
Abstract
Keywords
Introduction
Drug-drug interactions (DDIs) are type of adverse drug events (ADEs) that occur when one drug’s effect is influenced by another. Commonly it ends up with an alteration in drug efficacy or toxicity. 1 DDIs have the potential to harm patients severely. 2 Potential drug-drug interaction “is the possibility of one drug to interact with another when they are administered together”. 3
The majority of sudden cardiac deaths are attributed to an abnormal lengthening of the QT interval. 4 QT prolongation has the propensity to precipitate an erratic type of polymorphic ventricular arrhythmia, Torsades de Pointes (TdP). QTc measurements below 470 ms and 480 ms are considered normal for adult males and females respectively. 5 When the QTc interval is ≥500 ms, then there is an increased risk of TdP development in patients. 6 The use of certain drugs is expected to be a significant risk factor for QT prolongation. The effect of a QT-prolonging drug might be worsened in the presence of additional risk factors such as electrolyte abnormalities and other comorbidities, putting patients at a higher risk of a prolonged QT interval. 7
At least >280 drugs comprising various psychotropics, antidepressants, antihistamines, proton pump inhibitors and antimicrobials which can precipitate TdP based upon reliable evidence are accessible at AZCERT. 8 The impact of psychotropics on cardiac repolarization is gaining popularity. Because many antipsychotic and antidepressant drugs are linked to QT-prolongation, psychiatric patients can be regarded as a population at risk for drug-induced TdP. Phenothiazines have the propensity to cause arrhythmia thereby predisposing to TdP more than other psychotropic drugs. 9 Haloperidol has an escalated risk of QTc-prolongation when given intravenously. 9 Atypical antipsychotics are also associated with QTc- prolongation but carry lesser risk when compared to typical ones. Shreds of evidence show that clozapine extends the QTc- interval in dose-dependent manner 10 whereas Ziprasidone prolongs the QTc-interval in dose-independent manner. 9 Drugs to treat depression like Citalopram, Escitalopram and Sertraline are found to increase QTc significantly. 11 Citalopram has been associated with plentiful episodes of TdP leading to the imposition of dosage limits by the FDA. 12
Evidence shows that concomitant use of multiple QT prolonging drugs, or other drugs which can modify the metabolism of a QT-prolonging drug can result in harmful DDIs, as reported in studies involving cisapride and terfenadine. 13 The combination of medications and patient-specific characteristics should be taken into account to provide a more precise estimation of the risk of QT prolongation and TdP. 9 The risk factors which are specific to patients include sex, age, cardiac diseases, dyselectrolytemia, and use of diuretics and antiarrhythmics. 14 Psychotropic medication combinations can have cumulative effects on the QT interval.
Only a few studies have explored the frequency of usage of QT-prolonging drugs and the occurrence of QT-prolonging Drug-Drug interactions (QT-DDIs) in psychiatric patients. Hence, this study attempted to review and quantitatively estimate the pooled prevalence of QT-DDIs and associated risk factors in psychiatric patients.
Methodology
Study Protocol
The MOOSE (Meta-analysis of Observational Studies in Epidemiology) statement was followed in conducting this systematic review and meta-analysis. 15 The review protocol is registered on PROSPERO with reference ID number: CRD42021290855.
Search Question
We employed the PICO elements (P: psychiatric patients; I: QT-prolonging Drug-Drug Interactions (QT-DDIs); C: not applied; O: potential QT- DDIs) to develop the following research question to clarify our hypothesis, eligibility criteria, and search technique: The aim of this review is to find out the prevalence of potential QT-DDIs in psychiatric patients
Screening and Eligibility of Studies
SK conceptualized the study. The titles and abstracts of the articles were examined based on the inclusion and exclusion criteria by two authors, SK and SM. They also gathered the entire text, examined the studies’ eligibility for final inclusion, assessed the quality of the study, and analyzed the data. AM commented on the review and meta-analysis.
