
Abstract
Heart failure is associated with increased risk of morbidity and mortality, resulting in substantial health-care costs. Clinical pharmacists have an opportunity to reduce health-care costs and improve disease management as patients transition from inpatient to outpatient care by leading interventions to develop patient care plans, educate patients and clinicians, prevent adverse drug reactions, reconcile medications, monitor drug levels, and improve medication access and adherence. Through these methods, clinical pharmacists are able to reduce rates of hospitalization, readmission, and mortality. In addition, care by clinical pharmacists can improve dosing levels and adherence to guideline-directed therapies. A greater benefit in patient management occurs when clinical pharmacists collaborate with other members of the health-care team, emphasizing the importance of heart failure treatment by a multidisciplinary health-care team. Education is a key area in which clinical pharmacists can improve care of patients with heart failure and should not be limited to patients. Clinical pharmacists should provide education to all members of the health-care team and introduce them to new therapies that may further improve the management of heart failure. The objective of this review is to detail the numerous opportunities that clinical pharmacists have to improve the management of heart failure and reduce health-care costs as part of a multidisciplinary health-care team.
Introduction
Heart failure (HF) is a life-threatening chronic condition in which one or more abnormalities in cardiac structure or function lead to the inability of the heart to deliver sufficient oxygen necessary for cellular metabolism. 1 HF ranks among the most common causes of hospital admission in adults ≥65 years of age, 2 making it one of the most costly conditions in the United States. In 2012, the total estimated cost of HF was approximately US$31 billion, and this value is projected to approach US$70 billion by 2030. 3 Furthermore, these values underestimate the true costs of the disease and the burden of HF on the US health-care system. 4
Urgent hospitalization is often required for episodes of acute HF (AHF), which may be new presentations of HF or an exacerbation of chronic HF. 5 A number of factors can precipitate these acute episodes, including arrhythmias, ischemia, uncontrolled hypertension, pneumonia, and nonadherence to diet and medications. 5 Steps must be taken to effectively manage chronic HF including adherence to diet and medications. 5
Across the continuum of health care, clinical pharmacists are well positioned to influence HF management and associated costs by addressing medication-related issues such as developing patient care plans, educating patients and clinicians, preventing adverse reactions, reconciling medications, monitoring drug levels, and improving medication access and adherence. 6 Accumulating evidence suggests benefits for clinical pharmacists’ participation in intensive care unit (ICU)/coronary care unit (CCU) consultation, discharge education, and as members of outpatient health-care services. 6
The importance of pharmacist care in the treatment of HF was demonstrated in a systematic literature review of both inpatient and outpatient studies by Koshman et al. 7 This study found that patients who received pharmacist-directed care experienced a reduced rate of all-cause hospitalization (odds ratio [OR]: 0.71; 95% confidence interval [CI]: 0.54-0.94) and HF-related hospitalization (OR: 0.69; 95% CI: 0.51-0.94). Interestingly, collaborative pharmacist care led to greater reductions in HF hospitalization rates than pharmacist-directed care, emphasizing the importance of partnerships among patients, clinical pharmacists, and other members of the HF management team. 7 Additionally, in a recent systematic review of pharmacist-directed patient care, clinical pharmacy services were generally found to be cost-effective or to provide a good benefit-to-cost ratio. 8
The Heart Failure Society of America (HFSA) and the American College of Clinical Pharmacy Cardiology Practice and Research Network recently published an opinion on clinical pharmacy services in HF, outlining the roles for pharmacists in various aspects of care as well as evidence to support the value of such participation. 6 This article provides a clinically focused update on the approach to managing HF as patients transition from the emergency department through various aspects of inpatient care, and finally into outpatient care. Opportunities for clinical pharmacist intervention are discussed in each of these settings.
Pathophysiology
HF occurs when abnormalities in cardiac structure, function, rhythm, or conduction impair the ability of the heart to fill with or eject blood. 9 Most cases result from ventricular dysfunction due to myocardial infarction (systolic dysfunction), hypertension (systolic and diastolic dysfunction), or both. 9 Idiopathic or alcoholic cardiomyopathy and degenerative valve disease are other common causes. 9 These conditions can usually be effectively managed in patients with chronic HF, which can help prevent the need for hospitalization.
A number of different pathophysiologic mechanisms for AHF have been proposed, although the extent to which they are related and the underlying sequence of events are unclear. Cardiac structure and function, as well as hemodynamic abnormalities, are generally highly variable at HF presentation. It is believed that the population with HF is equally divided between patients with a reduced ejection fraction (HFrEF) and patients with a preserved ejection fraction (HFpEF). 10 A left ventricular ejection fraction ≤40% is generally defined as HFrEF and a left ventricular ejection fraction ≥50% commonly denotes HFpEF. Patients with an ejection fraction from 41% to 49% are considered borderline HFpEF and have similar characteristics and treatment patterns to patients with HFpEF. The clinical syndrome of HF results from progressive deterioration of cardiac structure and function. The condition is characterized by disruption of the natural balance between the natriuretic peptide system as well as other compensatory peptides (eg, bradykinin, adrenomedullin, etc) and pathophysiologic mediators of cardiovascular disease such as the renin–angiotensin–aldosterone system (RAAS) and the sympathetic nervous system. 11,12 Activity of the RAAS is elevated in patients with HF, resulting in alterations in blood volume, arterial pressure, and cardiac structure and function. Chronic stimulation of the RAAS, along with inadequate activation of or diminished response to compensatory peptides, leads to progression of HF and increased adverse cardiovascular effects. 11
The natriuretic peptide system counterregulates the effects of RAAS and sympathetic nervous system hormones via reductions in vascular tone and intravascular volume, inhibition of deleterious neurohormonal mediators, attenuation of tissue remodeling, and improvement in metabolic parameters. 12 The system consists of neurohormones synthesized by organs including the heart and brain. Increased secretion of these hormones occurs with cardiovascular diseases, such as chronic HF, in an attempt to normalize cardiovascular health. These hormones participate in long-term regulation of blood volume, arterial pressure, and sodium and water balance and they also decrease central venous pressure—reducing cardiac output—as well as increase glomerular filtration rate at the renal level. This activity results in natriuresis, diuresis, and decreased edema. Other effects are reduction in renin release through direct inhibition of renin production from cells in the juxtaglomerular apparatus and decreases in circulating levels of angiotensin II and aldosterone, resulting in further natriuresis and diuresis. The effects of the natriuretic peptide system in HF cannot overcome the chronic overstimulation of the RAAS and sympathetic nervous system, which lead to progression of disease and acute events.
There are a number of other potential contributory mechanisms to changes in cardiac structure and function, including processes that mediate myocyte damage, inflammation, oxidative stress, extracellular matrix regulation, and endothelial dysfunction. Beyond changes in cardiac structure and function, aspects of fluid status and renal function may play critical roles in the underlying pathophysiology of HF in a given patient. These include congestion, sodium and accompanying fluid retention, a blunted natriuretic peptide system, renal dysfunction, volume overload with increased renal vein pressure, and an attenuated response to oral diuretic therapy. In a patient with previously diagnosed chronic HF, a wide range of potential precipitants and causes of AHF exist that may result in either rapid or more gradual deterioration (Table 1).
