
Abstract
Background
Peritoneal dialysis (PD) training and education for patients and their caregivers, provided by PD nurses, are crucial for effective PD programs. The goal is to impart sufficient knowledge, skills, training, and support to minimize complications. However, the evidence regarding effective educational interventions during training has been unclear and inconsistent. The review question was: How do PD training methods and educational interventions impact on PD outcomes in adult patients?
Methods
A narrative review was undertaken with defined inclusion and exclusion criteria of articles published in the last 10 years. Databases were searched, followed by a selection process conducted with the project team. Quality appraisal and a final selection were uploaded to Excel, and data was extracted. A narrative description of the results was then completed.
Results
A total of 982 articles followed the selection process of these 21 studies, including mixed methods research design, but all met the inclusion criteria. The results were described under headings of training methods, educational interventions, patient characteristics, retraining, and outcomes reported.
Conclusions
The narrative review highlights gaps in robust evidence for educational interventions during training. However, some evidence supports adapting PD training methods to incorporate more individualized approaches, appropriate pre-training assessments, and consistent outcome measures.
Introduction
Patients (with their carers) opting for home peritoneal dialysis (PD) must first learn the procedure. This essential PD training, provided by PD nurses, forms the foundation for successful home-based PD programs. However, there is a significant lack of standardization and structured training programs worldwide, leading to considerable variation in the delivery and approaches to PD patient training. 1 Preventing PD-related complications, such as peritonitis and exit-site infections, is crucial. Peritonitis is the leading cause of PD discontinuation PD 2 and persists as a significant challenge in achieving widespread success in PD adoption. Consequently, efforts to enhance training programs and implement targeted educational interventions during training have been the subject of numerous reviews and commentaries. 1 A previous International Society for PD (ISPD) training curriculum has been published to provide guidance and best practice recommendations. 