
Abstract
Purpose:
Comprehensive review of gene replacement therapy with guidance and expert opinion on handling and administration for pharmacists.
Summary:
There are currently ∼2600 gene therapy clinical trials worldwide and 4 Food and Drug Administration (FDA)-approved gene therapy products available in the United States. Gene therapy and its handling are different from other drugs; however, there is a lack of guidance from the National Institutes of Health (NIH), FDA, Centers for Disease Control and Prevention (CDC), World Health Organization (WHO), and professional associations regarding their pharmaceutical application. Although the NIH stratifies the backbone biologicals of viral vectors in gene therapies into risk groups, incomplete information regarding minimization of exposure and reduction of risk exists. In the absence of defined guidance, individual institutions develop their own policies and procedures, which often differ and are often outdated. This review provides expert opinion on the role of pharmacists in institutional preparedness, as well as gene therapy handling and administration. A suggested infrastructural model for gene replacement therapy handling is described, including requisite equipment acquisition and standard operating procedure development. Personnel, patient, and caregiver education and training are discussed.
Conclusion:
Pharmacists have a key role in the proper handling and general management of gene replacement therapies, identifying risk level, establishing infrastructure, and developing adequate policies and protocols, particularly in the absence of consensus guidelines for the handling and transport of gene replacement therapies.
Introduction
Gene therapy offers a novel approach to treating rare and sometimes life-threatening genetic diseases and may require new responsibilities for pharmacy practice. 1 The American Society of Gene and Cell Therapy (ASGCT) defines gene therapy as the introduction or removal of genetic material or modification of gene expression to alter the biological function of an individual’s genetic code with the objective of achieving a therapeutic benefit. 2 These approaches include replacing a nonfunctional gene with a functioning healthy gene, inactivating a disease-causing gene, or introducing a new or modified gene into the body. Mechanisms of gene therapy can include gene replacement therapy, in which a fully functioning gene is introduced to replace a mutated gene; gene addition for complex cancerous and infectious diseases, in which a new gene is introduced into the body to help fight a disease; gene inhibition or “knockdown” to inactivate a mutated gene that is overproducing its product by targeting RNA; and gene editing that permits targeted changes to a gene sequence. 3,4 Although there are many types of gene therapy, this review will provide guidance related to safe handling and administration of gene replacement therapy, a form of gene therapy designed specifically to provide or transfer a fully functioning copy of a gene. Transfer of genetic material into cells may be accomplished through nonviral vector-based or viral vector-based delivery systems. 2 Although genome editing therapeutic approaches use similar vectors to deliver genetic information, this modality will not be reviewed. 3
Gene Replacement Therapy Design
Gene therapies using viral vectors can deliver the desired therapeutic gene both ex vivo and in vivo. In vivo gene therapy consists of direct delivery of the viral vector into the body with the option of systemic delivery or more targeted local delivery approaches. 5 Voretigene neparvovec-rzyl was the first in vivo gene replacement therapy to gain Food and Drug Administration (FDA) approval in 2017 6 for the treatment of patients with retinal dystrophy caused by bi-allelic RPE65 mutation. 7 Chimeric antigen receptor T-cell is a targeted ex vivo-based immunocellular therapy designed to genetically modify or reprogram T cells extracted from the patient, after which they are reinfused with the goal of eliminating cancerous cells. 8,9 Examples of FDA-approved ex vivo therapies include tisagenlecleucel for the treatment of B-cell precursor acute lymphoblastic leukemia (B-ALL) and relapsed/refractory (R/R) large B-cell lymphoma and axicabtagene ciloleucel for adult patients with R/R large B-cell lymphoma. 10,11 Both therapies consist of autologous T cells that have been genetically modified using a lentiviral vector (tisagenlecleucel) or a retroviral vector (axicabtagene ciloleucel) to encode an anti-CD19 chimeric antigen receptor. 10,11 In a multicenter trial of R/R B-ALL patients treated with tisagenlecleucel, event-free survival at 6 months was 73%, with a 90% overall survival (OS) at 6 months. 12,13 Progression-free survival at 6 months was 49% and OS at 6 months was 78% after axicabtagene ciloleucel infusion in patients with R/R aggressive B-cell non-Hodgkin lymphoma. 14
In selecting a specific gene therapy approach, certain disease attributes must be considered for optimal efficacy outcomes. Gene replacement therapy lends itself particularly well to monogenic diseases (eg, sickle cell disease, cystic fibrosis, and spinal muscular atrophy [SMA]) in which the phenotype is driven by the mutation or deletion of a single gene. Therefore, replacement of the nonfunctional gene via gene replacement therapy is considered a potentially viable therapeutic strategy. Although polygenic diseases, including many cancers, may be more challenging to target, some might benefit from gene replacement therapy. The targeted tissue to be transduced is also an attribute that must be considered. For example, the durability or persistence of transgene expression may vary based on the proliferative capacity of the target tissue and the ability of the vector to integrate into the host genome. 15 For non-dividing cells, it may be preferred to use a viral vector that does not integrate into the host genome, such as adeno-associated viral vectors (AAVs). 16 AAV viral vectors may allow for long-term transgene expression in non-dividing cells (eg, neurons and skeletal muscle) versus dividing cells (eg, hematopoietic cells), in which transgene expression may be diluted or lost with multiple cell divisions, necessitating repeat dosing. 15 The transgene construct may also affect the durability of transgene expression. 17 For genes that may require long-term expression, a strong, constitutive engine or promotor may be necessary to allow continuous transcription. In contrast, life-threatening conditions may require immediate, high-level gene expression required in early development; therefore, the selection of another promotor or combination may be preferred.