Inclusion and Exclusion Criteria
Inclusion criteria - Observational studies addressing the prevalence of QT-prolonging DDIS (Prospective, retrospective and cross-sectional studies) - All male and female patients of any age who are attending psychiatric outpatient department and/or getting hospitalized in the psychiatric ward. - All published papers without a time limit - Studies that were published in English and provided enough information for the review
Exclusion criteria - Articles with missing outcomes - Articles not published in peer-reviewed journal
Data Source and Search Strategy
We searched credible databases such as PubMed/MEDLINE, Science Direct, Google Scholar and Research gate for English Language publications. The focus of the literature search was to uncover findings which were related to the prevalence of potential QT-prolonging drug-drug interactions in psychiatric patients.
Without specifying a time limit, the search was performed using carefully chosen search words. “Prevalence”, “QT-prolongation”, “DDIs”, “associated factors” and “psychiatry” were the search terms used in this review and meta-analysis. AND/OR words were used for the identification of the articles. The specific search strategy used in PubMed was (“long qt syndrome” [MeSH Terms] OR (“long" [All Fields] AND “qt” [All Fields] AND “syndrome” [All Fields]) OR “long qt syndrome” [All Fields] OR (“qt” [All Fields] AND “prolongation” [All Fields]) OR “qt prolongation” [All Fields]) AND (“psychiatrie” [All Fields] OR “psychiatries” [All Fields] OR “psychiatry” [MeSH Terms] OR “psychiatry” [All Fields] OR “psychiatry s” [All Fields]) AND (“drug interactions” [MeSH Terms] OR (“drug” [All Fields] AND “interactions” [All Fields]) OR “drug interactions” [All Fields] OR (“drug” [All Fields] AND “interaction” [All Fields]) OR “drug interaction” [All Fields]) AND (“epidemiology" [MeSH Subheading] OR “epidemiology” [All Fields] OR “prevalence” [All Fields] OR “prevalence” [MeSH Terms] OR “prevalance” [All Fields] OR “prevalences” [All Fields] OR “prevalence s” [All Fields] OR “prevalent” [All Fields] OR “prevalently” [All Fields] OR “prevalents” [All Fields]). The studies which were published till September 2021 were taken into account.
Data Extraction
The investigators created a standardized data extraction form in Microsoft Excel. The vital information related to study characteristics like the author, year of publication, study design and setting, target population, interaction checking software, Number of patients, Number of patients with QT-DDIs and list of classes of drugs which caused the interactions were extracted. Furthermore, the outcome of interest (Prevalence of QT-prolonging DDI (%) and associated factors of QT-DDIs) was also extracted.
Based on the abstract, inclusion, and exclusion criteria, five studies were chosen. Studies published in the English language were identified and screened using a mixture of search engines.
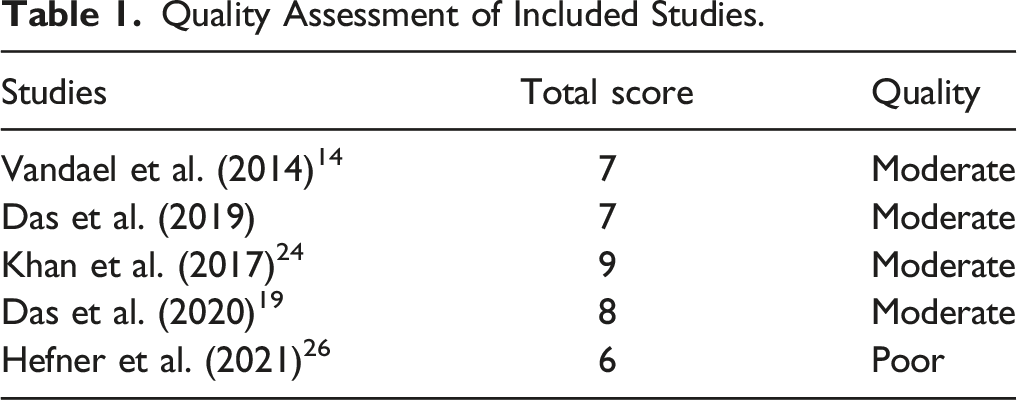
Quality Assessment
Quality Assessment of Included Studies.
Outcome Measurements
The outcome measure in this review and meta-analysis is the prevalence of potential QT-prolonging drug-drug interactions (QT-DDIs). Its primary goal was to evaluate the pooled estimates of potential QT-DDIs in psychiatric patients. The secondary outcome was to find out the associated factors for QT-DDIs.