3 The guidelines identified core components to successful training; including skills of the trainer, time dedicated to training, methods and protocols, assessment of learning styles, individual needs and flexible approaches required, home visits and retraining. 3 However, this training curriculum was published 8 years ago and provided a review of published literature available at the time. International Society for PD peritonitis guidelines emphasize the importance of patient training in peritonitis prevention and, in particular, reassessments and retraining. 4 A review of educational interventions published in 2015 included studies published before 2013, and 18 articles were reviewed. 5 This review highlighted the limited progress in establishing evidence for the most effective educational interventions in PD training. 5 A more recent review published on nursing educational interventions focused specifically on self-management interventions and included 11 studies, of which only two were specific to PD training. 6 All these publications and guidelines recognize the lack of evidence for key educational interventions, strategies and core components required for PD training.
Therefore, the purpose of this narrative review was to further update and identify relevant evidence to recommend best practice guidelines for teaching PD to patients and their caregivers.
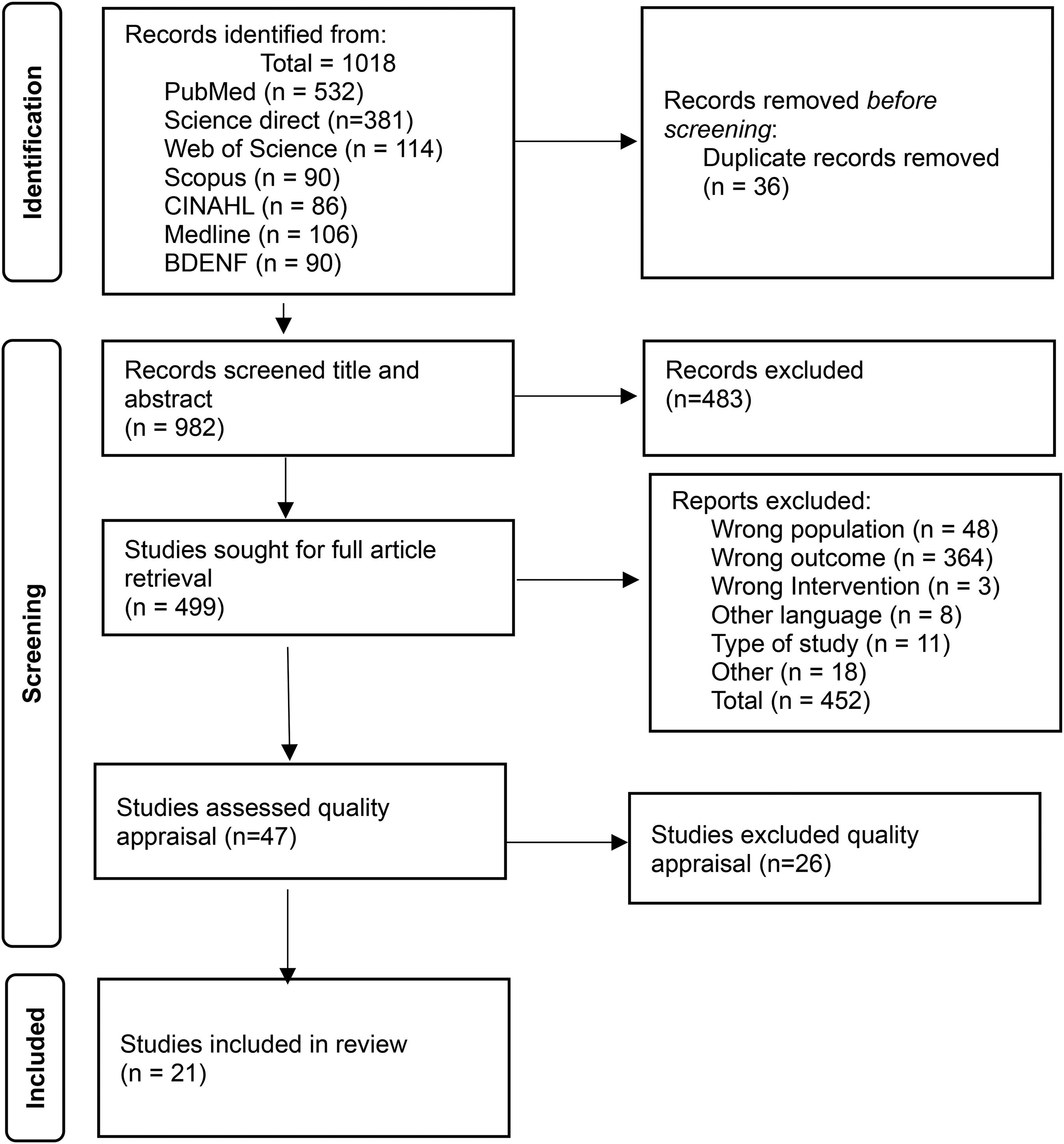
The PRISMA flowchart review identification and selection process.
Methods
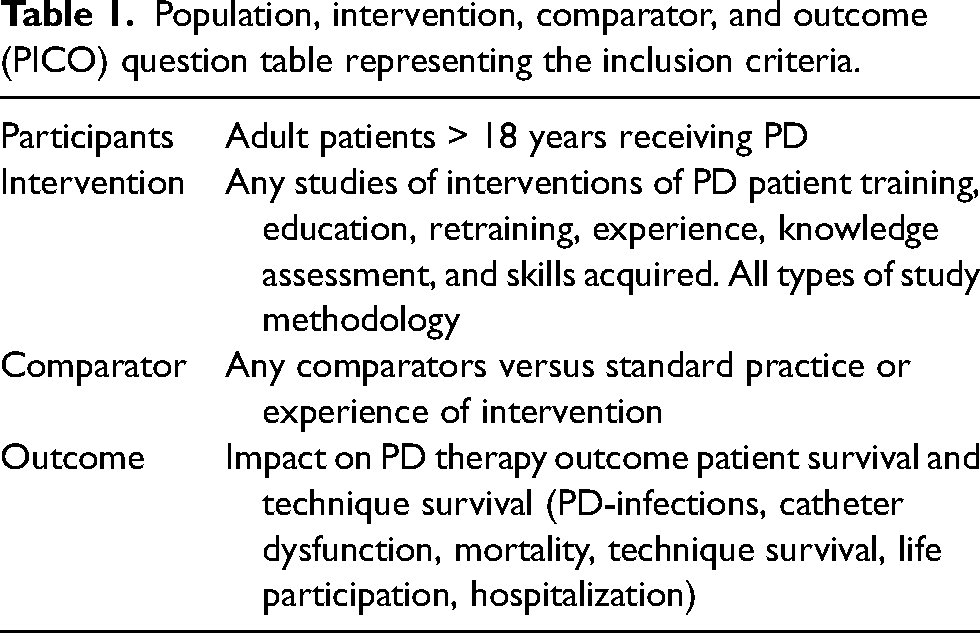
A narrative review was undertaken, incorporating elements of a systematic review process.7,8 A team of seven nurses was convened as part of the ISPD nursing working group of training guidelines (HH, AF, JC, GB, JN, DPM, and MT). The team had expertise in conducting literature reviews and was all involved in the review process. We report our methods and findings in accordance with the recommendations for the conduct, reporting, editing, and publication of scholarly work in medical journals. 9 The protocol was not registered. The research question was developed using standard population, intervention, comparator and outcome (PICO) described to enhance research and review questions, with clear inclusion and exclusion criteria (Table 1) . 10
Review Question: How do PD training methods and educational interventions impact on PD outcomes in adult patients?