Precipitants and Causes of Heart Failure.a
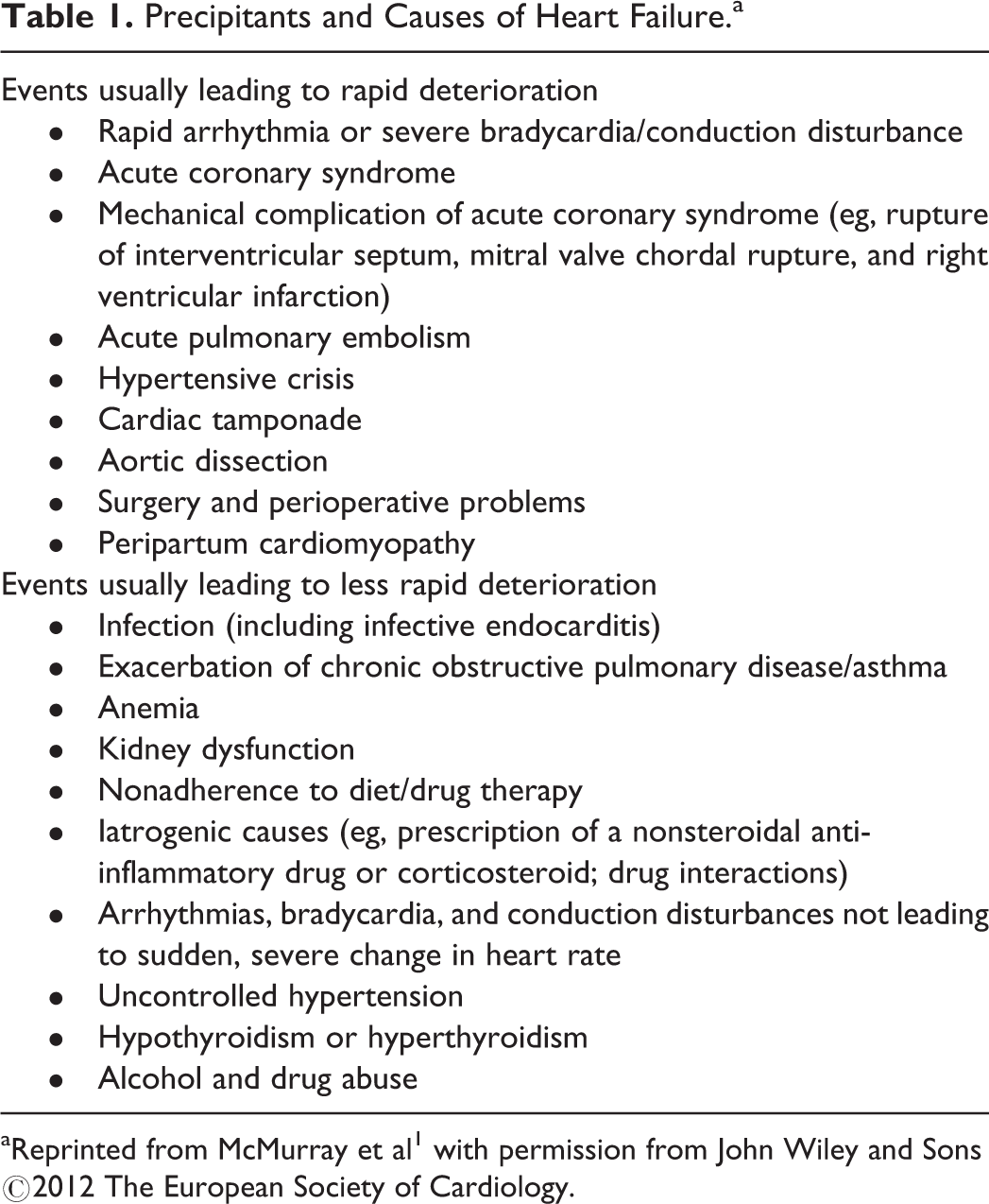
aReprinted from McMurray et al 1 with permission from John Wiley and Sons ©2012 The European Society of Cardiology.
It is important to note that the signs and symptoms of HF in a given patient often change during the transition from the emergency department to the CCU to ongoing inpatient and outpatient care. The goals of treatment during these transitions (Table 2) change, and the clinical pharmacist has different responsibilities in managing HF across care settings as illustrated in Figure 1.
Treatment Goals for Patients Admitted for Acute Heart Failure.a
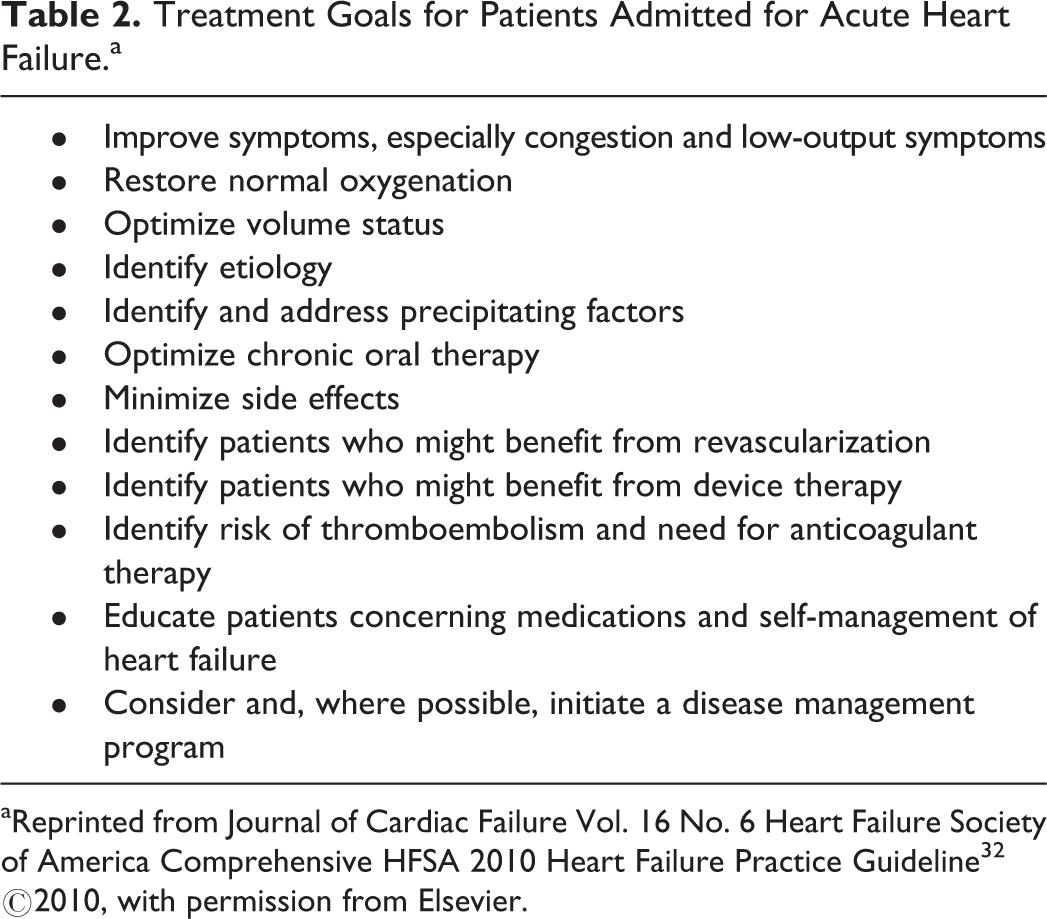
aReprinted from Journal of Cardiac Failure Vol. 16 No. 6 Heart Failure Society of America Comprehensive HFSA 2010 Heart Failure Practice Guideline 32 ©2010, with permission from Elsevier.
