
Abstract
Introduction
Influenza vaccination campaign takes on particular importance in times of COVID-19 pandemics. A massive vaccination campaign would help “to minimize the viral reservoir in the population” 1 and facilitate care delivery in a pandemic context. 2 Health Canada ordered 13 million influenza vaccines as part of public immunization programs for the 2020-2021 season, almost 2 million more than the previous year.3,4 In Quebec, an increase of nearly 25% in orders is also noted. 4 Due to the pandemic, the Ministère de la santé et des services sociaux du Québec (MSSS: Department of Health and Social Services of the Province of Quebec) highly recommended achieving 80% vaccination coverage in high-risk groups (Internal communication - Letter Dr Arruda Quebec National Public Health Director-June 15, 2020). To this end, the regional public health directorates had established “strategies aimed at better targeting and reaching out chronically ill patients”.
The Programme d’immunisation du Quebec (PIQ: Quebec Immunization Program) against influenza defines people at risk of complications and people at risk of transmission (as defined by the MSSS - June 15, 2020). These targeted populations are the ones receiving the vaccine free of charge. In Quebec, amongst those criteria, adults older than 75 years and patients with chronic conditions such as asthma, diabetes or cardiac diseases are listed as priority. For 2020-2021, vaccination was also accessible free of charge for people aged 60 to 74 with no health issues (MSSS - June 15, 2020). These choices, determined by age and clinical profiles, somehow defined specific “vulnerable populations”. However, in addition to these individual health vulnerabilities, social vulnerabilities remain. In Canada, getting flu shots is associated with living in a city, having a high income and education, and having a family doctor. 5 Thus, social vulnerabilities would need to be considered to ensure equitable access to vaccination in addition to clinical vulnerabilities (6)
Enabling pharmacists to vaccinate is seen as an opportunity to improve access and health systems efficiency.7,8 In March 2020, Quebec’s National Assembly implemented Bill 31, giving pharmacists the right to prescribe and administer vaccines, including the influenza vaccine, within terms and conditions determined by the regulation. 9 In the province of Quebec, influenza vaccine coverage among adults living with a chronic disease has reached 39%, for a stated target of 80%. 10 In 2017-2018, only 13.2% of those aged 60 and over received their vaccine at the pharmacy via a nurse. 10 Will the involvement of pharmacists improve these statistics? Limited data informs us about the impact of vaccination by pharmacists, their integration into existing public initiatives and the equitable access to vaccination for people considered as vulnerable. 11
Therefore, our objective is to describe the participation of community pharmacists in the influenza vaccination in Quebec since the implementation of Bill 31,
12
which enables pharmacists to vaccinate. To better understand this participation, 3 aspects are developed: (i) description of this practice as a public health offer
13
; (ii) opportunities and challenges related to this new practice; (iii) impact on equitable access for vulnerable populations.