Review Aims:
Identify educational and training interventions that demonstrate improvement in PD-related outcomes for patients on PD. What is the evidence for retraining on improving PD-related outcomes? What PD patient outcomes are reported for PD training? What gaps in knowledge remain for future research?
Exclusion criteria
Paediatric studies Educational interventions that did not relate to patient training or relevant outcomes as above.
Search strategy
A systematic search for relevant articles was performed by two independent researchers in 2023. To obtain greater coverage of possible articles, the search was executed in multiple databases. The databases searched were PubMed, Web of Science, Scopus, CINAHL, Medline, and BDENF. Based on relevant studies in this field, this combination should cover more than 90% of all relevant references.11,12 A range of medical subject headings and subheadings, key terms, and key words were identified covering the individual elements of PICO. These were translated into the appropriate terminology covering the intervention and a range of potential outcomes and adapted for each search interface and database. The range of year of publication was between 2013 and 2023. Supplement 1 has a full list of terms and strategies
Selecting studies
All studies were uploaded to Endnote and then to Rayyan systematic review software to support the screening process of the whole team. Duplicate records in the search results were removed using Rayyan. Two stages of selection occurred. First, the title and abstract were independently screened for eligibility by all seven members; any conflict was resolved with further discussion to ensure that the selected articles met all the inclusion criteria. The second stage involved a full-text review; selected members of the group were paired to agree to the total list of included articles and those to be excluded. Publications in English, Portuguese, and Spanish were included as two reviewers were proficient in translation and able to do so (Figure 1).
Quality assessment
All included studies were then reviewed for quality assessment as there were a variety of methods reported, and tools were selected from the Joanna Briggs Institute.
13
Two researchers independently conducted quality appraisal using a designed qualitative extraction tool, and 26 studies were excluded at this stage. While this number is large at the quality appraisal stage, studies lacked detail, were not specific about patient training and poor quality. It provided a further robust procedure
Data extraction
A process of data extraction of all included studies was conducted with author, country, methods, intervention, and outcomes incorporated (Supplement 2).
Results
A total of 21 studies were included in the full narrative review. By countries Australia (n = 1), Brazil (n = 1), China (n = 1), Denmark (n = 1), France (n = 1), Italy (n = 1), Israel (n = 1), Korea (n = 1), Spain (n = 3), Sudan (n = 1), Turkey (n = 1), USA (n = 3), Uruguay (n = 2), and international multicenter (n = 3).
The methods’ descriptors varied: five observational retrospective studies, four cross-sectional surveys, three RCTs, three observational prospective studies, two cohort studies, two qualitative studies, one mixed method, and one quality improvement study. The full table of included studies is in Supplement 2.
Study populations
All studies included details of the population of incident and prevalent PD patients as the learner in training, with demographic details included. Some studies included carers or third-party trainers and some included nurses as the learner. Studies varied in size, as to be expected, with mixed study design being included. Two published studies were from the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS), and both were conducted differently, Perl et al. 2 included prevalent and incident patients, and the primary outcome was peritonitis rates, whereas the Cheetham et al. study only included incident patients (on PD < 3 months) with primary outcome as time to first peritonitis. 17
Study outcomes
In the included studies where training methods, educational interventions or characteristics were used, the primary outcome used was peritonitis and/or exit-site infection rates, with some including time to first infection or infection-free time.15–23 Other outcomes that can be included as all-cause technique survival were not necessarily reported; the PDOPPS studies, while collecting multiple data sources at the patient and center level, focused on the primary outcome for training on infection risk.2,17 Only two studies included hospitalization as an outcome,14,24 with only one including quality of life (QOL). 14
Analysis
Due to the small number of RCTs and the mixed methods used, a meta-analysis was not possible. This analysis, therefore, is a narrative review of the evidence in line with the review question and aims.
