
Abstract
Introduction
The lack of medication adherence (or nonadherence) is a leading cause of poor health outcomes and hospitalizations. 1 It accounts for approximately 125 000 deaths and 10% of hospital admissions in the US. 1 In addition, those with chronic conditions may potentially be at risk of being nonadherent due to a complex medication regimen. This is concerning, as 6 out 10 adults in the US are diagnosed with a chronic illness. 2 Consequently, there are multiple factors associated with adherence, including behavioral barriers, personal views, social context, and medication access, which negatively influence therapeutic efficacy and disease progression. 3 With the persistent rise of nonadherence, the Centers of Medicare and Medicaid Services (CMS) identified 3 specific drug classes- (angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers ([ACEi/ARBs]), noninsulin antidiabetic medications, and HMG-CoA reductase inhibitors ([statins]) as part of CMS triple-weighted benchmark measures utilized to determine quality care among those with various diseases.4-6 Furthermore, to determine the quality of Medicare plans, Star Ratings are employed to allow Medicare beneficiaries the opportunity to compare the quality of health and drug plans being offered.4,6 Quality measures can be directly affected by medication use, including medication adherence to the above 3 drug classes. These measures may be used to tailor interventions to accommodate patient needs, reduce the risk of major cardiovascular and diabetes related event events (microvascular and macrovascular complications), while hopefully narrowing the gap of communication between providers and their patients.
Quality measures of medication use can be addressed by pharmacists as they are the most accessible healthcare providers. The role and responsibilities of pharmacists have evolved beyond dispensing medications and transitioned into providing clinical services.7,8 In the primary care practice setting, ambulatory care pharmacists are authorized to independently provide drug therapy management services, including medication prescribing, medication dispensing (ie, in-house insulin) and ordering of laboratory tests, according to collaborative protocols between physicians and pharmacists. Furthermore, ambulatory care pharmacists have direct access to the patient’s electronic health record (EHR), which allows them to view specialists’ notes, add additional therapeutic information, communicate with other healthcare professionals in a timely manner and provide greater healthcare efficiency. The resources available to these pharmacists allow for more effective and comprehensive clinical intervention services, in comparison to outside pharmacists, as they may be unable to view treatment plans and complete information about patients at the point of care.
Previous research conducted in a community pharmacy setting showed a significant impact of pharmacist interventions on adherence and a significant increase in proportion of days covered (PDC) scores among patients with hypertension and diabetes. 9 A PDC score is the preferred measure used by CMS to provide a representation of adherence with a threshold of ≥80%. 6 The PDC is the percent of days in the measurement period “covered” by prescription claims for the same medication or another in its therapeutic category. 6 These scores are often utilized in managed care and community pharmacy settings to provide interventions if necessary. However, there is still limited data available evaluating the impact of interventions provided by clinical pharmacists in a primary care setting.
As healthcare continues to shift towards value-based care models, ambulatory care clinics associated with accountable care organizations (ACOs) and management services organizations (MSOs) are held accountable for the quality of care provided to patients.4,10 Given the potential for improved quality measures, an effort to expand the pharmacists’ role in a clinical setting may facilitate improving adherence for certain chronic medications. The purpose of this study was to examine the impact of clinical pharmacists’ interventions on medication adherence and PDC scores for ACEi/ARBs, statins, and noninsulin antidiabetic medications in the primary care setting.
Methods
Study Design and Endpoints
This observational study was conducted at 4 primary care clinics within a managed service organization to evaluate adherence and PDC scores pre- and post-pharmacist interventions over a 9-month period (patients were contacted starting in April of the measurement year, as PDC scores from January- March were ≥85.0%). The study was approved by the institutional review board of Nova Southeastern University. The primary outcome of this investigation was change in PDC score. PDC was calculated based on the number of days in the measurement period “covered” divided by the total number of days in the period multiplied by 100. It was measured at baseline (pre-intervention), 1-month post-intervention, and at study-end (December 2020 for all subjects included in the study). Secondary outcomes were number, and types of adherence barriers identified, interventions provided by the pharmacist, and barriers and interventions category (pharmacy, patient, or physician-related).
Inclusion and Exclusion Criteria
Patients included in the study were Humana Part D beneficiaries ≥18 years or older with a baseline PDC score <85%, who were prescribed a statin, ACEi/ARBs, and/or a noninsulin antidiabetic medication and had ≥2 fills of medication during the 2020 measurement period. Of note, the specific number of days included in the measurement period, or calendar year, is determined based on the start date of the medication. Patients were excluded if they were pregnant, deceased, cognitively impaired, institutionalized (assisted-living facility, skilled nursing facility, rehabilitation facility, nursing home or hospice care), or had an inactive EHR at the time of the initial phone call or during follow-up phone calls.