Another factor that must be considered when developing a gene therapy is the potential immunogenicity of the chosen viral vector. Viral vectors are foreign to the body, and the immune mechanisms of developing potential anti-vector antibodies or an immune response may impact both safety and efficacy outcomes for gene therapy studies. 16 Not only could anti-vector antibodies potentially inhibit transduction, thereby rendering the therapy ineffective, they could also elicit a pro-inflammatory response (adenoviral vector) or a cellular T-cell response induced by the major histocompatibility complex 1 pathway, as has been shown with adenoviral vectors and AAVs. 18 However, there is currently no industry standard for the anti-vector immunoglobulin G (IgG) antibody titer permissible for each vector before dosing and no way to predict the potential expansion of capsid-specific memory CD8+ T cells. 19 Studies assessing the IgG humoral immune response have used different thresholds for the same viral vector. For example, gene replacement therapy studies with AAV vectors have used various anti-AAV thresholds, including undetectable, ≤1:50, and <1:400. 20 -22 The immune response to each viral vector may also differ. 23 Although both adenovirus and AAV infections induce antibody development, 23 adenoviral vectors elicit an inflammatory response that has not been detected with AAV wild-type infections. 24 In addition to determining antibodies specific for the particular viral vector being used before dosing, a short course of prophylactic and concurrent immune suppressive therapy (steroids) has been used in some programs as a strategy to suppress the expected immune response to the viral capsid by the host.
The objective of this review is to provide a comprehensive pharmacy review of gene replacement therapy with some guidance and expert opinion on gene replacement therapy handling and administration for pharmacists. 25 Other reviews are also timely addressing this topic. Although the National Institutes of Health (NIH) stratifies gene therapy delivery viral vectors into risk groups (RGs), it does not provide information on minimization of exposure and strategies to reduce risk in the clinical setting. 26 Thus, individual institutions have been left to develop their own policies and procedures, which can differ from one another. Furthermore, the novelty of the therapy has created a void in the establishment of guidelines for dispensing. Although there are intense regulation and oversight in conducting human gene therapy research trials, there is a lack of clinical guidance from the NIH, FDA, Centers for Disease Control and Prevention (CDC), World Health Organization (WHO), and professional associations regarding the clinical application of gene therapy. 26,27 This review provides an expert opinion about what pharmacists minimally need to know and their role in administering gene therapies in an effort to bridge these gaps to ensure minimal health safety risks to patients, health-care providers, caregivers, and the environment. Specifically, we discuss the role of pharmacists in institutional preparedness, as well as gene therapy handling and administration.
Era of Gene Therapies
The first gene therapy study in the United States was conducted by Steven A. Rosenberg in 1989 to treat metastatic melanoma. 28 From 1989 to 2017, approximately 2600 gene therapy clinical trials were initiated; the majority were phase I or II studies. Most clinical studies up to 2017 used adenovirus and retrovirus vectors. 29 These studies resulted in FDA approval of 5 gene therapy products: voretigene neparvovec-rzyl, talimogene laherparepvec (T-VEC), tisagenlecleucel, axicabtagene ciloleucel, and onasemnogene abeparvovec. A recent report from Massachusetts Institute of Technology estimates that approximately 40 gene therapy products will be approved by 2022. 30 The following case studies describe 3 FDA-approved gene therapies.
The first FDA-approved in vivo gene replacement therapy, voretigene neparvovec-rzyl, was approved for the treatment of inherited retinal dystrophy. This therapy consists of live, nonreplicating genetically modified AAV2 capsid that expresses RPE65. A single subretinal administration of voretigene neparvovec-rzyl resulted in rapid functional visual improvements from baseline, as determined by multi-luminance mobility testing, beginning 30 days post-dosing. 31 The durability of the treatment was shown to 3 years, with studies ongoing. 32 The absence of product-related serious adverse events or deleterious immune responses was also reported and largely attributable to the immune privileged route of administration and low viral dose. 31,32
T-VEC is an oncolytic viral gene therapy approved for the local treatment of inoperable cutaneous, subcutaneous, and nodal lesions in patients with melanoma recurrent after the initial surgery. 33 T-VEC is a live, attenuated herpes simplex virus designed to express granulocyte-macrophage colony-stimulating factor (GM-CSF), an immune stimulatory protein, in tumors. Cutaneous injection of T-VEC significantly increased the durable response rate, overall response rate, and OS compared with subcutaneous GM-CSF administration. 34 The safety of T-VEC was demonstrated in patients with surgically unresectable melanoma, with most adverse events being rated as mild or moderate. 33
AVXS-101(onasemnogene abeparvovec) is a newly approved gene replacement therapy that uses an AAV9-derived capsid for the treatment of SMA. 35 The most severe and common form of SMA, SMA type 1 (SMA1), is a rapidly progressing neuromuscular disease in newborns that leads to loss of motor function and permanent ventilation or death by age 2. 36 Because motor neurons are non-dividing, one-time intravenous administration of AVXS-101, which has been shown to cross the blood-brain barrier and transduce motor neurons in non-human primates, 37 has the potential for lifetime episomal transgene expression. The self-complementary feature of AVXS-101, which bypasses the rate-limiting step of second-strand synthesis from the single-stranded DNA template, allows for rapid survival motor neuron (SMN) protein production, and its hybrid cytomegalovirus (CMV) enhancer, chicken beta-actin promoter, 38 drives high and durable SMN expression in motor neurons of the central nervous system. 17,39 Importantly, use of the CMV enhancer alone and other viral constructs cannot induce CMV infection, and the AAV construct is replication-incompetent. All patients treated with a single proposed therapeutic dose of AVXS-101 in a phase 1 study achieved permanent ventilation-free survival to at least 24 months of age, a positive impact on the natural history of the disease. 36,40 -42
Challenges for Clinical Pharmacists in the Era of Gene Therapy
A European survey of 64 pharmacists showed that 75% of respondents expressed safety concerns, including concerns regarding pharmacokinetic and pharmacodynamics interactions. 43 Furthermore, of the 3543 pharmacists surveyed by the American Society of Health-System Pharmacists, the response rate was only 9%, which could reflect a lack of understanding of gene therapy. Moreover, the survey found that 37% of respondents were still planning where gene therapy products would be stored, and 30% of respondents were not sure whether they had the appropriate biologic safety cabinet. 44 Similarly, a recent review of pharmacy facilities in the United Kingdom revealed that most do not have adequate freezers or the requisite aseptic facilities for the storage, handling, and reconstitution of gene therapies. This is consistent with two other smaller surveys of 120 and 1440 pharmacists in the United Kingdom, in which a lack of familiarity with gene therapy was reflected by low response rate. 43 -45 The clinical pharmacists’ gap in gene therapy knowledge will require the development and implementation of educational programs such that they are capable of leading institutional preparedness when approved gene therapy products become available.