Main findings
This narrative literature review aimed to identify educational interventions that demonstrate improvement in PD patient outcomes. Studies evaluating these components will be discussed separately to acknowledge the difference between education and training for the purposes of the analysis. The results are therefore presented as:
Training methods Educational interventions Patient characteristics and assessments Retraining Outcome reported in studies.
Population, intervention, comparator, and outcome (PICO) question table representing the inclusion criteria.
Training methods
Training duration
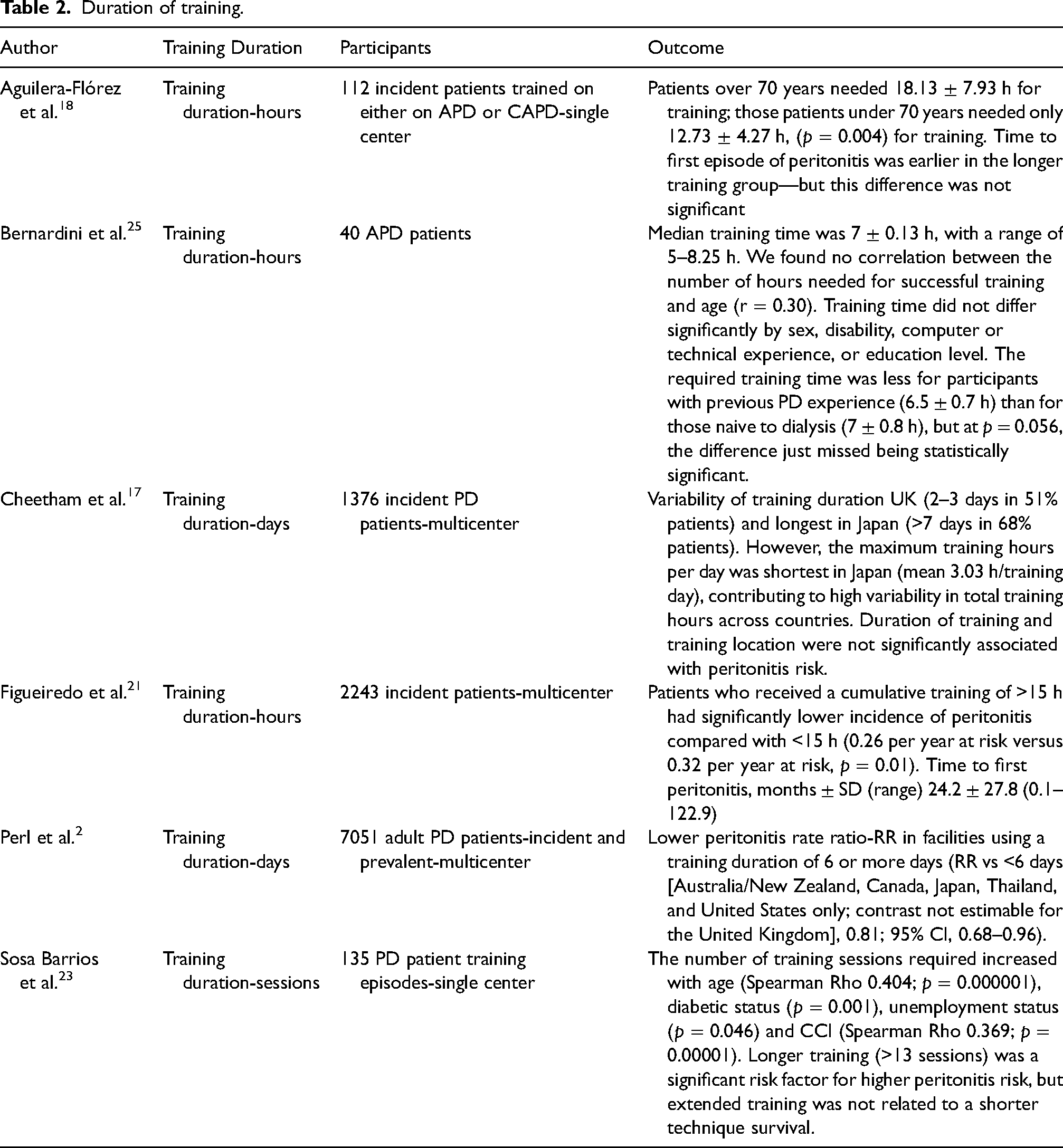
Training times are referenced in several studies to try and elicit if and how they impact on PD-related outcomes (a summary is provided in Table 2). The most significant large-scale studies to examine the relationship of training time to peritonitis include two large prospective cohort studies. A study from Brazil, which included 2243 incidence patients, examined training characteristics associated with peritonitis; cumulative training of >15 h had a significantly lower incidence of peritonitis compared with <15 h (0.26 per year at risk vs. 0.32 per year at risk, p = 0.01). 21 The analysis of PDOPPS by Cheetham et al., of 1346 newly started patients on PD across 120 facilities, unlike the Brazilian study, found training duration and timing were not significantly associated with peritonitis risk. 17 The authors of this large study highlighted the strengths compared to the Brazilian study as being able to adjust for a larger number of patient, facility and training characteristics. 17 Similarly to the Brazilian study, the PDOPPS study first publication by Perl et al. of incident and prevalent (7051) patients across 209 facilities, did find a correlation with training time with facilities reporting an initial period of patient training that was 6 days or longer had lower risk for peritonitis as compared with facilities that had an initial period of 6 or fewer days. 2 Consideration of many confounding factors has led to recommending individualized approaches as the length of training time may be influenced by patient characteristics such as health literacy or disability challenges. Smaller studies have attempted to address this with differing results. One study of 40 participants with a range of disabilities with mean age of 53.8 ± 11 years showed median training time as 7 ± 0.13 h. This study focused on 1-day specific automated peritoneal dialysis (APD) training using a cycler with audio, visual, and animation, there was no follow up. Training time did not differ significantly by sex, disability, computer or technical experience, or education level. 