
Abstract
Objective
The aim of this systematic review and meta-analysis of randomised controlled trials is to evaluate the impact of pharmacist-led interventions on cardiovascular disease (CVD) risk factors among patients with type 2 diabetes.
Keywords
Introduction
Diabetes mellitus (DM) is a chronic condition that can lead to complications and is increasing worldwide. 1 In addition, more than one-third of patients with T2D have a higher risk of mortality from CVD compared to those without diabetes. 2 Therefore, controlling the major risks for CVD, such as hypertension, dyslipidaemia and obesity, reduces long-term diabetes progression. 3 Hypertension and T2D are commonly associated with diabetes because they share severe risk factors, such as insulin resistance, obesity and stress. 4 As hypertension affects about 70% of people with diabetes, 5 the appropriate management of HbA1c and cardiovascular risk factors can substantially reduce complications. 6 However, despite published studies confirming that controlling statistics blood glucose levels reduces macrovascular and microvascular events, related to CVD risk factors among patients with T2D are alarming and remain poorly managed. 7 According to the International Diabetes Federation (IDF), diabetes is a major expense for individuals, society and healthcare providers. In 2017, the accounted cost was USD 850 billion globally and the expenditure is estimated to increase by 12.7% in 2045. 8 Even worse, the incidence of medication adherence ranged from 38% to 93%. 9 However, intensivecomplex interventions and effective models of diabetes care are required to maintain tight clinical parameters, improve quality of life and decrease healthcare costs.
Several studies have highlighted the value-added by the pharmacist in chronic disease management,10-12 for instance, improving diabetes care, CVD, hypertension and hyperlipidaemia. 13 The role of pharmacists is more than dispensing medications; it has shifted from a product-centred approach to patient-centred care. 14 Pharmaceutical care is defined as ‘the responsible provision of drug therapy to achieve definite outcomes which improve a patients’ quality of life’, 15 and the care provided by the pharmacist is an essential element for patient health. 16 The collaboration of pharmacists with other healthcare professionals to design, structure and implement a shared care plan is critical to ensure optimum health outcomes.17,18 Pharmacists can also provide appropriate care through patient education and improve communication between pharmacists, healthcare teams and patients, 13 when found to be acceptable by patients and physicians. 18
Moreover, pharmacists’ knowledge of diabetes therapy and the relationship between pharmacists and patients during prescription refills build trust, promote good healthcare and help patients attain the required outcome.19,20 Extensive international studies10,17,18,21 have assessed the effectiveness of pharmacist-led interventions in supporting individuals with T2D and CVD. The components of the pharmacist interventions varied between the studies and are divided into 4 categories including: • Educational interventions: educate patients about their condition and the medications offered by a pharmacist, nurse or other healthcare professional. The information is delivered to patients via phone, email, video and/or through individual or group sessions.
22
. • Behavioural interventions: assist patients in changing their lifestyle and attitude, including advice on smoking, diet and exercise.
23
• Psychological interventions: work directly on mood states such as anxiety, depression and stress. They aim to increase problem-solving using cognitive approaches to change their behaviours.
24
• Clinical interventions: work directly towards improving the use of medications by solving drug-related problems, such as drug interactions, side effects and drug duplication issues.
25
Diabetes self-management education considers the pharmacist an integral part of designing curricula, delivering diabetes care and teaching self-management practices. 26
Diabetes and the Risk of Developing Cardiovascular Disease
Addressing CV risk factors in T2D patients is essential to avoid further complications such as coronary heart disease (CHD), stroke and myocardial infarction (MI). 27 While CVD is the principal cause to death, lowering HbA1c alone is not enough to prevent or delay diabetes progression. 28 Therefore, complex interventions are in high demand and include complex therapy regimens comprising diet, physical activity, smoking cessation. Treating T2D is complicated and a challenge for healthcare providers. 29 Nevertheless, such treatment is crucial in reducing diabetes complications and cardiovascular risk factors and improving clinical outcomes and quality of life. The effectiveness of self-management education and techniques are well documented by pharmacists. 23 Increasing patients' awareness and through education that focused on their illness, complications related to diabetes and medications adherence; they also need to be encouraged to promote lifestyle modification such as exercise and diet plan, which are keys to disease management. 30 In addition, self-monitoring of blood glucose is a crucial tool in controlling T2D. 31 The purpose of this systematic review is to evaluate the impact of pharmacist-led interventions, in comparison with standard care, on HbA1c levels among patients with T2D and cardiovascular risk factors in primary care, diabetes clinics and hospitals.
