
Abstract
Introduction
Cancer is the second leading cause of mortality worldwide1,2 and the burden of cancer is increasing globally, as a result of varied at-risk behaviours and the growth of an aging population. 3 According to the Canadian Cancer Statistics 4 one in two Canadians will be diagnosed with cancer in their lifetime. The risk of cancer increases with age, where 90% of newly diagnosed cases will consists of Canadians over the age of 50 years. 4
The prevalence of multimorbidity, defined as the co-occurrence of two or more chronic health conditions, it is very common among older persons, 5 and is increasing among younger adults.6,7 Cancer is also considered a chronic disease that is prevalent in the elderly, and therefore multimorbidity among persons with cancer is common. 8 A challenge related to multimorbidity is polypharmacy, as each co-occurring condition may require different therapeutic approaches.
Polypharmacy has various definitions, it is defined by numerical groupings with associated terms such as hyper polypharmacy or excessive polypharmacy,9-12 or by a descriptive definition such as appropriate or inappropriate polypharmacy.11,13 In the literature the most common definition is the use of five or more drugs.10,11,14 Polypharmacy may be a consequence of both cancer 15 and multimorbidity. 16 Not surprisingly, persons with cancer and multimorbidity have an increased number of medications prescribed. 11 For example, a more advance cancer disease is linked to an even higher number of medications. 17
Other factors associated with polypharmacy include age and sex.18,19 In Canada approximately one-quarter of elderly people are prescribed 10 or more medications over a year. 20 Being female is also a risk factor for polypharmacy, as is the combination of being female and age 85 years and older.21,22
Pharmacotherapy plays an integral role in cancer treatment. However, the risk of adverse drug events increases as a result of increased number of prescribed medications. 21 The added adverse events incurred by polypharmacy can lead to higher health service utilization, such as emergency room visits and hospitalizations, and death, especially in the elderly.16,23-25
The prevalence of polypharmacy and the associated negative health outcomes among older adults with cancer and multimorbidity has been extensively discussed in the literature, however the prevalence and impact of polypharmacy among young adults with cancer and other chronic diseases are not adequately represented in the literature. Thus, this study examines whether the prevalence of polypharmacy differs by age, sex, level of multimorbidity and type and stage of cancer among both young and older adults. In addition, it assesses the relationship between polypharmacy and health service utilization (ie, emergency room visits and hospitalizations) in the year following cancer diagnosis.
Ethical Approval
Ethics approval was obtained from Lakehead University Research Ethics Board and the Institute for Clinical Evaluative Services (ICES), who provided access to the data.
Method
Study Design and Population
This study used a retrospective longitudinal design linking health administrative databases. This study included Ontarians 18 years and older with a valid Ontario Health Insurance Plan (OHIP) card, diagnosed with cancer between April 1, 2010 and March 31, 2013 (they may have been diagnosed with one of the selected chronic conditions prior to the cancer diagnosis). Our study population consists of persons with and without Ontario Drug Benefit (ODB) program coverage for the entire follow-up period (one year post-diagnosis). ODB program recipients include all Ontarians 65 years or older. Ontarians who are under the age of 65 will qualify for the ODB program if they are residents of long-term care facilities or homes for special care, persons receiving services under the Home Care Program, Trillium Drug Program recipients, persons receiving special assistance (eg, Ontario Works, Ontario Disability Support Program), and persons who are eligible for the Special Drugs Program (SDP), regardless of age. It was only as of January 1, 2018, that all persons 24 years and younger who were not covered by a private insurance plan also qualified for the ODB program. 26 Different data sources were used, and eligibility for each program (eg, Ontario Drug Benefit Program) is defined by provincial rules regarding health coverage. All individuals covered by OHIP are eligible for physician, primary care, hospital and emergency services, and thus are included in OHIP physicians’ claims, Discharge Abstract Database (DAD), and National Ambulatory Care Reporting System (NACRS). People over 65 as well as a portion of those <65 (as described above) are eligible for medication coverage and included in ODB. Persons who died within one year of their cancer diagnosis were excluded from the study. These persons may have had more severe disease or complications of their chronic diseases and cancer and were excluded to avoid bias and to minimize reverse causality.27,28
Follow-up data was used to assess service utilization within one year after diagnosis.
Data Sources
Institute for Clinical Evaluative Services Databases That Provided Data for the Study.