Intervention
A total of 3 clinical pharmacists and 2 post graduate year-2 (PGY-2) ambulatory care pharmacy residents completed adherence telephone interventions. Each pharmacist worked at their respective clinic while pharmacy residents were assigned to these clinics as well as a fourth clinic on alternating days. Pharmacists and residents received monthly medication adherence reports from the insurance company Humana from April 2020 to December 2020. Reports contained patient demographics, calculated PDC scores, location and phone number of preferred pharmacies, last fill date, day supply, last date on hand, prescriber information, targeted medication name, and disease indication. In addition, adherence reports listed the preferred pharmacy each study medication was last filled. If a patient changed pharmacies, the new pharmacy was listed on subsequent reports, as this information is processed and updated through the insurance. Unfortunately, reports did not mention how patients specifically received their medication(s), however if patients received medication(s) from Humana, next to each prescription “Humana Pharmacy Mail Order” was named as preferred pharmacy.
Upon receiving PDC reports, a pharmacist contacted patients whose PDC scores were <85% from their respective clinics. Of note, medication nonadherence is defined as a PDC <80%; however, for this study, patients with a PDC score <85% were contacted to proactively prevent their score from declining and possibly becoming nonadherent. Patients received at least 1 pharmacist outreach telephone call from a pharmacist or resident prior to the next fill date of their prescription(s). If the patient agreed to the interview, the pharmacist proceeded to conduct a 5 to15-minute interview using a standardized template that allowed pharmacists to consistently gather the same information (Supplemental 1). The template included an introduction explaining the purpose of the phone call and was designed to identify barriers and implement interventions based on patient response. Pharmacist conducting interviews had ≥1 of the following: an active state pharmacist license, Board Certified Ambulatory Care Pharmacist Certification or Board-Certified Cardiology Pharmacist Certification. Residents received proper training from their preceptor(s) on motivational interviewing to improve adherence among adults.
The interview began with the pharmacist assessing if the patient was currently taking the prescribed medication(s). If so, the patient was instructed to verify the dose, route, frequency, and indication. As the interview progressed, open-ended questions were used to gather the greatest amount of information, for example: When was the last time you missed a day taking your medication(s)? How often do you miss a dose? What side effects are you experiencing while taking this medication? How do you feel this medication is helping you? Based on patients’ response, the pharmacist reviewed different adherence barriers (eg, forgetfulness, pill burden, transportation, denial, refills needed) and discussed recommended interventions (eg, change to a 90-day supply, refill request, pill reminder alarms) with the patient. Throughout the interview, pharmacists noted any discrepancies between what the patient reported vs what was documented in the EHR and communicated concerns or recommendations directly to the physician face-to-face or through the EHR via “Pharmacy Telephone Encounters”. Additionally, the pharmacist used the patient’s EHR to access laboratory findings, physician notes, and other clinical information needed for intervention purposes. Each pharmacist was given an “Adherence Dictionary Code” to document barriers and interventions using numerical codes that translated to the appropriate intervention and barrier for data collection. Additional comments per pharmacist discretion regarding the telephone call were documented as well.
When appropriate, the pharmacist contacted the patients’ pharmacy to discontinue medication(s) that were discontinued by the physician and documented in their assessment notes. Interventions requiring physician approval or attention (eg, change in therapy, dosing discrepancy) were communicated to prescribers via messages in the EHR. Follow-up phone calls were attempted for patients whose PDC score declined upon receipt of the subsequent adherence report. If a patient did not answer the phone, a voice message requesting a callback to the clinical pharmacist was left when possible. Lastly, the details of each pharmacist’s telephonic encounter were documented in the EHR when necessary. Required EHR documentation included, medication discontinued by patient/provider, side effects/adverse reactions, follow-up, refills needed, and hospital admission. Other barriers and interventions such as, forgetfulness, transportation, or medication counseling were documented on the pharmacist’s “Patient Adherence” spreadsheet list. A maximum number of 4 telephone attempts made to patients was indicated for this study. Data collection included demographic information (age, gender, ethnicity), number of hospitalizations within the year, prescriber specialty (cardiology, endocrinology, family practice and other), baseline PDC (pre-PDC score [patients initial contact], monthly post PDC scores, identified adherence barriers, pharmacist interventions and intervention and barrier category.