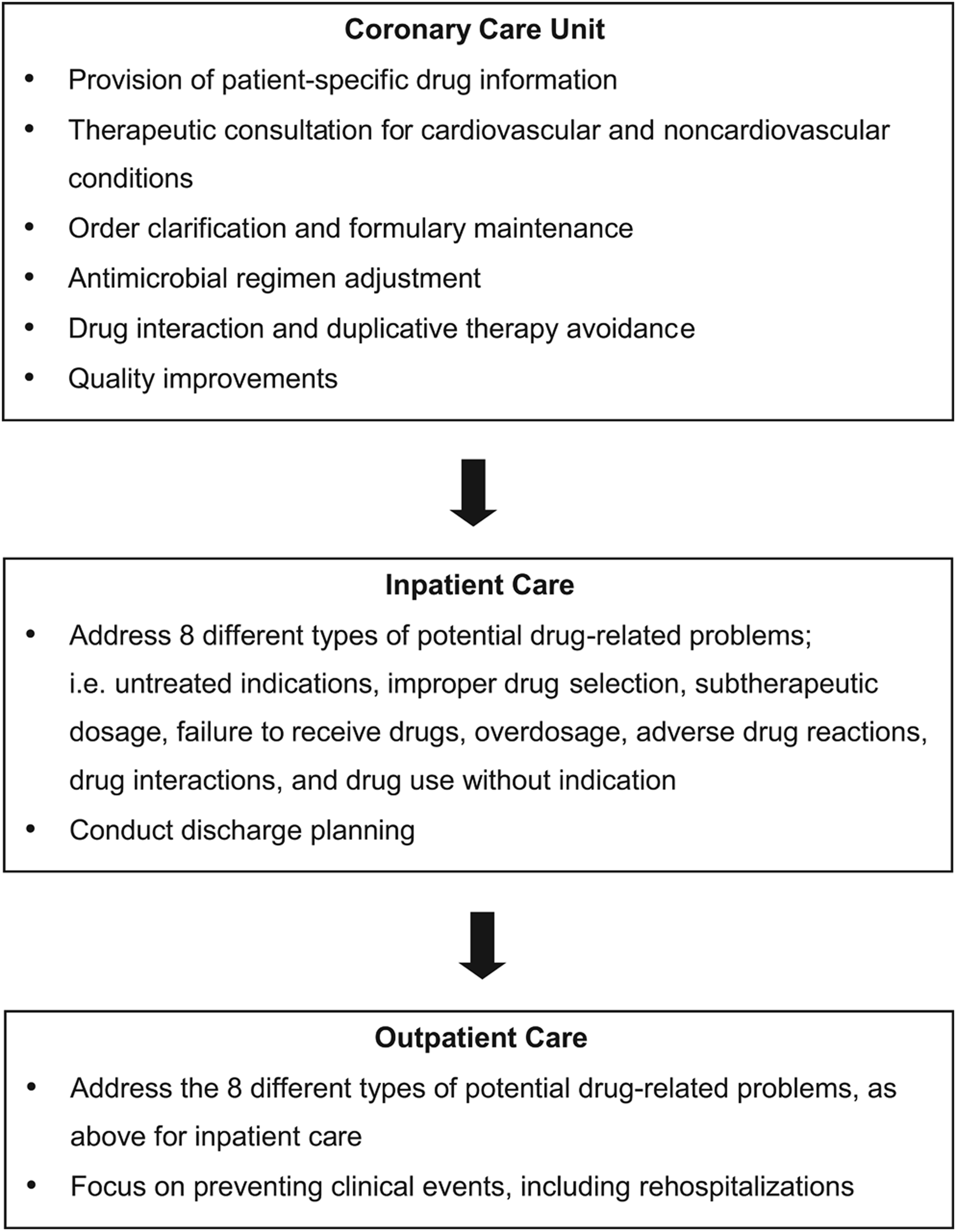
Clinical pharmacist involvement across the continuum of heart failure management.
Opportunities for Clinical Pharmacists in the Care of Patients With HF
Multidisciplinary-coordinated inpatient care, discharge planning, and subsequent outpatient care are critical areas where clinical pharmacists can contribute to optimal management and care of patients with HF. 13 –15 Clinical pharmacists can play an important role in improving the care of individuals with HF by providing education to patients, caregivers, physicians, and nurses about proper dosing strategies and considerations for improving medication adherence. Clinical pharmacists also can help monitor and track medication refills to ensure that patients are taking their medications as prescribed. We discuss in this article opportunities in which clinical pharmacists may improve patient management and outcomes in HF.
ICU/CCU Setting
The clinical pharmacist has numerous responsibilities in caring for patients in an ICU, and critical care pharmacy services have been found to reduce medication errors and adverse events. 16,17 Pharmacotherapy in the setting of AHF is initially tailored according to hemodynamic status, with efforts to alleviate fluid overload, hypoperfusion, or both. 18 The 4 Forrester hemodynamic subsets, based on cardiac index and pulmonary capillary wedge pressure, are used to guide decision-making in patients with AHF (Figure 2). 18,19
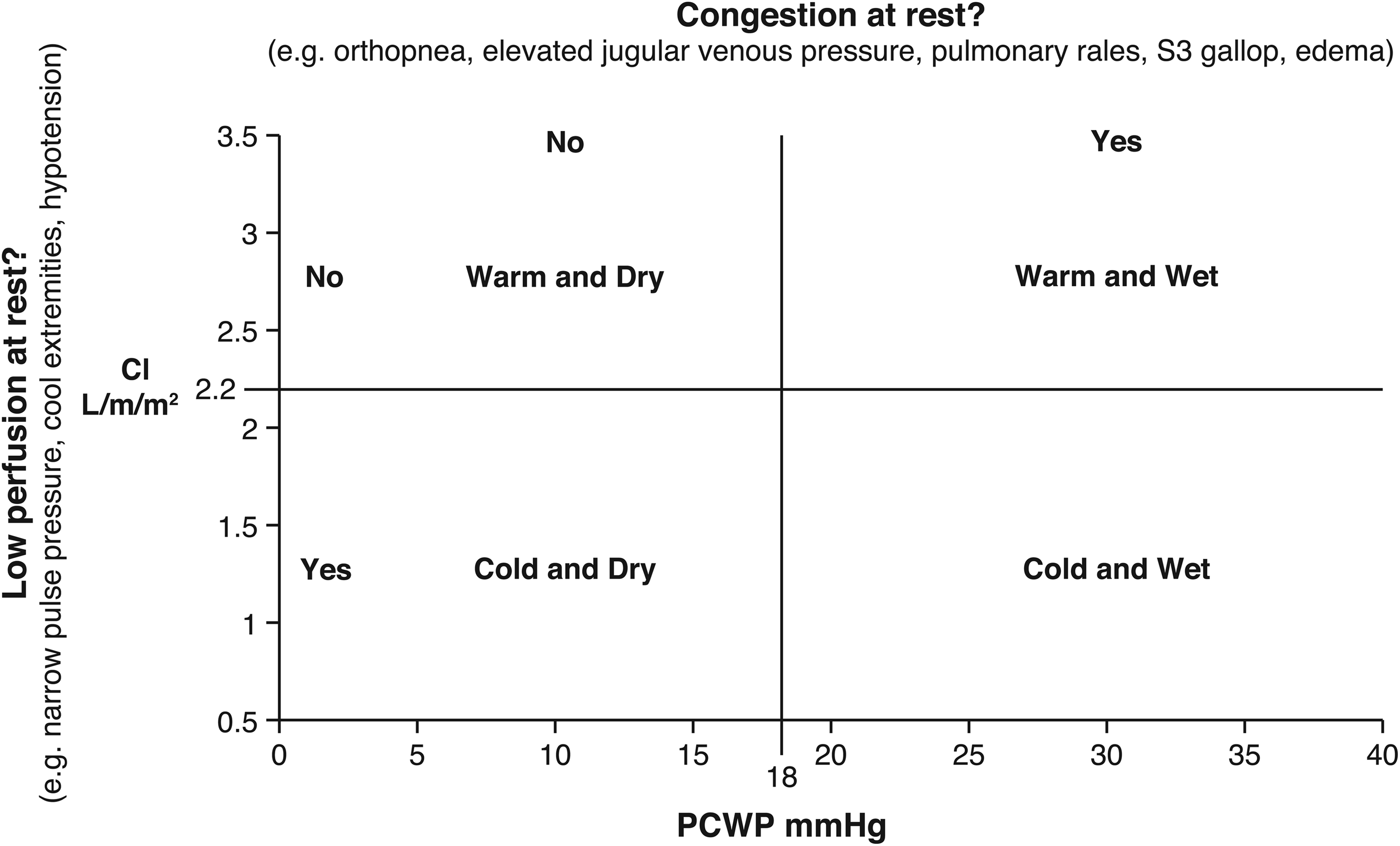
Classification of patients presenting with acute heart failure. Adapted with permission from Circulation 2013;128:e240-e327 10 ©2013, American Heart Association, Inc. CI indicates cardiac index; PCWP, pulmonary capillary wedge pressure.