Methodology
Search Strategy
We searched a comprehensive literature database using Embase, MEDLINE, CINAHL and Cochrane Central Register of Controlled Trials from inception to May 2020. The search terms included keywords and subject headings combined with Boolean operators: diabetes mellitus or diabetes mellitus type 2; cardiovascular disease or hypertension; clinical pharmacy or hospital pharmacist or pharmacy service or pharmaceutical care; and randomised control trials.
Inclusion and Exclusion Criteria
Studies were included in the review if they did the following: (1) they were RCT with comparable groups (pharmacist care compared to standard care groups); (2) they evaluated the impact of pharmaceutical care delivered by pharmacists either independently or in collaboration with the healthcare team; (3) the intervention was conducted mainly in hospitals, primary care clinics or diabetic clinics; (4) they targeted adults with T2D and hypertension or cardiovascular risk factors (compared to standard care); (5) they reported 2 or more clinical indicators, including HbA1c, SBP, DBP, fasting blood glucose, lipid profiles (LDL-C, HDL-C, TG and total TC), BMI and smoking and other outcomes, including medication adherence, health-related quality of life, 10-year CHD risk and the cost-effectiveness of the interventions; and (6) the full article was published in the English language. The exclusion criteria were non-English publications, conference papers, protocols and practice guidelines.
Study Selection
Data were extracted independently by 2 reviewers, who screened all titles, abstracts and full articles that were retrieved from the electronic databases. The full-text articles were obtained through the University of Bradford’s catalogue and open sources. The reviewers read the full papers independently before they were included, and any disagreement was solved by discussion.