Statistical Analysis
Mean and standard deviation and count and percent were used to describe continuous and categorical variables, respectively. A non-parametric related-samples Wilcoxon Signed Rank test was used to test the difference in PDC scores between baseline (pre-intervention) and second (1-month post-intervention) and baseline and study-end. An alpha level of 5% was used.
Results
Demographic and Clinical Characteristics of Patients.
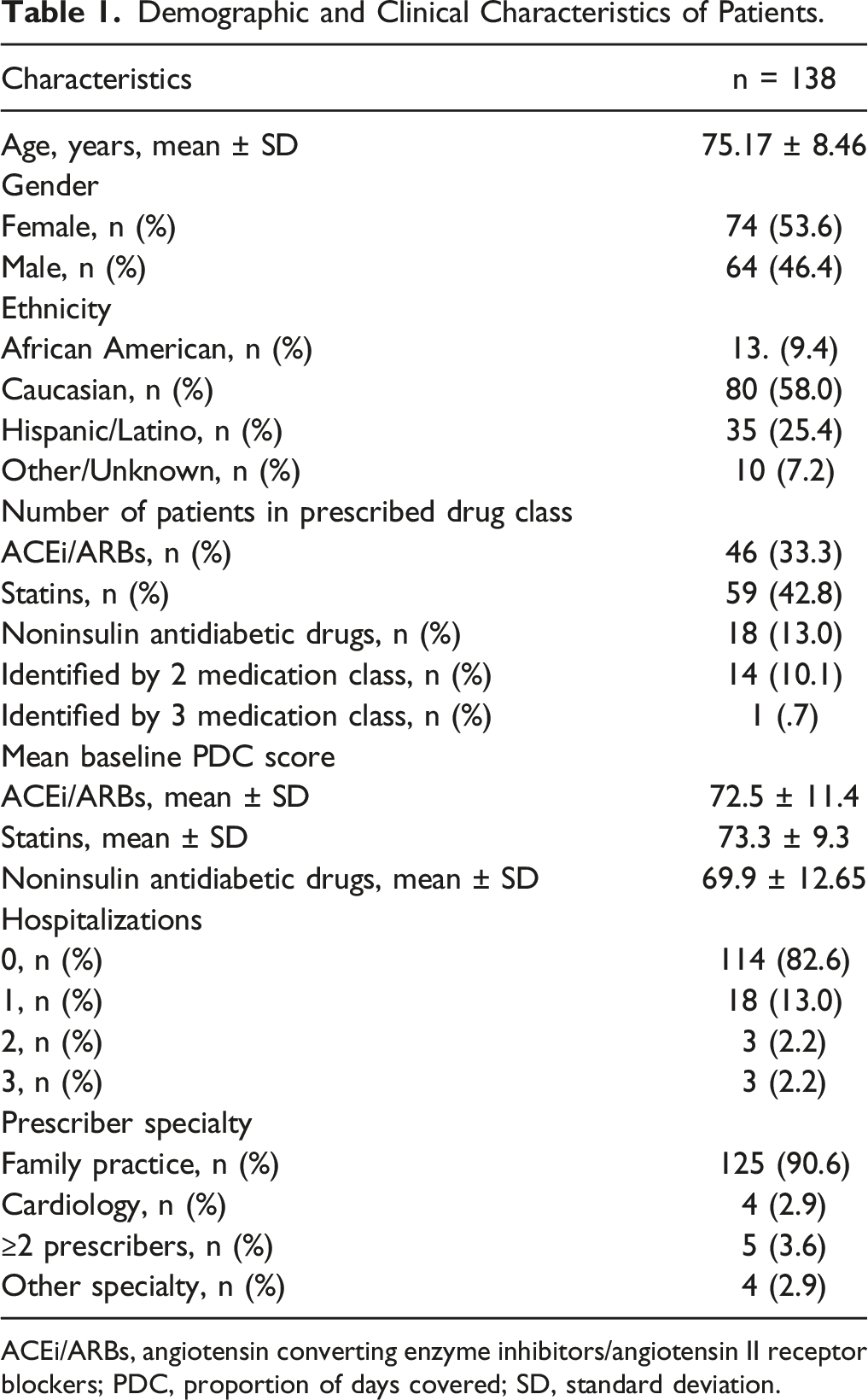
ACEi/ARBs, angiotensin converting enzyme inhibitors/angiotensin II receptor blockers; PDC, proportion of days covered; SD, standard deviation.