25 Whereas a retrospective study from Spain of 135 patients reported days rather than hours, with patients requiring a median of 10 (IQR 8–13) sessions to acquire enough skills to perform the PD technique with a median of 19 days (IQR 14–28). 23 Thirty-one patients (23%) needed more than 13 sessions and were considered to have a prolonged training time. Prolonged training time patients were older and had more comorbidities, with a significantly higher predictive risk of developing peritonitis demonstrated by the higher rates of peritonitis in this group, although there was no difference in time to first peritonitis episode in each group. 23 Similarly, a further cross-sectional observational study of 112 patients trained in APD and continuous ambulatory peritoneal dialysis (CAPD) examined the learning time and risk of first peritonitis in older and younger patients. 18 On average older patients (>70 years) required more training time (an average 4 h more) and developed first episode of peritonitis earlier than the younger cohort. 18
Duration of training.
Training location
Other than training time, the place of training has been examined, for example, either a hospital setting or a patient's home, often dependent on country and unit variations as demonstrated in PDOPPs. 17 There was no strong evidence of PD modality or location on peritonitis risk. 17 One retrospective study from Italy reviewed CAPD and APD home training (n = 17) versus video training (n = 21) with only small numbers of patients. 26 The video training was used for both CAPD and APD and replaced a home visit. The outcomes including time for training, number of home visits, and number of procedures to complete training and clinical outcomes. The video training group needed fewer home visits, and the home training group had more episodes of peritonitis and higher dropout; no episodes of peritonitis were reported in the video training group. 26
Person training
The association of who does the training on outcomes was not reported in detail across many studies. Often terms such as “experienced PD nurse” were highlighted; the PDOPP's study described a reduction of peritonitis risk when third-party trainers delivered the training, but this was only in the UK with small numbers. Within this study, when carers were trained, there was also a lower risk of peritonitis. 17 Patient-to-nurse ratio and individual versus group training found no correlation to peritonitis risk. 17
Educational interventions
Educational interventions were predominantly aimed at patients and carers, with some studies including nurses as the learners. Table 3 outlines the educational interventions and outcomes across the studies.
Educational interventions.