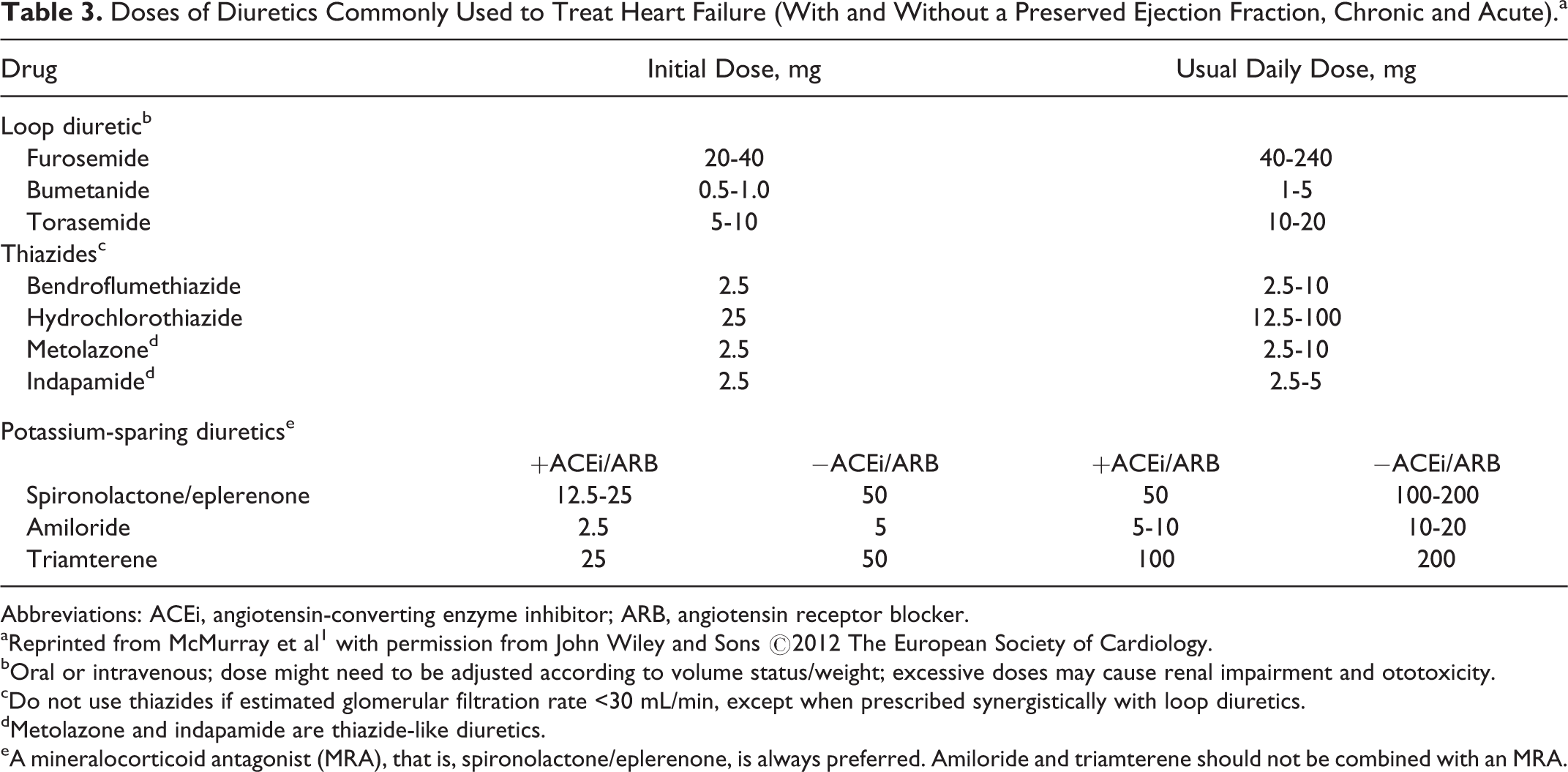
Intravenous loop diuretic therapy forms the cornerstone of managing Forrester subsets II or IV (wet or congestive). 18 See Table 3 for doses of diuretics that are commonly used to treat HF. Considerations for improving diuresis include administering loop diuretics via continuous infusion, adding a second diuretic with a different mechanism of action such as the thiazide metolazone and adding a vasodilator when symptoms persist in the setting of intense diuresis. 18 A recent retrospective cohort study (N = 55) evaluating the efficacy and safety of oral metolazone versus intravenous chlorothiazide as an add-on therapy to loop diuretics in patients hospitalized with acute decompensated HF and renal dysfunction found sequential nephron blockade with either thiazide-like diuretic medication to be safe and efficacious but noted the considerable cost difference favoring oral metolazone. 20 A meta-analysis of 19 randomized clinical trials (N = 112 113) assessing the cardioprotective effects of thiazide diuretic treatment in patients with hypertension also reported that thiazide-like diuretics had greater protective effect against cardiac events than thiazide-type diuretics, especially on HF. 21 In a comparison of furosemide administered at high or low dose or by bolus with continuous infusion, the high-dose strategy was associated with greater diuresis, although it also resulted in transient worsening of renal function. 22 It has been noted in other studies that increased diuresis was not observed with the continuous infusion of furosemide. 23 This could be due to the use of a continuous infusion placebo that increased the time patients were supine, a position that enhances diuresis. Loop diuretics also have been shown to increase length of ICU and hospital stay. 24 However, higher doses of diuretics may be given to patients with more severe AHF and prospective studies are necessary to fully understand the relationship between diuretic use and adverse outcomes. 25
Doses of Diuretics Commonly Used to Treat Heart Failure (With and Without a Preserved Ejection Fraction, Chronic and Acute).a
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
aReprinted from McMurray et al 1 with permission from John Wiley and Sons ©2012 The European Society of Cardiology.
bOral or intravenous; dose might need to be adjusted according to volume status/weight; excessive doses may cause renal impairment and ototoxicity.
cDo not use thiazides if estimated glomerular filtration rate <30 mL/min, except when prescribed synergistically with loop diuretics.
dMetolazone and indapamide are thiazide-like diuretics.
eA mineralocorticoid antagonist (MRA), that is, spironolactone/eplerenone, is always preferred. Amiloride and triamterene should not be combined with an MRA.