Average Change in Final PDC and Change in PDC 1 Month Following Intervention.
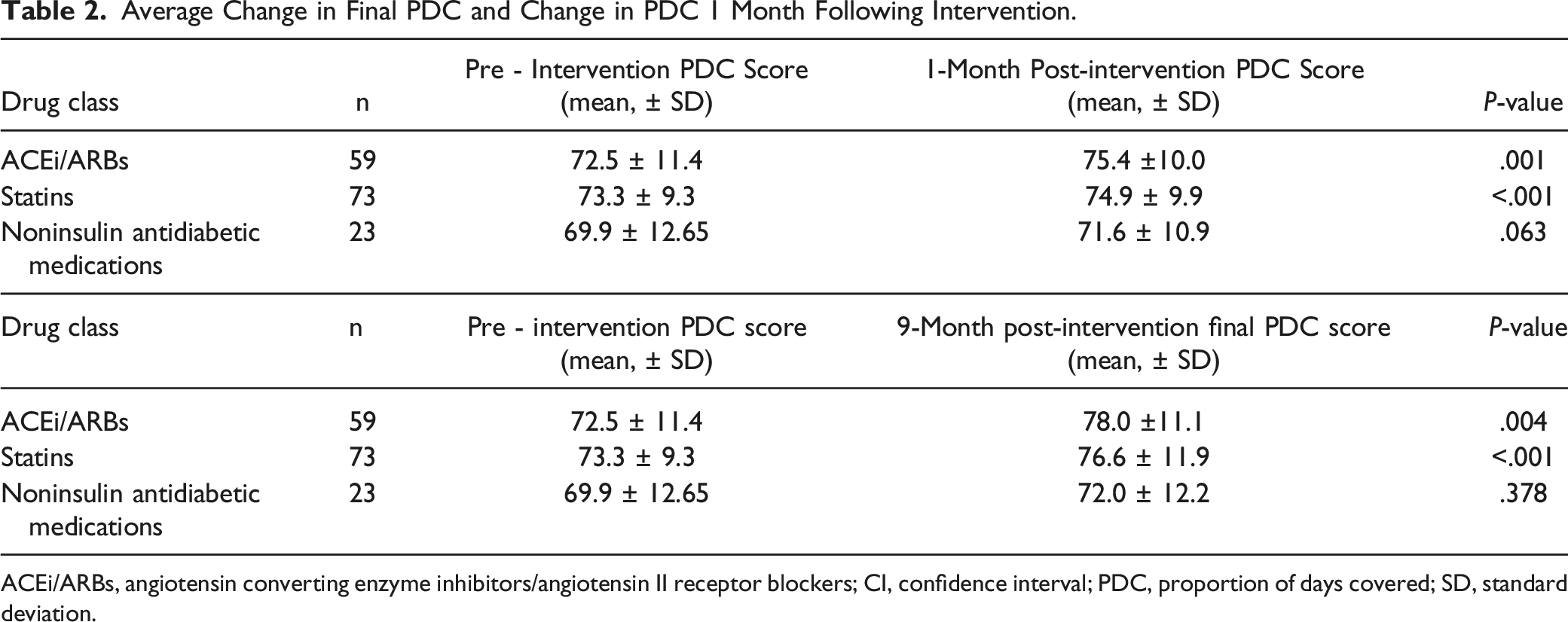
ACEi/ARBs, angiotensin converting enzyme inhibitors/angiotensin II receptor blockers; CI, confidence interval; PDC, proportion of days covered; SD, standard deviation.
Identified Patient Barriers.