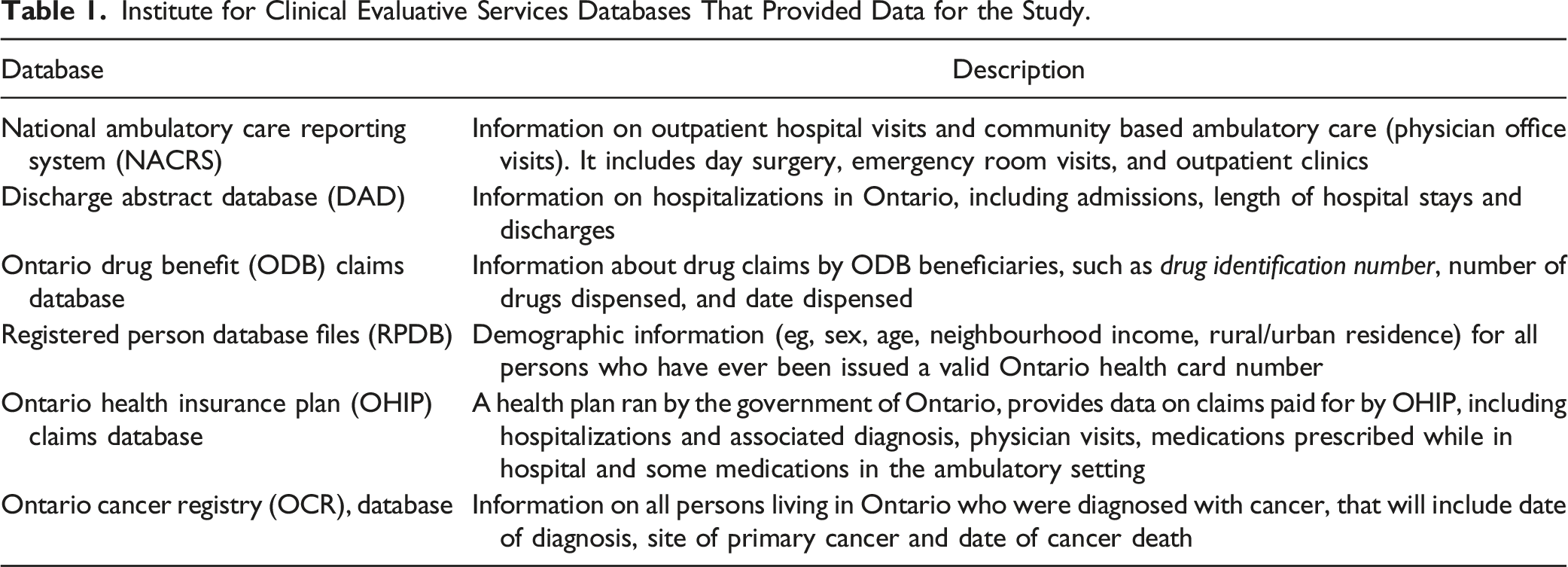
Approaches to identifying similar study cohorts and chronic conditions from provincial datasets are presented in previous studies.30,31 The list of ICD codes used to identify these chronic conditions is provided in Supplementary Appendix A.
Variables
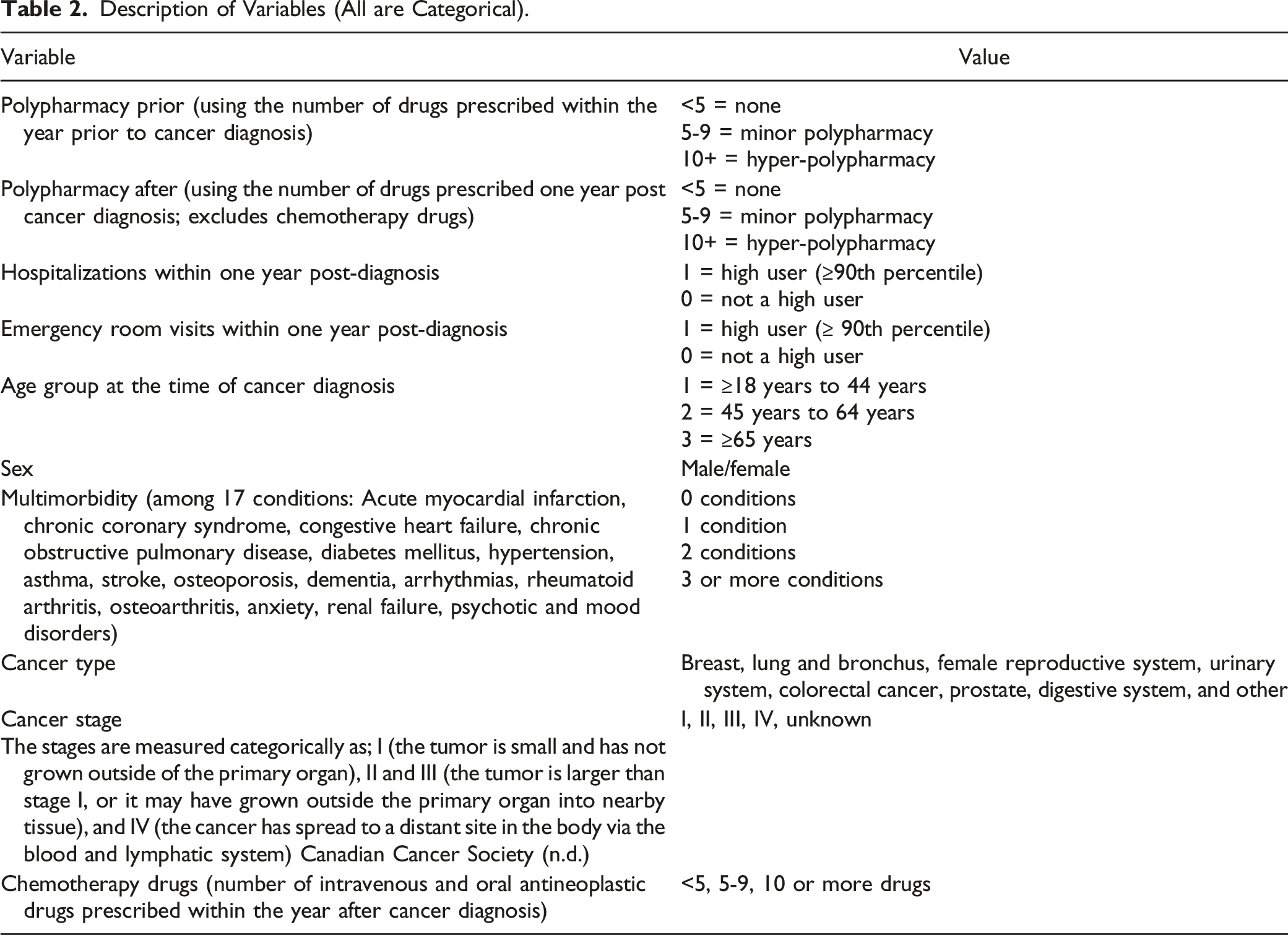
Description of Variables (All are Categorical).