In 2007, the European Association of Hospital Pharmacists guidelines were developed by gene medicine specialist pharmacists to provide the minimum requirements for storage, transportation, preparation, dispensing, administration, disposal, decontamination, spillage, and accidental exposure procedures based on the available evidence and practical experience. 46 Practice protocols published in the United Kingdom also discuss the lack of systematic procedures for the handling of gene therapies. 46 In 2018, the FDA did publish a draft guidance for industry that outlines the necessary information to provide to clinical study sites to ensure product safety, identity, quality, purity, and strength; however, these procedures are in the context of the clinical study setting and may not be adaptable to clinical pharmacy practice. 47 The absence of guidelines for handling gene therapy in the clinical setting from the NIH, FDA, WHO, or CDC in the United States has been noted in various pharmacy publications since 1999. As a result of the lack of guidance from research to clinical practice, a few institutions, including the University of North Carolina and the University of Kentucky, have published their own research handling practices for gene therapies that may serve as a reference for clinical practice. 48,49 Ultimately, as more gene therapy products are approved, institutions that want to provide these advanced therapies to their patients must be prepared to develop their own policies until such guidelines are published. 1,6,27,50 -53
Different Viral Vectors Have Different Levels of Risk
Viral vectors can differ substantially in their replication status and virulence, each with advantages and disadvantages. Viral vectors can be (1) integrating (eg, retroviral and lentiviral viral vectors), which integrate the desired transgene into the host genome, or (2) nonintegrating (eg, herpes, adenoviral, and AAV vectors), which do not generally integrate the desired transgene into the chromosomal DNA, but allow the transgene to remain within the nucleus as an episome or extrachromosomal DNA. 16 With nonintegrating vectors, the transgene can be lost during cell division because episomal DNA is not replicated along with cellular DNA. 15 Viral vectors can also be replication competent in that they contain genes required for virion synthesis. Alternatively, they can be replication deficient, lacking in factor(s) necessary for viral genome replication or synthesis and assembly of viral particles. The replication competency status of the viral vector requires consideration given the potential virulent secondary transmission risks associated with some parental strains. 52 Although most vector systems have been modified to eliminate genes associated with viral replication, rendering them replication incompetent, the possibility of recombination events with wild-type virus could restore competency, particularly with retroviral vectors. 54 As such, the FDA offers draft guidance regarding replication competency testing for retroviruses during manufacturing, as well as subsequent monitoring of patients for retroviral infection. 55 For other viral vectors that are not known to be associated with human diseases, such as AAVs, 23 recommendations are less stringent, with no such recommendations for patient testing or monitoring.
Of the gene therapy products currently available or under investigation, adenoviral products (20.5%; n = 547) are the most common and are often used as cancer therapies. Adenoviruses have high transduction efficiency, infecting a wide range of host cells, both dividing and nondividing. 29,56 Retroviruses, which are used in 17.9% of clinical gene therapy trials, can integrate genetic cargo into the host’s genome and may provide stable, long-term gene expression in dividing cells (lentiviruses can transduce both dividing and non-dividing cells); these viral vectors are used primarily for ex vivo gene therapy treatments of hereditary disorders. 29,56 Although AAV vectors generally do not integrate into host genomes, they may induce long-term gene expression in non-dividing cells (eg, neurons) and are primarily being used to develop gene therapy treatments of monogenic hereditary disorders. 29,56 Thus, gene therapy product safety risks are inherent to the parent wild-type virus, as well as considering the potential toxicity of the desired transgene it contains. 4,48,54
The NIH and WHO guidelines categorize wild-type infectious agents into RGs for laboratory research; however, these may be adapted for clinical application. 26,57 The classification of recombinant or synthetic nucleic acid molecules places gene therapies into the following 4 RGs according to their pathogenicity for humans: (1) RG1 agents are not associated with disease in healthy adult humans; (2) RG2 agents are associated with human disease that is rarely serious and for which preventive or therapeutic interventions are often available; (3) RG3 agents are associated with serious or lethal human disease for which preventive or therapeutic interventions may be available; and (4) RG4 agents are likely to cause serious or lethal human disease for which preventive or therapeutic interventions are not usually available (Table 1). 26 For example, AAV vectors are classified as RG1 agents, whereas adenovirus, retrovirus, and herpes simplex virus vectors are classified as RG2 agents. Few, if any, agents from RG3 or RG4 are being investigated as clinically therapeutic agents for human use. 16,26 However, this classification system provides only a minimum level of standards for laboratory research and may not be fully applicable to real-world clinical practice.