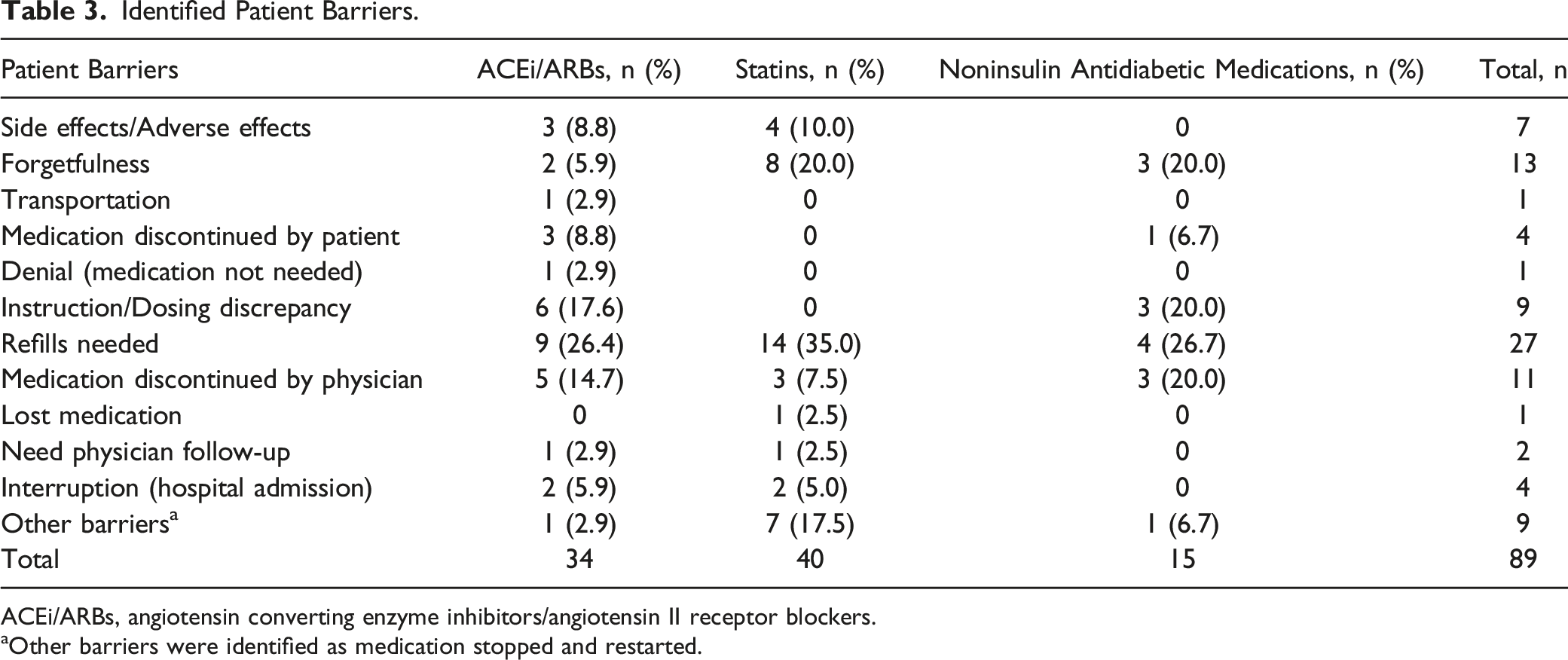
ACEi/ARBs, angiotensin converting enzyme inhibitors/angiotensin II receptor blockers.
aOther barriers were identified as medication stopped and restarted.
Pharmacist Interventions.
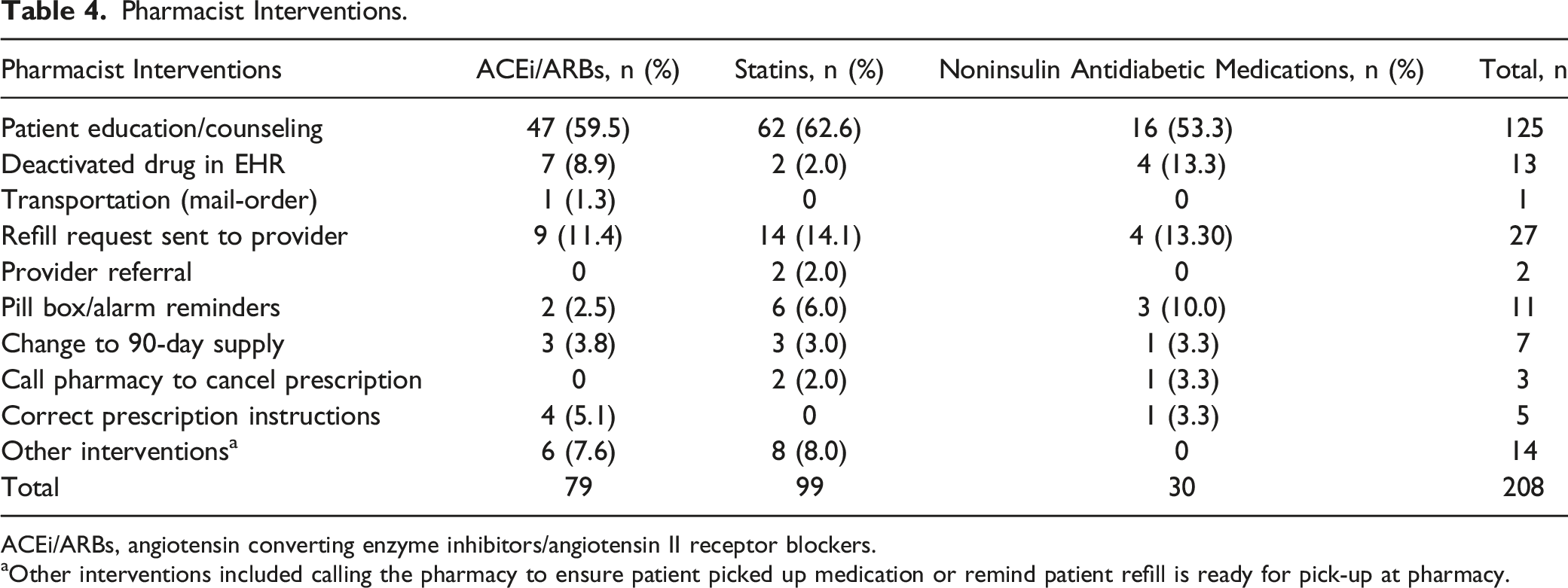
ACEi/ARBs, angiotensin converting enzyme inhibitors/angiotensin II receptor blockers.
