
Abstract
Introduction:
Proton pump inhibitors (PPIs) may rarely cause thrombocytopenia. To our knowledge, only one case of lansoprazole-induced thrombocytopenia has been reported previously.
Case:
We report a case of a 50-year-old South Asian male who was admitted to the intensive care unit (ICU) after cardiac arrest during general anesthesia for ureteroscopy. During ICU stay, his platelet count dropped from 315×103/µL to 57×103/µL after 5 days of initiation of lansoprazole for stress-ulcer prophylaxis. After excluding other causes of thrombocytopenia; lansoprazole was stopped and his platelets recovered over the next few days. Later exposure to lansoprazole resulted in another drop in his platelet count with subsequent recovery after discontinuation of lansoprazole. A review of his home medications showed that he had been taking pantoprazole prior to hospitalization.
Discussion:
Thrombocytopenia has been previously reported with different PPIs. In the previously reported lansoprazole-induced thrombocytopenia, the level of certainty was not high due to lack of re-exposure. In the present case, another exposure to lansoprazole, without intention of rechallenge, reproduced the same adverse drug reaction (ADR). Although platelet-reactive antibodies testing was not available to confirm causation in this case, the Naranjo score was 8 which indicated probable causation by lansoprazole. Despite probable lansoprazole-induced thrombocytopenia, our patient had been tolerating pantoprazole. This finding highlights the different effects of individual PPIs on platelet counts in the same patient.
Conclusion:
Lansoprazole may cause thrombocytopenia. However, patients who develop lansoprazole-induced thrombocytopenia may tolerate other PPIs.
Introduction
Proton pump inhibitors (PPIs) are commonly used in critical care settings mainly as treatment for upper gastrointestinal (GI) bleeding or as prophylaxis against stress-related mucosal damage especially if the patient requires mechanical ventilation for ≥ 48 hours or has coagulopathy (defined as international normalized ratio [INR]> 1.5 or platelet count < 50×103/µL). 1,2 PPIs are prodrugs which require an acidic medium to be converted to the active moieties, and they suppress gastric acid secretions by inhibiting the parietal cell H/K-ATPase. 3 Available PPI molecules include omeprazole, esomeprazole, lansoprazole, rabeprazole, and pantoprazole. Serious adverse effects associated with PPI use include acute and chronic kidney disease, Clostridium difficile–associated diarrhea, osteoporosis, and hypomagnesemia. 4 –7
Although thrombocytopenia was infrequently reported with some agents from the PPIs class, 8 –12 only one case report of lansoprazole-induced thrombocytopenia was published previously. 13 The hypothesized mechanism of PPI-induced thrombocytopenia is platelet destruction by drug-dependent platelet-reactive antibodies. 8,14
Case
We describe a case of 50-year-old South Asian male with past medical history of diabetes mellitus type II, hypertension, and coronary artery disease who was admitted for elective ureteroscopy under general anesthesia for ureteric stone. His home medications were aspirin 100 mg once daily, clopidogrel 75 mg once daily, metformin 500 mg twice daily, rosuvastatin 10 mg once daily, and pantoprazole 40 mg once daily. Additionally, he was prescribed levofloxacin 500 mg once daily for 7 days which were completed on the day of admission. His medication refill history from the outpatient pharmacy was regular and implies compliance to his home medications. After cardiology consultation, his urologist held aspirin and clopidogrel 6 days prior to the procedure to minimize the risk of bleeding.
On admission, his blood pressure was 100/62 mm Hg, heart rate was 64 bpm, respiratory rate was 20 bpm, and oxygen saturation was 99% on room air. Before anesthesia induction, he received 2 g of ceftriaxone intravenously, then he developed facial swelling, hypotension, and bradycardia, which progressed to pulseless electrical activity so cardiopulmonary resuscitation was performed and the patient was intubated. Although the cause of cardiac arrest was not clearly identified, it was thought to be an anaphylactic reaction to ceftriaxone.