Data Processing and Statistical Analysis
The pooled estimate of outcome measure ie, the prevalence of QT-DDIs was done by meta package R software. The presence of publication bias was evaluated by using egger’s regression test. In this review, the random-effects model was used by considering clinical heterogeneity among studies. Clinical heterogeneity was assessed using I2 statistics.
Results
Article Search Results
A total of 99 articles were identified through search strategy. After removing the duplication, 54 articles have remained for screening. From these, 47 articles were excluded by their title and abstract. The remaining seven articles were then evaluated as per prespecified inclusion criteria. Two articles were excluded due to insufficient information and missing outcome. Finally, a total of five articles were included for final review and analysis (Figure 1). Flow diagram for selection of studies.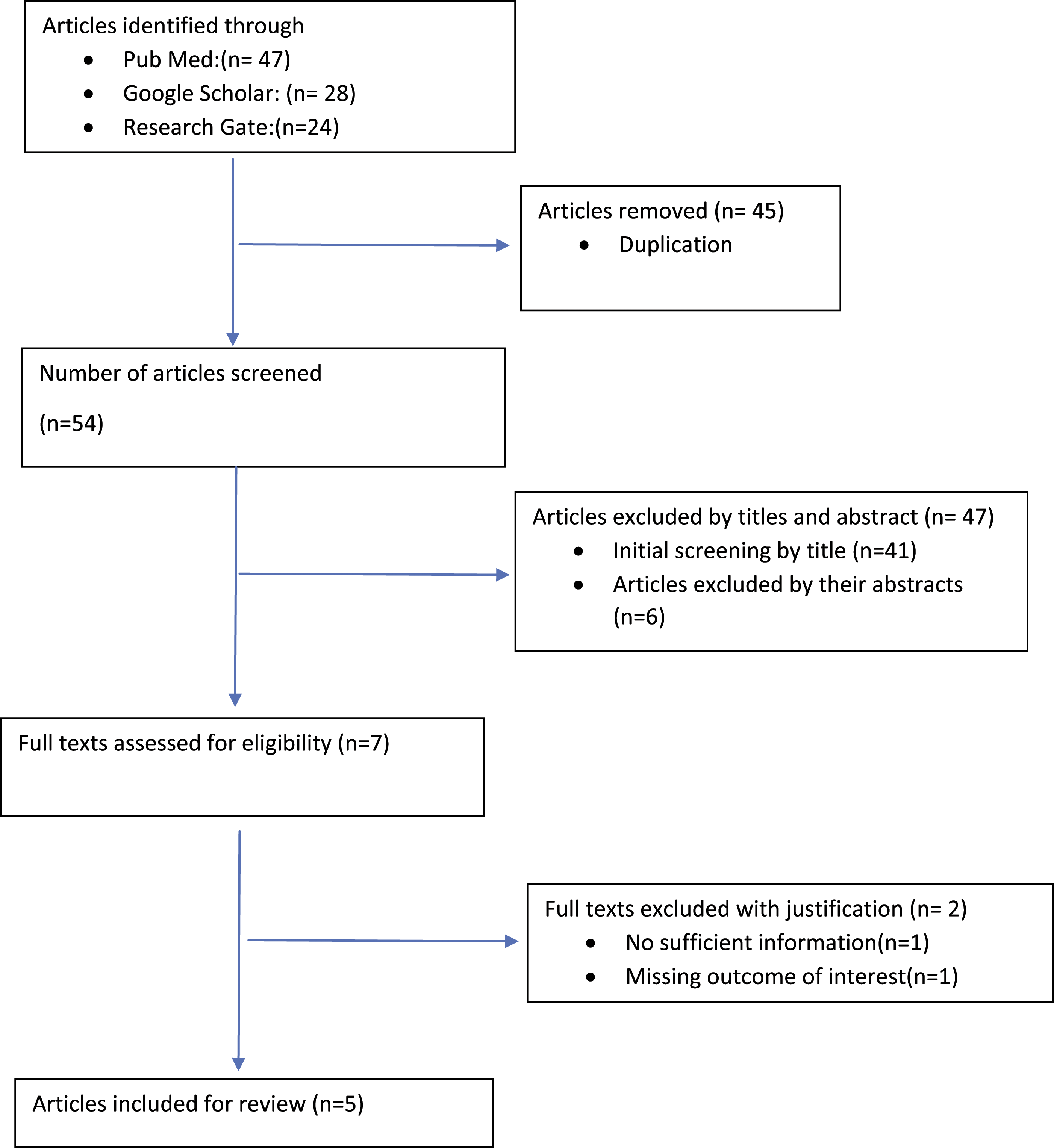
General Characteristics of the Included Studies
General Characteristics of Studies Included for Systematic Review and Meta-Analysis.