aOther interventions included calling the pharmacy to ensure patient picked up medication or remind patient refill is ready for pick-up at pharmacy.
Category of Barriers.
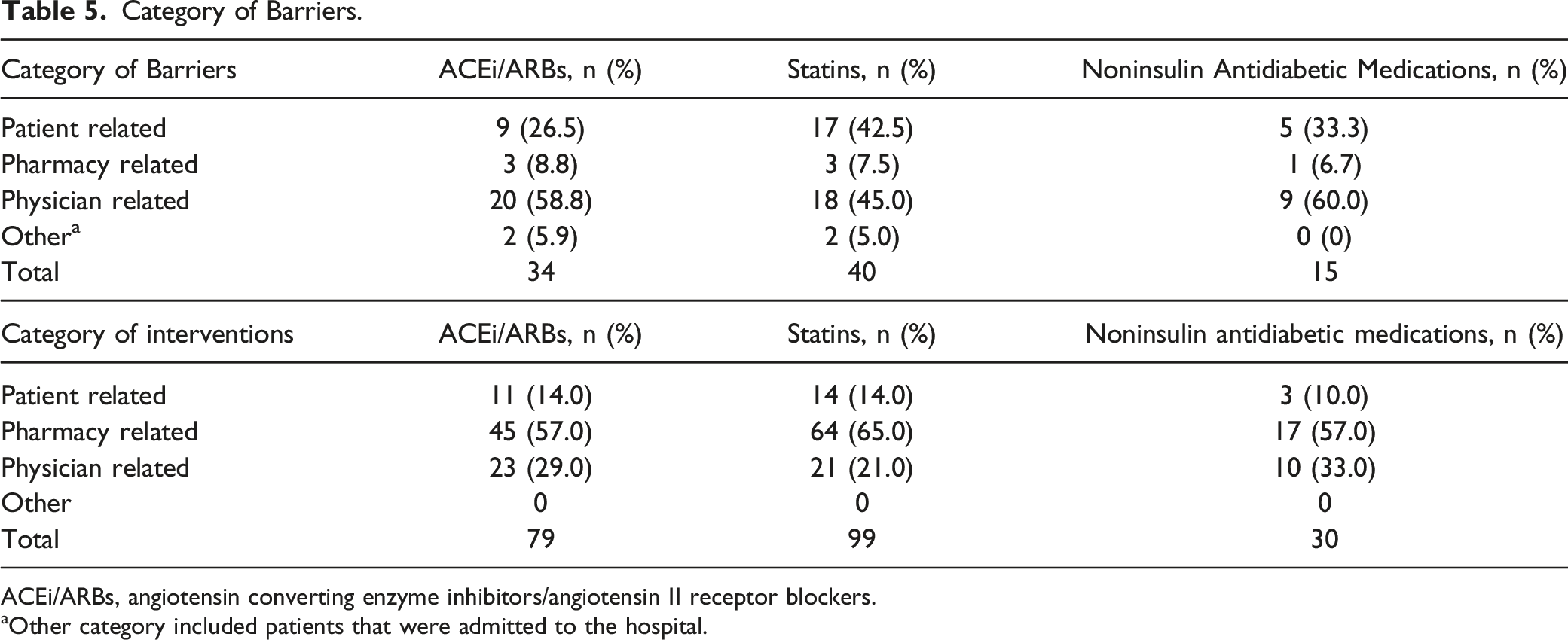
ACEi/ARBs, angiotensin converting enzyme inhibitors/angiotensin II receptor blockers.
aOther category included patients that were admitted to the hospital.