Once optimal diuretic therapy has been achieved, treatment with an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) and, when appropriate, a β-blocker is initiated. Recommended starting doses for these medications are provided in Table 4. Initiation of β-blocker therapy may be considered at this point because patients have been reported to be more adherent to β-blockers when they were started during the inpatient period (vs when started in an outpatient setting). 26 Gattis and colleagues found that, at 60 days postdischarge, patients who began therapy with the β-blocker carvedilol as an inpatient were more likely to remain adherent compared with those who began β-blocker therapy after hospital discharge (91.2% vs 73.4%; P < .0001), with no increase in length of hospital stay or risk of adverse events. Patients in the early treatment group also were more likely to achieve a higher mean percentage of their target β-blocker dose (36.3% vs 28.6%; P = .02). 26 Clinical pharmacists can play an important role in achieving target doses and optimizing medication adherence for this class of drugs by recommending that β-blocker therapy is initiated before hospital discharge.
Evidence-Based Doses of Disease-Modifying Drugs Used in Key Randomized Trials in Heart Failure (or After Myocardial Infarction).a
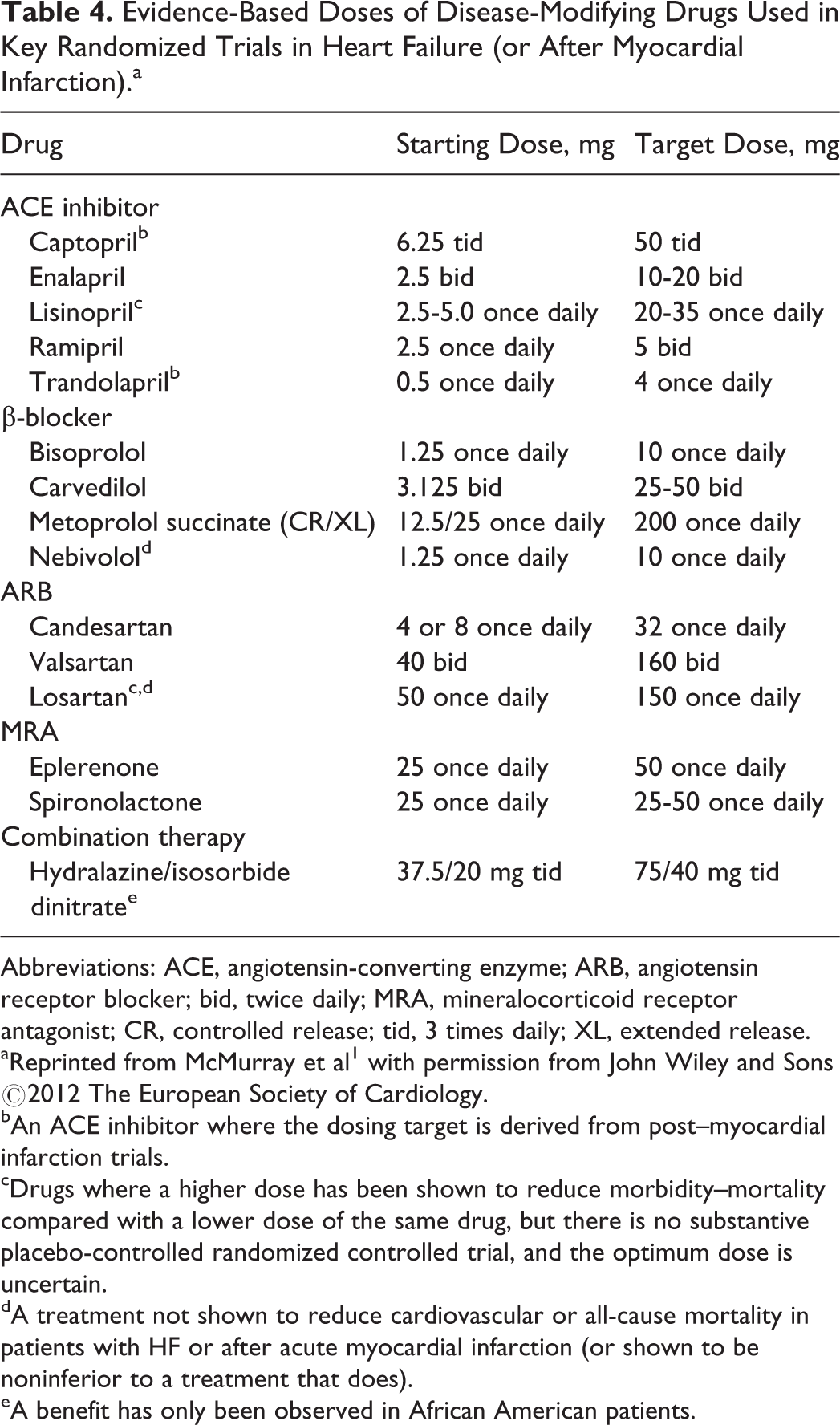
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; bid, twice daily; MRA, mineralocorticoid receptor antagonist; CR, controlled release; tid, 3 times daily; XL, extended release.
aReprinted from McMurray et al 1 with permission from John Wiley and Sons ©2012 The European Society of Cardiology.
bAn ACE inhibitor where the dosing target is derived from post–myocardial infarction trials.
cDrugs where a higher dose has been shown to reduce morbidity–mortality compared with a lower dose of the same drug, but there is no substantive placebo-controlled randomized controlled trial, and the optimum dose is uncertain.
dA treatment not shown to reduce cardiovascular or all-cause mortality in patients with HF or after acute myocardial infarction (or shown to be noninferior to a treatment that does).
eA benefit has only been observed in African American patients.