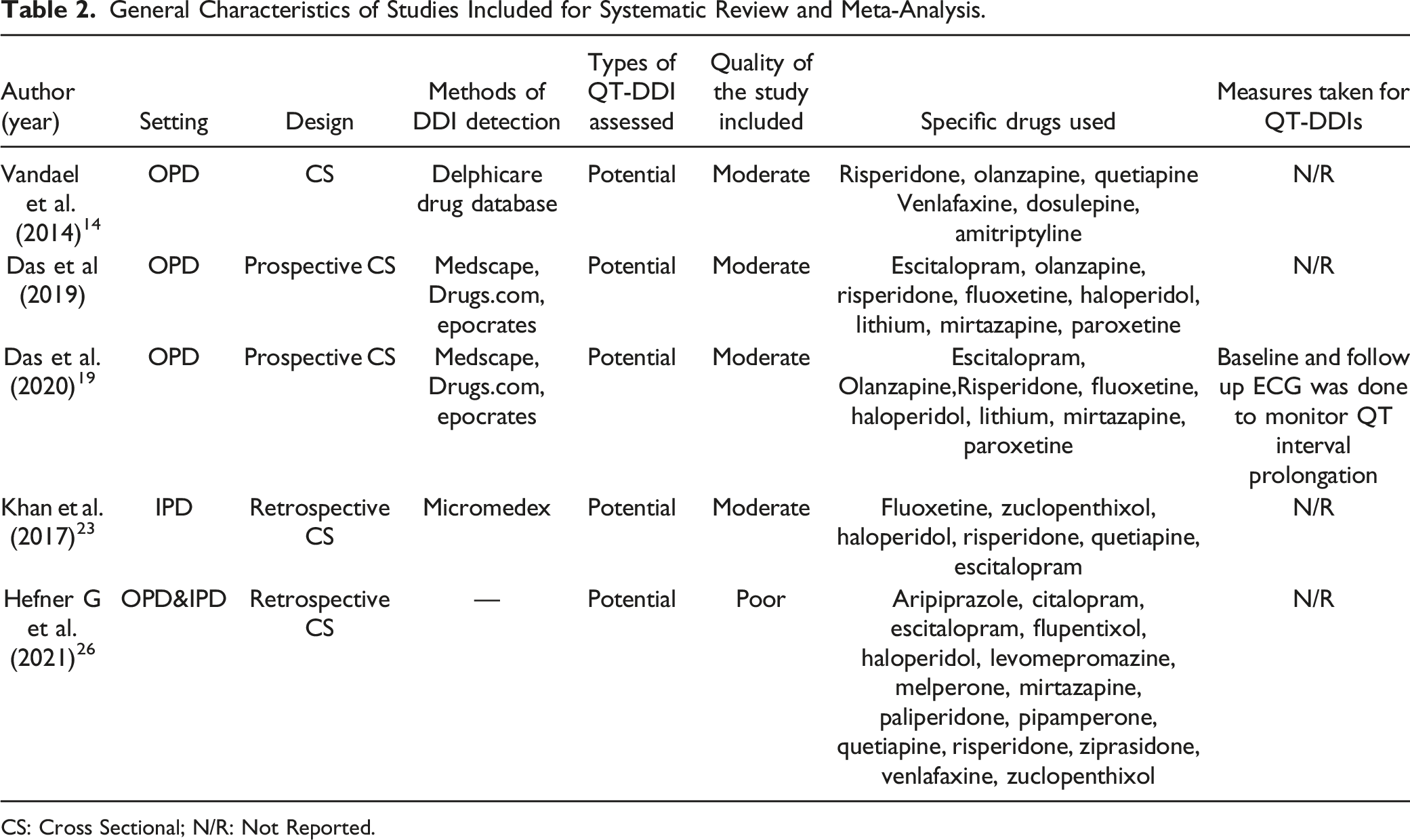
CS: Cross Sectional; N/R: Not Reported.