6
These aspects are based on a theoretical framework that combines the analysis of Community health partnerships
13
and the question of equity (6) in access to public health care, see Figure 1. As Braveman highlights in her framework,
6
health disparities and equities should be analyzed with the lens of social positions in all aspects of health care, such as the allocation of resources, how they are utilized, distributed and financed to better shape health policies. We assumed to ensure health equity (6), strong community health partnerships must be fostered aligning environment forces, governance strategies and partnership capabilities (13) . These frameworks6,13 informed the study design, interview guide and qualitative analysis. We focused on the process on how community pharmacists determine the access of the influenza vaccine to the general population, especially regarding the services offer, the challenges faced, and how this offer was linked to public health partners in the territory.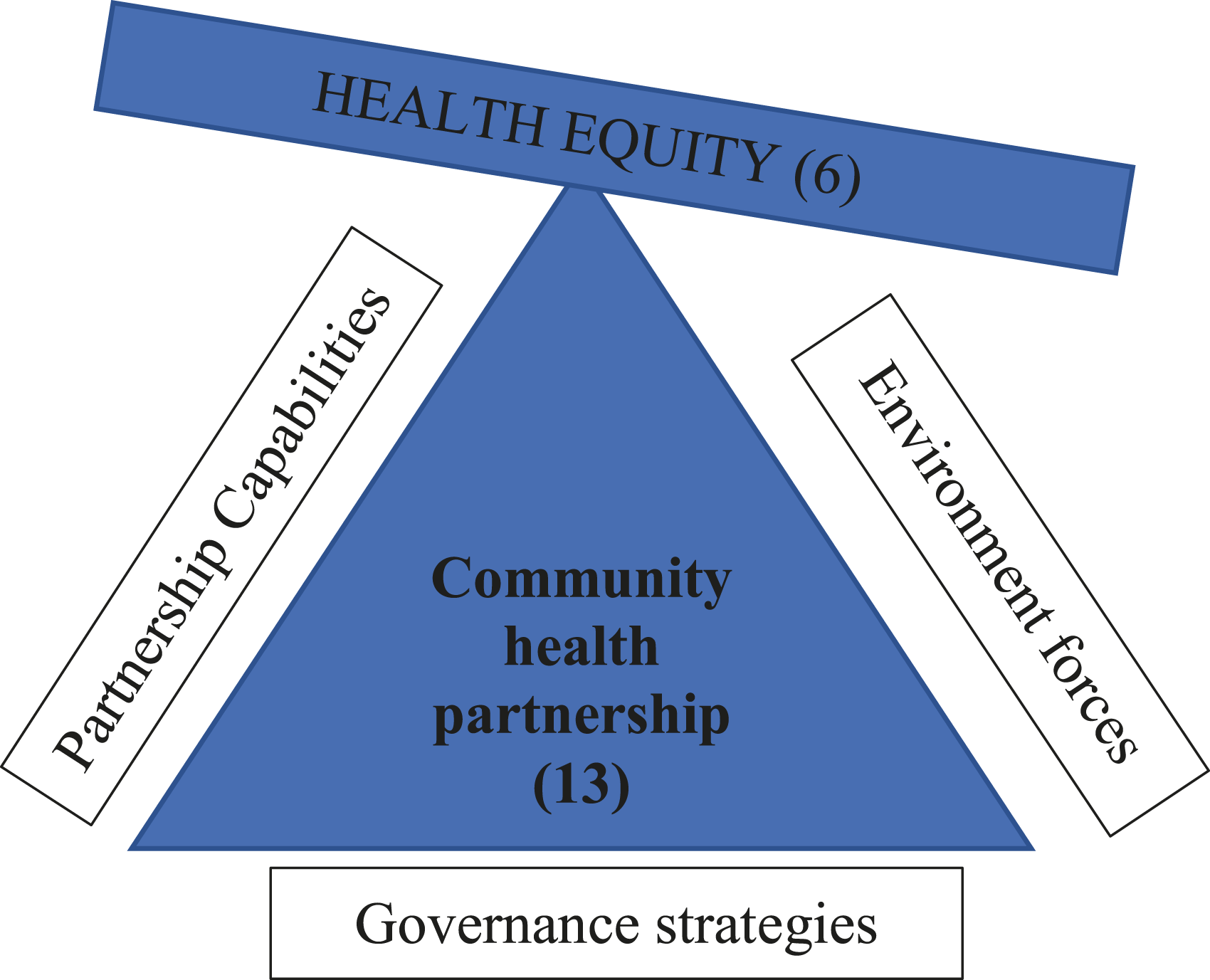
Methods
Case Study
An exploratory qualitative approach led to a case study in of 1 of the territories most affected by COVID-19 in Canada: Laval. In July 2020, Laval was at the height of the epidemic, in second place in Quebec, with a rate of 1,342.1 confirmed cases per 100,000 inhabitants. 14 In terms of mortality, the city ranked just after Montreal. 15 Laval health territory has a centralized structure called the Laval CISSS (CISSS: Integrated Health and Social Services Centre). As in other CISSSs, the regional public health directorate is a sub-department under the Chief executive of the CISSS and coordinates the regional influenza vaccination campaign.
