
Abstract
Introduction
Pharmacists are recognized by the American College of Cardiology (ACC), 1 the Heart Failure Society of America 2 and the International Society of Heart and Lung Transplantation 3 as valuable members of the multidisciplinary team caring for patients with heart failure (HF) and post-orthotopic heart transplantation (OHT). In 2018, medication adherence and the cost of care were identified as two of ten pivotal issues affecting the attainment of optimal outcomes in HF patients. 1 To optimize medication access and adherence, recommended tactics include the involvement of pharmacists in medication education during hospitalization, navigating insurance coverage and assistance programs, performing telephone call backs to assess medication adherence and drug access post-hospitalization, and ensuring optimal transitions of care (ToC) from the inpatient to outpatient setting. 1 As such, the key tactics to address these pivotal issues span the spectrum of inpatient and outpatient pharmacy services supporting the development of a complementary pharmacy practice model (PPM).
In 2019, a meta-analysis of 18 studies involving 4630 HF patients revealed a reduction in HF hospitalizations (OR .72, 95%CI 0.55-.93, P = .01) associated with pharmacist inclusion in the multidisciplinary approach to HF management. 4 Single center studies included in this meta-analysis demonstrated the impact of HF pharmacists working in the cardiac care unit, cardiothoracic unit and the outpatient setting on medication error reduction, medication adherence and rates of unplanned hospitalizations. 4 Of note, most of these studies involved fragmented pharmacy services with pharmacist involvement in a particular patient setting, either inpatient or outpatient.2,4 In 2019, Murphy and colleagues 5 described the combined efforts of inpatient and outpatient pharmacists on the 30-day readmission rate of HF patients. 5 Although the readmission rates did not differ significantly between the pre-intervention and intervention groups, the ‘high touch’ pharmacist-driven ToC program serves as a model of complementary pharmacy practice.
To our knowledge, a PPM dedicated to an advanced HF/OHT program that provides complementary services in the surgical unit, cardiomyopathy unit and outpatient clinic, with technical support at all points in the patient’s care, has not been previously described. In keeping with the recommendations of the Pharmacy Practice Model Initiative (PPMI),6,7 our PPM was established to meet the dynamic and pivotal needs of an expanding Advanced HF/OHT program and to maximize the roles of both pharmacists and a technician dedicated to this multidisciplinary program.
Methods
Study Setting
The institution in which this PPM was developed is an urban, 415-bed tertiary care academic medical center. It is a level 1 trauma center with 48 adult intensive care beds and a full-service provider to ambulatory, medical, pediatric and surgical patients. The Advanced HF/OHT Service has 600 to 700 inpatient admissions per year. Of these, approximately one-third are patients with acute decompensated heart failure requiring mechanical circulatory support and/or IV inotrope therapy who undergo formal evaluation for an advanced HF therapy (eg, left ventricular assist device (LVAD), OHT). Approximately 40% of these admissions are related to complications associated with LVAD implantation (eg, gastrointestinal bleeding, infection) or OHT (eg, infection, rejection, severe neutropenia). During the past 5 years (2017-2021), 205 patients have been transplanted with an average of 40 patients per year, and 98 patients have undergone LVAD placement with an average of 20 patients per year. During this same period, the ambulatory volume for the Advanced HF/OHT Service has ranged between 4000 and 4500 visits per year. In 2021, 392 patients post-OHT received follow-up care by this service, a 35% increase since 2018.
Rationale for the PPM
Establishment of this PPM was prompted by the expansion of our OHT program, nearly doubling in volume in 1 year (2015 to 2016). Prior to establishment of our model, only 1 full-time equivalent (FTE) inpatient HF/OHT pharmacist was allocated to the program based on the Centers for Medicare and Medicaid Services standards for transplant centers. 6 With the expanded volume of the OHT population, an outpatient pharmacy technician was dedicated to the program in 2015 to assist with medication access, navigate medication insurance coverage, and provide follow-up telephone calls to facilitate outpatient prescriptions in a timely manner. Two additional pharmacy positions, a cardiothoracic unit (CTU) pharmacist and an outpatient clinic HF pharmacist, needed to be justified to complete the four-member complementary pharmacy team.
Pharmacy Personnel Involved in our Practice Model.