Discussion
This study aimed to improve medication adherence and PDC scores among a total of 138 Humana beneficiaries. This study demonstrated that a brief telephone call conducted by clinical pharmacists in 4 different primary care settings did improve medication adherence, mean change in final PDC score and PDC score 1-month following pharmacist interventions in patients prescribed ACEi/ARBs and statins. This significant difference was not observed with the noninsulin antidiabetic medications, however, an overall improvement in PDC scores for this drug class was observed which may be attributed to some patients receiving diabetes management from pharmaists. The effects of unreported monthly PDC scores for patients on noninsulin antidiabetic medications who also received insulin billed through Humana decreased the sample size and may have impacted outcomes in comparison to other drug classes. Furthermore, diabetic medication management is further complicated by treatment complexity and fear of hypoglycemia that can be associated with problematic adherence. 11 The most significant impact that may have led to increased adherence with ACEi/ARBs and statins included patient counseling and refill requests sent to the provider. Additionally, many barriers identified among all groups were prescriber-related (eg, refills needed, instruction/dosing discrepancy, or medication was inadvertently discontinued by the physician).
The importance of improving medication adherence is paramount, especially among geriatric population, as health literacy and the day-to-day aspects of medication (ie, timing, dosage, and frequency) can be determinants of adherence. 12 On average, patients ≥60 years of age takes at least 2-9 medications per day due to multiple chronic conditions. 13 This translates to multiple prescriptions and a complex medication regimen, resulting in an increased risk for nonadherence, which makes the challenge of managing chronic health conditions more difficult. 14 Patients within this study average age was 75 years old, had multiple chronic conditions, and prescribed ≥3 medications per day. Many faced various contributing factors, such as visual, hearing, or cognitive impairment that greatly impacted medication adherence. This potentially led to patient’s lack of knowledge or understanding about different doses, frequencies, routes of administration, or the reason a medication is needed. Additionally, some patients experienced impaired dexterity which is needed for medications requiring pill splitting.
Clinical pharmacists in a primary care setting serve as an integral team member that can improve health outcomes and at the same time impact quality measures. The pharmacists in this study provided direct patient services in addition to completing medication adherence calls. These services include heart failure, diabetes, and hypertension management under a collaborative practice agreement (CPA). Patients are referred by the physician to schedule follow-up appointments with the pharmacist for comprehensive medication management, review labs, and discuss available therapeutic alternatives. In addition, pharmacists participate in transitions of care management during in-clinic visits providing counseling and post-discharge follow-up. Understanding the benefits of a multidisciplinary team, many providers have continued devoting resources towards building comprehensive physician-pharmacist collaborative models, where pharmacists emerging in the ambulatory care specialty are considered resources to address medication management and expand the pharmacist’s role. 15 Pharmacists practicing in physician’s offices under a CPA can access EHRs, make referrals and perform specific patient care functions such as administer drugs, discontinue therapy and adjust drug treatment regimens. 16 Therefore, having direct access to this information allows for more informed clinical interventions.
A single method cannot improve adherence by itself, but a combination of various adherence techniques can be implemented to address the problem. 3 The most common method utilized in practice is analyzing PDC scores. One study used PDC scores to categorize patients into the following groups (nonadherent who remained nonadherent, nonadherent who became adherent, adherent who became nonadherent, and adherent who remained adherent) to examine pharmacist impact after interventions (eg, explain the benefits of the medication and called the responsible provider to confirm medication was appropriately discontinued) and determined which group showed a significant increase in PDC scores. 5 The results showed among nonadherent subjects who became adherent, the mean PDC increased by 14%, with a 12% decrease in mean PDC score in the nonadherent who remained nonadherent group. 5 Other studies targeted patients with a PDC score <80% to improve Medicare Part D overall Star Ratings and demonstrated medication adherence improvement for targeted maintenance medications, overall health plan quality performance, star ratings, and health outcomes.17,18 Pharmacists interventions in this study improved overall PDC scores, however, the final mean PDC scores for December among all drug classes was <80%. This may be attributed to our mean baseline PDC scores being lower in comparison to other studies; 10% of patients were prescribed medications from ≥2 drug classes, and the mean age of patients in this study was 75 years of age, making them more complicated to manage medication adherence.
