
Abstract
Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome is a rare and potentially life-threatening hypersensitivity reaction with cutaneous presentation and internal organ involvement. We herein present a case of phenytoin induced DRESS syndrome in a 56- year-old male who presented with high-grade fever and chills, cough with expectoration and generalized maculopapular rash. Laboratory findings revealed eosinophilia, leukocytosis, thrombocytopenia, transaminitis and elevated inflammatory markers. Further clinical, radiological and histopathological assessments confirmed the diagnosis. Phenytoin was discontinued, and patient was started on intravenous dexamethasone, which was later switched to oral prednisone. Rapid resolution of fever, eosinophilia and progressive improvement in skin rash and liver dysfunction was observed. Our report highlights the importance of prompt recognition of DRESS syndrome and the need for a guideline directed therapy for the management of this adverse drug reaction.
Introduction
Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, is a rare and potentially life-threatening multiorgan system reaction with a constellation of symptoms such as rash, fever, swelling, lymphadenopathy, leukocytosis and eosinophilia,with the most distinct feature being end organ dysfunction.1-3 The incidence of DRESS syndrome in new users is approximately 1 per 1500 and has a mortality rate of 10%. 4 The most frequent culprit drugs are anticonvulsants (phenytoin, phenobarbital), allopurinol and sulfonamides, with a long prodromal period of 2 to 6 weeks.5-8 The lack of unified guidelines makes the early suspicion of DRESS challenging for clinicians, thereby often resulting in worsening of the condition. 2 Hence, prompt identification of the prognostic markers and clinical findings are imperative for initiation of appropriate therapy.
The following case report on phenytoin-induced DRESS syndrome emphasizes the importance of early recognition and appropriate treatment in preventing the potential sequelae of this hypersensitivity reaction.
Case Summary
A 56-year-old male, who was a known case of seizure disorder on oral phenytoin 100 mg thrice daily(TID), since 2 weeks and levetiracetam 500 mg twice daily (BD), since 2 years presented with chief complaints of high-grade fever and chills since 4-5 days, cough with expectoration and generalized maculopapular rash without mucosal erosion. The patient noted rash and pruritis over extremities 3 days prior to presentation, which over the next few days progressed to his chest, back, and face. On initial examination, the patient was febrile to 38.8 °C (101.84-degree Fahrenheit) with a heart rate of 80 beats/minute, respiratory rate of 20/min, blood pressure of 120/80 mmHg and oxygen saturation of 96%. Preliminary investigations revealed hemoglobin 10.5 g/dl, total leucocyte count 13260/mm3, differential leucocyte count eosinophils 8%, polymorphs 62%, lymphocytes 26% and monocytes 4%. Thrombocytopenia was evident with an initial platelet count of 1,13,000 cells/mm3 and there was a profound elevation in the levels of inflammatory markers, namely Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP). Peripheral smear showed dimorphic anemia with occasional reactive lymphocytes. Liver Function Test (LFT) indicated normal serum bilirubin with elevated alanine aminotransferase (255 U/L) and aspartate aminotransferase (386 U/L). Blood and urine cultures were sterile. Echocardiogram (ECHO) report was found to be normal with no vegetation and good Left Ventricular (LV) function. Evaluation for Human Immunodeficiency Virus, Epstein-Barr Virus, Cytomegalovirus, dengue and hepatitis with serologies were found to be negative. The histology findings from the skin biopsy showed spongiosis and patchy exocytosis with no specific pathology in the dermis, suggestive of a drug reaction. Cardiology, neurology, pulmonology and dermatology consultation was done. Alternative diagnosis such as erythema multiforme, toxic epidermal necrolysis, an exanthem due to viral infection, vasculitis and auto-immune conditions such as systemic lupus erythematosus were ruled out. Based on the overall clinical picture and the current criteria, it was confirmed as a case of phenytoin-induced DRESS syndrome. On chest X-ray, there were patchy opacities suggestive of pulmonary invasion of DRESS and an ultrasound of chest indicated minimal pleural effusion with underlying segmental collapse. Transaminitis was consistent with hepatic involvement of DRESS syndrome.