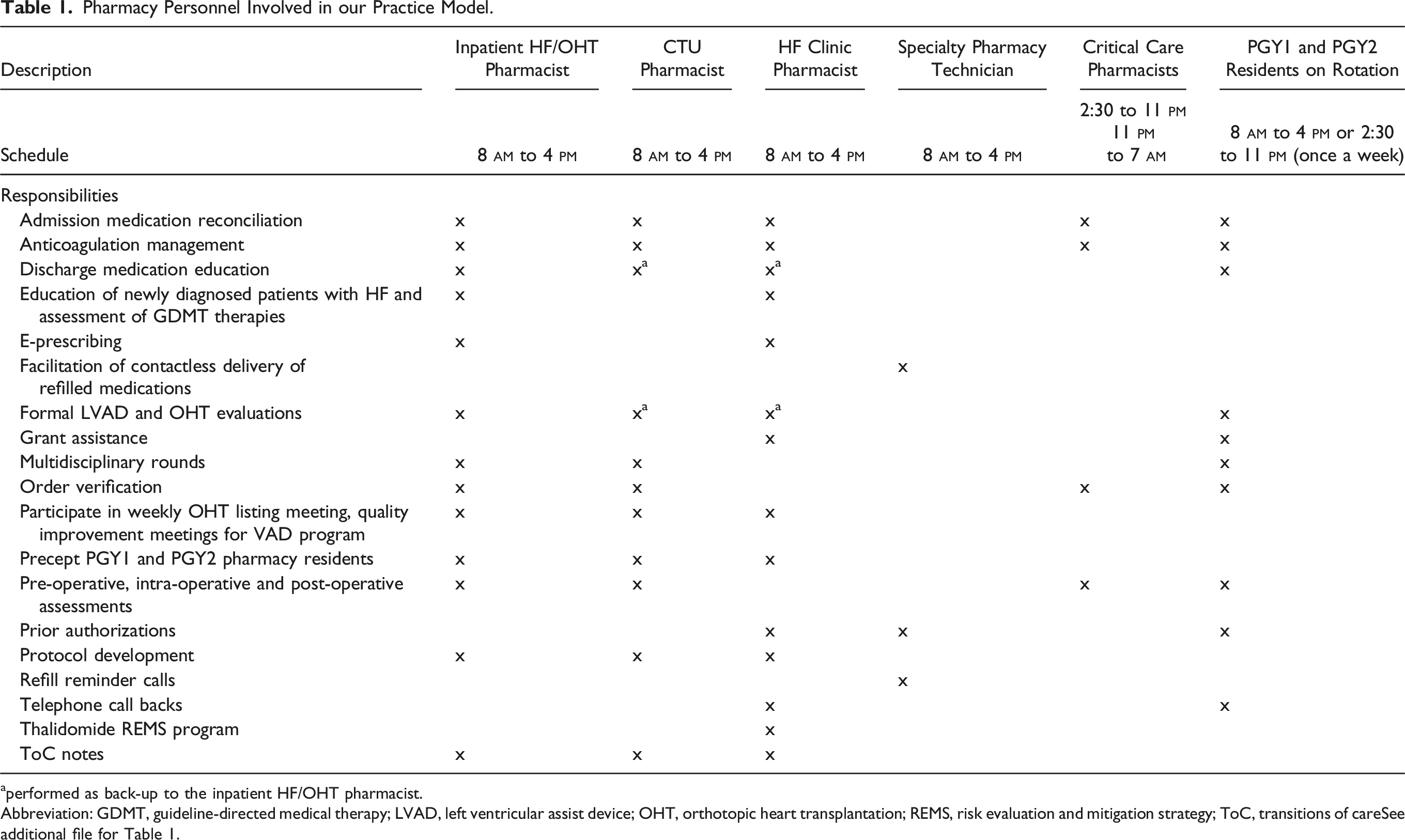
aperformed as back-up to the inpatient HF/OHT pharmacist.
Abbreviation: GDMT, guideline-directed medical therapy; LVAD, left ventricular assist device; OHT, orthotopic heart transplantation; REMS, risk evaluation and mitigation strategy; ToC, transitions of careSee additional file for Table 1.
Design of the PPM
Our PPM was specifically designed to address gaps in care, particularly in the areas of medication access, medication education and ToC, to our highest risk cohort within the Advanced HF/OHT population, our LVAD-supported and post-OHT patients. These patients were targeted due to their higher rate of readmission within our Advanced HF population and their routine use of high-risk medications. In addition to focused efforts on this patient cohort, our 4-member pharmacy team also provides routine pharmaceutical care to all patients admitted to the Advanced HF/OHT inpatient service, to all patients housed in the CTU, and on request to all patients seen in cardiology clinic. The PPM was also designed based on recommendations in the Consensus on PPM Initiatives7,8 to (1) increase accountability of the pharmacist as a member of the multidisciplinary team, (2) prioritize patients based on the complexity of their medication regimen, (3) prevent medication errors through improved ToC, (4) maximize the role of the technician through task shifting, and (5) contribute to the financial initiatives of the institution through revenue generation. The methods by which these gaps were addressed are described below.
Medication Access
Prior to the model, medication access issues in our high-risk population were largely identified and addressed at the time of discharge medication prescribing. With the new PPM, the pharmacy technician proactively investigates medication access and affordability when an evaluation for an advanced therapy (ie, LVAD and/or OHT) is initiated. In particular, the technician investigates insurance coverage of essential, high-cost medications including immunosuppressants, antiviral agents, antibiotics and injectable anticoagulants. Identified issues are shared with the multidisciplinary team (eg, inpatient and outpatient HF pharmacists, social worker, Director of the OHT program) prior to LVAD implantation or at the time of OHT listing. Members of the multidisciplinary team can then develop a proactive plan to ensure medication access at time of patient discharge. At time of discharge, all outpatient medications for our cohort are e-prescribed by the inpatient pharmacist under a collaborative practice agreement and provided at the patient’s bedside as part of the hospital’s ‘meds to beds’ service. Discharge medications are provided by the medical center’s outpatient pharmacy or via a specialty pharmacy, if warranted by the patient’s insurance. Following discharge, the clinic HF pharmacist works with the technician to ensure continued medication access. Transplanted patients are encouraged to continue to fill their outpatient prescriptions via our outpatient pharmacy for at least the first year post-OHT. Medications are provided via contactless delivery with refill reminders offered via telephone by our dedicated pharmacy technician. The outpatient HF pharmacist e-prescribes medications under a collaborative practice agreement and coordinates medication access via manufacturer assistance programs and grant agencies. All medication access issues and resolutions are documented in the patient’s electronic health record (EHR).
