
Abstract
Domestic animals are common in Australian households; however, there is little research into the potential risks these animals pose to patients undergoing in-home peritoneal dialysis (PD). Cats and dogs are known to carry many potential pathogens, including Pasteurella multocida. We reviewed the ANZDATA Peritoneal Dialysis Peritonitis Registry for cases of peritonitis due to Pasteurella multocida between 2011 and 2023. Cases identified were younger and more likely to be female compared with the Australian PD population who developed peritonitis due to other organisms. Of the total 32 episodes, 75% were using automated PD with glucose-based solutions. Two cases requiring removal of the PD catheter and transfer to haemodialysis and no deaths were reported. Whilst outcomes were largely favourable, it is likely that many of these cases could have been prevented. Education for people undergoing PD should include information about the potential infectious hazards of domestic animals.
Background
Peritonitis remains a significant complication of peritoneal dialysis (PD), associated with decreased ultrafiltration capacity and is the most common reason for change to haemodialysis (HD). 1 PD as an alternative to HD gives greater freedom and convenience, with reduced impact on quality of life. 2 However, it is associated with greater risk of peritonitis. Catheter insertion through the peritoneum provides a direct passage for infections, particularly with regular catheter and equipment manipulation required.
Pasteurella multocida (P. multocida) is a gram-negative coccobacillus, which represents a rare but serious cause of PD peritonitis. It is primarily transmitted to humans by domestic animals, especially cats. In Australia, 60% of households have at least one domestic animal, with 40% having a dog and 27% having a cat. 3 Up to 40% of dogs and 60% of cats sleep on their owner's beds. This occurs more in smaller, 1–2 person households. 3
There is little documented evidence about the potential infectious hazards of these animals in the home PD setting, despite their prevalence and proximity to the PD environment. The International Society for Peritoneal Dialysis guidelines 4 (ISPD guidelines) recommend that animals should be excluded from the space where PD is being performed, due to the associated zoonotic risks.5,6
This study aims to investigate the reported cases of PD peritonitis related to P. multocida in Australia between 2011 and 2023 and analyse the characteristics of this group compared to PD peritonitis related to other infectious causes within the same time period.
Methods
We reviewed the Peritoneal Dialysis Peritonitis Registry at the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) for episodes of PD peritonitis due to P. multocida from 1 January 2011 (commencement of PD peritonitis registry) until 1 January 2023 (most recent data available). ANZDATA is a clinical quality registry that includes all people in Australia and New Zealand who are treated with PD, HD or received a kidney transplant, using opt-out consent. All data on peritonitis is submitted by the treating Australian units (New Zealand has a separate peritonitis registry). A control population of all other peritonitis episodes in Australians during the study period reported to ANZDATA was used. 7
The primary outcome was complete cure, defined as complete resolution of peritonitis and no relapse or recurrent episodes, catheter removal and transfer to HD for 30 days, or death within 30 days of P. multocida peritonitis diagnosis. Secondary outcomes were hospitalisation, PD catheter removal and transfer to HD, and death. Relapsing peritonitis was defined as a peritonitis episode that occurred within 4 weeks of completion of antibiotics with the same organism. Recurrent peritonitis was defined as a peritonitis episode that occurred within 4 weeks of completion of antibiotics but with a different organism.
Data is presented as mean (standard deviation) or median (interquartile range (IQR)). Statistical significance was set at p < 0.05 with t-test used for comparisons of continuous data and chi-square test or Fisher's exact test (where cell size was less than 5) for categorical comparisons. Predictors of P. multocida peritonitis were analysed by univariate and multivariable logistic regression. Covariates with a p-value <0.2 in univariate analysis were included in the multivariable logistic regression.
The study was approved by the Tasmanian Health and Medical Human Research Ethics Committee (Approval H0018330).