Gene Therapy and NIH Risk Groups/BSL Designation for Research Handling.
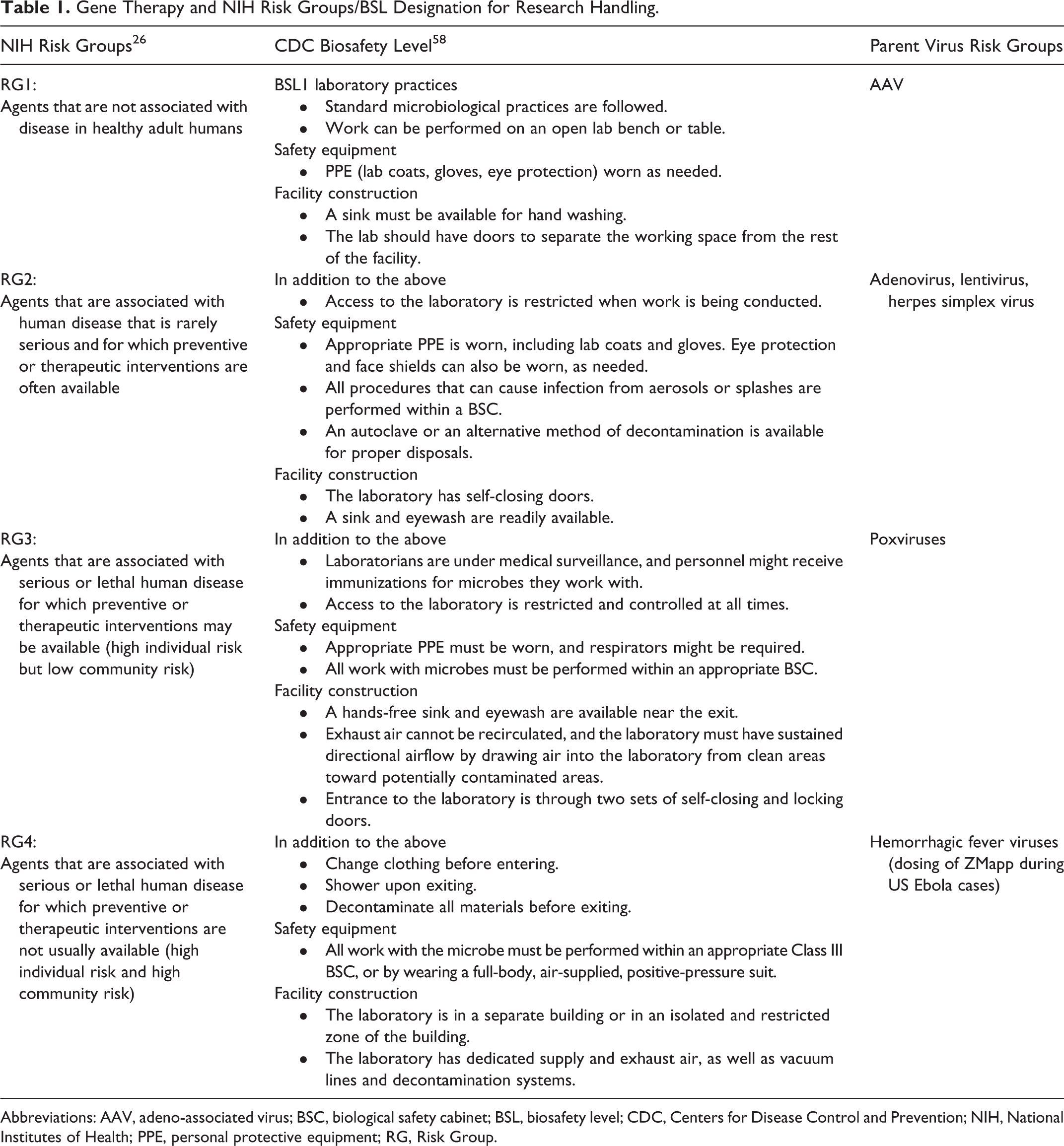
Abbreviations: AAV, adeno-associated virus; BSC, biological safety cabinet; BSL, biosafety level; CDC, Centers for Disease Control and Prevention; NIH, National Institutes of Health; PPE, personal protective equipment; RG, Risk Group.