Data Extraction and Synthesis
Each reviewer extracted the following data: (1) study characteristics (study design, setting, sample size, duration of follow-up and year); (2) characteristics of patients (uncontrolled T2D HbA1c >7% (53 mmol/mol) with modifier cardiovascular risk factors); (3) characteristics of interventions (including education, medication consultation, self-care assessment, intervention delivered by a pharmacist only or with other healthcare providers); (4) characteristics of the standard care group; and (5) clinical indicator measurements (including HbA1c, BP and lipid profile from the baseline to the end of the intervention).
Risk-of-bias Assessment
The Cochrane tool for assessing the risk of bias was used to evaluate the quality of the individual included studies. 32 The risk of bias identifies the following criteria: random sequence generation, concealment of allocation, the blinding of participants and personnel, the blinding of the outcome assessment, selective reporting and other sources of bias. Due to the nature of delivering the intervention for the included studies, the healthcare personnel could not be blinded. For each factor, the bias risk was rated as low, unclear or high. Two reviewers double-checked this assessment, and any disagreements were discussed until a consensus was reached.
Data Analysis
Statistical analyses were conducted following the recommendations of the Cochrane guidelines. For continuous data, the SBP, HbA1c and LDL-C results were pooled in a meta-analysis. Review Manager 5.3 (RevMan) software was used to analyse and produce forest plots using a random-effects model due to clinical heterogeneity across the studies. The heterogeneity of the studies was assessed using I2 and the P-value.