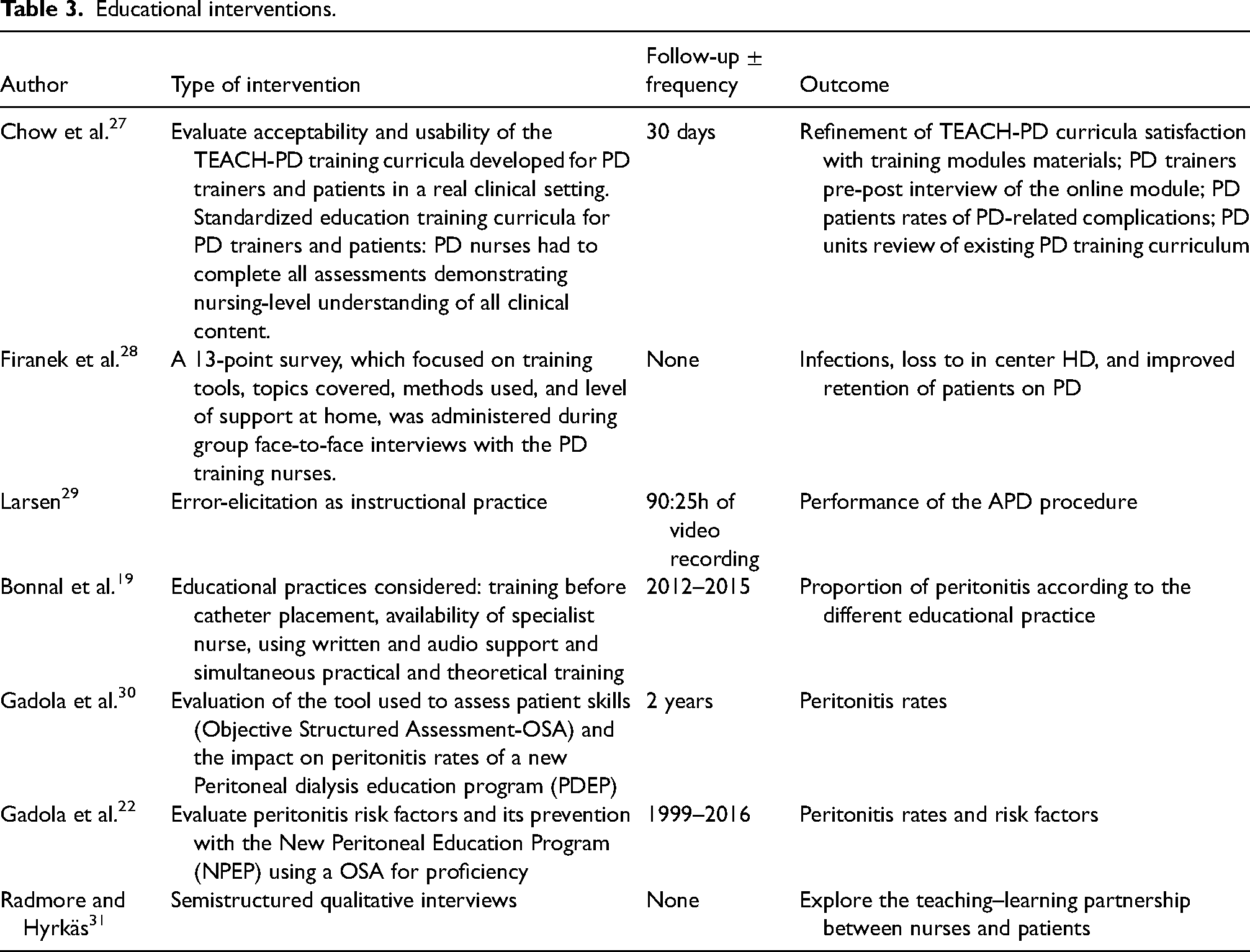
Various methods, interventions, and outcomes were used, including a pilot project, TEACH-PD, focused on a curriculum for patients and nurses; the results of the larger study are yet to be published. 32 The survey by Firanek et al. of training practices that likely contribute to successful training outcomes in APD focused on six centers in the USA of successful PD programs with excellent clinical outcomes. 28 The clinics provided ongoing education, reinforcement, and retraining of concepts and skills through discussion, quizzes, and topic-specific monthly training sessions. 28 Although retrospective, the study from the French Registry by Bonnal et al. analyzed 1035 patients. 19 The authors conducted multiple covariate analyses to elucidate the impact of different educational approaches on the impact of developing peritonitis. The use of written support during PD learning and starting PD learning with hands-on training alone was associated with a lower survival free time of peritonitis, whereas the use of audio support and starting PD learning with hands-on training in combination with theory were associated with a lower risk of presenting further episodes of peritonitis after a first episode. 19 It is important to note only 4% of centers used audio support.