An agent’s risk group informs its biosafety level (BSL) and, therefore, its safety and handling protocol, and thereby the level of containment needed to minimize risk. 58 Regarding physical containment, the CDC, WHO, and NIH have published recommendations for BSL (levels 1–4) for wild-type virus and viral vector handling in laboratory research, and these recommendations may be adapted for clinical application (Table 1). 26,57,58 As with RG classification, BSL classification differs by virus. Adenovirus is classified by some research institutions, including Emory University, as requiring BSL-2 practices, and several research institutions, such as the University of North Carolina and the Cleveland Clinic, classify AAVs as an RG1 agent, requiring BSL-1 handling. 49,59 However, these practices may be subject to change because to date, the National Institute for Occupational Safety and Health (NIOSH) has not formally classified current FDA-licensed gene therapy products. 60 In addition, depending on the classification and the implementation of USP 800, handling of these agents may change. For instance, viral vectors (retrovirus) that integrate the therapeutic genetic material into patient DNA have been shown to cause cancers in clinical trials, and replication-competent viral vectors may cause risk of secondary transmission and thus may meet some of the NIOSH criteria for hazardous drugs. 60
Expert Recommendations for Institutional Preparedness
Until NIOSH updates are available, we recommend that each institution adopt its own procedures and evaluate gene therapy products individually, taking into consideration the risk group and BSL of each viral vector, including the potential risk associated with the encoding transgene. Because pharmacists play an integral role in providing oversight for current drug therapies, we recommend that pharmacists become institutional leads in gene therapy product handling, and similarly, we recommend that pharmacists provide oversight of gene therapy product handling, which will include training, education, informing policies and procedures, and ensuring compliance. Recommendations provided below are also summarized in Table 2.
Expert Recommendations for Institutional Preparedness.
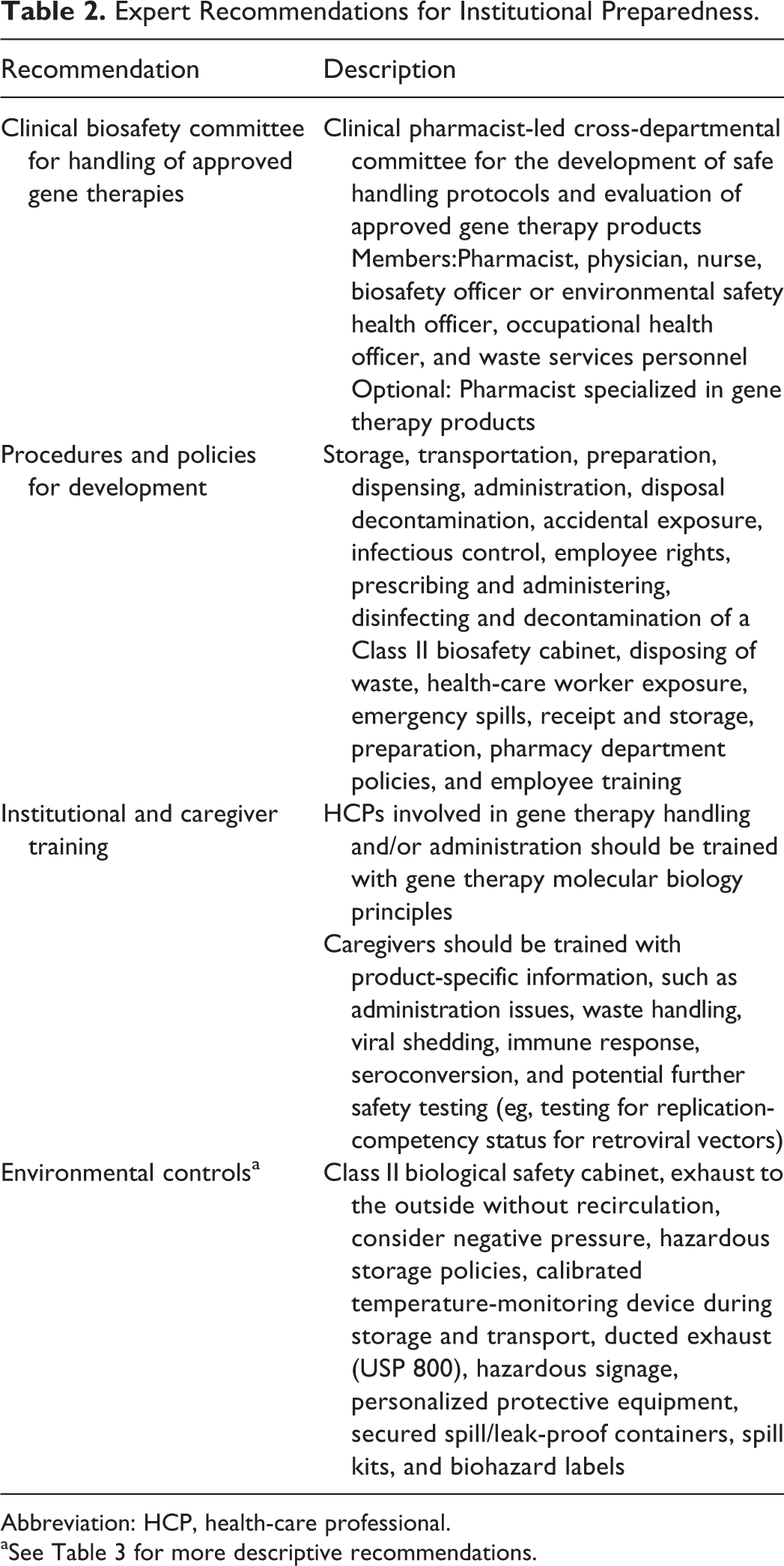
Abbreviation: HCP, health-care professional.
aSee Table 3 for more descriptive recommendations.