Medication Education
Prior to the PPM, all newly transplanted patients received medication education using a standardized, individualized tool (known as a ‘medication card’) on discharge to home or rehabilitation facility. Pill box filling by the patient was facilitated by the inpatient HF/OHT pharmacist at the time of discharge to home or from rehabilitation facility to home. With the new PPM, standardized discharge education has been expanded to include all newly implanted LVAD patients and all OHT patients whether newly transplanted or admitted for a transplant-related complication. LVAD-supported patients receive standardized oral and written education on warfarin therapy with teach back to ensure understanding of medication administration, need for monitoring, INR goal, common signs of bleeding and the potential for drug interactions. These patients also receive standardized oral and written education on an injectable anticoagulant (ie, enoxaparin or fondaparinux). A 5-day supply of the injectable anticoagulant is dispensed at time of discharge to prevent delays in access when indicated as outpatient bridge therapy. With expansion of our PPM to include an outpatient pharmacist, updated medication cards are provided to all OHT patients at each clinic visit. The outpatient HF pharmacist is also now responsible for e-prescribing, educating and facilitating pill box filling for all newly transplanted patients discharged from a rehabilitation facility to home. The outpatient HF pharmacist also facilitates medication adherence through providing individualized medication cards to select LVAD-supported patients, coordinating blister packing of medications by our outpatient pharmacy, and conducting routine pill box filling with team-identified nonadherent OHT patients. Reinforcement of medication education is also provided by the outpatient HF pharmacist via telephone call backs (see ToC section). Copies of all medication cards are posted on a shared drive for access by all multidisciplinary members. All communications regarding medication education conducted via telephone call backs are documented in the patient’s EHR.
Transitions of Care
Prior to this PPM, ToC activities were limited to medication reconciliation for all patients admitted to the Advanced HF/OHT Service and a ToC note on discharge to home or rehabilitation facility. Within 24 hours of admission, reconciliation is completed; discrepancies are reconciled and documented in the patient’s EHR. At the time of discharge, a ToC note is provided by the inpatient HF/OHT pharmacist to the outpatient providers (ie, OHT coordinators, LVAD coordinators) via email and documented in the patient’s EHR. This communication provides a summary of any pertinent medication-related issues (eg, current drug-drug interaction requiring close monitoring, restricted access to a medication based on insurance, concern for nonadherence) in addition to a copy of the patient’s medication card. Following institution of the new PPM, the ToC initiative has expanded to include the CTU and outpatient pharmacists. In addition to the aforementioned ToC activities, a ToC note is now provided by the inpatient HF/pharmacist to the CTU pharmacist upon patient transfer to the OR for LVAD implant or OHT. This communication focuses on drug allergy information, prior home medications that require continuation, concerns regarding pain or sleep management, and other pertinent, patient-specific medication needs. The CTU pharmacist assesses the pre-operative and intra-operative medication needs of the patient and provides daily pharmaceutical care during the patient’s post-operative stay. With inclusion of the CTU pharmacist, medication reconciliation is performed pre-operatively, post-operatively and at the time of transfer to the cardiomyopathy ‘step down’ unit. In our OHT population, the CTU pharmacist documents a comprehensive assessment of the patient’s immunosuppressant and antimicrobial regimen in the EHR within 24 hours post-surgery. This note also addresses the patient’s chronic medications (eg, thyroid replacement therapy, anxiolytics, antidepressants, antihyperglycemics) to ensure continuity of care. Upon transfer from the CTU to the cardiomyopathy unit, the CTU pharmacist documents a ToC note directed to the multidisciplinary team resuming the patient’s care. In the cardiomyopathy unit, the inpatient HF/OHT pharmacist resumes responsibility for the pharmaceutical care of the patient until discharge. Following the provision of discharge education with medication access as previously described, the inpatient HF/OHT pharmacist submits a ToC note to the outpatient OHT and/or LVAD coordinators in addition to the outpatient HF pharmacist. The outpatient HF pharmacist now assumes responsibility for the patient, conducting a telephone call back within 48 hours of discharge to reinforce medication education. The outpatient HF pharmacist also meets with the patient in clinic within 7 days post discharge to review the medication list, assess medication adherence and knowledge, and address any drug access issues. All interventions are documented and communicated in the EHR. If the patient is readmitted, the outpatient HF pharmacist provides a ToC communication to the inpatient HF/OHT and CTU pharmacists prior to or at the time of patient admission. Information provided in this note includes an accurate, updated medication reconciliation and notation of any ongoing medication issue (eg, intolerability of post OHT medication, recent diagnosis of leukopenia or infection, reason for dose adjustment of immunosuppressant or other post OHT medication). As such, a circle of care is provided by all pharmacist providers in this PPM.