Results
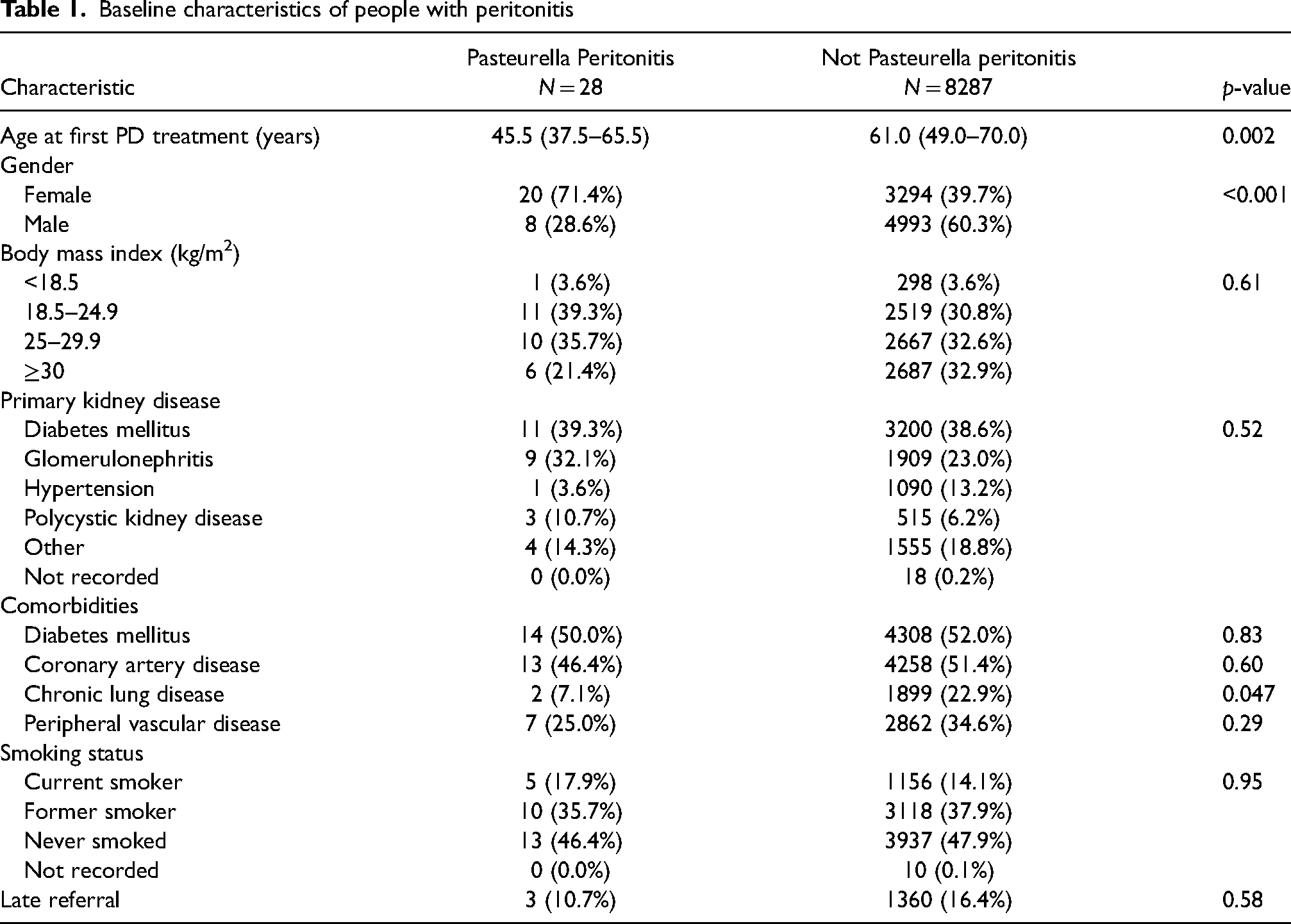
A total of 19,683 Australians were treated with PD during the study period. Of these, there were 32 episodes of PD-associated peritonitis due to P. multocida in 28 people and 17,027 episodes of PD-associated peritonitis in 8287 people due to other organisms. Compared with the control cohort, cases with P. multocida peritonitis were younger (median age 45.5 [IQR 35.0–66.5] years vs. 62.0 [IQR 50.0–71.0] years, p = 0.002) and more likely to be women (71.4% vs. 39.7%, p < 0.001; Table 1 and Supplementary Table 1).