Results
Study Characteristics
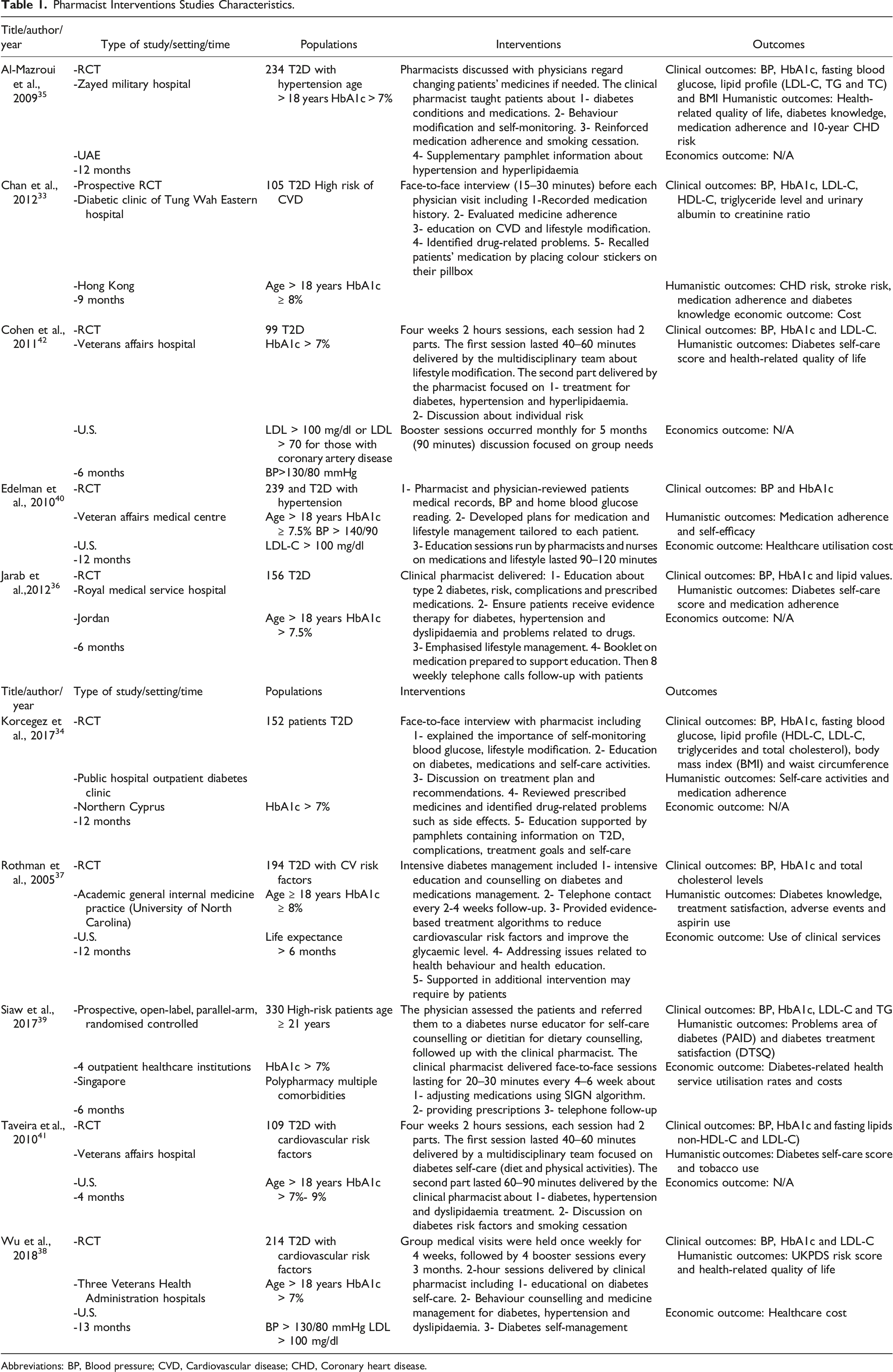
As shown in Figure 1, a total of 448 studies were identified from the electronic database searches. After screening the titles and abstracts, 141 potentially relevant studies were assessed for eligibility, with ten studies being identified as meeting the inclusion criteria. The excluded articles and reasons for exclusion are stated. The included studies were RCTs in different settings and countries that targeted patients who had been diagnosed with T2D and had CVD and cardiovascular risk factors. Participants were followed up in hospitals, primary care clinics, diabetic clinics or health centres. Out of ten studies, 5 were conducted in North America (United States), 2 in the Middle East (United Arab Emirates and Jordan), 2 in Asia (Hong Kong and Singapore) and 1 in Europe (Cyprus). The included studies’ characteristics are presented in Table 1. Flow diagram of the literature search process (PRISMA 2009 Flow Diagram). Pharmacist Interventions Studies Characteristics. Abbreviations: BP, Blood pressure; CVD, Cardiovascular disease; CHD, Coronary heart disease.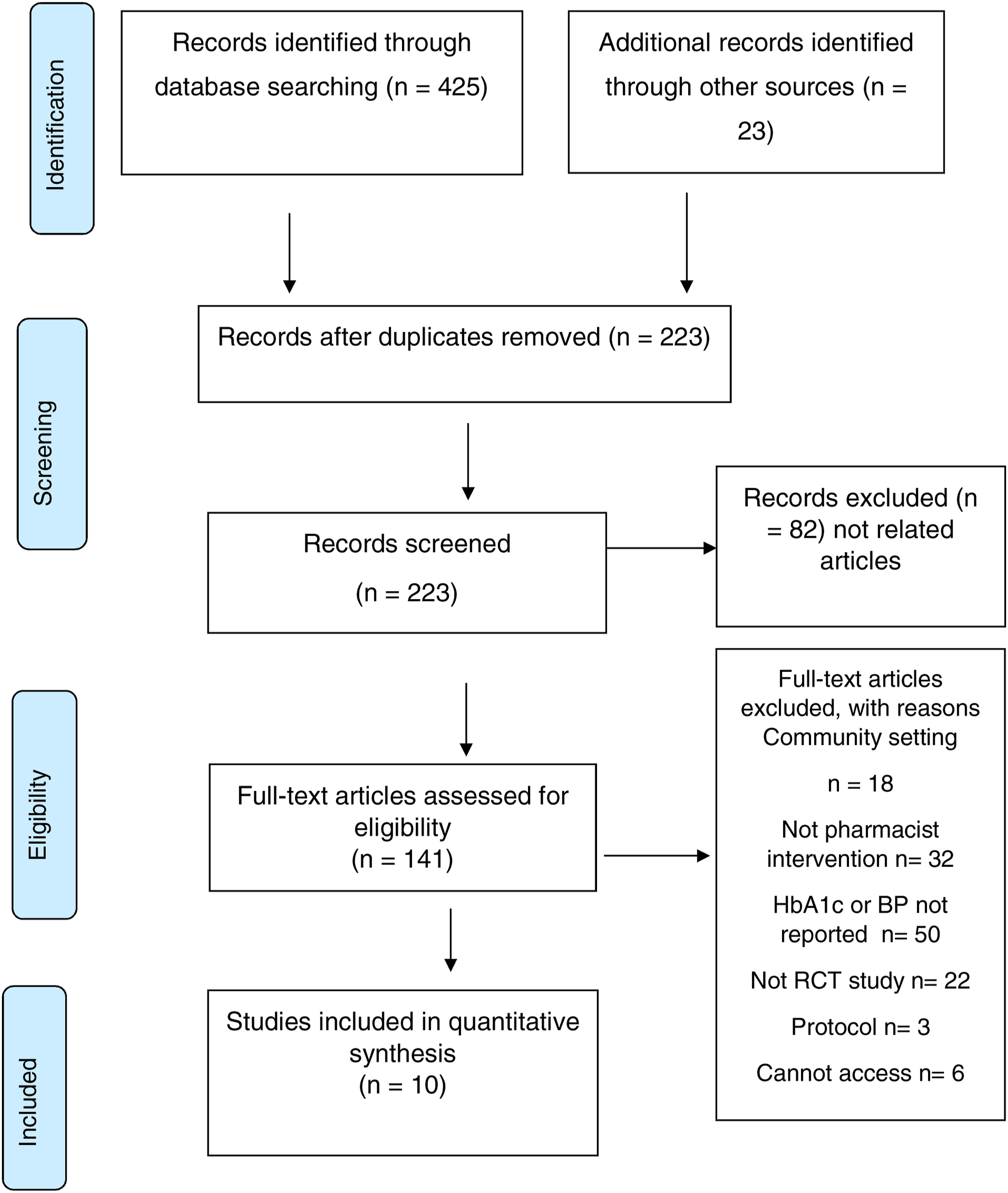
Description of Included Studies and Type of Intervention
The interventions were delivered by the pharmacist either directly33-36 or collaboratively with other healthcare professionals, such as a specialist nurse, diabetes educator or dietitian.37-42 The follow-up duration ranged from 4 to 13 months. The nature of the pharmacist intervention for each study is presented in detail in Table 1.