Medication Errors
Prior to this model, medication errors were prevented on admission via medication reconciliation with discrepancies rectified within 24 hours. The inpatient HF/OHT pharmacist also participates daily in multidisciplinary rounds with the Advanced HF/OHT Service providing prospective medication review, order verification, formal evaluation of patient candidates for LVAD implantation and/or OHT and monitoring of high-risk medications. With the model’s expansion, additional opportunities were identified for prevention of medication errors. In the CTU, the dedicated pharmacist participates in daily multidisciplinary rounds with both the surgical and Advanced HF/OHT Service teams. The CTU pharmacist assesses each patient prior to surgery for risk of intra-operative vasoplegia and manages the patient accordingly based on a protocol developed by the pharmacist in collaboration with cardiovascular surgeons and anesthesiologists. This pharmacist assists in the selection of intra-operative antibiotics based on drug allergy assessments, in the selection and dosing of blood products (eg, anticoagulant reversal agents, blood factors), and ensures safe and timely administration of immunosuppressants for OHT patients in the intra-operative and post-operative settings. Expansion of the PPM to include an HF clinic pharmacist provides opportunity to proactively prevent clinically significant drug interactions at the time of outpatient medication prescribing, evaluate the likelihood of drug-induced diseases, and optimize anticoagulation and immunosuppressant drug dosing. The outpatient HF pharmacist works collaboratively with outpatient providers to optimize anticoagulant therapy for both LVAD-supported and OHT patients requiring anticoagulation.
Study Objective
The objective of this prospective study was to describe and quantify the activities of a 4-member pharmacy team working collaboratively to address gaps in the care of a high-risk cohort of Advanced HF/OHT patients. The inpatient cohort was defined as LVAD-supported and OHT patients with any admission (index admission or admission for a complication) to the Advanced HF/OHT Service in fiscal year 2020. The outpatient cohort included LVAD-supported and OHT patients in addition to other HF patients seen on request (eg, new referrals, patients with amyloidosis). The specific gaps in care targeted by the pharmacy team were (1) ensuring medication access at the time of hospital discharge and as an outpatient; (2) providing comprehensive medication education on a continuum in both the inpatient and outpatient settings; and (3) preventing medication errors through improved ToC. In addition, the economic benefits of this pharmacy initiative on revenue generation were quantified. This project was submitted to the institutional review board (IRB) at our medical center. It was not deemed as human subject research warranting patient consent.
Date Collection and Analysis
The number of admissions to the Advanced HF/OHT Service for patients in the high-risk cohort was identified from the hospital’s daily census reports upon review by the inpatient/HF pharmacist. Clinic visits for patients meeting the definition were also identified via review of daily clinic census reports by the outpatient pharmacist.
During fiscal year 2020, the 4-member team maintained a dashboard of interventions that addressed the targeted gaps in care. Each month, the following interventions were quantified: • medication reconciliations completed for admissions to the Advanced HF/OHT Service in the high risk cohort; • admission medication discrepancies identified and reconciled; • documented ToC notes; • patient consultations/encounters; • cohort patients (number and percentage) who received discharge education and ‘meds to beds’; • telephone call backs conducted by outpatient pharmacist; • prior authorizations sought and approved; • patients who received assistance through grants or manufacturer-based programs; • cohort patients receiving anticoagulation management coordinated by the outpatient pharmacist; • OHT patients contacted via telephone for refill reminders by specialty technician;
The number of OHT patients who received medications via contactless delivery from our outpatient pharmacy in fiscal year 2020 was also quantified. Annual revenue generated from prescription volume attributed to the Cardiology Clinic was determined in 2017 through 2020. Summative fiscal year metrics were used to determine changes in both prescription volume and net revenue. Due to the evolving role of the clinic pharmacist during this period, all high-cost and difficult to access cardiovascular medications were tracked and included in the comparisons.
Results
FY 2020 Metrics for Pharmacy Advanced HF/OHT Program in High-Risk Cohort.