Though levetiracetam is also known to cause DRESS syndrome, phenytoin was recently introduced for better seizure control.Since there weren’t any other routine medications, except the occasional use of an antacid, phenytoin was regarded as the culprit drug in this case.Thus, phenytoin was suspended and corticosteroid therapy was initiated with intravenous dexamethasone 4 mg BD, which was later switched to oral prednisone 20 mg daily (OD). The patient showed remarkable clinical response to treatment.Other presenting symptoms were managed with the use of pantoprazole 40 mg OD, acetaminophen 650 mg TID, silodosin 8 mg OD, loratidine 10 mg BD, potassium chloride syrup 15 mL TID, lorazepam 1 mg OD and fusidic acid topically. On the subsequent days, rash and fever subsided, inflammatory markers and hematological parameters were normalized. Chest X-ray was clear and transaminitis resolved. After 1 week of hospitalization, the patient was discharged on steroid taper.
Discussion
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) syndrome is 1 of the severe cutaneous adverse reactions to a drug.9,10 The most common pharmacologic triggers for DRESS include aromatic anticonvulsants (mainly phenobarbital, phenytoin, and carbamazepine), antibiotics (mainly trimethoprim-sulfamethoxazole, minocycline, vancomycin, and anti-tubercular drugs), dapsone, allopurinol, and nevirapine. 11 Although DRESS syndrome is most commonly associated with antiepileptic drug phenytoin, the first case of levetiracetam induced DRESS was reported in 2010. Since then only a few cases have been reported so far.12-14
In addition, ibuprofen, acetylsalicylic acid, sulthiame, and griseofulvin are considered possible triggers in children. 11 A potentially life-threatening syndrome occurs in 1-in-1000 to 1-in-10000 drug exposures, and the mortality rate is 10%, primarily due to liver involvement. 9 Adults are more likely to be affected than children. 11
Drug reaction with eosinophilia and systemic symptoms syndrome is characterized by fever ≥38 °C (100.4-degree Fahrenheit), skin lesions, lymphadenopathy, leukocytosis, eosinophilia, abdominal pain, and multiple organ involvement.5,9-11 It initially presents as a maculopapular or erythematous rash, which later progresses to a diffuse, pruritic rash. Severe cases may produce pustules, exfoliation, or mucosal eruptions. 1 A distinct feature of DRESS is the delayed onset of symptoms, that appear 2 to 6 weeks post-drug initiation and the illness usually lasts for more than 15 days.9,11,15
Hematological derangements are common, with eosinophilia being the most frequently occurring hematological abnormality (>50% of the cases). Impairments of solid organs such as liver, lung, heart and kidneys may be observed during the course of the condition. One of the most common visceral abnormalities encountered in these cases is hepatocellular necrosis with transaminitis. Acute respiratory distress syndrome and impaired pulmonary function are the common findings associated with pulmonary involvement, whereas cardiac involvement manifests in the form of left ventricular dysfunction and electrocardiographic changes. Risk factors such as old age or underlying renal or cardiovascular diseases may predispose individuals to acute kidney injury, but these changes are usually mild and will be recovered from in time without obvious sequelae. 9