After return of spontaneous circulation, he was shifted to the intensive care unit (ICU) for further care. Aspirin and clopidogrel were resumed while rosuvastatin and metformin were held due to elevated liver enzymes and critical illness, respectively. Additionally, lansoprazole 30 mg once daily by nasogastric route and heparin 5000 units subcutaneously twice daily were started for stress ulcer prophylaxis and for venous thromboembolism prophylaxis, respectively. Blood counts on the day of admission were as follows: white blood cells 18.2 ×103/µL, hemoglobin 15.1 g/dL, platelets 289×103/µL. Other laboratory investigations were normal except INR 1.3, creatinine 1.36 mg/dL, potassium 3 mEq/L, bicarbonate 19 mEq/L, and albumin 3 g/dL. He was extubated at the evening of the second day of admission to the ICU. He developed acute kidney injury and required 3 sessions of hemodialysis over the first 5 days of hospitalization then his kidney function started to improve gradually over his ICU stay. On day 2 of hospitalization, he started to have severe abdominal pain and diarrhea. Computed tomography of chest and abdomen showed multiple rib fractures and diffuse bowel edema.
On day 5 of hospitalization, his platelets dropped gradually to 57×103/µL from 315×103/µL on admission (Figure 1). Heparin was held and heparin-induced thrombocytopenia (HIT) antibodies and fibrinogen level were requested to screen for HIT and disseminated intravascular coagulation (DIC), respectively. His medical record was reviewed, but no previous episodes of thrombocytopenia were identified. HIT antibody test was negative and fibrinogen level came to be 5.34 g/L (normal). Abdominal ultrasound was done which excluded splenomegaly.
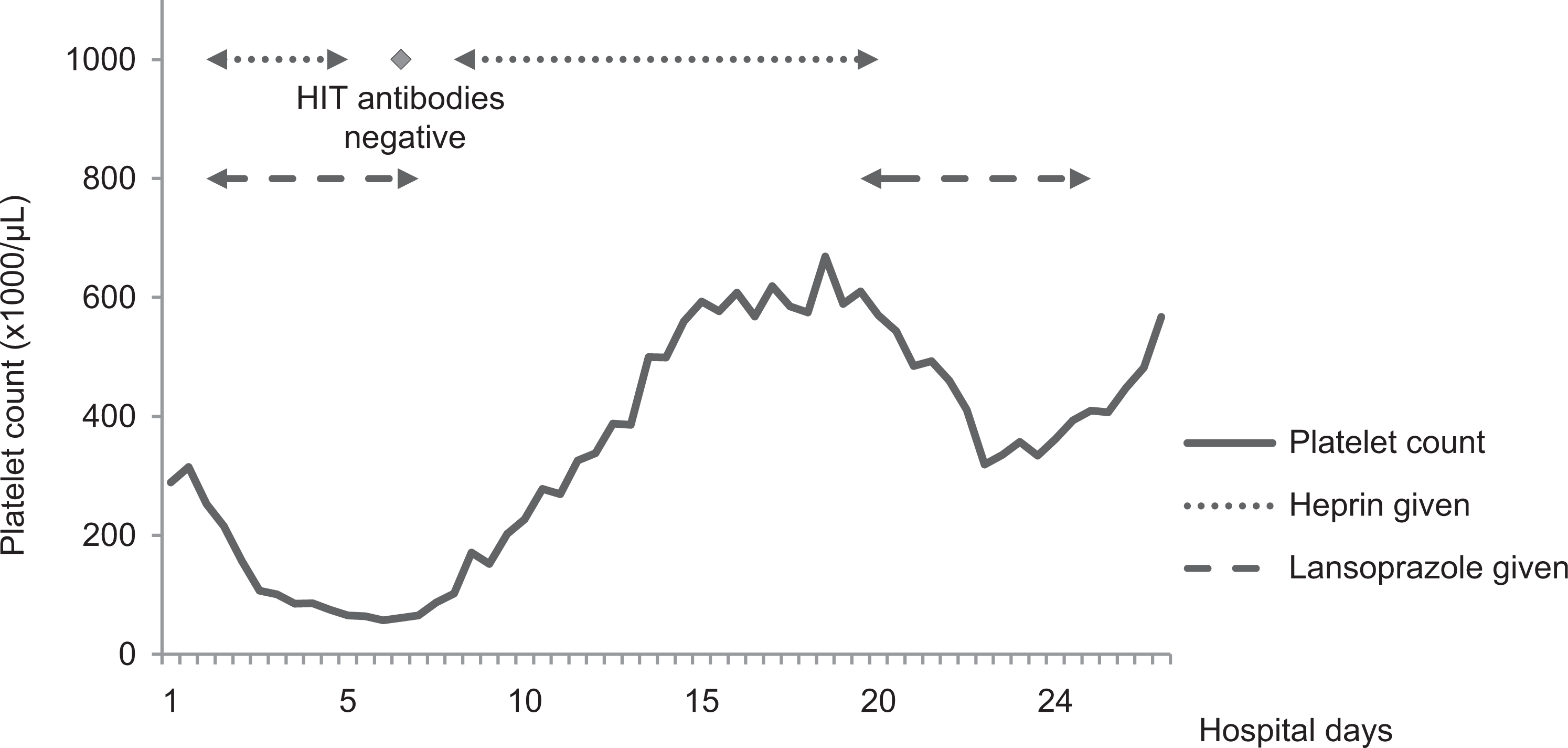
Trend of platelet count during hospital stay.