Data Collection
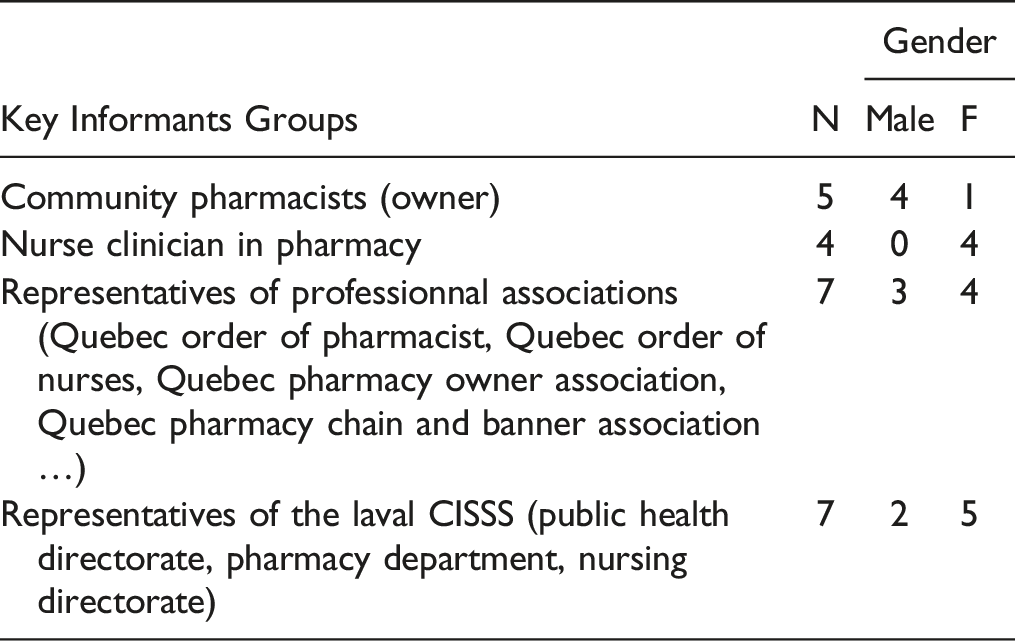
Data were collected using semi-structured interviews towards 4 groups: (1) Community pharmacists, (2) Nurse clinicians working in community pharmacies, (3) Representatives of professional associations and (4) Representatives of the Laval CISSS. Community pharmacies were identified by the Laval regional public health directorate. From an initial list of the 90 pharmacies, a convenience sample of 20 was contacted by email or telephone invitation in order to balance the participant’s location and type of pharmacy (banner or independent). 30% of emails or telephone invitation were answered. Representatives (Quebec Order of Pharmacist, Quebec Order of Nurses, Quebec Pharmacy Owner Association, Quebec Pharmacy Chain and Banner Association, Laval CISSS regional public health directorate, Laval CISSS pharmacy department, Laval CISSS Nursing directorate) were recruited using a sample of experts and a snowball method. All key informants contacted accepted to participate in the study.
Data collection took place from June 1 to August 20, 2020. In total, 23 semi-structured interviews were carried out in French, by first authors (PMD, AR) with 5 pharmacists 4 pharmacy nurses, 7 representatives of professional associations and 7 representatives of the Laval CISSS. All interviews were recorded and done by ZOOM or over the phone, after receiving each participant signed consent form. The interviews lasted between 30-60 minutes. Ethics approval was issued by the Université de Montréal.