Three articles study QT-DDIs in the outpatient psychiatry department. One article included inpatients and one article included both inpatients and outpatients in psychiatry. Among the five studies included in this review, five different databases were used to detect potential DDIs.
Study Outcome Measures
Prevalence of Potential QT-DDIs
Studies of the Prevalence of QT-DDIs in Included Article.
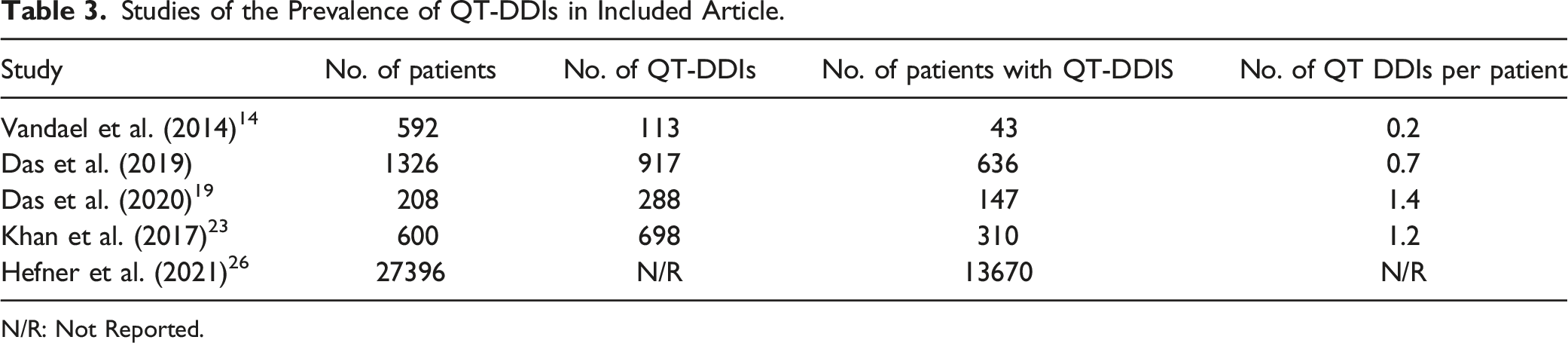
N/R: Not Reported.
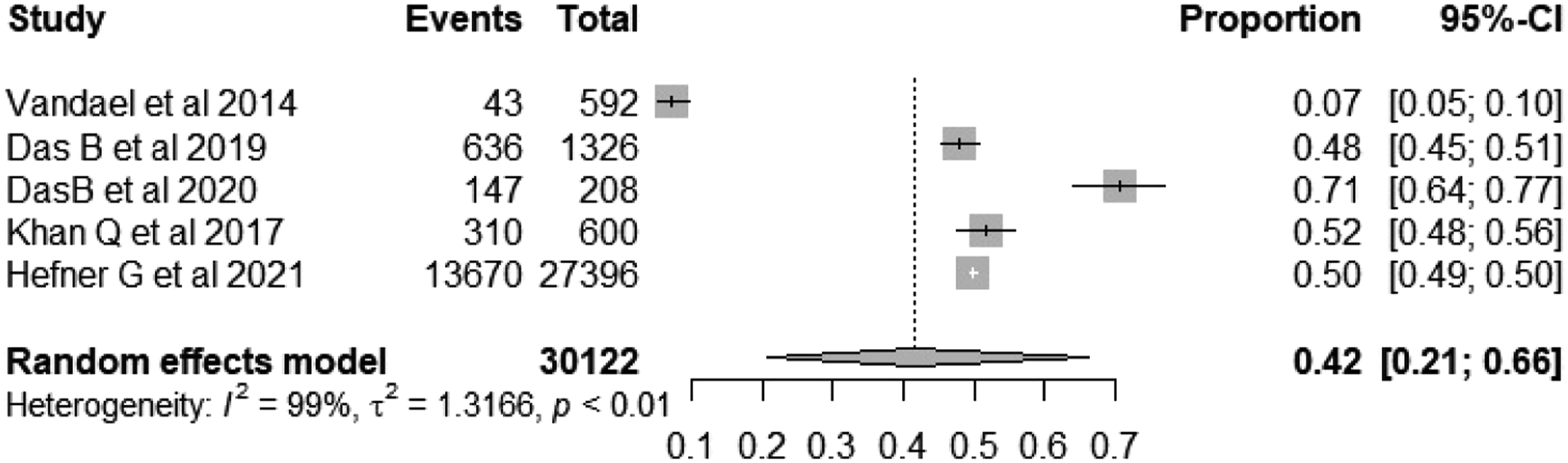
Forest plot depicting the pooled prevalence of QT-DDIs in psychiatric patients.