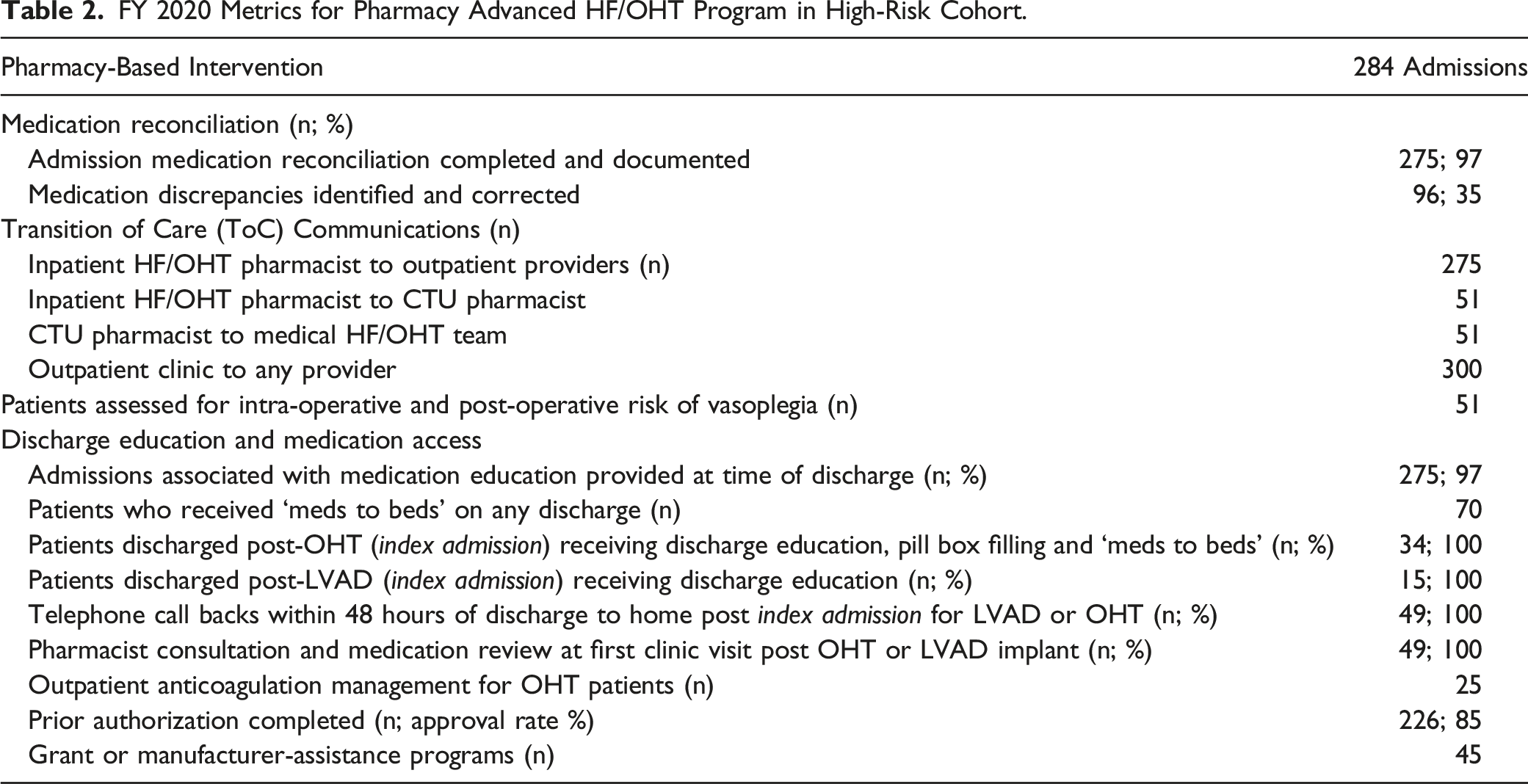
A ToC communication was submitted by the inpatient HF/OHT pharmacist to the CTU pharmacist for 100% of patients in the cohort (n = 51) transferred to the surgical service for OHT (n = 36) or LVAD implantation or exchange (n = 15). Prior to surgery, 100% of these patients (n = 51) were screened by the CTU pharmacist for risk of intra-operative vasoplegia and for risk of serotonin syndrome in the setting of potential methylene blue administration. Within 24 hours post-OHT, a ToC note was documented in the EHR in 100% of transplanted patients. For all patients in the high-risk cohort who were transferred to the surgical service for any reason during the admission (n = 51), a ToC communication was documented by the CTU pharmacist upon transfer of the patient to the cardiomyopathy unit. At time of hospital discharge, a ToC communication to next provider was documented for 275 (97%) of the 284 total admissions. This communication was provided to the clinic providers within 48 hours of discharge; 87% were documented in the EHR within 24 hours of discharge.
The majority of this cohort (97%) received some form of discharge education by the inpatient HF/OHT pharmacist or another member of the pharmacist care team. All patients who survived OHT to discharge (n = 34) received individualized education with pill box filling and provision of discharge medications via the hospital’s ‘meds to beds’ program. Most OHT patients (>75%) admitted to the Advanced HF/OHT Service for an OHT-related complication received an updated medication card at time of discharge. All patients who underwent LVAD implantation or exchange in 2020 (n = 15) also received anticoagulation-related education for both oral and injectable agents upon discharge. Discharge medications were provided by the hospital’s ‘meds to beds’ program for LVAD-supported patients based on patient request.
Expansion of the PPM to include an outpatient HF clinic pharmacist resulted in telephone call-backs in 100% of newly transplanted and LVAD-implanted patients within 48 hours of discharge. The outpatient HF pharmacist documented a total of 300 ToC notes during 2020, including those for patients in the admitted cohort and in high-risk patients seen as outpatients for routine follow-up appointments. A total of 1800 patient encounters were documented by the outpatient HF clinic pharmacist in 2020 with 45% of these visits involving patients who met the definition of the high risk cohort. During 2020, the HF pharmacist’s role was expanded to include the care of OHT patients requiring anticoagulation. As of 2020, 25 OHT patients receive follow-up care by the pharmacist for anticoagulation management, INR monitoring and drug dosing.
In 2020, all newly transplanted patients received their outpatient medications at time of discharge to home or from rehabilitation facility as part of the hospital’s ‘meds to beds’ program. E-prescribing was performed by a team pharmacist in 100% of these patients. Based on data obtained from our outpatient pharmacy, approximately 65% of our total OHT population continues to receive their medications from our outpatient pharmacy on a monthly basis via contactless delivery. In 2020, a total of 900 reminder calls were made by the dedicated pharmacy technician with approximately 75 OHT patients contacted per month.
