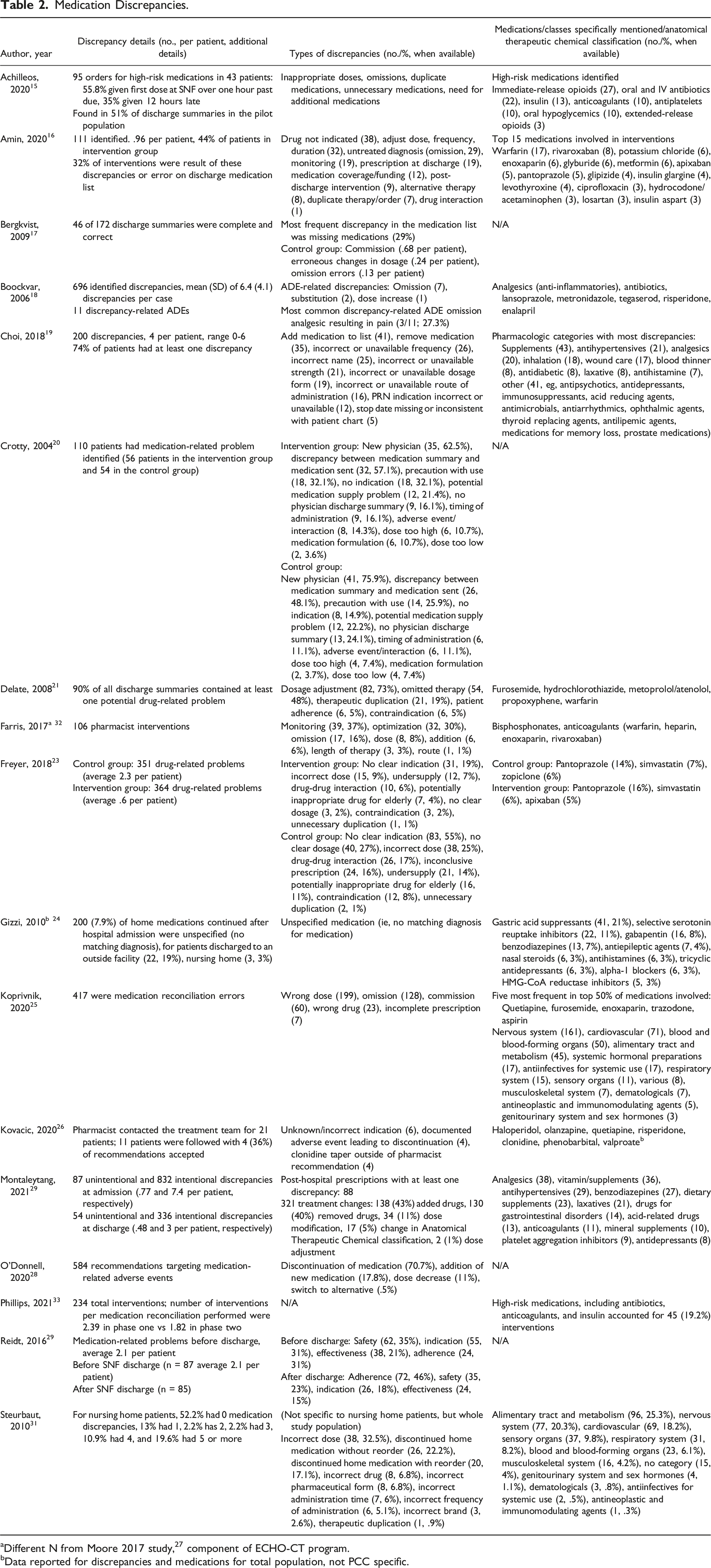
aDifferent N from Moore 2017 study, 27 component of ECHO-CT program.
bData reported for discrepancies and medications for total population, not PCC specific.
Two authors (S.S., E.P.) scanned the titles and abstracts of the search results as a “first pass” review and the full text articles of those meeting the inclusion criteria were acquired. Five reviewers (K.M., E.P., C.B., K.B., K.U.) examined the full text articles as a “second pass” for exclusion or inclusion. Any articles that were questionable for inclusion after the second pass were discussed with the entire group of authors and inclusion was determined through consensus.