On the next day (day 6 of admission), lansoprazole was suspected to be the cause of thrombocytopenia as it was the only newly introduced medication during admission and it was changed to ranitidine 150 mg once daily while heparin was reinitiated. His platelet count started to recover to normal gradually over the next 3 days. A full list of medications received during the first week of hospitalization is provided in Table 1. On the same day, the patient developed a urinary tract infection for which aztreonam 1 g every 8 hours was started. Two days later, his urine and blood cultures revealed extended spectrum beta-lactamase Escherichia coli, so aztreonam was changed to ertapenem 1 g once daily for 14 days according to microbiological sensitivity results. On day 14 of admission, patient developed thrombocytosis (560 ×103/µL) which was thought to be reactive secondary to infection, and his platelet count continued to increase gradually over the next few days. His peripheral smear on that day showed mild anisopoikilocytosis, anisochromia, and toxic neutrophils.
Medications Received During the First Week of Hospitalization.
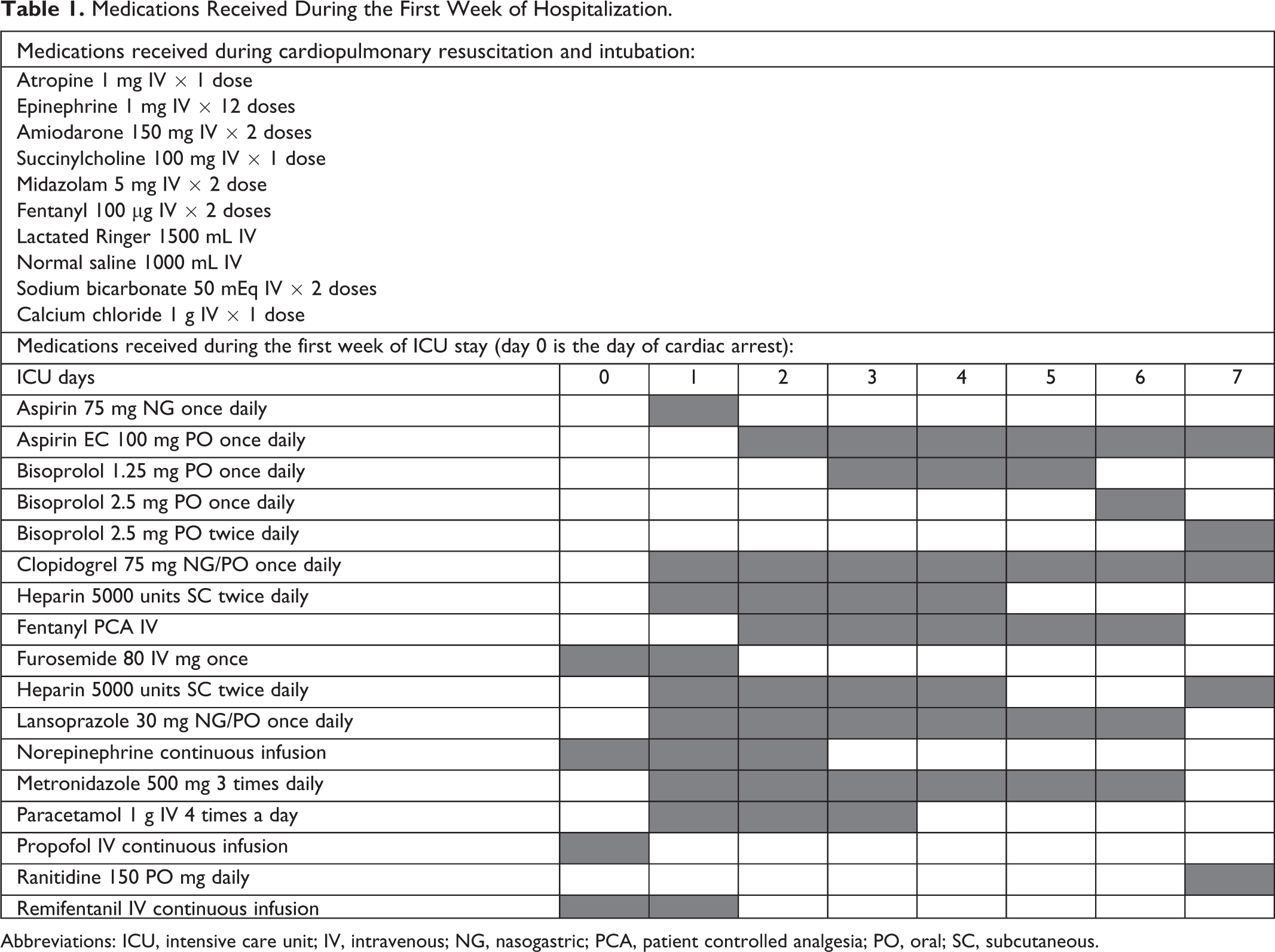
Abbreviations: ICU, intensive care unit; IV, intravenous; NG, nasogastric; PCA, patient controlled analgesia; PO, oral; SC, subcutaneous.
On day 18 of admission, lansoprazole 30 mg daily was prescribed due to suspicion of upper GI bleeding suggested by drop in hemoglobin (rechallenge was not intended). Packed red blood cells were transfused and colonoscopy was done that showed severe colitis with no evidence of bleeding and several biopsies were taken. After lansoprazole reinitiation, his platelets dropped from 669×103/µL to 319×103/µL on day 5 of reinitiation. On day 20 of admission, he started to pass fresh blood with stools and received 2 units of packed red blood cells. After stopping lansoprazole, there was rebound increase in his platelets to 567×103/µL. On day 25, the histopathology result of colonic biopsies was released and was suggestive of inflammatory bowel disease so mesalamine 1 