As depicted in Figure 1, the number of prescriptions generated from the Cardiology Clinic increased by 42% from 2017 to 2020. This increase in prescription volume was associated with a 157% increase in net revenue from 2017 to 2020. The increased revenue is attributed to an increase in both OHT prescriptions and prescriptions for a number of high-cost specialty medications (eg, PCSK9 inhibitors, tafamadis) facilitated by the outpatient HF pharmacist. Outpatient prescription volume 2017-2020.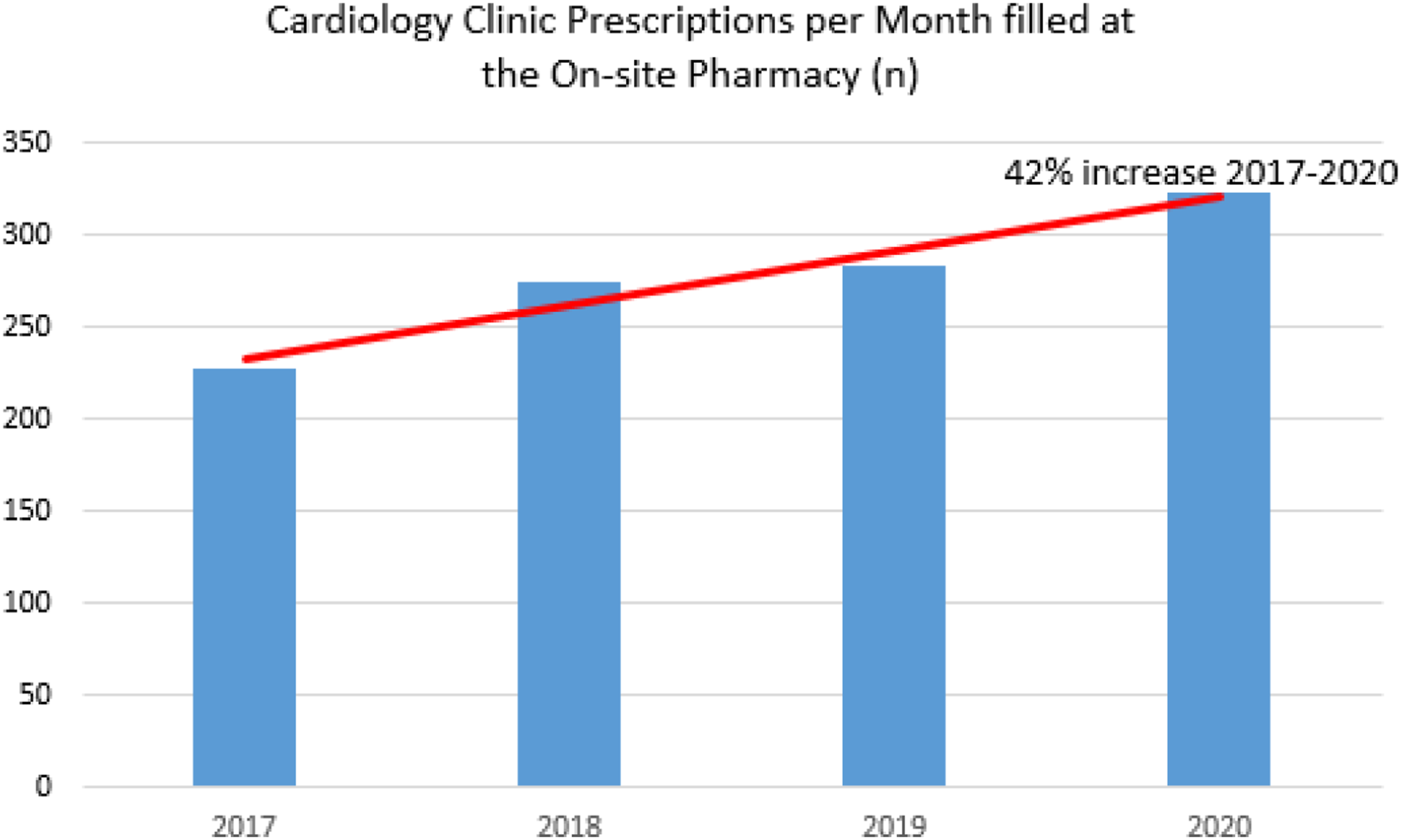
Discussion
As Murphy and colleagues
5
described, a ‘high touch’ pharmacist model is needed to care for the patient with HF. The high readmission rates unique to this patient population support multiple opportunities for medication errors, drug access issues, inadequate medication reconciliation, and patient confusion about their medications. Pharmacists in both the inpatient and outpatient settings have been shown to contribute to the overall success of multidisciplinary HF teams.2,4,9 In the majority of studies, the effects of individual pharmacists providing care at one or two specific points in the patient’s care have been described and quantified.2,4,9 Our PPM advances the practice of pharmacy by providing complementary services with multiple points of collaboration and communication throughout all phases of the patient’s inpatient and outpatient care. As such, a circle, rather than a longitudinal model of practice, best describes our pharmacy model based on the extent of interplay and communication between the team members at each point in the patient’s care. Figure 2 illustrates these contact points as patients transition from home to hospital, throughout the hospital stay, and from hospital to home. Points of Contact and Coordination of Care. Each star signifies a point of contact between 2 pharmacists. (1) Patient on service is admitted to a specific unit and a medication reconciliation is completed. (2) Prior to cardiothoracic surgery, in-hospital