Subgroup Analysis
Subgroup analysis was done and it showed that the occurrence of QT-prolonging DDIs were independent of gender (Supplementary Appendix S1).
Factors Associated With Potential QT-DDIs
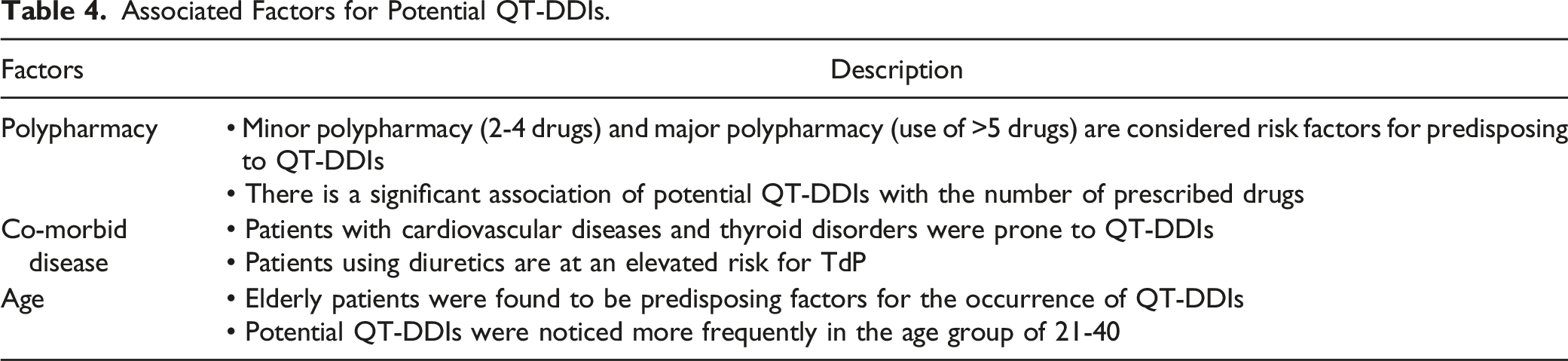
Associated Factors for Potential QT-DDIs.
Publication Bias
Egger’s regression test confirmed that there is no evidence of publication bias in studies reporting the prevalence of potential QT-DDIs in psychiatric patients (Estimate: −3.314(SE = 5.53), P = .5912)
Discussion
This systematic review and meta-analysis aimed to analyse and summarize the prevalence of potential QT-DDIs and associated factors in psychiatric patients. A total of 30122 patients were included for the pooled estimation of the primary outcome. The overall prevalence of QT-DDIs in psychiatric patients in our study was found to be 42% (95% CI: 21.66%).
Haueis P et al. 17 evaluated drug interactions in a large sample of psychiatric patients and found that 79% of the patients were exposed to drug interactions which are higher than our study. A retrospective analysis conducted by Curtis LH et al. 18 in a cohort of outpatients reported that 2.2% of patients were exposed to QT-DDIs which is lesser than compared our study. The different classification systems that were utilised could explain these disparities. The lack of uniformity in the classification and information offered by various drug interaction sources can lead to confusion among health care professionals about how to address interactions, a topic that has been highlighted in multiple studies.