All authors summarized the included articles for pertinent data from the studies including the setting, study population, trial design, intervention, outcomes, and major findings pertinent to the study’s evaluation. A second review of this data was conducted by multiple authors for consistency in terms of terminology and information included. The entire group of authors meet to discuss all areas requiring clarity.
Results
The search strategy resulted in 873 abstracts. After duplicates were removed, 676 abstracts and titles were reviewed in the initial first pass. An additional 59 abstracts from reference lists of systematic reviews were also evaluated, totaling 735 abstracts. The exclusion of articles in the first and subsequent passes are depicted in Figure 1. One hundred and twenty-six full-text articles were reviewed in the second pass with 104 being removed based on the exclusion criteria. The number of articles that met the inclusion criteria for this review totaled 22 (Table 1). Flow diagram of search results (separate attachment). Abbreviations: PCC, patient care centers; TOC, transitions of care; *other - educational initiatives (9), survey (6), descriptive articles (2), abstract only (1), editorial (1), report (1), article not available (1).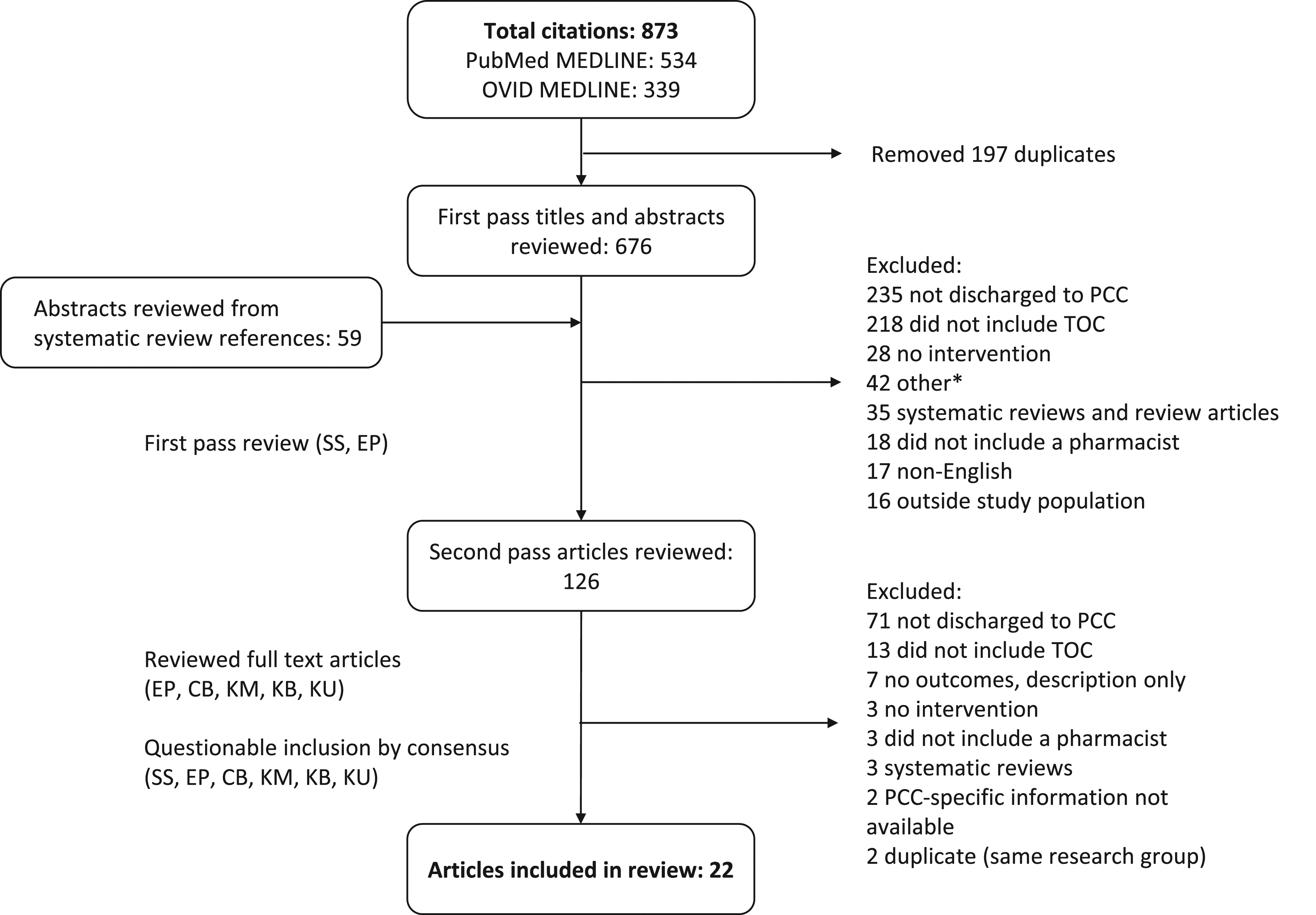
When summarizing the included articles, age, gender, and race were reported, if available. Total population demographics were included for subgroup analyses if that was all that was obtainable. Depending on availability, age was reported as mean or median, and gender and race were reported as percentages. For each study, the trial design, intervention, and outcomes were summarized with major findings reported.