Recommendations for Policies and Procedure Development
Safe dispensing and administration of approved therapies are not only a concern of the clinical pharmacist but may also involve physicians, nurses, and other healthcare professionals. We recommend that clinical pharmacists lead in the formation of clinical biosafety committees if their institutions are expecting to administer any approved gene therapy products and that the following roles (or delegates) be represented in a committee tasked with developing appropriate safe handling procedures: pharmacist, physician, nurse, biosafety officer or environmental safety health officer, occupational health officer, and waste services. Moreover, we recommend that as more gene therapies become approved and widely used, a pharmacist specialized in the therapy should be appointed within each institution.
Future efforts should move toward standardization of gene therapy handling that reflects a scientifically valid, rational balance of safety and practice practicalities to ensure broad access to these potentially transformative therapies. Such efforts might involve the addition of therapy-specific biosafety protocols or standard operating procedures, similar to how current cytotoxic agents and biologics are traditionally handled, to ensure the integrity of the product and personnel safety. 60 Given the heterogeneity of gene viral vector therapies in terms of integrating/nonintegrating and hazardous/nonhazardous transgenes (i.e., transgene encodes a potentially tumorigenic product or toxin or nonhazardous product, respectively), each gene therapy should undergo an assessment of risk based on specific viral vector and transgene properties. An example of a risk identification tool that may be useful for such a committee is provided in Figure 1. Handling recommendations from previously approved products vary widely, in part because of the different viral vectors used. Voretigene neparvovec-rzyl is an AAV vector-based gene therapy, and product guidance generally states that universal biohazard precautions for handling should be followed; however, no specific guidance is included. 7 Because low-level shedding of capsid can be present in patient tears, proper handling of dressings, tears, and nasal secretions (i.e., storage of waste material in sealed bags before disposal) is recommended for up to 7 days after dosing. 7 No guidelines for stool and urine have been provided. Detailed guidance has been provided regarding the preparation and handling of T-VEC, an attenuated herpes simplex virus, including instructions for minimizing exposure, surface cleaning, and disposal because accidental exposure could lead to herpes infection. 52 Development of consensus guidelines on the proper use and handling of gene therapy products will facilitate the standardization of handling recommendations from product to product; however, procedures for specific products should also reflect what is known about product shedding.
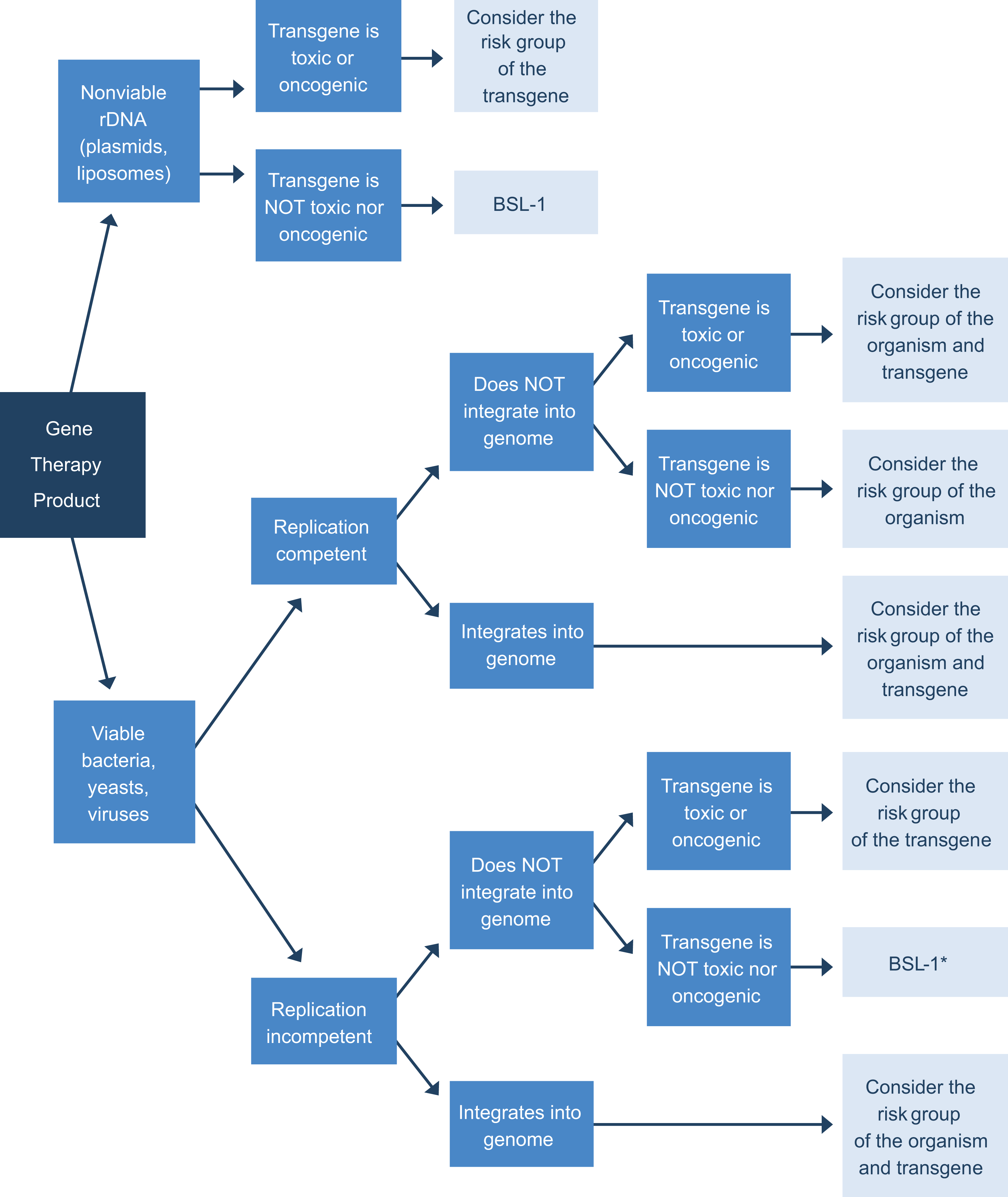
Risk identification for gene therapy products based on replication competency status, ability to integrate into the genome, and toxicity of transgene. The flow chart tool emphasizes the gene therapy safety attributes that should primarily be considered when deciding BSL handling and procedures. If a gene therapy product has the ability to replicate or can integrate into the genome or contains a toxic transgene, it is recommended that a more detailed risk evaluation by an institutional committee will be conducted to determine safety handling processes. *BSL-1 classification is recommended provided that the gene therapy product was manufactured without using adenovirus or any other helper virus of human origin. BSL1, biosafety level 1.