Intravenous inotrope therapy (Table 5) is frequently used for subsets III or IV (cold or hypoperfusion) and is indicated in patients with shock or impending shock and/or end-organ perfusion limitation, 18 but treatment with these agents remains controversial for long-term or outpatient therapy. 27 The etiology of HF must also be considered when administering inotropes because they have been shown to be deleterious in ischemic HF but have neutral or beneficial effects in nonischemic HF. 28
Positive Inotropes Used to Treat Acute Heart Failure.a
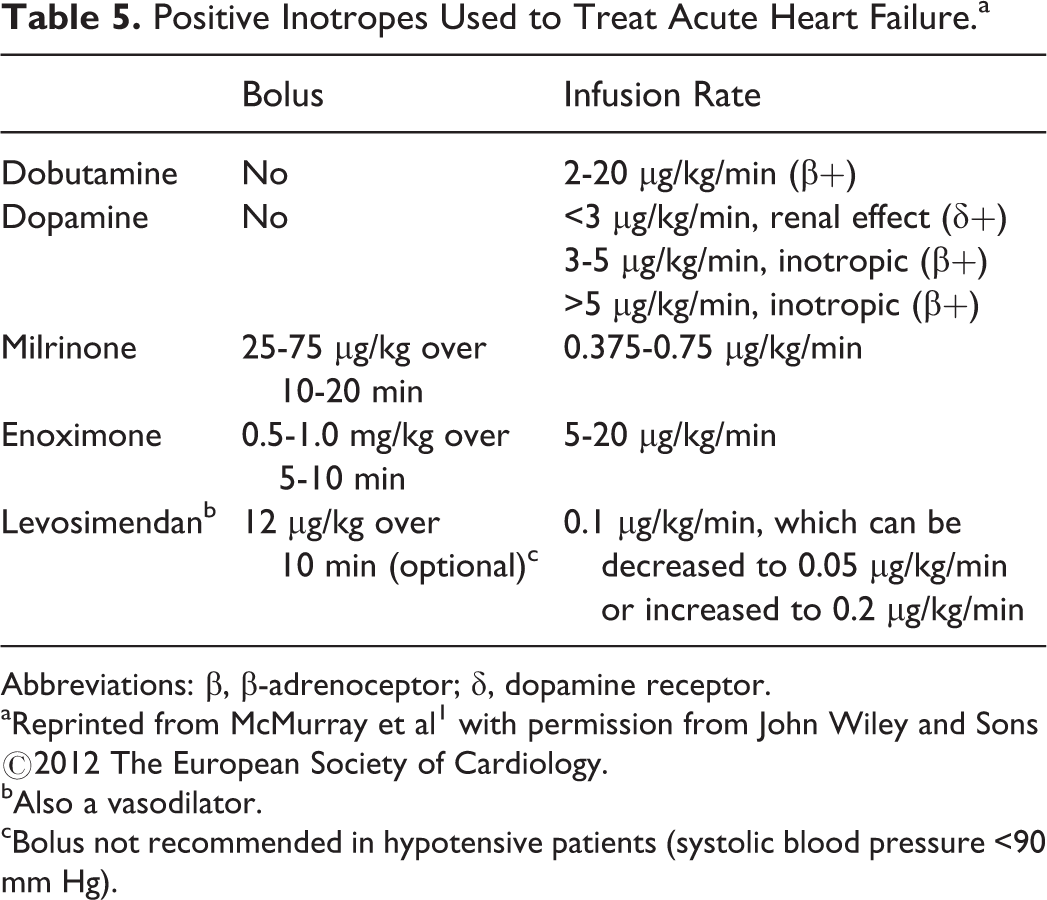
Abbreviations: β, β-adrenoceptor; δ, dopamine receptor.
aReprinted from McMurray et al 1 with permission from John Wiley and Sons ©2012 The European Society of Cardiology.
bAlso a vasodilator.
cBolus not recommended in hypotensive patients (systolic blood pressure <90 mm Hg).
Clinical pharmacist involvement in the CCU confers economic benefits that can lead to substantial cost savings. Gandhi and colleagues published a study on the impact of clinical pharmacy services on direct drug costs in a CCU where they found that clinical pharmacist intervention leads to a reduction in mean drug costs per admission from US$374 during the nonintervention period to US$234 during an intervention period (P = .002). It was estimated that savings associated with reduced drug costs totaled US$372 384 over 1 year. 29 An investigation of focused rounds by clinical pharmacists in a CCU noted an estimated net cost savings of US$2219 was achieved over a 14-day period. 30 Common clinical pharmacist interventions in the CCU from these 2 studies include the provision of patient-specific drug information, therapeutic consultation for cardiovascular and noncardiovascular conditions, order clarification and formulary maintenance, antimicrobial regimen adjustment, drug interaction and duplicative therapy avoidance, and quality improvements. 6 For example, while evaluating patients in the CCU setting, the clinical pharmacist could optimize titration of inotropic agents while recommending an agent with a proven mortality benefit or recommend discontinuation of contraindicated medications and/or medications without an indication. 6 Clinical pharmacists also can assist by identifying potential drug–drug, drug–nutrient, and drug–disease interactions. 6 Overall, clinical pharmacists play a crucial role in patient care in the ICU setting, where their recommendations regarding optimal pharmacotherapy initiation, dosage and timing, and treatment goals can improve patient outcomes.
Nonemergency Care
Clinical pharmacists are well positioned to assist with the coordination of care across practitioners in the inpatient setting. They may help to resolve any of the 8 different types of potential medication-related problems, which are untreated indications, improper medication selection, subtherapeutic dose(s), failure to receive medications, overdosage, adverse medication reactions, medication interactions, and medication use without indication. 6 Many of these problems relate to both discharge planning and the outpatient setting, and examples commonly found in the treatment of HF are provided in Table 6.
Examples of Common Medication-Related Problems Encountered in HF.a
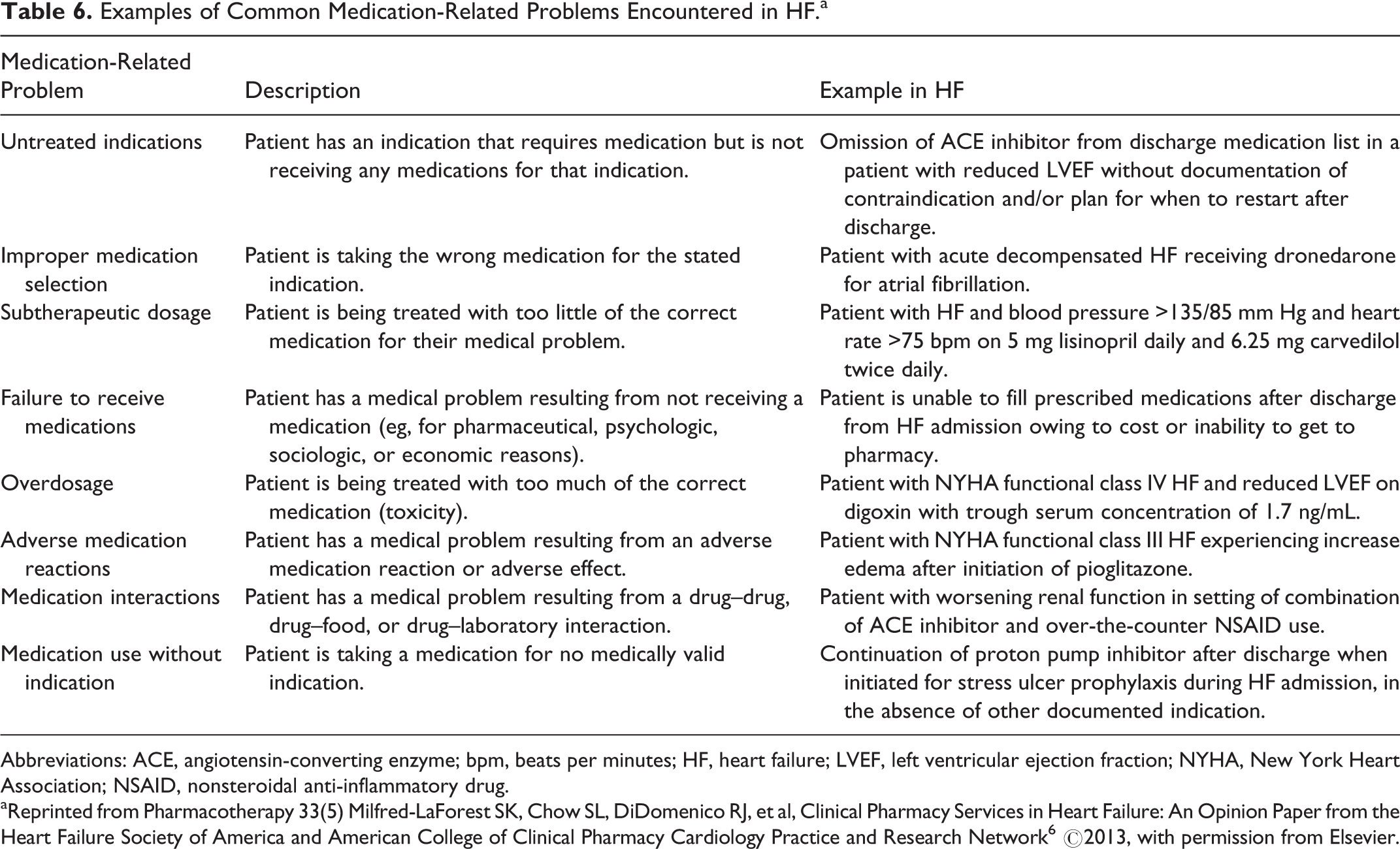
Abbreviations: ACE, angiotensin-converting enzyme; bpm, beats per minutes; HF, heart failure; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; NSAID, nonsteroidal anti-inflammatory drug.