Several themes were identified when reviewing the 22 included articles. Overall, these studies were limited in duration, sample size, and reported variable interventions. The majority of participants were female and White, with mean age greater than 70 years. The most common type of setting in which TOC was captured included from hospital to PCC15-19,21,23,27-33 or PCC to community,20,22,24,34 with a few studies looking at the transition from PCC to hospital25,36 or any location to PCC. 26 The sample size for most studies was less than 300 patients15,16,18-21,27,29,32-34,36 however two studies assessed several thousand transitions.26,35 Most of the studies were prospective in nature with an intervention and control group or a pre/post intervention design.15-19,22-24,28,30,32,34,35 There was one randomized, single-blind, controlled study 21 and one retrospective, economic analysis that provided cost savings data. 31 Another analyzed two different phases of a quality improvement project compared to a baseline where no intervention occurred. 33 A few trials included only descriptive outcomes such as number of medication discrepancies, medication errors, or number of patients counseled.20,25-27,29,36
In terms of interventions, most studies examined the addition of a pharmacist to the TOC service or having a pharmacist complete medication-related tasks to facilitate care transitions within PCC or the hospital.15,17-29,31-34,36 Several studies included multiple interventions, not limited to the pharmacist, making it difficult to determine the extent to which the pharmacist contributed to improved outcomes.16,30,35
Most studies reported a reduction in surrogate outcomes such as medication errors and/or discrepancies,15-21,24-26,28,33,34,36 mean time for medication order entry and/or administration,15,17,23,33 adverse drug events,19,21 and continuation of therapy after intervention.27,29 One economic analysis estimated an average cost savings of US$622 per patient when a long-term care pharmacist initiated medication reconciliation within 48 hours of admission to PCC 31 whereas another found that pharmacist inclusion in TOC reduced 30-day total healthcare costs. 30 A study that evaluated provider satisfaction found that staff and physicians were satisfied with pharmacists providing TOC services. 23
The most noteworthy outcomes reported were 30- and 60-day mortality, with one study showing no statistically significant reduction in 30-day mortality 30 and another showing a significant reduction in 60-day mortality. 22 Several of the studies showed statistically significant reductions in 30-day readmission rate15,30,32,34,35 and hospital usage, 21 while others found no significant reductions in hospital readmissions.16,17,22,32,33 The wide variability of study results is likely related to the heterogeneity in sample size, trial design, intervention, and how outcomes were measured.
A review of medication discrepancies, type of discrepancies, and medication classes involved in those discrepancies is described in Table 2. This data was extracted from studies where the information was readily available. The most common medication discrepancies included unnecessary medications or medication omissions, inappropriate dosing, duplicate therapy, or drug interactions. The most common medications involved in these discrepancies included antibiotics, analgesics, anticoagulants/antiplatelets, diabetic agents, antipsychotics, and proton pump inhibitors.