Data Analysis
The interview grid (see Appendix 1) included questions on the roles of different actors towards this new vaccination practice (pharmacist participation), the vaccine supply circuit, opportunities linked to the implementation of vaccination practices in community pharmacies, support received by public health authorities and their business approach. The data collection and analysis were done simultaneously (PMD, AR). Interviews were fully transcribed. Interviews were coded using Dedoose qualitative data analysis software. The data was analyzed with thematic analysis. 16 Inductive initial coding was done independently by 2 team members and was systematically reviewed and discussed by team members. This iterative process stopped when no new themes emerged from the interviews, ie when the data was saturated. The data was grouped into 3 major categories in relation to our theoretical framework: offer description, opportunities and challenges of pharmacists’ vaccination, and public health perspective, ie impact on equitable access.
Findings
Influenza Vaccination in Community Pharmacies for 2020-2021
Changing Strategies
Unlike previous years, the community pharmacies no longer need to be certified as a vaccination site. Until Bill 31, the Regional Public Health Department had to recognize a pharmacy as being a vaccinating pharmacy so that it could offer public doses via a registered nurse, which required a number of procedures and administrative steps: registration as a vaccinating site, updating of information, transmission of the temperature register, table of vaccination statistics, register of unused doses to be destroyed when expired. Regional Public health no longer manages the supply of vaccines to the pharmacy. The supply now goes directly through private drug wholesalers, regardless of the type of dose (free vaccine-public dose- or paying vaccine-private dose). The supply by the regional public health directorates posed a problem because there was no uniformity in the criteria, there were downright regional directorates who did not want to distribute them in pharmacies, entire regions. And there were others who favored certain pharmacies over others. (Representative of professional association - No.4)
Changing Capabilities
For 2020-2021, just over two-thirds of Quebec pharmacists anticipated offering influenza vaccination, a percentage similar to other provinces.
17
However, as of July 2020, only around 20% of Quebec pharmacists had trained to become a vaccinator (interview No.11). It’s not something that pays off so we won’t say “we drop everything and we do vaccinations”. We wouldn’t make enough profit from that. (Community pharmacist - No.6)
According to respondents, to enhance the number of pharmacists able to immunize, some institutional changes have been promoted—for instance, the end of the certification obligation for health institutions. Also, the MSSS offered a special grant to encourage pharmacists follow the mandatory trainings free of charge (until January 22, 2021).
Competing Environment Forces
The MSSS also modified the supply of vaccines. It is now left in the hands of pharmacists, via private wholesalers, for all types of doses (public or private). As of August 25, 2020, for all Quebec, approximately 650,000 public doses and 100,000 private doses had been pre-ordered by community pharmacies, compared to 400,000 (200 000 public and 200 000 private) the previous year.
Indeed, as in previous years, influenza vaccination in community pharmacies remained at the discretion of the pharmacy owner (the choice to offer vaccination or note, the choice of the vaccinator (registered nurse or now, pharmacist), number of doses ordered, public/private ratio, vaccination modalities). This questions the relationship between public and private management of vaccine supply. We’re going to order it. I’m going to try it, but we’ve never done it. It is complicated to order a vaccine, with public health. I’ve been talking to other owner pharmacists for years, I’m on Facebook groups, I see messages, and I see how complicated it is., They don’t receive the vaccines, they order 200 doses and they make appointments and in the end, they only have half. I didn’t feel like getting into it. So this year, we have a bit of a choice to get on board, at some point we have to add grist to the mill to move forward. So, I said to myself we’re going to try it, I’m going to try myself and we will see. So we are going to see how we will receive the vaccines. My concern was that, that it is too complicated. Now via wholesalers it’s much simpler. (Community pharmacist - No.8)
The Laval Regional Pharmaceutical Care Committee (CRSP) is a structure specifically dedicated to the coordination of pharmaceutical activities with the rest of the services in the territory. As a result this committee should have been an important place of discussion and decision making between public and private interests. As for the CRSP, it is to consider that it does not exist. It’s as if nothing existed. We don’t have the resources to make this committee work. In hospital pharmacies, they don’t have time for this. This is time that will be taken away from the clinic if they come to a meeting. In return, we are paid, but there is no time allocated for that. So like in the hospital, it’s difficult on our side. Honestly, when it comes to exchanging information with social networks, Facebook, there are plenty of groups of pharmacists everywhere, at some point we say to ourselves “really who is it for and for what?”. Currently, with the pandemic it puts everything in the coffin. So, for the moment the CRSP is in a coma. I hope he will be revived. (Community pharmacist - No.8)
According to the participants, the CRSP does not seem to have any real power over the organization of the vaccination campaign and the mobilization of the actors, having little or no resources to operate. As a result, there is no real institution of dialogue between public and private management of vaccination in this territory.