g 3 times daily was started, and the patient was transferred to the medical ward after 28 days in the ICU. Diarrhea and abdominal pain improved slightly after starting mesalamine, but they didn’t resolve completely. Repeat colonoscopy was planned after few days, but the patient requested discharge to travel back to his home country so he was discharged after 30 days of hospital stay. A thorough review of his medical record showed that the patient had received lansoprazole for 7 days 30 months before this admission, but platelets were not checked at that time.
Discussion
Although lansoprazole-induced thrombocytopenia has been previously reported, 13 association could not be confirmed due to lack of rechallenge. In the present case, the patient developed thrombocytopenia after starting lansoprazole which recovered within few days after discontinuation. Additionally, there was more than 50% decrease in platelet count after reinitiation of lansoprazole. These findings suggested lansoprazole-induced thrombocytopenia. The adverse drug reaction (ADR) probability score (Naranjo) was calculated and found to be 8, indicating probable lansoprazole-induced thrombocytopenia, Appendix A. 15
To our knowledge, thrombocytopenia incidence rate was not reported in previous clinical trials of lansoprazole, this may be due to low actual incidence or low clinical suspicion by the investigators leading to underreporting of thrombocytopenia.
Drug-induced thrombocytopenia (DIT) is a diagnosis of exclusion; therefore, other causes of thrombocytopenia should be excluded before the diagnosis of DIT. 16 In the present case, splenomegaly was excluded by abdominal ultrasound, DIC was excluded by normal fibrinogen level and HIT was excluded by the absence of HIT antibodies. Although peripheral smear was not done with the first episode of thrombocytopenia, it was done 1 week later and no platelet abnormality was found. Additionally, the patient didn’t receive transfusions or intravenous fluids in the days preceding the thrombocytopenia event to suspect dilution thrombocytopenia.