Data Analysis
Descriptive statistics (%, mean, SD) characterize the study population for all considered variables. Bivariate analysis (i.e., chi-square test) was used to determine if polypharmacy (pre and post cancer diagnosis) differs by age, sex, multimorbidity, type of cancer, and stage of cancer. Stratified crosstables and chi-square tests inform on the interactions between multimorbidity level, sex, age, and polypharmacy post cancer diagnosis, while a multivariate model was created adjusting for type and stage of cancer. Next, multivariate logistic regression was used to quantify the adjusted relationship between polypharmacy and health service utilization. All data analyses were performed using Stata version 16.1. 33 Due to large population sample size, level of significance was fixed at P < .0001.
Results
Study Population Characteristics
Study Population Characteristics (Adults ≥18 Years Who are Eligible for Drug Coverage).
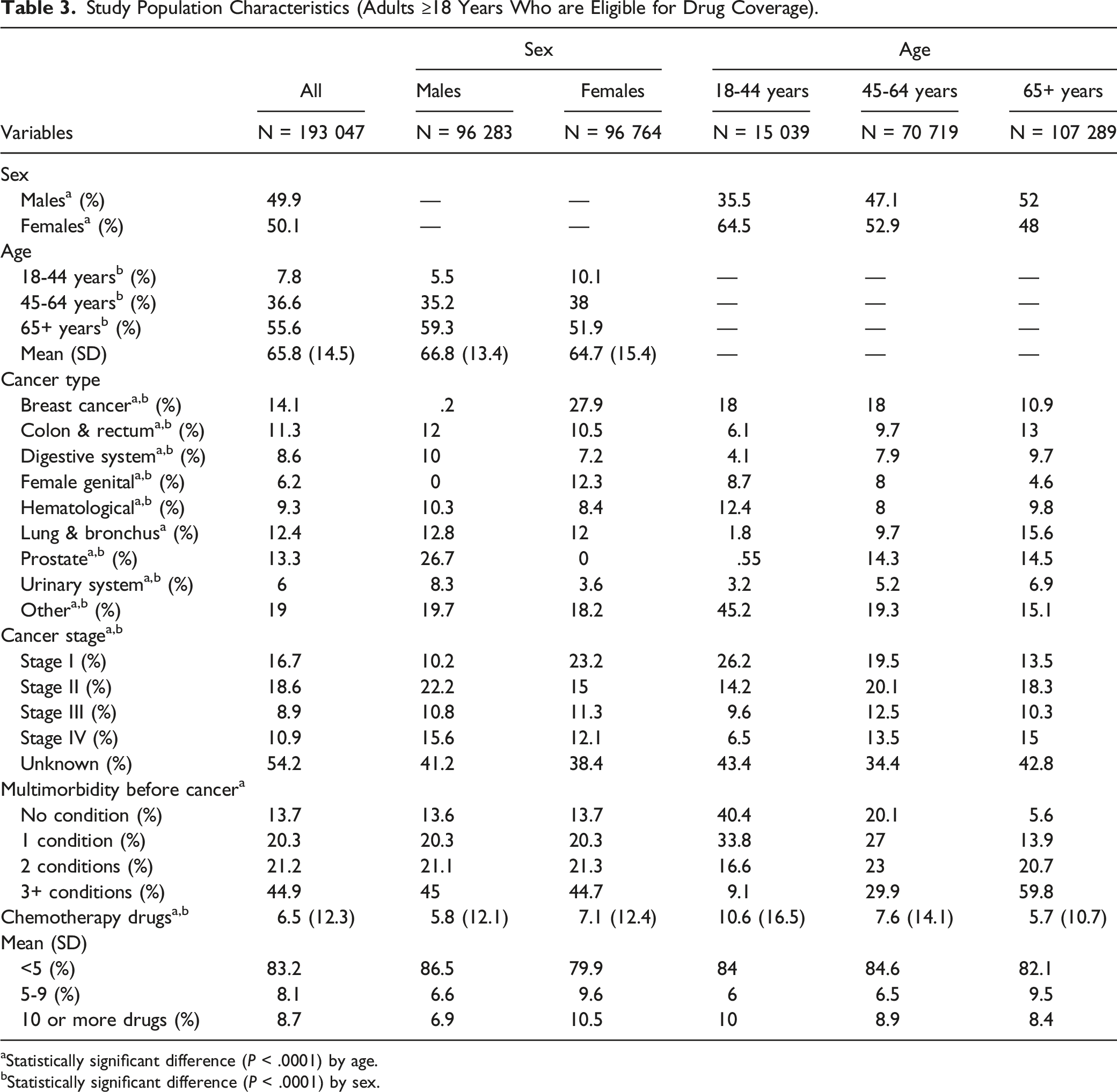
aStatistically significant difference (P < .0001) by age.
bStatistically significant difference (P < .0001) by sex.