Quality of Included Studies
The risk-of-bias assessment varied among the included studies, as illustrated in Figure 2. All studies used adequate methods for randomisation, and 9 studies contained insufficient information about allocation concealment. No participants were blinded to the intervention due to the nature of the research. Blinding the outcome assessment was discussed, and incomplete outcome data were reported as low risk because an intention-to-treat analysis was used in all studies. The outcomes were unclear in 2 studies, and other biases testified as an unclear risk in 9 studies. Cochrane risk-of-bias tool for randomised controlled trials.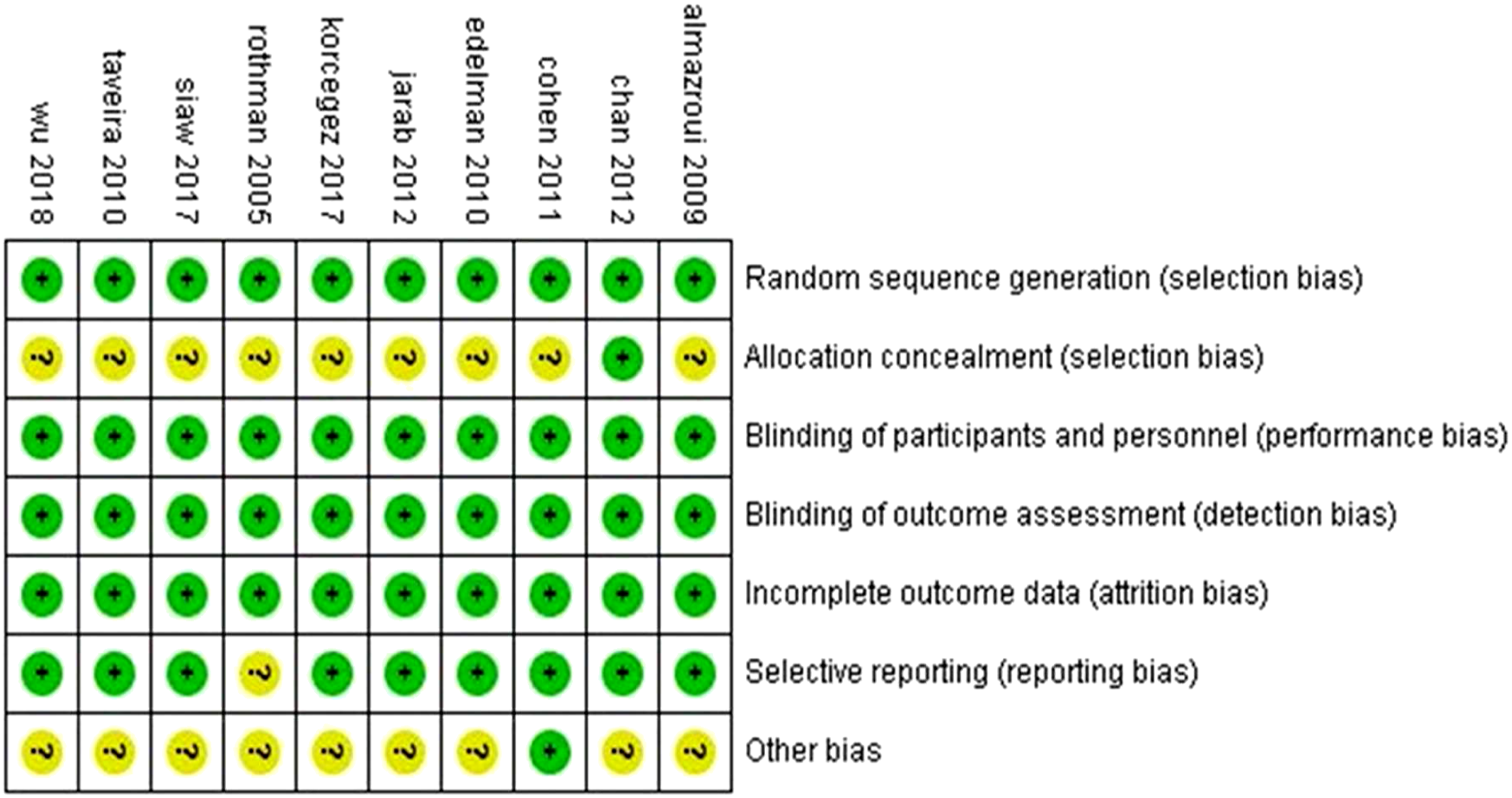
Study Outcomes Measures
All the studies considered HbA1c as an outcome for their interventions.33-42 The mean value of HbA1c at the baseline was 8% across the studies. The pooled analysis indicated that the intervention group showed a significant reduction in HbA1c (SMD −.53, 95%; CI: −.84, −.23) (Figure 3A). However, 6 studies reported a positive effect and 3 a slight improvement associated with pharmacist care. Whereas 1 study revealed no difference between the groups (95%; Cl: −1.88, −1.32).
43
It was noted that T2D patients with HbA1c >8.5% greatly benefited from pharmacist intervention, as it reduced by .3%–1.6% (95%; Cl: –1.88,–1.32). Pooled results (meta-analyses). (A) Meta-analysis HbA1c. (B) Meta-analysis SBP. (C) Meta-analysis LDL-C.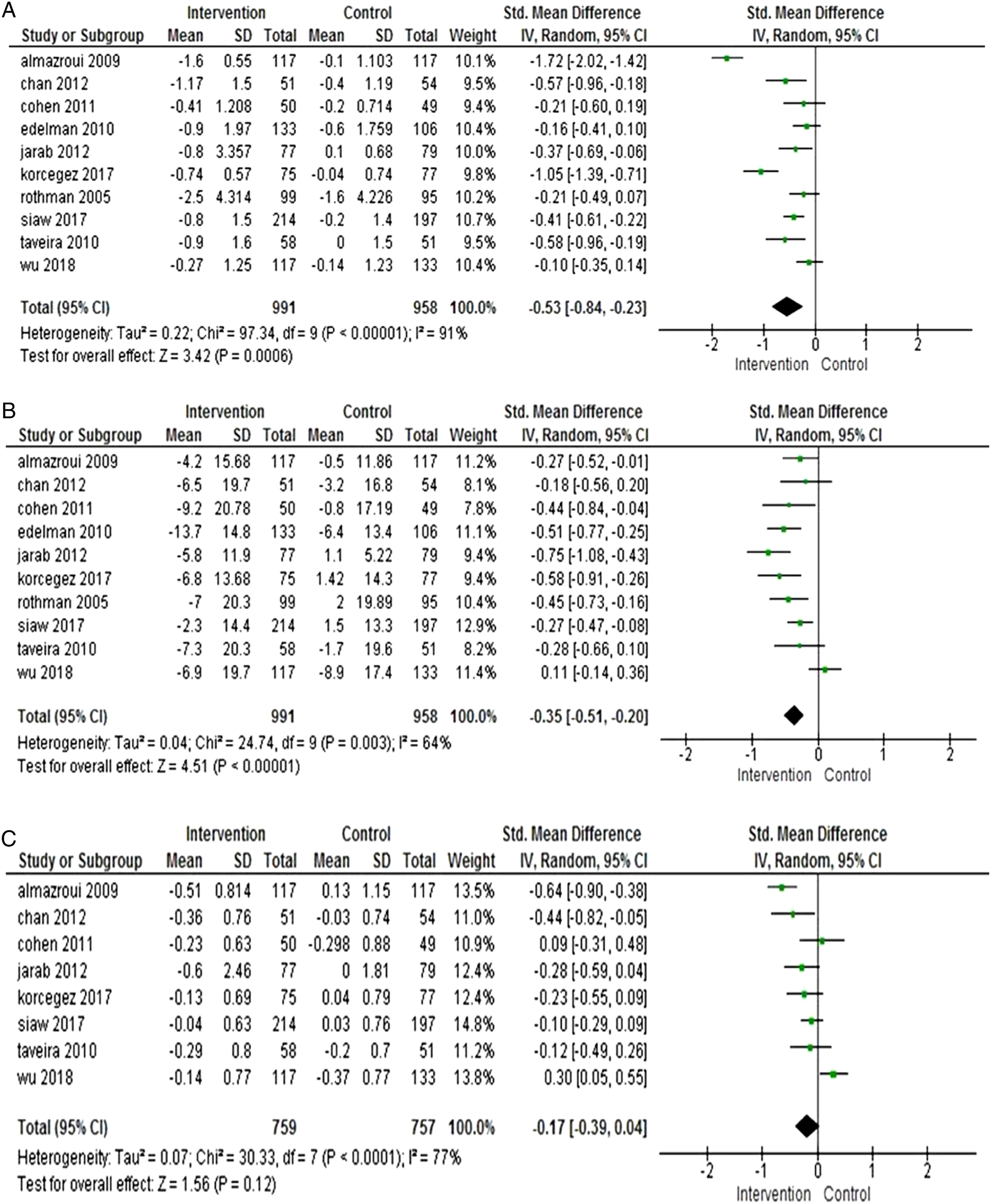