aReprinted from Pharmacotherapy 33(5) Milfred-LaForest SK, Chow SL, DiDomenico RJ, et al, Clinical Pharmacy Services in Heart Failure: An Opinion Paper from the Heart Failure Society of America and American College of Clinical Pharmacy Cardiology Practice and Research Network 6 ©2013, with permission from Elsevier.
Clinical pharmacists working with nurses in the management of HF can help provide patient education and identify challenges that can lead to medication nonadherence. Patient education should begin before discharge and continue into the outpatient setting. A randomized controlled study of patients with HF in an acute-care facility was conducted to examine the effect of a clinical pharmacist and clinical nurse specialist team who identified patient issues (eg, medication nonadherence, adverse drug reactions) posing potential risk for rehospitalization and determined corrective action. 15 The pharmacist could, if necessary, recommend medication changes to physicians. The control group received regular care (ie, discharge counseling and printed medication information). Readmission related to HF within 1 year of discharge was significantly lower in the intervention group (4 [23.5%] of 17 vs 10 [58.8%] of 17; P <.05), as was death or readmission (5 [29.4%] of 17 vs 14 [82.3%] of 17; P < .01), demonstrating that clinical pharmacist participation in coordinating clinical services in the acute-care setting contributed to positive outcomes for patients with HF. 15
Medication dosages should target levels shown to improve heart function (Table 4), and dosage levels should not be based on specific blood pressure readings or symptom relief. It should be noted that the commonly used dosing levels for many therapies are well below the target levels, and increased dosing may result in improved patient outcomes (reduced morbidity and mortality) even if patients appear to be stable and well managed. Patients identified as being intolerant to ACE inhibitors or β-blockers should be encouraged to try the medication again because these therapies have few contraindications and have been demonstrated to improve patient outcomes. 31
Discharge Planning
The importance of discharge planning and follow-up is advocated by the American College of Cardiology/American Heart Association (ACC/AHA) and HFSA guidelines. 10,32 Components of evidenced-based discharge care include treating exacerbating factors, achieving and maintaining optimal volume state, and transitioning to outpatient oral therapy. 18 Participation in discharge planning allows for clinical pharmacists to offer education related to safe and effective medication use while also facilitating the dispensing of medication at the time of discharge. 6
Many patients are admitted to the hospital during their initial diagnosis of HF. During their admission, a patient can be initiated and discontinued on several therapies prior to discharge. A clinical pharmacist plays an important role in educating the patient of these medication changes and their importance in the management of HF. The American College of Clinical Pharmacy’s Cardiology Practice and Research Network developed a best practices model for discharge counseling among patients hospitalized for HF and myocardial infarction. 33 This model emphasizes the need for education related to general disease-state information (including risk factors, complications, and signs and symptoms of exacerbation), safe and appropriate medication use, the postdischarge follow-up plan, therapeutic interventions directed against modifiable HF-related risk factors, and lifestyle modifications. 33 Patient education provided by a clinical pharmacist on the day of hospital discharge regarding the pathogenesis and symptoms of HF, diet, and pharmacotherapy, with regular follow-up by telephone, has been shown to reduce mortality (12.9% vs 29.7%; P < .05) and adjusted rates of rehospitalization (hazard ratio [HR]: 0.56; 95% CI: 0.32-0.97) at 12 months, compared with no clinical pharmacist intervention. 13
Clinical pharmacists should be proactive in engaging physicians, patients, social workers, nurses who follow up with patients out of the hospital, and caregivers to discuss and resolve any logistical, psychological, or socioeconomic barriers to obtaining and administering prescribed therapies. It is important to ensure the implementation of ACE inhibitors (or ARBs), β-blockers, and mineralocorticoid receptor antagonists or document the specific reasons why such agents are not appropriate. 6,34,35 Pharmacists also should contribute to educating patients about the purpose of their prescribed medications to ensure that they can accurately explain the medication and its intended use to others (ie, to the staff of a hospital that does not have a patient’s medical records or to physicians who may not understand the need for, and importance of, these therapies). By educating patients to be their own advocates, they can be empowered to ensure that they continue to receive their intended therapies and they can help prevent unnecessary or incorrect changes throughout the transitions of care that could reduce heart function and result in the need for hospitalization.
Underutilization of evidence-based therapies has been identified as a clinical problem in the population with HF. 34 The underlying reasons as to why evidence-based guidelines are not routinely applied in real-world practice are not fully understood, but potential contributing factors include clinician inertia (eg, reluctance to add a new therapy, which may apply to stable patients with mild to moderate disease as well as clinically unstable patients with advanced disease), lack of data to guide use in specific patient subsets that tend to be underrepresented in clinical trials (eg, minorities, women, and elderly patients), dosing variability, and concerns related to polypharmacy, cost, and tolerability/adverse events. Interventions by clinical pharmacists in inpatient and outpatient settings can help achieve optimal prescribing of evidence-based HF medications, ultimately leading to improved patient outcomes.
Outpatient Care
The overarching goal of outpatient care is to prevent hospitalizations, rehospitalizations, and mortality due to acute decompensation. The ACC/AHA guidelines recommend follow-up by telephone within 3 days of discharge and a follow-up visit within 7 to 14 days of discharge. 10 The clinical pharmacist can help improve outpatient care by educating patients and identifying methods to improve drug adherence in collaboration with primary care physicians and cardiologists.