medication reconciliation is completed. (3) When patient is transferred to the step-down cardiomyopathy unit (CMU), a ToC note is performed. (4) At time of discharge, the HF/OHT pharmacist provides ToC note to outpatient clinic pharmacist. (5) The outpatient clinic pharmacist provides medication updates to the inpatient pharmacy members to facilitate timely and accurate medication reconciliation at time of patient admission. Med rec = medication reconciliation; MCS = mechanical circulatory support; ToC = transitions of care; CTU = cardiothoracic unit; CMU = cardiomyopathy unit.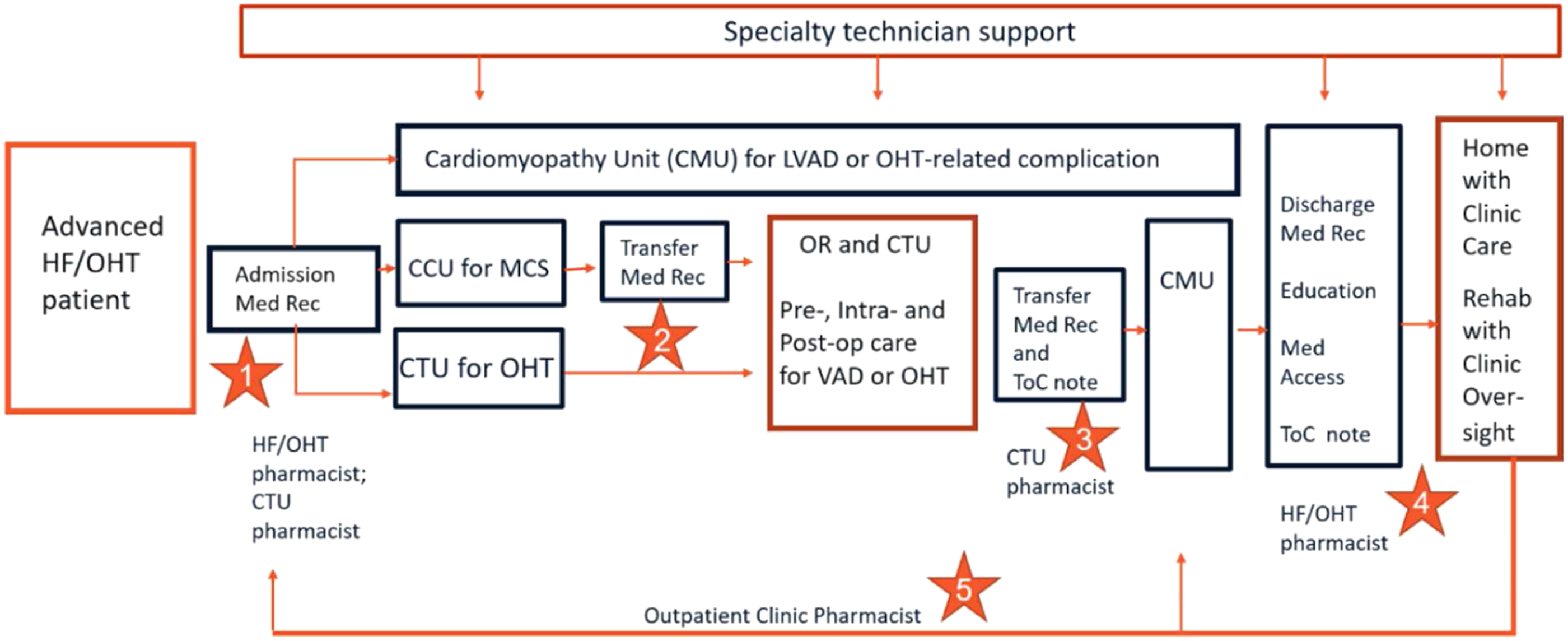
In a 2018 ACC Expert Consensus Decision Pathway, 1 both medication adherence and the cost of care were identified as pivotal issues affecting the achievement of optimal outcomes in HF patients. Multiple strategies were described to address these gaps in care including the involvement of pharmacists in providing structured medication education prior to hospital discharge, navigating issues with insurance, and performing telephone call backs to assess adherence and medication access post-hospitalization. Our PPM was designed to address these gaps in care, particularly in our high-risk cohort of LVAD-supported and OHT patients. By working together in a complementary fashion, our pharmacy team provided discharge education to 97% of the cohort followed by timely outpatient care. The individualized medication card has been identified by the multidisciplinary team as a valuable tool in enhancing medication adherence. Patients routinely request an updated copy of the card on hospital discharge, when seen in clinic, or when ordering refills of their medications in conversation with our dedicated technician. Providing access to updated medication cards on the shared drive has also proved to be valuable. Such access allows all member of the multidisciplinary team to be aware of the patient’s current medication list and regimen allowing for improved coordination of care.