Three studies analysed fasting blood glucose.34–36 Korcegez et al. 34 found an improvement in fasting blood glucose in the intervention group compared to the control group (intervention group –1.7 mmol/L, control group –1.3 mmol/L). Al-Mazroui et al. 35 and Jarab et al. 36 reported a significant reduction in the intervention group compared to the control (intervention group –3.01 mmol/L, control group –.78 mmol/L). (intervention group –2.3 mmol/L, control group +.9 mmol/L), respectively. The pooled analysis revealed a significant reduction under pharmacist care compared to standard care (standardised mean difference –.61 mmol/L, 95%; CI: –.78,–.43).
Systolic blood pressure (BP) was measured in all studies. In total, 9 studies revealed a significant reduction in SBP in the intervention group at the end of the research in contrast to Wu study. 38 Pooled analysis indicated a significant reduction in the intervention compared to the control group (SMD −.35 mmHg 95%; CI: −.51, −.20) (Figure 3B). Seven studies also measured the diastolic 36 blood pressure and reported a reduction of approximately 2.8 mmHg in the intervention group. Pooled results indicated a significant reduction with the intervention group (SMD −.57 mmHg 95%; CI: −.69, .45).
Lipid profiles levels varied across the studies. LDL-C measurements were found in 8 studies.33-39,41,42 The pooled analysis reported nonsignificant results between both groups (SMD −.17 mmol/L; 95% CI: −.39, .04) (Figure 3C). Four studies measured HDL-C, and the pooled result showed (SMD −.01 mmol/L; 95% CI: −.09, .06). Triglyceride (TG) levels were measured in 4 studies revealed no significant difference between groups (SMD .39 mmol/L; 95% CI: −.84, .07). In total, 5 studies reported total cholesterol (TC).33,34,36,41 The pooled analysis estimated a significant reduction in the intervention group compared to the control group (SMD –.45 mmol/L, (95% CI: –.79, –.12).