The benefit of adding a clinical pharmacist to a multidisciplinary outpatient HF team was demonstrated in the Pharmacist in Heart Failure Assessment Recommendation and Monitoring Study. 36 In this study, 181 patients with HF and left ventricular dysfunction were randomized to undergo clinical pharmacist evaluation (including medication evaluation, therapeutic recommendations to the attending physician, patient education, and follow-up telemonitoring) or usual care. There was a median follow-up time of 6 months after which patients in the clinical pharmacist intervention group experienced a significantly lower incidence of all-cause mortality and HF events compared with those receiving standard care (4 vs 16; OR: 0.22; 95% CI: 0.07-0.65; P = .005). Patients in the clinical pharmacist intervention group were also more likely to receive dosages of ACE inhibitors closer to target levels (median fraction of target dose [25th and 75th percentile]: 1.0 [0.5 and 1] vs 0.5 [0.1875 and 1]; P < .001), and patients not receiving ACE inhibitors were more likely to receive alternative vasodilator therapy (75% vs 26%; P = .02). 36
A separate outpatient trial assessed the effect of a clinical pharmacist educating elderly patients (>65 years) with HF on HF pathophysiology, prescribed medications, and symptom management. This approach was shown to decrease medication nonadherence (27% vs 75%) and reduce hospital readmissions (33% vs 66%; P = .006) compared with patients who did not receive the intervention. 37 A collaborative relationship between physician and pharmacist also has been shown to benefit patients with HF. A study of veterans with HF who received a general practitioner–pharmacist collaborative home medication review reported that adjusted results showed a 45% reduction in the rate of HF-related hospitalizations compared with veterans who did not receive this review (HR: 0.55; 95% CI: 0.39-0.77). 38 The review also included a home visit by the pharmacist to resolve mediation-related issues.
Medication review and evaluation via the pharmacist can also help increase the rate of appropriate use of treatments and reduce subsequent rates of hospitalization with, consequently, reductions in health-care costs. In an outpatient trial in 117 patients with recent congestive HF hospitalization, an ejection fraction less than 20%, or symptoms consistent with New York Heart Association class III or IV HF, pharmacists provided medication and educational material review with patients, as well as medication evaluation to physicians with subsequent team-coordinated initiation of a plan for further diagnostic evaluation, medication titration, and follow-up. This intervention resulted in increased β-blocker use (76% vs 52%; P < .01), higher attainment of target β-blocker dose level (13% vs 6%; P < .01), and a decreased hospitalization rate (1.5 vs 0 hospitalizations per patient-year; P < .01). 39 This trial also reported that outpatient pharmacist intervention resulted in a median total costs savings of US$8571 per patient-year. 39 Medication adherence rates also have been observed to improve by 32% (P < .001) in patients with HF who received intensive, home-based medication counseling by a pharmacist. 40 Taken together, the results of these outpatient trials of pharmacist interventions/collaborations demonstrate the clear benefit that clinical pharmacists can have in improving outpatient care for patients with HF.
Pharmacists should be vigilant of the need to uptitrate medications to guideline-directed therapeutic doses in order to prevent decompensation and the need for hospitalization. 1 Even if a patient seems stable, medications should be uptitrated to guideline-directed dosage levels to improve disease management. The implementation of a pharmacist-managed, outpatient HF medication titration clinic was found to significantly increase the proportion of patients achieving optimal doses of evidence-based therapies and highlights the expanding role of pharmacists in making treatment decisions. 41 In this study, pharmacists were granted prescribing privileges that allowed them to initiate and adjust medication dosages, and they tracked the patients’ daily body weight, vital signs, volume status, and whether the patient was experiencing adverse events by telemonitoring. Pharmacists made decisions to adjust medication dosages based on this information, clinical judgment, and established protocols during clinic visits, and patient education was also given during the clinic visits to reinforce the importance of dietary and medication adherence as well as the purpose of uptitration. 41
Patient education about HF is another important part of disease management and is an area in which pharmacists can help improve drug adherence and reduce the need for rehospitalization. 37 Although patient education should begin in the inpatient setting, it is important to continue education once patients are discharged. 13 During the outpatient visits, clinical pharmacists can reinforce the mechanism of which medications are being used to treat their HF, the presence of potential side effects, and monitoring parameters. Patients should be instructed to detect signs and symptoms of fluid accumulation so that outpatient intervention can be taken before volume overload requires hospitalization. Daily weight measurements should be conducted after urinating each morning and while wearing the same amount of clothing. Patients should be counseled about how to identify pitting edema in the lower extremities, a common sign of fluid accumulation. Further, patients should pay attention to how clothes and rings fit and should recognize that a lack of appetite can signal fluid accumulation. These signs and symptoms should alert the patient to contact their health-care provider for treatment, which may prevent the need for hospitalization. Dietary changes may also help prevent volume retention. Patients should be advised to restrict sodium intake but also be cautioned that they could become volume depleted if both sodium and fluids are restricted.
In summary, clinical pharmacists are primed to play a critical role in optimizing the care of patients with HF transitioning from the hospital to primary care by performing such tasks as discussing with patients what medications the patient is taking and how and when they are taking them. By opening a dialogue with patients concerning their medications, pharmacists can identify barriers to medication adherence and access (eg, medication affordability) and find solutions to these issues. Additionally, the pharmacist can provide suggestions for adjustment of dosing schedules to improve patient quality of life and the management of symptoms. For example, diuretics can be taken earlier in the evening if the patient is frequently waking at night to urinate or avoided first thing in the morning when the patient is at their driest weight. By making recommendations to personalize treatment, such as by modification of dosing schedules, clinical pharmacists can improve patient care and quality of life and may also improve patient medication adherence.
Conclusion
There are numerous opportunities for clinical pharmacists to positively impact outcomes and reduce health-care costs in HF as key members of the multidisciplinary care team during the early admission period and throughout the subsequent continuum of care. Education is a critical area in which intervention by a clinical pharmacist can improve the management of patients with HF. Importantly, education by clinical pharmacists should not be limited to patients but should encompass all members of the health-care team, including physicians, nurses, social workers, and patient caregivers. The overarching goal of education should be to improve medication adherence, which, in turn, results in improved HF outcomes.
Due to the complex nature of HF, dosing and selection of therapeutic agents must be customized to the individual needs of the patient. Pharmacists can assure therapy optimization of dosing and drug selection to prevent drug–drug interactions and limit adverse effects. Medications should be uptitrated for maximum therapeutic effect, and treatment decisions should focus on improvement of ejection fraction, patient stability, and quality of life. Additionally, maintaining patients on target doses of evidence-based therapies can reduce costs by preventing rehospitalization. Education by pharmacist on medication regimens and adherence is important for the long-term management of HF. However, despite optimal treatment strategies, HF is still associated with significant morbidity and mortality. Therefore, the development and clinical acceptance of new agents that can improve the quality of life and reduce mortality in patients with HF are needed to improve patient management. As these new treatment modalities become available, pharmacists have a primary role in introducing them to the health-care team and maintaining target dosing levels that provide maximal benefit to the patient and health-care system.
Footnotes
Author’s Note
The author was fully responsible for all content and editorial decisions. The opinions expressed in the manuscript are those of the author, and Novartis Pharmaceuticals Corporation had no influence on the contents.
Acknowledgments
Technical assistance with editing and styling of the manuscript for submission was provided by Oxford PharmaGenesis Inc, Newtown, Pennsylvania, and funded by Novartis Pharmaceuticals Corporation, East Hanover, New Jersey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.