Only 1 study has reported the prevalence of QT-DDIs that resulted in patient harm. 19 In that study, out of 208 elderly psychiatric patients, 78 patients were advised ECG by the treating psychiatrist. Fifteen subjects were found to have clinically significant QT-prolongation evidenced by the ECG findings. One elderly female developed TdP and failed to survive. In this study, 70.7% of patients experienced a potential QT-DDI, with only 7% experiencing QT-DDI relating harm. The substantial disparity between these prevalence rates shows that potential QT-DDIs are poor predictors of QT-DDIs that can cause actual harm in a patient, and decisions to enforce strategies to combat QT-DDIs should not be made based only on potential QT-DDIs. 20
In this review and meta-analysis, age, polypharmacy and comorbidity were significantly associated with the occurrence of potential QT-DDIs in psychiatry patients. A meta-analysis by Ayenew et al. 21 concluded that age, polypharmacy and comorbid disease were significantly associated with the occurrence of potential DDIs in hospitals which is consistent with our study findings. Sudden Cardiac Death (SCD) has become a serious clinical concern when giving psychotropics to older people. When comparing patients over 65 who are receiving first and second-generation antipsychotics (FGA and SGA) to people on placebo, there is nearly a 2-fold increase in inpatient death rates. 22 In our review, 2 studies reported that young adults were exposed to potential QT-DDIs.19,23 The number of younger adult patients obtaining psychiatric care was higher in some studies from developing nations.24,25 Childhood exposure to household and social stress can lead to psychiatric disease in maturity.
Polypharmacy elevates the risk for potential QT-DDIs supported by different studies.19,23 Prescribing combinations of various antipsychotics and antidepressants concomitantly can elevate the risk for QT-DDIs in patients. The intake of multiple QT-prolonging medications can heighten the risk of cardiac arrhythmia because of increased cumulative drug dosage.19,26 In a study by Nose et al., 27 , polypharmacy involving antipsychotics was found to be positively associated with QT prolongation and also Beach et al. 28 reported that combinations of QT-prolonging drugs increase the risk of QT prolongation. Clinicians should undertake a careful analysis of QT risk factors when prescribing psychotropics.
The presence of comorbid diseases exposes psychiatric patients to potential QT-DDIs. Patients with cardiovascular diseases and thyroid disorders were prone to QT-DDIs in psychiatry. 19 The reason might be, that the drugs used for the management of the comorbid disease are often used concomitantly leading to the possibility of the occurrence of potential QT-DDIs. The other risk factors which predispose to TdP include electrolyte abnormalities and the use of diuretics.19,29 Long-term use of proton pump inhibitors leads to serious complications of hypomagnesemia, which can cause QT prolongation and fatal ventricular arrhythmia. 30 Similarly, the use of 5HT-3 antagonists like ondansetron which is commonly used as an antiemetic can prolong QT interval and it also induces hypokalaemia. Hypokalaemia is a modifiable risk factor for drug-induced TdP. 31
Before initiating a drug, which can prolong QT-interval, the physician should consider patient factors, the risk posed by that specific drug and the impact of adjuvant drugs that which patient was already taking for comorbid diseases. The clinician should also consider the availability of alternate solutions that could reduce the risk of QT prolongation without compromising safety and efficacy. Physicians are advised to record baseline ECG and repeat ECG after treatment when drug levels are at a steady state (4 to 5 half-lives). If there is any significant change in ECG, the prescriber can check electrolytes and correct any abnormality; if QTc prolongation is not resolved, reduction of dosage or withdrawal of the drug can be considered. 32
Only one study analyzed the actual harm due to QT-DDIs in patients whereas other studies reported only the potential QT-DDIs, this is the first limitation. The discrepancy in the sample size between the studies could have led to bias. The other limitation was clinical heterogeneity among included studies, so it should be considered with caution.
Conclusion
The prevalence of potential QT-DDIs was found to be in 42% of psychiatric patients who were treated. The associated risk factors were found to be old age, polypharmacy and comorbid diseases. There is a need to adopt precautionary safety interventions, to be alert and forestall QT prolongation in the clinical setting. To avoid significant consequences, selecting the right drugs is critical.
Supplemental Material
Supplemental Material - Prevalence of QT-Prolonging Drug-Drug Interactions in Psychiatry: A Systematic Review and Meta Analysis
Supplemental Material for Prevalence of QT-Prolonging Drug-Drug Interactions in Psychiatry: A Systematic Review and Meta Analysis by Saravana Kumar Ramasubbu, Archana Mishra, and Soumitra Mandal in Journal of Pharmacy Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.