Opportunities and Challenges to Vaccination in Pharmacies
The actors interviewed, such as Laval public health respondents, perceive vaccination in community pharmacies as an “opportunity” (Internal communication - Note from 2017) to reach vulnerable groups, such as patients with chronic illnesses. Community pharmacists who vaccinate also said that it can improve vaccines’ accessibility and, more generally, influenza prevention. Community vaccinating pharmacists agree with this conviction of public health professionals that vaccination in pharmacies can make it possible to carry out more proactive prevention and prevention that focuses on accessibility for the benefit of the patient: Pharmacists know their patients. When they are going to give a medicine, they can say « ah I see you have diabetes, I can recommend that you also make an appointment for influenza ». Therefore they can maximize this kind of opportunity, to do prevention and to be more proactive… (Representative of professional association - No.11)
On the other hand, commercial interests are also mentioned as 1 advantage of this practice. Pharmacists, chains and banners seemed to find here an opportunity to enhance the commercial influence of community pharmacies. Among other things, with loyalty programs that exist at certain retailers, there is a way to see, depending on what products the person buys, to be able to detect that the person may be suffering from a chronic illness or has a certain age. To be proactive in targeted promotional campaigns to reach the right clientele through vaccination. So there is a capacity that the private sector and the chains and banners have that we may not find for different reasons in the public sector… (Representative of professional association - No.11)
Offering the flu shot for free to people who would transfer their records to the community pharmacy has been reported off the record. However, this business interest canbe nuanced. Some pharmacists indeed perceived vaccination as a way to anchor the profession in a global public health offer, in particular through prevention. So the income that was associated with it, for me, it was incidental because I really do it from the social perspective of maximizing vaccination and meeting the needs of my clients. So no matter what income I could have had, I see it a bit like visibility for pharmacy and health. So that’s why, no matter what I would have received, I would still have gone into the adventure. (Community pharmacist - No.6)
Lastly, vaccination by pharmacists allows freeing nurses from this task, particularly in the context of the COVID-19 pandemic. Some respondents (from the pharmaceutical sector and decision-makers) suggested that this would improve nurses' availability, for example, in long-term care facilities, who were very affected by the pandemic in this territory. Some other respondents also predicted that soon, licensed practical nurses would be authorized to vaccinate under the pharmacist’s supervision or the pharmacy nurse (which the MSSS confirmed in August 2020). These licensed practical nurses would then constitute a less expensive workforce, making vaccination in community pharmacies more profitable.
Public Health Perspective: Impact on Equitable Access for Vulnerable Populations
According to pharmacists' representatives, pharmacists are aware of vulnerable populations within their clientele (including patients with chronic illnesses). The fact that pharmacists would be in the best position to target patients requiring an influenza vaccine is an argument favouring their involvement and often mentioned by respondents. On the other hand, other factors, such as poor access to these types of information via the Quebec Health Record, might constitute barriers to identifying these vulnerable populations. Access to the drug profile makes it possible to see if the person is part of the ‘vulnerable clientele’. However, it is not possible to quickly and easily see if the patient has already been vaccinated or not in the Quebec Health Record profile… It is certain that everything is registered in the Vaccine Register, except that it is not easy to consult this thing. (Representative of the Laval CISSS – No.15)
Targeting chronically ill patients or other vulnerable populations (older adults, for example) to grant appointments does not seem to be implemented yet. Faced with a heavy workload, the respondents mentioned that they will even opt for a “first come, first served” approach. We will announce it, word of mouth too, employees will talk to patients. Every year, I have dozens of patients who ask me if we vaccinate for the flu. So again this year, they will surely ask and there, I will be able to say yes. I wouldn’t make appointments until I had the vaccines in hand, that’s for sure. (…) However, in the end, the fact remains that appointments are made on a “first come, first served” basis. (Community pharmacist - No.7)
Indeed, several respondents seem to have been scalded by their previous experience, including delivery concerns, which led to the cancellation of appointments. In the pandemic context, pharmacists are thinking of favoring a “small steps” approach to learn from this year’s experience and ensure minimal success for this vaccination campaign instead of making a risky business decision.