Given the lack of guidance and risk variability between gene therapy products, we recommend the following procedures be developed at institutions expecting to handle gene therapy products: infectious control, employee rights, prescribing and administering, disinfecting and decontamination of the Class II biosafety cabinets (BSC), disposing of waste, health-care worker exposure, emergency spills, receipt and storage, preparation, pharmacy department policies, and employee training. The manufacturer’s guidance should be consulted and normal hospital procedures will need to be consulted when developing product-specific procedures. As much as possible, these procedures should be general, with few modifications added for specific products as necessary.
Recommendations for Institutional and Caregiver Training
As with any other therapeutic agents, gene therapies should enter health-care facilities through the pharmacy, which is responsible for their safe receipt, preparation, dispensing, and storage; however, pharmacies may be currently underequipped and staff uninformed to handle these therapies. As gene therapy evolves, pharmacists will serve a critical role in the multidisciplinary team to ensure the safe and efficacious delivery of these therapeutic agents. 61 Therefore, molecular biology principles and additional training or competencies may be necessary to fill any educational gaps resulting from additional or changing roles and responsibilities. 1 Furthermore, we recommend that this training be specific to each discipline, including pharmacists, infusion nurses, and investigators and research personnel.
Caregiver education is also crucial and should be tailored to specific products. Pharmacists have a role in educating and counseling patients and caregivers about administration issues, as well as waste handling and any other issues specific to the particular gene therapy, including viral shedding, immune response, seroconversion, and further safety testing (eg, testing for replication-competency status for retroviral vectors). We recommend training regarding a possible immune response or seroconversion in employees be conducted in a product-specific manner such that all employees are informed of potential risks and hazards and trained to minimize those risks. Although the risk of seroconversion from contact with patients dosed with any gene therapy product is not available, caregivers and healthcare professionals should be informed that theoretically, seroconversion may limit the possibility of future dosing with gene therapy. In the absence of gene therapy product-specific infectious information, policies may be developed based on what is known about the parent wild-type virus. 51
Environmental Controls
We also recommend that a proper infrastructure be in place to ensure safe handling and administration of gene therapies. In the case of biologics and viral vectors, contained use includes protection of the product, the worker, and the environment; thus, safety precautions extend not only to patients but also to healthcare professionals. Appropriate equipment for storing and handling is necessary, including BSC for low- to moderate-risk biological agents. 45 A model of proper infrastructure is shown in Table 3. Although CDC guidelines do not require that RG1 products handled at BSL-1 be handled in a hood for research practices, human delivery of gene therapy preparation should not be performed on an open bench but rather should follow the established USP aseptic technique guidelines and utilize a Class II BSC to ensure product sterility and personnel safety. 50,62 Class II BSCs ensure product sterility and personnel safety by providing 4 levels of protection: protect the operator from airborne biological hazards, protect the laboratory and the environment from hazards, protect the samples in the BSC from airborne contamination in the laboratory with a downward flow of filtered air, and prevent cross-contamination within the BSC work area through the use of a flowing, uniform down flow onto the BSC work area. 63
Suggested Model for Needed Infrastructure for Gene Therapy Handling.