Polypharmacy
Prevalence of Polypharmacy Within One Year Prior and Within One Year Post Cancer Diagnosis Overall and by Age, Sex, Multimorbidity, Cancer Type, and Cancer Stage.
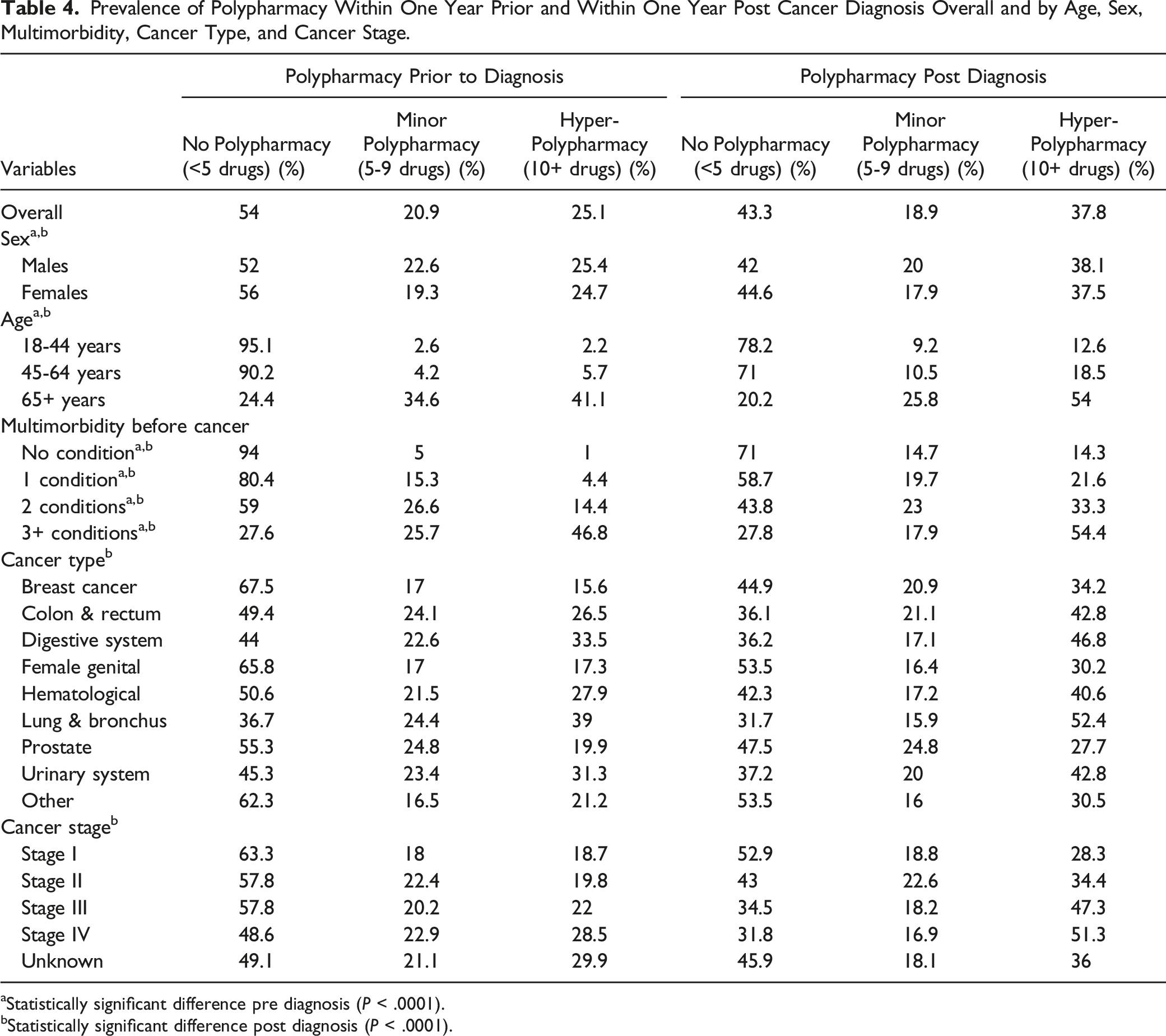
aStatistically significant difference pre diagnosis (P < .0001).
bStatistically significant difference post diagnosis (P < .0001).
Polypharmacy status post cancer diagnosis differed significantly by type of cancer (P < .0001). There was a large difference in the proportion of persons with no polypharmacy between types of cancer; in persons with lung & bronchus, only 31.7% were not on polypharmacy but there were 53.5% for female genital cancer, a very large difference between types of cancer. The proportion of persons taking fewer than five medications steadily decreased with increasing stages of cancer, while hyper-polypharmacy steadily increased (P < .0001).