Two studies from Uruguay evaluated a multidisciplinary educational training program. The results indicated a reduction in peritonitis episodes and time to first infection following the introduction of a new training program.22,30
Patient characteristics and assessments
Many studies included in this review examined specific patient characteristics to assess the risk of developing peritonitis. The French registry study used multivariate analysis to evaluate these characteristics and risks. One group with higher risk was individuals with a learning disability (HR 1.43, 95% CI 1.05–1.95). Conversely, another group with a hearing impairment had a lower risk of developing peritonitis (HR 0.35, 95% CI 0.16–0.75). 19 The study reported from Uruguay did not find any differences in patient characteristics associated with peritonitis risk. 22 The PDOPPS data also did not identify any significant risk factors for peritonitis, except for instances where a carer or third-party person (usually a nurse in a different location) conducted the training. 17 In contrast, a large study from Brazil found lower educational levels and literacy to be independently associated with peritonitis incidence. 21
Studies have retrospectively assessed knowledge of patients undergoing training to explore correlations to peritonitis risk. A small survey study from Sudan assessed knowledge and literacy in 50 prevalent patients (young cohort mean age 42 years). Compared with patients in the middle and lower quartiles, patients in the upper quartile of knowledge score had lower rates of peritonitis, exit-site infection, and hospitalization. 24
Retraining
One important question to understand is how retraining or programs focused on retraining improve education or PD-related outcomes. Six of the included studies focused on retraining efforts and are all characterized in supplement 3, with only three being prospective RCTs.14–16,20,33,34 No two studies were the same in design, and the heterogeneity makes comparisons difficult. The intervention of retraining was different; for example, in one study, the focus was on reassessments and then deciding if retraining was required, 15 whereas in other studies, delivering enhanced programs of care/retraining was the intervention.14,20,34 All the interventions differed in content from just additional home visits 14 to observed practices, 20 , theory and practical, 15 theory test only, 34 comparison of practical versus oral education 16 to a self-efficacy training program. 33 In all the studies, routine training at the start of PD treatment was delivered but different on start and follow up of retraining programs. Large dropout rates were noted with many cited factors including transplantation, transfer to HD and patients’ reluctance to attend frequent retraining.15,16
Discussion
This comprehensive review provides an update on the evidence for training methods, educational interventions, and retraining in patients receiving PD. Like previous reviews, there is still inconsistency and variable results, the largest studies being observational and the lack of RCTs. The ISPD guidelines for both peritonitis and training highlight specific areas related to PD training to improve outcomes, such as peritonitis and exit-site infections.3,4 Both acknowledge the lack of strong evidence to support many recommendations.
The training methods within this review and, more specifically, the time needed to train patients and caregivers adequately remain unclear, with differing results across the large observational studies.2,17,21 However, there is some consistency in training times being adapted according to the different needs of the population, with older patients requiring longer periods18,23 and people with low health literacy being at higher risk of peritonitis.19,21 This emphasizes the need to assess patients before training to understand their differing needs and thus adopt different approaches to training. This was recommended in the ISPD training curriculum with specific emphasis on adult learning styles. 3
There is a lack of evidence of appropriate methods to assess health literacy in PD studies or self-management programs.6,35 No studies in this review provided strong evidence for self-efficacy programs with only one small study on hand hygiene practices. 33 For patients and carers undertaking PD, success is not solely based on technical skills but also on the ability to make decisions, manage risks, and adjust to the burden of the treatment. Peritonitis stigma and underreporting has been highlighted in previous studies, recommending supportive approaches into education about peritonitis. 36
Starting training before catheter insertion or planned training seems to be relevant but not always clear in studies; the PDOPP's data reported the majority of the training was carried out after catheter insertion, 2 whereas the French data training commenced one month prior to catheter insertion. 19 Education before the commencement of PD has been reported in a larger study by Hsu et al., showing an improvement in peritonitis outcome, 37 similar to the Brazilian cohort. 21 Providing support and assessments has also been described as beneficial before the commencement of PD training. 38 This would align with opportunities to assess patients beforehand, as described earlier and recommended in previous guidelines. 3
Other training methods included in this narrative review were video training. 26 This is not a new concept, as many centers during COVID had to look at more remote ways to provide training. The advancement of virtual reality-assisted training is now of interest and may provide alternative approaches to PD training. 39
The only RCTs included in this review were those that examined retraining, the ISPD peritonitis guidelines recommends retraining as part of any PD program. 4 The design of the studies varied hence inconsistent results. In the context of PD programs, many factors should be considered, which are often not described in full within studies. For example, in routine care, how is support at home provided, that is, routine home visits, telephone support, or follow-up/access to teams if peritonitis or other problems occur? Many programs likely deliver retraining in a more informal capacity or when a problem has occurred rather than in a preventive way.