Discussion
A Strategy That Cannot Assure Equity yet
Pharmacists’ involvement in vaccination is recognized to improve vaccination coverage, 18 particularly its equitable access for certain vulnerable populations. 19 However, professional engagement 20 and conditions for this improvement are rarely described. Improvement in the structure of the vaccination campaigns, within a public health perspective, seems necessary as no initiatives to ensure equitable access have been shown in our results. Pharmacists, as an additional workforce to vaccination campaigns, should be considered as to what extent they will reduce - or not - inequalities and target vulnerable populations. Their involvement goes beyond a technical intervention; it involves a set of strategies and their integration into a coordinated public health response. “First come, first served” is a strategy that at first glance strengthens equality. However, not all patients are equal when it comes to – for instance, influenza vaccination. Influenza vaccination is associated with some determinants (socioeconomics and clinical ones) 5 that do not seem to be considered yet in the strategies reported by our respondents. This appears to limit the public health impact of vaccination by community pharmacists. Pharmacists maintain personal relationships with many patients by building trust through repeated encounters, thus proving a unique opportunity to take on an advocate role. 21 Indeed, regarding Braveman’s definition of equity, as taking into account disparities, pharmaceutical services of vaccination do not favor equity yet. Further research on how to better address health inequities in pharmacy should be led. This seems feasible considering the amount of data gathered in the pharmacy files, but do pharmacists really have access at those informations in real time practice? These questions remain to address in order to have an intervention which would take into account equity.
Increasing general population access to vaccination does not automatically increase the proportion of the vulnerable population vaccinated. Accessibility is also poorly studied in the context of pharmacy. Although most studies focused on realized accessibility (the health care services that an individual receives) rather than on financial or vaccine availability. 22 The systematic review from Spinks et al highlights the high variability of pharmacists’ contribution on influenza vaccination rates in older adults (.4-11%). Pharmacists in jurisdiction with the most autonomy demonstrated higher uptake. 23 The promoted strategy could, on the contrary, reinforce social inequalities by protecting the most socio-economically advantaged ones. 6 On a governance level, Laval’s public health Directorate has no authority over the community pharmacies of Laval, which develop their own strategies or the one of their banner. Therefore, the vaccination campaign is in the hands of community pharmacists, who are private actors. No institutional and public health coordination is provided because of these structural issues. This reality constitutes a major limitation to community health partnership 13 that weaken structured vaccination offer dedicated to promoting equitable access.
Limited Community Health Partnership
A local public health management capacity, in partnership with community pharmacies, seems, therefore, necessary. 24 The role taken by pharmacist’ and the success of their interventions will vary according to the policy aim, whether it is to increase vaccine uptake, target specific groups, maintain or enhance documentation of vaccination status et to reduce immunization costs. 23 Some institutional structures already exist, including the Regional Pharmaceutical Care Committees (CRSP), dedicated to coordinating pharmaceutical activities with other health services in a given territory. But this CRSP did not receive a clear mandate nor specific power or resources in this area. A strong mandate would be essential to facilitate links between public and private vaccination, especially in the context of historical tensions between the public health Directorate and community pharmacists. In the end, old recommendations - dating back more than 10 years - for better coordination between community pharmacies and public health institutions remain relevant, 25 even more if pharmacists are to be involved in COVID-19 vaccination.