Nevertheless, medication adherence interventions completed by a pharmacist in the primary care setting differ from those in a community pharmacy setting. As community pharmacists can incorporate medication synchronize programs and easily determine prescription cost savings, their ability to make accurate therapeutic recommendations and change therapy is limited due to restricted access of health records. The impact of medication adherence involves more than interviewing a patient and asking standardized questions. It involves assessing the patient entirely and reviewing past encounters to understand disease progression and treatment history. Therefore, prior to making an adherence phone call, pharmacists in a primary care setting have acquired enough background information about the patient to easily navigate through the interviewing process and effectively address barriers and concerns.
Implementing telephonic or remote pharmacist services were positive solutions during the coronavirus disease 2019 (COVID-19) global pandemic and can be utilized moving forward as it helped reduce disease exposure for staff and patients. In March 2020, the United States implemented social distancing and restricted access to healthcare facilities which put a huge strain on patient’s health. 19 Many individuals were unable to visit healthcare facilities due to canceled or postponed preventative appointments and laboratory tests, leaving a gap in disease management, and impacting medications regimens. Providers faced considerable challenges in trying to provide high-quality and accessible care, while maintaining safety regulations. 19 Additionally, obtaining prescription drugs became difficult as medication availability was limited due to drug shortages, contamination of drug supplies, and the closing of pharmacies. Unfortunately, the psychological impact of the pandemic left many with chronic diseases little hope of improving medication adherence, and perhaps eroding health gains made prior to the pandemic. 19 Although, various methods have been incorporated into practice to help patients maintain their drug regimens, the pandemic greatly put a huge strain on the healthcare system.
This study has several limitations. First, the sample size was small and during the study period several patients were unable to be reached after multiple attempts for follow-up interventions. Monthly PDC scores for patients on noninsulin antidiabetic medications were unreported if they received insulin billed through Humana insurance. This made it difficult to gather data and analyze medication adherence. Additionally, follow-up calls were not always conducted prior to next fill date, as the date reported on the adherence report did not coincide with refill eligibility. Furthermore, not all clinics began telephone interventions at the same time, 2 clinics started telephone interventions in April, while the other clinics started interventions in May and June when PDC scores were <85%, and patients were interviewed using a non-validated adherence tool. Lastly, a PDC score was used instead of MPR (medication possession ratio), another method utilized to evaluate medication adherence by determining patient accessibility to the medication. MPR is calculated based on the sum of day supply dispensed from the first fill until the end of the time frame divided by the sum of the number of days from the first fill until the end of the time frame times 100. 20 Unfortunately, MPR overestimates adherence because it does not take into consideration the date a prescription was filled but rather the day supply and days within the time frame. 20 This often leads to an adherence score exceeding 100% for patients who routinely fill their medications early. In contrast, a PDC calculation adjusts for overlapping supply (early refills), and prevents adherence scores from becoming inflated. Further research is needed to measure the impact of clinical pharmacists’ interventions in a primary care setting on quality measures, cost, reimbursement, and patient-physician satisfaction.
Conclusion
This study demonstrated that a pharmacist telephone call intervention significantly improved PDC scores and medication adherence to patients prescribed ACEi/ARBs and statins, as well as a positive trend of increased PDC scores among noninsulin antidiabetic medications was shown. Given the need to reach quality measures benchmark goals in value-based care models, a targeted effort to improve adherence for chronic medications may help achieve quality care and improve health outcomes. Clinical pharmacists in a primary care setting serve as an integral team member that are uniquely positioned to assist with medication adherence and quality measures in ACOs.
Supplemental Material
Supplemental Material - Evaluating Pharmacist-Driven Interventions in a Primary Care Setting to Improve Proportion of Days Covered and Medication Adherence
Supplemental Material for Evaluating Pharmacist-Driven Interventions in a Primary Care Setting to Improve Proportion of Days Covered and Medication Adherence by Dominique D Davis, Genevieve Hale, Cynthia Moreau, Tina Joseph, Alexandra Perez and Elaina Rosario in Party Politics
Footnotes
Acknowledgments
The authors would like to acknowledge the MSO and the providers/staff of the four primary care clinics for their support of this research. Additionally, the authors would like to acknowledge research assistant Noor Alawwa, PharmD 2022 Candidate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.