Discussion
This scoping review revealed that there continues to be a lack of randomized controlled trial data assessing the effectiveness of pharmacist interventions related to TOC to and from PCC. Most of the data surrounding TOC to and from PCC involves small sample sizes with only surrogate outcomes showing statistically significant improvements in the TOC process with pharmacist intervention.
This review occurred 11 years after the review by Chabbra et al and found sixteen additional studies that reviewed a TOC to and from PCC. 12 One study by Koehler et al. was included in the Chabbra systematic review but was excluded from this review due to the inability to subgroup the outcomes for the five patients in that study who were from PCC. 39 The Chabbra review included only two studies with clinical outcome results, including mortality 22 and hospital usage, 21 while scoping systematic review included eight additional studies that assessed mortality or hospital readmission data.15-17,30,32-35 Furthermore, this review identified two cost savings studies.30,31 Despite the additional outcome and cost savings data, large randomized controlled trials are still lacking, and evidence continues to be mixed about which interventions are the most efficacious and impactful.
Based on this review, pharmacists continue to be a valuable resource in identifying and mitigating medication errors and discrepancies. A systematic review of twenty studies by Redmond et al showed that medication reconciliation during TOC within multiple healthcare settings, not specific to PCC, reduced discrepancies, but the evidence to support this is weak. They concluded that the effect of medication reconciliation, in particular pharmacist-mediated, to reduce medication discrepancies is uncertain and further research is needed. 11
Mansah and colleagues reviewed the effectiveness of various strategies employed by the multidisciplinary team across TOC. They concluded that pharmacist-led interventions could reduce utilization of medical resources, improve the quality of medications prescribed by physicians, and reduce medication non-adherence. 40 These results are consistent with those of the current review, in that pharmacists can improve the quality of medication prescribing, and perhaps improve clinical outcomes.
While it is well established that pharmacists can play a role in TOC, their optimal role is unknown. Pharmacists can be involved in medication reconciliation upon admission or discharge, patient counseling, and/or clinical medication reviews. Ensing and colleagues found that isolated medication reconciliation is not adequate to reduce readmission rates. 41 Pharmacists need to collaborate with other healthcare professionals (ie, doctors and nurses), tailor interventions to individual patient needs, provide patient education, and perform a clinical medication review. This further supports the idea of team-based care and the importance of pharmacists working with other healthcare providers to improve outcomes. In order to improve access to pharmacists as part of an interprofessional team for patients involved in TOC to and from PCC, research focused on clinical outcomes, including reduction in readmission rates, mortality, and cost, from large randomized controlled trials evaluating pharmacist interventions is warranted.
There are numerous publications outlining pilot programs which aim to improve TOC services in PCC.42-47 These programs vary in how they are implemented, but they demonstrate several important ways pharmacists can function as a member of an interprofessional team in TOC: (1) development of an accurate medication list that can be easily understood by staff and patients 43 ; (2) including patient engagement and education42,45; and (3) providing timely bidirectional communication between providers within hospitals and nursing homes and patients.44,46,47 It is imperative that current models being explored publish outcomes-related results. With this review serving as a foundation, interprofessional teams including pharmacists can implement effective TOC services within PCC to improve health outcomes for older adults.
This scoping review has several strengths, including the review process with multiple authors performing data extraction and review. Additionally, data was captured in several ways, including database searches, reviewing reference lists, and contacting authors directly for subgroup data. Several limitations should also be noted. While multiple methods were utilized to gather studies, those that were not in the English language, indexed in PubMed or Ovid MEDLINE, and those in which authors were unable to subgroup the data were excluded, which could result in publication and selection bias. Furthermore, studies could have been missed if the title and/or abstract did not specifically mention pharmacists or describe transitions that involved PCC. The studies included had a variety of methodological approaches and heterogeneity of outcomes, so results could not be pooled and analyzed.
In conclusion, there are a limited number of studies reporting clinical outcome data for TOC services to and from PCC involving a pharmacist. Current literature is limited by sample size, methodological flaws, and mixed evidence related to effectiveness, but does suggest that pharmacists are pivotal in improving health outcomes and should be included in interprofessional teams within PCC. Large randomized controlled trials that include clinical outcomes data are needed to evaluate the effectiveness of TOC services performed by pharmacists in PCC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.