The training and expertise of nurses delivering training are often referenced as important. Even from this review some of the smaller qualitative studies referenced how skilled nurses adapt different methods and develop relationships which can all help and support patients in training.29,31 The standardization and competencies required by nurses undertaking PD training are not well understood; often, references to experience are described with conflicting results. 21 The TEACH-PD study may offer some insights into what should be included in a curriculum for nurses. One study in this review did describe nurses following principles of adult learning but details were lacking on what this entailed. 22
Outcomes reported in the included studies were mainly infection-related. The overall improvement in peritonitis rates has been studied over 30 years with multiple factors contributing. 40 Before 2000, advancements in technology and technique likely contributed to improvements. In more recent years, these improvements are less obvious but may be attributed to better adherence to guidelines for peritonitis prevention and increased standardization. 40 In addition, factors that are specific to the training and education of patients and families/carers are less obvious but may be contributing, although this review lacks consistency. Furthermore, there was a lack of patient-reported outcomes within the included studies. The Standardized Outcomes in Nephrology PD (SONG-PD) initiative reported inconsistencies in infection outcomes and emphasized that standardized outcomes for PD trials are required to improve efficiency and relevance. 41 While infection and technique survival were the most important core outcomes, life participation was also included. 42 The SONG-PD further identifies outcomes relevant to patient and caregiver burden, emphasizing developing strategies to adapt and build resilience to prevent or minimize burnout. 43 Future studies for training and education interventions should standardize reporting of infections and include other reported outcomes such as those described by SONG-PD.
Strengths and limitations
The strengths of this narrative review were the search strategy which followed a systematic and robust methodology. A team approach reduced bias of included studies. The limitations of this review need to be acknowledged. The review protocol was not registered as is, therefore, a limitation. As the lack of high certainty evidence, a systematic review methodology process could not be truly applied which usually only include RCTs and follow strict adherence to quality appraisal, risk of bias and statistical meta-analysis. A decision was made to include all study designs and produce an integrated narrative review to allow for a broader review to examine the evidence base following an initial scoping exercise where few RCTs were identified. A further limitation is the number of articles excluded at the quality appraisal stage, but the authors acknowledge they should have been excluded at the screening stage; however, the quality appraisal process provided additional robustness to ensure all eligibility criteria were followed.
Implication for practice and research
This review will underpin future guidelines for training and education of peritoneal dialysis patients and caregivers. The need for robust research to establish evidence to guide best practice on training methods and educational interventions. Consideration of assessments prior to training to individualize training programs and methods. The use of novel techniques, technology, videos, and virtual training needs expanding.
Conclusion
In conclusion this updated review highlights inconsistencies in approaches to training and education; however, some encouraging recommendations of adapted methods in training with individualized approaches, appropriate assessments before training, and the need for consistent outcomes across future studies including QOL and life participation.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608251328517 - Supplemental material for Peritoneal dialysis training and interventions: A narrative review
Supplemental material, sj-docx-1-ptd-10.1177_08968608251328517 for Peritoneal dialysis training and interventions: A narrative review by Helen Hurst, Ana Elizabeth Figueiredo, Diana Perez Moran, Gillian Brunier, Joanna Lee Neumann, Miguel Angel Trejo-Villeda and JSF Chow in Peritoneal Dialysis International
Supplemental Material
sj-docx-2-ptd-10.1177_08968608251328517 - Supplemental material for Peritoneal dialysis training and interventions: A narrative review
Supplemental material, sj-docx-2-ptd-10.1177_08968608251328517 for Peritoneal dialysis training and interventions: A narrative review by Helen Hurst, Ana Elizabeth Figueiredo, Diana Perez Moran, Gillian Brunier, Joanna Lee Neumann, Miguel Angel Trejo-Villeda and JSF Chow in Peritoneal Dialysis International
Supplemental Material
sj-docx-3-ptd-10.1177_08968608251328517 - Supplemental material for Peritoneal dialysis training and interventions: A narrative review
Supplemental material, sj-docx-3-ptd-10.1177_08968608251328517 for Peritoneal dialysis training and interventions: A narrative review by Helen Hurst, Ana Elizabeth Figueiredo, Diana Perez Moran, Gillian Brunier, Joanna Lee Neumann, Miguel Angel Trejo-Villeda and JSF Chow in Peritoneal Dialysis International
Footnotes
Acknowledgements
N/A
Author contributions
All authors contributed to the design, development and review of this systematic review. All authors endorsed the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This is a narrative review and Ethical clearance is not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
N/A
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.