Interaction Between Multimorbidity, Sex, Age, and Polypharmacy Post Cancer Diagnosis
As shown on Figure 1, the association of polypharmacy post cancer diagnosis with sex and age was significant for each level of multimorbidity. The combination of old age and highest level of multimorbidity contributes to the highest prevalence of hyper-polypharmacy, regardless of sex, though in the older age group, the prevalence of hyper-polypharmacy remains higher for females across all levels of multimorbidity. The lowest prevalence of hyper-polypharmacy is seen in the youngest age group across levels of multimorbidity. However, the relationship with sex is less straightforward. Specifically, it appears that hyper-polypharmacy is lowest among females with no or two conditions, and among males with either one or three or more conditions. Prevalence of Polypharmacy, by Multimorbidity Level, Age and Sex Among Patients Diagnosed With Cancer, Ontario. *P < .0001.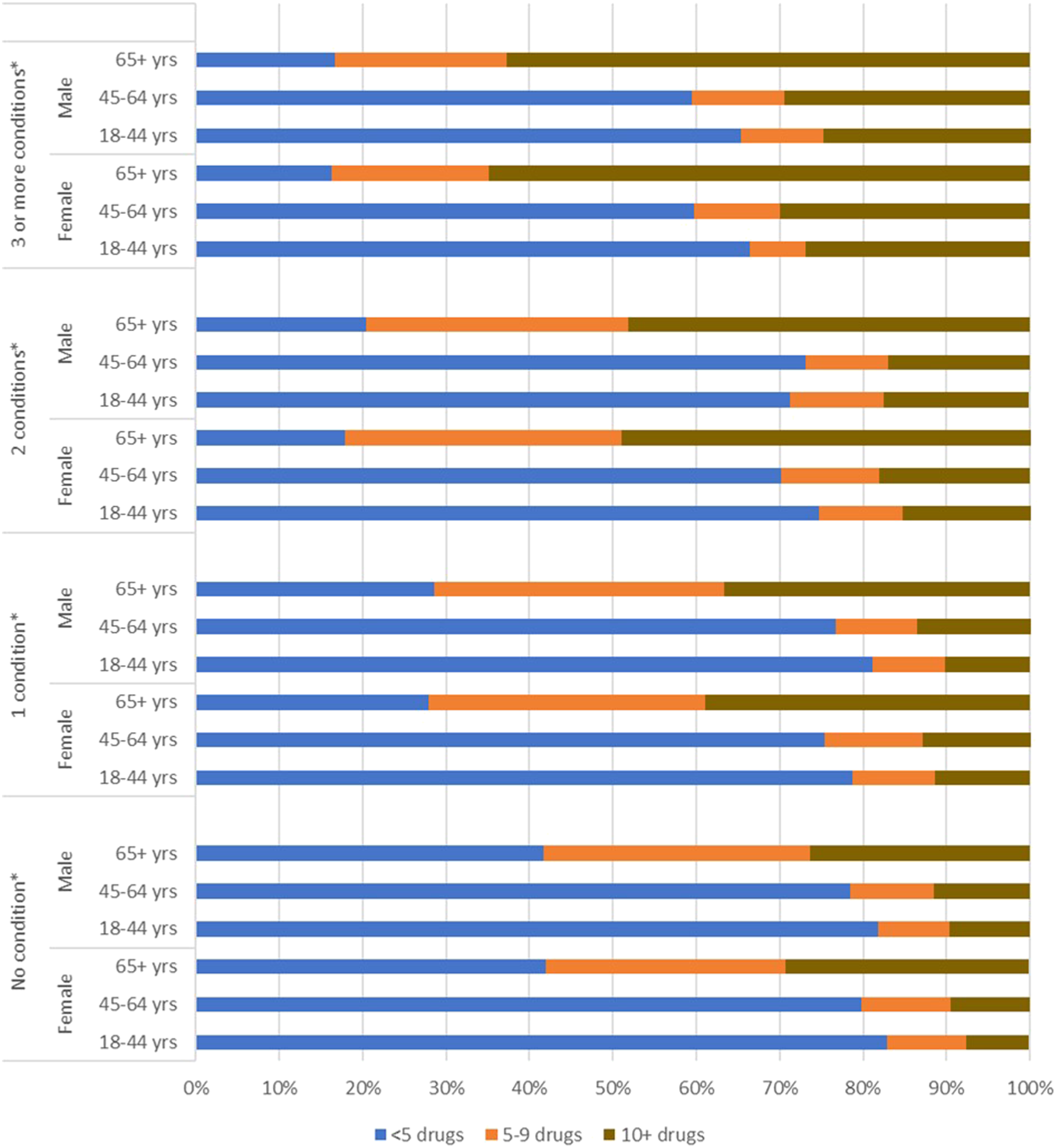
Logistic Regression Model Assessing the Interaction Between Multimorbidity and Age on Polypharmacy (5+ Drugs) After Cancer Diagnosis (N = 193 047).