Our new PPM also improved medication access. In 2020, our team ensured medication access to 100% of our newly transplanted patients on discharge to home and such access was sustained via contactless delivery to 65% of our overall OHT population. Prior to institution of our PPM, OHT patients received their initial fill of their discharge medications from our outpatient pharmacy, but the majority subsequently obtained refills from numerous pharmacies throughout our region with no direct oversight by our OHT team. This led to patient frustration with medication refill delays and inefficient use of HF/OHT team resources to solve medication-related issues at outside pharmacies. With our current PPM, any issue with refills (eg, insurance coverage gaps, drug shortages) can be conveyed by the pharmacy technician directly to the multidisciplinary team. Moreover, any medication issue expressed by the patient to our specialty technician and/or outpatient pharmacist can be forwarded to the appropriate multidisciplinary team member and addressed in a timely manner. Our PPM has not only improved medication access for our OHT population but also for our LVAD-supported patients. As of 2020, all newly implanted LVAD patients are assessed for insurance coverage of injectable anticoagulants at time of index admission and provided with a 5-day supply at discharge or first post-implantation clinic visit. Many LVAD patients previously experienced issues with access to enoxaparin or fondaparinux due to cost or availability, delaying the initiation of outpatient bridge therapy. Our PPM has extended our outreach to the LVAD patients by providing individualized medication education, access to injectable anticoagulants, telephone call backs and anticoagulation oversight by the outpatient pharmacist.
As stated by Manasse, 7 redefinition of a care model takes time. It takes time to reconfigure and redeploy human resources to achieve the progress that is needed. It also takes time to enact a vision, build a cohesive team of accountable providers, engender support from health care colleagues, and examine the impact of the model on key outcome measures. Our PPM was established in 2017 and is still evolving. Time was needed to build a cohesive team, to cross-train and to ensure cross-coverage. In 2017, monthly meetings of the 3 pharmacists on the team were initiated. During these meetings, the pharmacists discussed medication topics (eg, conversion of patients from one immunosuppressant to another, frequently occurring drug-induced diseases such as neutropenia), shared journal articles and performed journal club activities, and discussed program developments (eg, thalidomide program for LVAD-associated GI bleeding, updated graft rejection protocols). Both the CTU and clinic pharmacist were trained in performing formal LVAD and OHT evaluations and in providing discharge counseling/pill box filling for OHT patients. Cross-training also occurred between the inpatient and outpatient pharmacists relative to outpatient processes for specialty drug access. Training of PGY1 and PGY2 residents (critical care, cardiology) was extended to include rotations in the CTU and outpatient HF clinic. To sustain this model, routine communication and collaboration between the 4-member team remain essential. In addition, the continued development of pharmacy staff members, both pharmacists and technicians, to cover the service during off-hours and paid time off (PTO) days is critical to success of the PPM.
Most important, our PPM provides an example of a synergistic, complementary practice directed toward a high-risk population with pharmacy-provided ToC occurring at multiple points in the patient’s hospital stay and continued in the outpatient setting. This circle of care has not been previously described in the HF pharmacy literature. By working together with a focus on optimal patient care, the results of our efforts appear greater than the sum of its parts. Prior to the institution of our PPM, activities that promoted quality ToC for our patients were limited to admission medication reconciliation and provision of a documented ToC note by the pharmacist to the next provider at time of hospital discharge. By justifying one additional FTE pharmacist position in the outpatient clinic and reconfiguring an ICU pharmacist position to allocate dedicated time in the CTU, our PPM has extended pharmacist oversight to include targeted medication assessments on admission, pre-operatively, intra-operatively, post-operatively and on a routine outpatient basis. Moreover, ToC communications from the outpatient to inpatient pharmacists allow for more timely and accurate medication reconciliation at the time of patient admission. Although not measured in this descriptive study, high quality ToC in HF populations has been shown to increase the odds for lower 30-day all-cause readmission rates. 10 Our descriptive study did not include a comparator group prior to implementation of the model such that we could not measure a change in readmission rate post-implementation. Moving forward, our goal is to further measure the impact of our ToC activities on avoidance of medication errors, delays in medication access and possibly readmission rates.
Conclusion
Our PPM was developed to address gaps in care in an Advanced HF/OHT patient population specifically in the areas of medication access, medication education and ToC. As opposed to a longitudinal model of care, our circle of care involves multiple points of contact and communication between inpatient and outpatient pharmacists and a specialty pharmacy technician working synergistically within a larger multidisciplinary HF team. Inclusion of this pharmacy team in the multidisciplinary Advanced HF/OHT team has resulted in improved drug access, improved medication education with ToC at multiple points in the care process, and revenue generation as demonstrated by outpatient prescription volume. This PPM can be applied to not only patients with heart failure and OHT but to other patient populations. Collaboration between pharmacists and technicians working in inpatient, outpatient and specialty pharmacy settings is encouraged to provide complementary care to high-risk patients. Our PPM is applicable to numerous patient populations of chronically ill patients having high readmission rates and requiring costly, complex medication regimens.
Footnotes
Acknowledgments
We acknowledge the significant contributions of Lam Huynh, CPhT- Adv, Prior Authorization Specialist, to our complementary pharmacy team for the Advanced Heart Failure/Transplant Program at Tufts Medical Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.