This study has limitations. This study was carried out within very short deadlines related to the pandemic context and legislative uncertainties; further research will be needed to document an offer of pharmaceutical vaccination services that is in the process of being structured. The response rate of community pharmacists was 30%, which may have overrepresented highly engaged pharmacists. Vaccination in community pharmacies in the province of Quebec is an emerging practice, still in the process of being defined. This is 1 of the first study on vaccination in community pharmacies in the province of Quebec. Admittedly, this is a study on a specific territory, Laval, but this study is nonetheless revealing the effects of provincial regulation on vaccination in community pharmacies and public health issues. Moreover, the choice of the theoretical framework adapted from Braveman(6), and Mitchell and Shortell 13 of this study is unique. Anchoring the issue of health equity in governance and community partnerships makes it possible to analyze the implications of legislative change beyond a change in professional practices. Further studies are needed to continue to assess the impact of this new regulation.
Conclusion
In conclusion, vaccination seems to be an excellent opportunity to build closer partnerships between community pharmacies and public health institutions, improving equitable vaccination coverage. This study highlight a common strategy used by community pharmacist to give access to the population: first come, first served. It reveals a lack of alignment in the partnership between the governance, the capabilities and the strategies. The lack of public health perspective regarding vaccination campaigns could constitute challenges to carry them out and address health inequities. These issues should be urgently seized as the COVID-19 pandemic waves revealed the importance of these partnerships to improve health systems' efficiency. 1 Future research would need to understand better the association between some determinants and access (or not) to vaccination 26 and to analyze better coordination between public health actors and community pharmacists for interventions such as vaccination. More elaborate, and by extension more equitable, targeting strategies could thus be developed to meet better the population’s needs in terms of vaccination, whether towards influenza or COVID-19.
Footnotes
Author Contributions
PMD; responsible for design and methodology:
PMD, AR; supervised project:
PMD and AR; reviewed final draft:
PMD, LM, ED, MG, AC;
wrote final draft: PMD, AR; translated: MG.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chaire Sanofi-Aventis en soins pharmaceutiques ambulatoire de l'Université de Montréal.
Interview Guide
Pharmacist Owners (adapted for other health care personnel or professionals)
Characteristics: Number of years of experience; Number of prescriptions per day in the pharmacy; Number of pharmacists/technicians (1) Can you briefly introduce yourself, your pharmacy settings and its specificities? (2) How did you come to offer (or not) immunization services in your pharmacy? • How did you adapt the operations of the pharmacy? • What training have you provided, internally and externally, to offer this service? • What is the importance of this service for your clientele? Is the vaccine a drug like any other? For the image of the pharmacy? • What advantages does the flu vaccination bring to vaccination in general? (3) How does the vaccination service work in practice for the patient? • Who offers it? • How much does it cost? • How is the vaccine administered? • How is the follow-up done? • Benefits/risks (4) How does the pharmacy provide vaccination? • Who orders the vaccines? • How much does it cost? • How do you target patients? • What are the procedures to explain to patients? • How is the delivery done? • How is the follow-up done? (5) Are you always recommending vaccination? • examples of referrals to the physician? • examples of non-vaccination? (6) How do you perceive vaccination in relation to individual or collective health? • Address the issue of social responsibility: of the pharmacist, of the patient (7) How do you keep data on vaccines and vaccination? (8) Do you have access to epicentre, SI-PMI register? (9) How many vaccinations have you performed this year (2019-2020 season)? • unused doses? • return or destruction strategies? (10) What would be relevant elements to improve in relation to vaccination in your pharmacy? • interprofessional aspects? (11) What additional skills would you like to have in order to be more comfortable with immunization? (12) What changes to the organization of immunization in your pharmacy do you anticipate after Bill 31? (13) What are the key issues related to the pharmacist vaccinator? • remuneration, space, workload, management, burden, commercial importance…