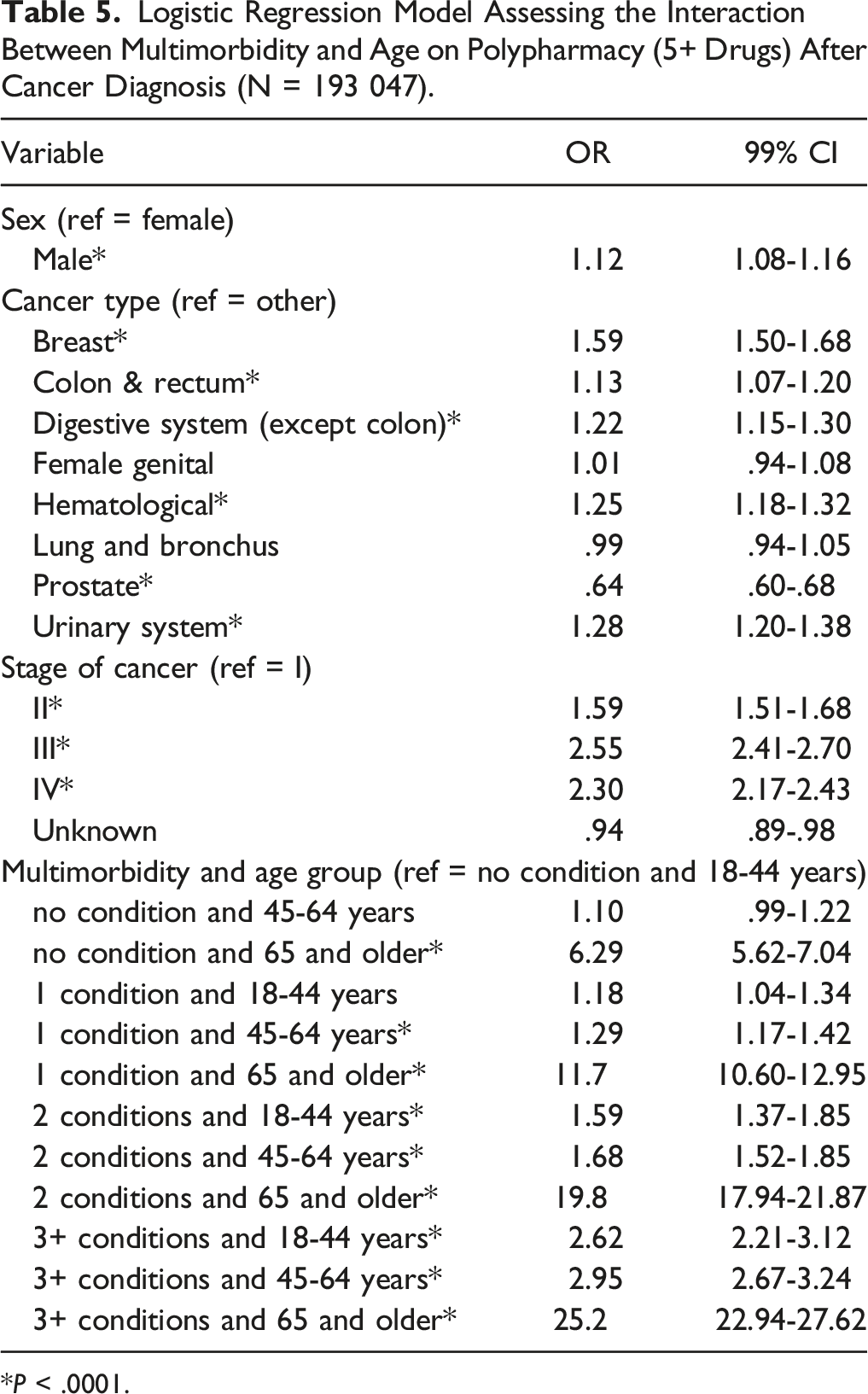
*P < .0001.
Impact of Polypharmacy on Health Service Utilisation
Logistic Regression Models on the Association Between Polypharmacy and Service Utilization.
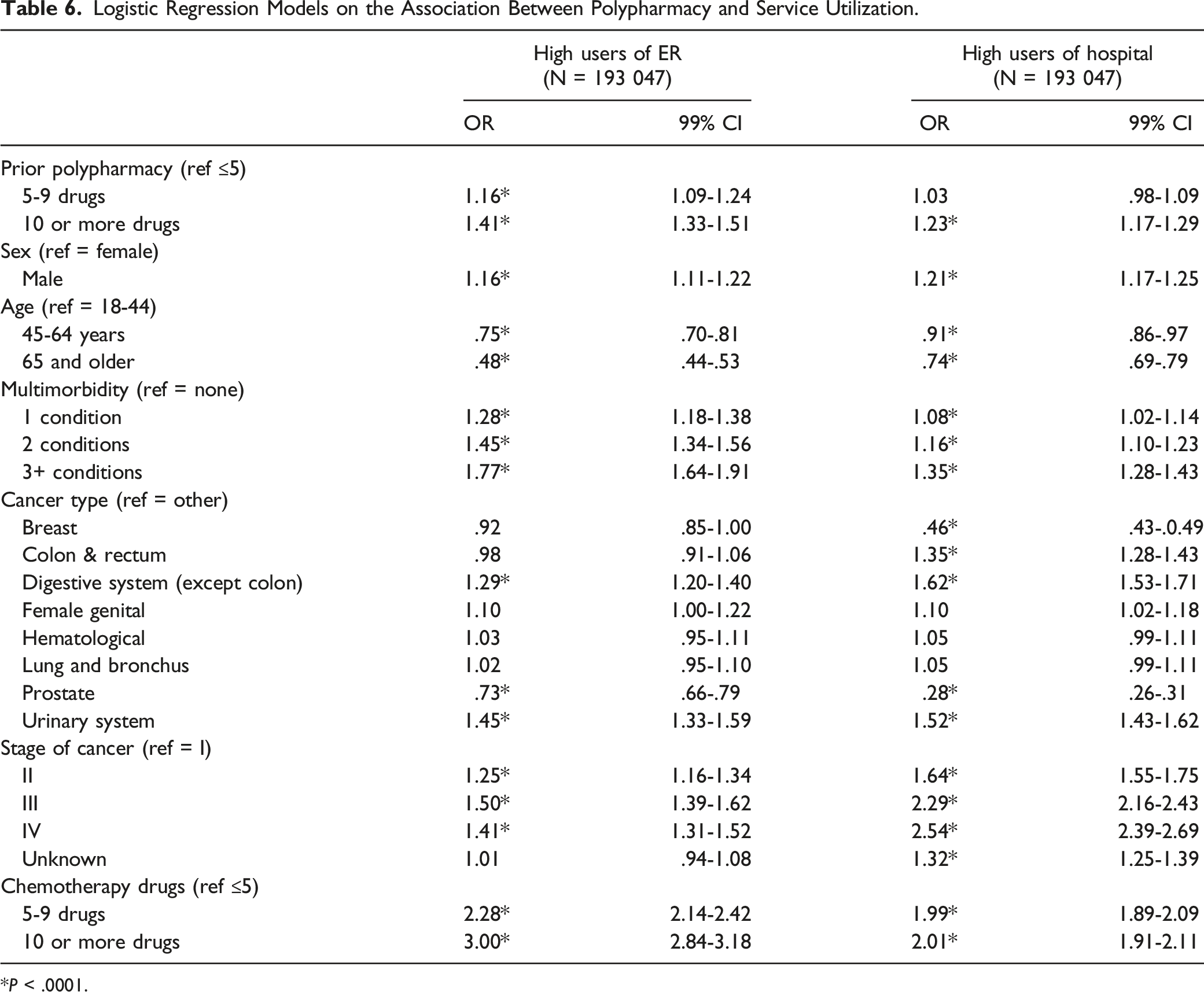
*P < .0001.
Discussion
The results of this study add to the body of literature demonstrating a relationship between polypharmacy (before and after cancer diagnosis) and older age and morbidity. 34 It also adds to the body of literature by examining younger age groups, which are not often considered.
Polypharmacy has numerous definitions, and regardless of the definition the presence of multimorbidity often leads to multiple medications. 3 The prevalence of polypharmacy was higher in males and older age; it also differed by levels of multimorbidity, which, combined with age had the largest impact. Adults 65+ years had the highest proportion of 3+ conditions, which explains the higher prevalence of polypharmacy in this age group. The observed increase in polypharmacy within and across multimorbidity levels by age is consistent with other general studies,35,36 and studies that included persons with cancer and multimorbidity.37,38 While comparable proportions of polypharmacy both across and within multimorbidity level were observed among males and females, regardless of age, other studies have shown variations in the prevalence between the sexes at different ages.39,40
The prevalence of polypharmacy was higher after a cancer diagnosis in all age groups; this is not surprising as pharmacotherapy is one of the most common treatment modalities for cancer management. 41 However, it is crucial to point out that, consistent with the literature, 42 the youngest age group was prescribed more chemotherapeutic drugs. As such, there was an absolute increase in polypharmacy in this group post cancer diagnosis. Further, older adults in particular may experience drug therapy related problems that require additional drugs as a form of management. 