Four studies measured the body mass index (BMI).33-35,41 The mean value of BMI was lowered by 1 kg/m2 from the baseline to the endpoint in the intervention groups. At the same time, the BMI value increased by .4 kg/m2 in the control groups. pooled analysis documented a reduction under pharmacist care (standarised mean difference –.26 kg/m2 ; 95% Cl: –.41, –.1).
The United Kingdom Prospective Diabetes Study (UKPDS) risk engine, CHD risk and stroke risk scores were found in 4 studies. They calculated the estimated risk factors in T2D patients. The CHD score was reported in 2 studies33,35 using Framingham, British National Formulary and a validated cardiac risk score that is specific to the Hong Kong population. Both results showed a statistically significant reduction in CHD risk scores during the study in the intervention group compared to the control group. In addition, the stroke risk score in the intervention group decreased. 33 Finally, UKPDS was recorded in 1 study. 38 The mean change in the UKPDS coronary events risk was reduced significantly in both the intervention and control groups.
Medication adherence was assessed in 6 studies33-36,40,42 and measured using the Morisky self-reported scale. There was no difference in medication adherence between the groups in the 2 studies.36,40 Two studies34,35 used the Morisky–Green test and self-reported adherence questionnaires and found a significant increase in pharmacotherapy adherence in the intervention group. One study used a medication possession ratio and found an insignificant difference between the comparison groups. 42 A final study 33 used an equation to calculate medication adherence, which improved the compliance score following intervention to 96.0% compared to the control group at 84.1%. An additional one 42 reported nonsignificant results with medication possession ratio. Pooled analysis indicated a significant results with pharmacist intervention group (SMD 18.14%, 95% CI; [13.05, 23.23]).
Three studies33,35,37 demonstrated the level of diabetes knowledge regarding the purpose of using medicines in T2D. The studies showed improvement by 20% in diabetes knowledge for patients who received the pharmacist intervention (SMD 55.68%, 95% CI; [33.67, 77.68]).
The health-related quality of life was reviewed in 3 studies35,38,42 using the SF-36 questionnaire. There was no difference between the 2 groups in the 2 studies.38,42 The mean change was −.02 + .9 vs −.4 + .09 and 2.13(95% Cl) vs 2.73 (95% Cl), respectively. The third study 35 reported improved health-related quality scores with the intervention patients, whereas those in the control group remained unchanged. Pooled results scores were SMD .15, 95% CI; [−.22, .51] for physical and SMD 1.35, 95% CI; [.55, 2.16] for mental.
Diabetes self-care scores were reported in 4 studies.34,36,41,42 Diabetes self-care comprised diet, physical activity, self-management of blood glucose (SMBG) and foot care. The studies noted a slight improvement in the intervention group compared to the control group in the overall score. One study revealed that the total self-efficacy score was significant with the pharmacist interventions SMD 1.6, 95% CI; [.9, 2.4]. The 3 studies observed a slight improvement of 2 to 3.8 out of 5 points in the intervention group compared to the control. The achievement was mostly in diet, SMBG and foot care. Pooled results were SMD .24 [−.06, .54] for general diet, SMD .26, 95% CI; [.06, .45] for physical activity, SMD .31, 95% CI; [.08, .54] for SMBG and, SMD .69, 95% CI; [−.32, 1.70] for foot care.
Cost calculations were reported in 4 studies.33,38-40 Pharmaceutical care was found to be more cost-effective in 3 studies. Furthermore, there was an incremental reduction in healthcare utilisation for the patients under pharmacist care compared to standard care (USD 4220 ± 31 091 vs 5752 ± 29 690), 38 USD 5,086 for preventing CHD events, 33 and (USD 516.77 ± 222.1 vs 607.78 ± 268.39) for outpatient diabetes-related care 39 ; and (USD 460 vs 504) for education sessions, 40 respectively.
Discussion
This systematic review demonstrated that pharmaceutical care programmes positively influence clinical parameters, health-related quality of life and health costs when T2D is poorly controlled. The pharmaceutical care programmes in the identified studies focused on 3 fundamental concepts: (1) -Medication management included reviewing medicines, explaining drug-related problems, monitoring therapy progress, adjusting dosage and optimising administration. (2) -Disease management included education, counselling and using evidence-based care algorithms. (3) -Advice on lifestyle modification, such as self-care practice skills and training, self-management education and encouragement on a healthy diet and smoking cessation.
Despite the diversity in pharmacist-led interventions, they all aimed to improve the clinical outcomes and quality of life among patients with diabetes. The pharmacist interventions were delivered in 2 ways, either individually or in group sessions, performed by pharmacists only or with the healthcare team collaboratively.