Another possibility that we have to rule out is idiopathic thrombocytopenic purpura (ITP). There is no diagnostic test for ITP and diagnosis has to be considered after ruling out all other possible causes for thrombocytopenia. 17 In this case, the patient's platelet count improved within days after discontinuation of lansoprazole and this improvement occurred without receiving any corticosteroids or immunoglobulins; which excludes the possibility of ITP diagnosis.
Thrombocytopenia has been previously reported with omeprazole, esomeprazole, pantoprazole, and dexlansoprazole. 8 –10,12 In some of these case reports, thrombocytopenia recurred after reexposure to the culprit drug as seen in the present case. Furthermore, a retrospective study demonstrated a significant reduction in platelet counts after administration of pantoprazole for upper GI bleeding. However, results of that study should be interpreted with caution owing to the difficulty of differentiation between DIT and consumption or dilution thrombocytopenia due to blood transfusion in the settings of acute GI bleeding. 11
In the previously reported lansoprazole-induced thrombocytopenia case, the patient received a dose of 60 mg every 12 hours as a treatment for GI bleeding, while in the present case, the patient was on 30 mg daily. 13 This might suggest that this ADR is unlikely to be dose-related.
In the present case, our patient did not develop thrombocytopenia when he was previously prescribed another PPI (pantoprazole), indicating different effects of individual PPIs on platelet counts in the same patient. The same finding was reported by Kallam et al, where the patient had thrombocytopenia with pantoprazole but not with omeprazole. 12
There are several mechanisms for DIT, including drug-dependent antiplatelet antibodies (DDAb), bone marrow toxicity, or thrombocytopenia induced by Arginine-glycine-aspartic acid mimetic platelet inhibitors. 18 Daniel and his colleagues reported a positive testing for lansoprazole-dependent platelet-reactive antibodies, which suggested that DDAb may be the mechanism of lansoprazole-induced thrombocytopenia. 14 In another case report, an 80-year-old woman was admitted with jaundice, anemia, and thrombocytopenia associated with bleeding tendency after 5 weeks from starting omeprazole, when platelet-associated IgG (PAIgG) was measured, it was found to be elevated. After stopping omeprazole, hemoglobin and platelets counts start to increase gradually, and on day 27 of hospital stay, PAIgG came back to normal. 8 Unfortunately, platelet-reactive antibodies were not tested in the present case due to unavailability of the test in our institution.
In the present case, no bleeding occurred during the period of thrombocytopenia and platelet counts recovered spontaneously after discontinuation of lansoprazole. Our patient was treated conservatively without platelet transfusion as the patient didn’t develop bleeding and his platelets didn’t drop less than 20 × 103/µL. 19
Further studies are needed to exactly address the mechanism of this ADR and identify whether one PPI is safer than the other in this regard.
Conclusion
Lansoprazole may cause thrombocytopenia. However, patients who develop lansoprazole-induced thrombocytopenia may tolerate other PPIs. Clinicians should be vigilant to such ADRs when other common causes of thrombocytopenia are excluded.
Footnotes
Appendix A. Naranjo ADR Probability Scale
Abbreviation: ADR, adverse drug reaction. Score interpretation: above 9 = highly probable, 5-8 = probable, 1-4 = possible, and 0 = doubtful. Source: Naranjo et al.
15
Question
Yes
No
Don’t Know
Score
1.
Are there previous conclusive reports on this reaction?
+1
0
0
0
2.
Did the adverse event appear after the suspected drug was administered?
+2
−1
0
+2
3.
Did the adverse reaction improve when the drug was discontinued, or a specific antagonist was administered?
+1
0
0
+1
4.
Did the adverse reaction reappear when the drug was readministered?
+2
−1
0
+2
5.
Are there alternative causes (other than the drug) that could on their own have caused the reaction?
−1
+2
0
+2
6.
Did the reaction reappear when a placebo was given?
−1
+1
0
0
7.
Was the drug detected in the blood (or other fluids) in concentrations known to be toxic?
+1
0
0
0
8.
Was the reaction more severe when the dose was increased or less severe when the dose was decreased?
+1
0
0
0
9.
Did the patient have a similar reaction to the same or similar drug in any previous exposure?
+1
0
0
0
10.
Was the adverse event confirmed by any objective evidence?
+1
0
0
1
Total score
8 (probable)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.