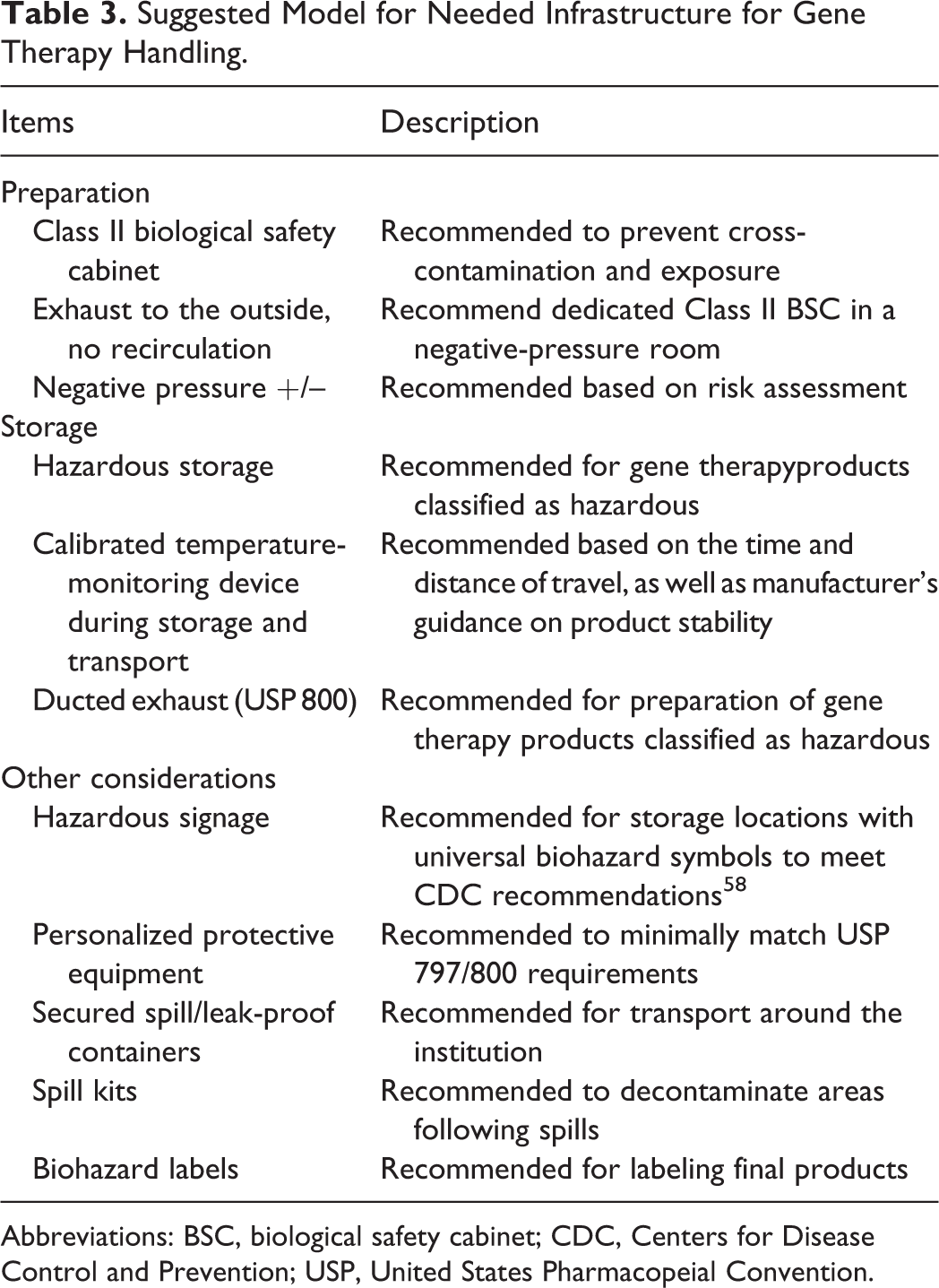
Abbreviations: BSC, biological safety cabinet; CDC, Centers for Disease Control and Prevention; USP, United States Pharmacopeial Convention.
To ensure the safety of personnel, it might be necessary to develop a specific standard operating procedure for products that would encompass the following: storage, cleaning, preparation, dispensing, accidental spillage/exposure, personal protective clothing, equipment (eg, BCS), disinfection and decontamination procedures, transport, disposal of waste products, and worksheets specific to each gene therapy dispensed, if applicable. Processes and procedures should be made available for personnel who might come into contact with gene therapies or patients receiving gene therapy to minimize nosocomial transmission. In addition to an appropriate biohazard waste disposal protocol for disposable materials, sharps, laundry, and non-disposable items used for gene therapy dispensing/administration (eg, protocols for sealing, incinerating, and cleaning),we recommend universal personal protective equipment requirements and before-and-after decontamination and disinfection protocols to ensure that the virucidal product used is appropriate for the agent, including contact inactivation time. Some viral vectors are enveloped, and some have only a proteinaceous capsid; therefore, susceptibility to virucidal agents may vary. 51
Regarding transporting the gene therapy from the pharmacy to the infusion site, we recommend the product be transported in a container labeled with a universal biological hazard warning label to only a nearby walkable distance between sites for in vivo gene therapy to reduce risk of spills and contamination of other areas. In-person handoff between dedicated pharmacy staff and the nurse or provider administering the therapy is also recommended.
Conclusions
Gene therapy opens a new paradigm in the management of cancers and genetic disorders. As with any first-in-class handling of new medicines (eg, biological therapies) and cytotoxic agents, 64 gene therapy and its handling are different from other drugs. Gene therapy requires contained use and aseptic principles to protect health-care workers, patients, and the environment. 53 However, biohazardous materials can be administered safely with minimal risk once institutional procedures are in place and with personnel, patient, and caregiver education and training. 27 Pharmacists have a key role in the proper handling and general management of gene therapies, identifying risk level, establishing infrastructure, and developing adequate policies and protocols, particularly in the absence of consensus guidelines for the handling and transport of gene therapies. 50
Footnotes
Acknowledgments
This review was developed with writing assistance from Jessica Cardenas, PhD, and Marjet Heitzer, PhD, for inVentiv Medical Communications, a Syneos Health group company, and was supported by AveXis, Inc.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dominic Marchese is an employee of AveXis, Inc. Chris Jenkins owns a for-profit clinical trial organization supporting AveXis, Inc., as well as other gene and cell therapy organizations. Michael Storey has received honoraria from AveXis, Inc., for consulting services. John Petrich has received honoraria from AveXis, Inc. for consulting services.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.