Reduction in HbA1c, lower BP and better lipid profiles were associated with pharmacist involvement in patient education, consultation and follow-up. Previous systematic reviews demonstrated a similar reduction in HbA1c for intervention groups.44,45 Moreover, every 1% reduction in HbA1c is associated with a 14% decrease in MI, a 12% decrease in the risk of stroke and a 37% decrease in microvascular complications. 46 Notably, patients with HbA1c greater than 8.5% gain more benefit from the pharmaceutical intervention programmes because they have the highest risk of cardiovascular disease. 47
Included studies focused on SBP as a critical risk factor in T2D. The results revealed that every 1 mmHg elevation in SBP is associated with a 2% increase in the risk of hyperglycaemia 48 and every 10 mmHg reduction in SBP is associated with a 12% CV risk reduction; with the lowest risk occurring at an SBP less than 120 mmHg. 49 Similar to our finding, another systematic review 50 reported a reduction in the diastolic BP by −3.9 mmHg in patients under pharmacist care.
LDL-C is related to insulin resistance and is the strongest predictor of CHD development, followed by HDL-C. 51 Our pooled estimate showed a significant reduction in TC associated with pharmaceutical care equivalent to reviews conducted by Machado et al. 52 and Charrois et al. 53
The role of the clinical pharmacist in diabetes self-management was demonstrated to be positive. 54 A previous review mentioned that lifestyle consultation might reduce cardiovascular disease by 50%. 55 Another analysis indicated that medication adherence was enhanced with the education provided by the pharmacist, including discussion issues related to patients’ therapy. 13 Similar to Jamshed’s findings, 56 our review suggests that pharmacist intervention is cost-effective. A significant improvement in BMI was also shown in our study. Impressive results were previously reported by Bukhsh et al. 57 Pharmacists have the opportunity to play a fundamental role in managing diabetes and its complications by directing patients to monitor their therapy to improve medication adherence and provide counselling and advice on lifestyle issues for improving quality of life. This systematic review suggests that pharmacist interventions can lead to relatively more significant improvements in glycaemic control when comparing T2D interventions among all healthcare professionals (Shamala Ayadurai, 2020, Pousinho et al., 2020).
The strength of the review was randomised controlled trials conducted in the same setting (hospitals). Direct pharmacist-led interventions and pharmacist-collaborative interventions are both highlighted to be effective models in diabetes management. The study’s limitations were as follows: a small number of patients enrolled; self-reported questionnaire responses may have been affected by social desirability and recall bias; there may have been variation in education programmes for the patients; and limited studies reported the cost of the pharmacist-led intervention.
The limitations with the systematic review were that many results were reported in different units, making it hard to pool out the results. In addition, there were variations in the study design and the way of conducting the intervention, causing the level of information delivered to individuals not at the same standard.
Our study emphasises the influential role of pharmacists in diabetes care. Delivering pharmacist interventions among T2D patients supports the patients’ knowledge of diabetes and delays long-term complications, and it also assists in medication adherence and motivates lifestyle modification. Although HbA1c and BP often share risk factors, controlling them with a lipid profile is essential in reducing CVD in the future.
Overall, the randomised controlled trials conducting in the same setting (hospitals), included provide a comprehensive review of pharmacist interventions consisting of patients cousneslling and education on T2D and it is complications, and advice on medication adherence revealed that pharmacist interventions associated with a significant improvement in clinical outcomes, medication adherence, diabetes knowledge and health-related quality of life outcomes when compared with standard care. Direct pharmacist-led interventions and pharmacist-collaborative interventions both highlighted to be effective model in diabetes management. The limitation was the variation reported results, small number of patients enrolled in the studies, self-reported questionnaire responses may have been affected by social desirability and recall bias, no education programme for the patients and limited studies reported the cost of the pharmacist-led intervention.
Conclusion
This systematic review and meta-analysis emphasise the effect of pharmaceutical care programmes in minimising the risk factors associated with T2D. The studies documented an overall improvement in glycaemic control, lipid profiles, BP levels and BMI with various pharmacist-led interventions. Increasing medication adherence and lifestyle modifications were also reported. Future research should evaluate smoking cessation in reducing CVD risk and investigate the cost-effectiveness of pharmacist intervention in hospital settings for T2D patients. The most effective elements of pharmacist-led interventions have been not identified. Ultimately, numerous studies in different countries have documented the satisfaction of pharmacist interventions for T2D patients with CVD risk factors. Moreover, this systematic review suggests that well-trained clinical pharmacists can assist other healthcare professionals in improving diabetes care.
Footnotes
Acknowledgements
I am sincerely thankful to my supervisors Dr. Jonathon and Professor Anne for their support and providing me with the opportunity to write this paper. I am also thankful to MORG group especially Kristina to help me with the assessment of risk bias.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.