Drug reaction with eosinophilia and systemic symptoms syndrome is considered as non-immediate DHRs (reactions that occur at least 1 hour after the initial drug administration or even after several hours or days) which is a delayed T-cell-dependent type of allergic mechanism. 11 The drug or metabolite accumulating in individuals with genetic predisposition induces drug specific T lymphocytes and triggers DRESS syndrome. On the other hand, the reactivation of viral infections caused by inciting drugs or their metabolites, or the creation of “cytokine storms” caused by anti-drug immune responses may induce robust anti-viral responses, contributing to the development of the disease. 9 The progression of DRESS is unpredictable, as severe cases are rare. 16 In a study by Pereira de Silva et al, an exposure period between 9 and 72 days until the onset of clinical manifestations was observed for phenytoin induced DRESS syndrome.Here,the reaction occurred post 2 weeks of drug initiation. 17
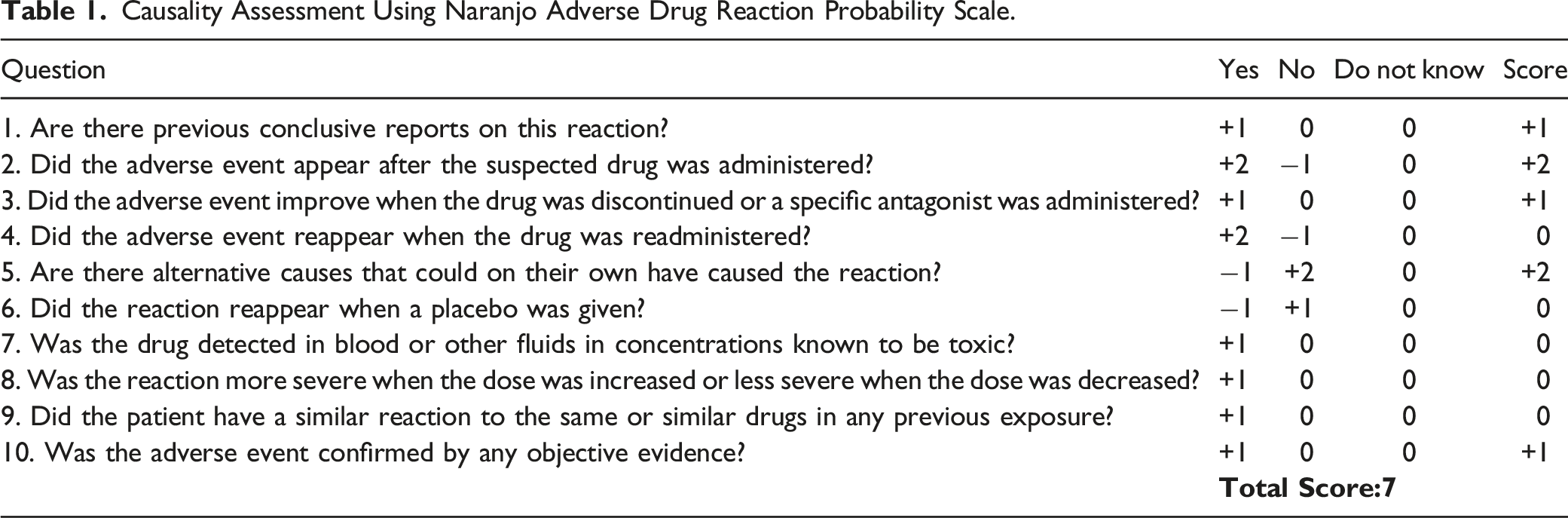
Causality Assessment Using Naranjo Adverse Drug Reaction Probability Scale.
The most important step in the treatment of patients suffering from DRESS syndrome is the immediate withdrawal of the inciting drug. By far, systemic corticosteroids administered IV alone or followed by oral corticosteroids is the mainstay treatment which can produce rapid improvements in symptoms. It is suggested to start with a dose of prednisolone, or the equivalent, of .5-1.0 mg/kg/day, tapered gradually over 2 to 3 months. Adjustments should be made according to the severity of the disease and any underlying co-morbidities.9,11,18 Supportive therapy consists of antipyretics, antihistamines, topical steroids and moisturizers. 4 Though the use of intravenous immunoglobulin (IVIG),immunosupressants and anti-viral treatment such as ganciclovir has been proposed, such management is not validated by well-designed controlled studies. 9
Conclusion
In conclusion, this report illustrates that the diagnosis of DRESS syndrome requires careful clinical observations and thorough laboratory examinations. Given the long prodromal period, systemic symptoms, and multi-organ involvement, a high index of suspicion is necessary to prevent fatal outcomes. Though corticosteroids are the mainstay treatment for patients with DRESS syndrome, most systemic treatments lack sufficient clinical evidence, as majority of these have been derived from case series or experts’ opinions. Hence, the development of evidence-based guideline directed therapy for the management of DRESS syndrome is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.