43 However, older adults with cancer who are frail, have very high levels of multimorbidity, or other physiologic compromises are less likely prescribed chemotherapy than younger adults.44,45 Also, the increase in the number of drugs prescribed in younger adults can possibly be due to nonadherence issues. Nonadherence to drug therapy is common in young adults (18+ years) with cancer; studies report that it ranges from 27% to 60% in some types of cancer.46,47 Failure to comply with recommended drug regimens can result in worsening of disease that may result in additional drug therapy or alternative management in younger adults.
Presence of hyper-polypharmacy prior to cancer diagnosis was significantly associated with being a high user of ER services and hospitalizations one year post diagnosis. Polypharmacy can be considered a marker for an individual’s underlying health status.48,49 Other population-based studies showed that the risk of ER visits and hospitalizations increased with the number of drugs prescribed in persons with different cancer types.50,51 An adverse drug event can be a consequence of polypharmacy and is one of the main drug related reasons for ER visits and hospitalizations.50,51
Consistent with other studies, those with 3+ chronic conditions were more likely to be high users of ER services and hospitalizations. This study also showed that people 45-65 years and 65+ years were significantly less likely to be high users of ER services and hospitalizations than those aged 18-44. These findings contradict other study results52,53 regarding older age being associated with increased health service utilization. This could potentially be explained by the fact that older adults typically have longer length of hospital stay, and this study focused on extremely frequent use, rather than overall use. In fact, more older adults may use the services, and longer, but not as repetitively as younger adults.
This study’s results support current literature regarding the relationship between health service utilization and sex, 54 types of cancer, 55 advanced stages of cancer, 56 and increased number of chemotherapy drugs.57,58 Moreover, we found that some types of cancer, advanced stages of cancer, and increased number of chemotherapy drugs were associated with a higher risk of being a high user of ER services and hospitalizations, similar to other studies.55-57,59 Certain cancer types and more advanced stages of cancer determine the frequency of health service utilization. For example, people with lung cancer have more symptom distress compared to other cancers which may result in more frequent health service utilization59,60 and more advanced stage cancer increases the risk of health service utilization due to their requirement for supportive management.60,61 Both the type and stage of cancer impact the number of drugs prescribed, including the type of chemotherapeutic agents which can potentiate the severity of drug therapy related problems. Studies also show that certain types of cancers that require high dose antineoplastic therapy may involve hospital admission,62,63 thus increasing the risk of health service utilization. Various determinants such as dosing frequency and required continuous infusions make the inpatient administration of chemotherapy the preferred practice for these persons.64-68 Chemotherapy regimens consisting of high doses can potentially cause toxicities and adverse drug events, and therefore hospital admission is recommended as best practice.62,66
This study is a population-based study using a cohort design with established methods, which was a major strength. As such it included all persons covered by the Ontario Drug Benefit program during the study period and also persons not covered, particularly all persons aged 65+ years, therefore minimizing selection bias. Most studies that assessed the prevalence of polypharmacy included mainly older adults with and without cancer; however, this study has extended the age of the population to include younger adults (18-64 years). We included all persons, those with ODB program coverage and those without coverage and therefore, the impact of polypharmacy was underestimated, a misclassification bias. Persons with no coverage were classified as having zero medications, this may not have been the case, they may have had private insurance coverage or paid out of pocket for their medications. According to the literature Canadians have their prescription drugs covered by private or public plans, with employer-sponsored drug benefits being a large source of drug coverage, about 60%.69,70 In 2012, public drug plans covered roughly 44% of drug costs, with the remainder being covered by private insurance plans and out of pocket. 70 According to the Ontario Ministry of Health fiscal year report 2019-2020 more than 940 000 Ontarians 24 years and younger receive ODB program coverage. 71
However, an important limitation is that only a small proportion of those 18-64 years is eligible to have their drugs covered by the Ontario Drug Benefit program. Besides, given the data sources, the study population included individuals who received care through the health care system of Ontario which may have also resulted in a selection bias. 72 However, Ontario has a universal health coverable for its population and such bias should be minimized. Misclassification bias with regards to multimorbidity is also a possible limitation, given that the diagnosis and documentation of concomitant diseases may be based on physician practices and the reporting of diseases. 73 However, if anything, the impact on the prevalence of polypharmacy would have been underestimated, as it is possible that some people deemed with no condition and their related medications should have been included in higher levels of multimorbidity. This study evaluated only the number of additional chronic conditions, which may be insufficient to understand the extent of polypharmacy related to disease severity among persons with cancer and multimorbidity. Being prescribed 10+ drugs was significantly associated with being a high user of ER services one year after cancer diagnosis (according to the literature increased number of drugs increases the risk of adverse drug events, and adverse drug events are one of the main drug related reasons for emergency room visits). Our study did not specifically study disease progression and whether it resulted in being a high user of ER services, however, it showed that persons with 3+ chronic conditions were more likely to be high users of ER services. The extent of polypharmacy related to disease severity or progression was not studied, though this may be somewhat captured by cancer stage, as disease may progress rapidly (within one year) for more severe cases. Also, we did not know the stage of cancer for about half of the sample. Though relevant for the impact on patients’ outcomes, inappropriate prescribing was beyond this paper and not considered in the study; this could be addressed in further work, as well as other possible additional confounders that were not available in the data.
Conclusion
Given that the prevalence of multimorbidity is increasing across age groups, there is need for additional studies that delve further into the nature of polypharmacy – ie, appropriate vs inappropriate, to ensure not only better quality of life for individuals, but also more effective use of the health care system. While older adults were at increased risk for polypharmacy and multimorbidity, our study showed that these issues are also present in younger adults. The inclusion of a younger group in our study is important as it may inform age-specific recommendations and targeted actions, such as patient education. Based on our study findings, it is evident that involvement of a multidisciplinary team that includes the input of clinical pharmacists, is needed to monitor and adjust medication lists to reduce or control polypharmacy, and thus ensure optimal outcomes in adults, both young and old, with cancer and multimorbidity.
Supplemental Material
Supplemental Material - Understanding the Extent of Polypharmacy and its Association With Health Service Utilization Among Persons With Cancer and Multimorbidity: A Population-Based Retrospective Cohort Study in Ontario, Canada
Supplementary Material for Understanding the Extent of Polypharmacy and its Association With Health Service Utilization Among Persons With Cancer and Multimorbidity: A Population-Based Retrospective Cohort Study in Ontario, Canada by Tamara Dean, Anna Koné, Lynn Martin, Joshua Armstrong, and Caroline Sirois in Journal of Pharmacy Practice.
Footnotes
Acknowledgments
This study contracted ICES Data & Analytic Services (DAS) and used de-identified data from the ICES Data Repository, which is managed by ICES with support from its funders and partners: Canada’s Strategy for Patient-Oriented Research (SPOR), the Ontario SPOR Support Unit, the Canadian Institutes of Health Research and the Government of Ontario.
Author Contributions
The opinions, results and conclusions reported are those of the authors. Yu Qing (Chris) Bai, Associate Analyst at ICES@UofT cut and linked the necessary data for the study population.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was derived from a larger research program supported by the Ontario Ministry of Health (MOHLTC) grant, #06034 to Dr. Kone Pefoyo as part of a HSPN team grant.
Data Availability
The data that support the findings of this study are available from ICES but restrictions apply to the availability of these data, which were used under the service agreement ICES DAS # 2020–727, and so are not publicly available. Access may only be granted under specific criteria and confidentiality conditions; please see ![]() .
.
Disclaimer
The opinions and statements expressed herein are solely those of the authors and do not reflect those of the MOHLTC; no endorsement is intended or should be inferred.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.