Baseline characteristics of people with peritonitis
Clinical outcomes of PD-associated peritonitis
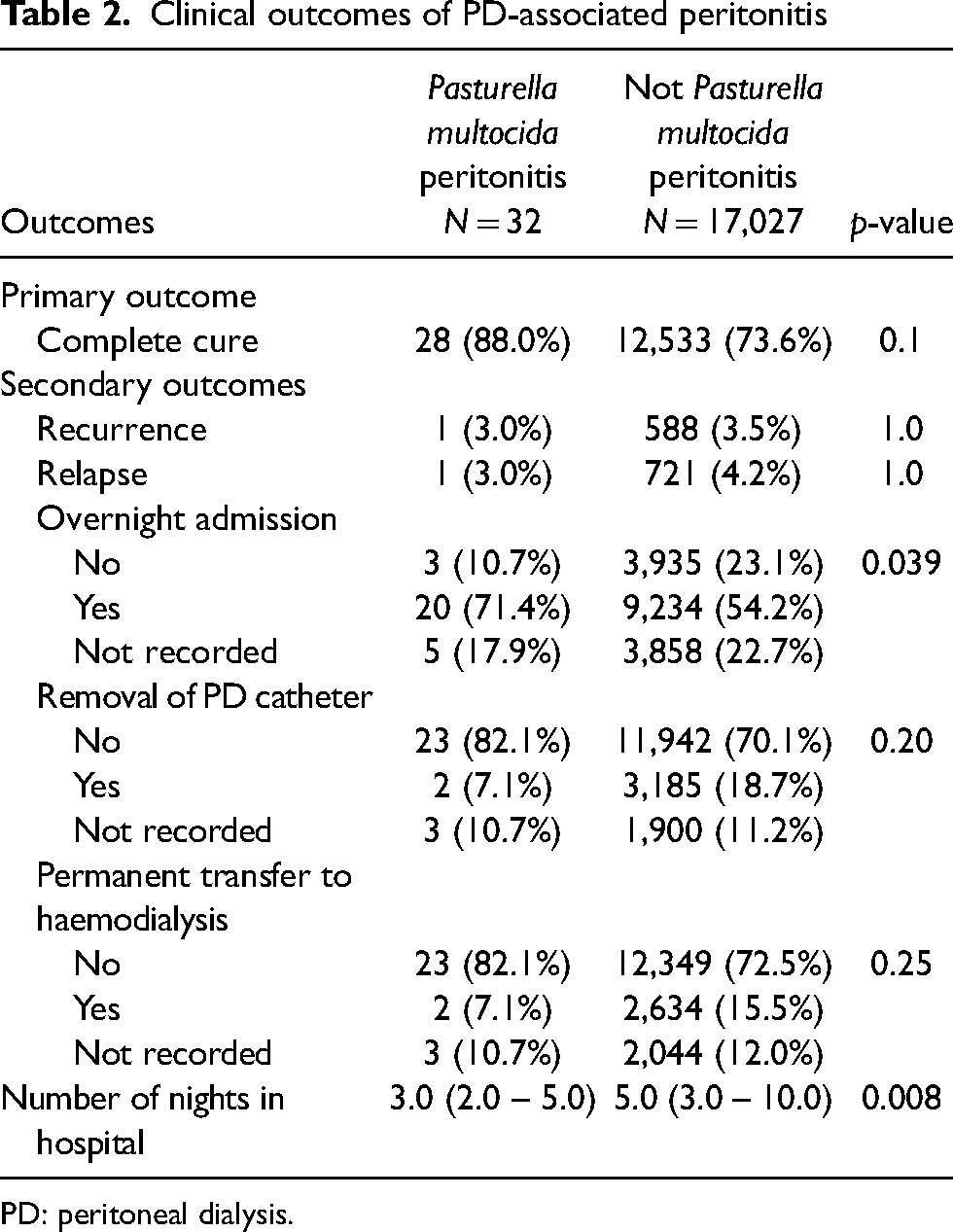
PD: peritoneal dialysis.
Antibiotic treatment of Pasturella multocida peritonitis
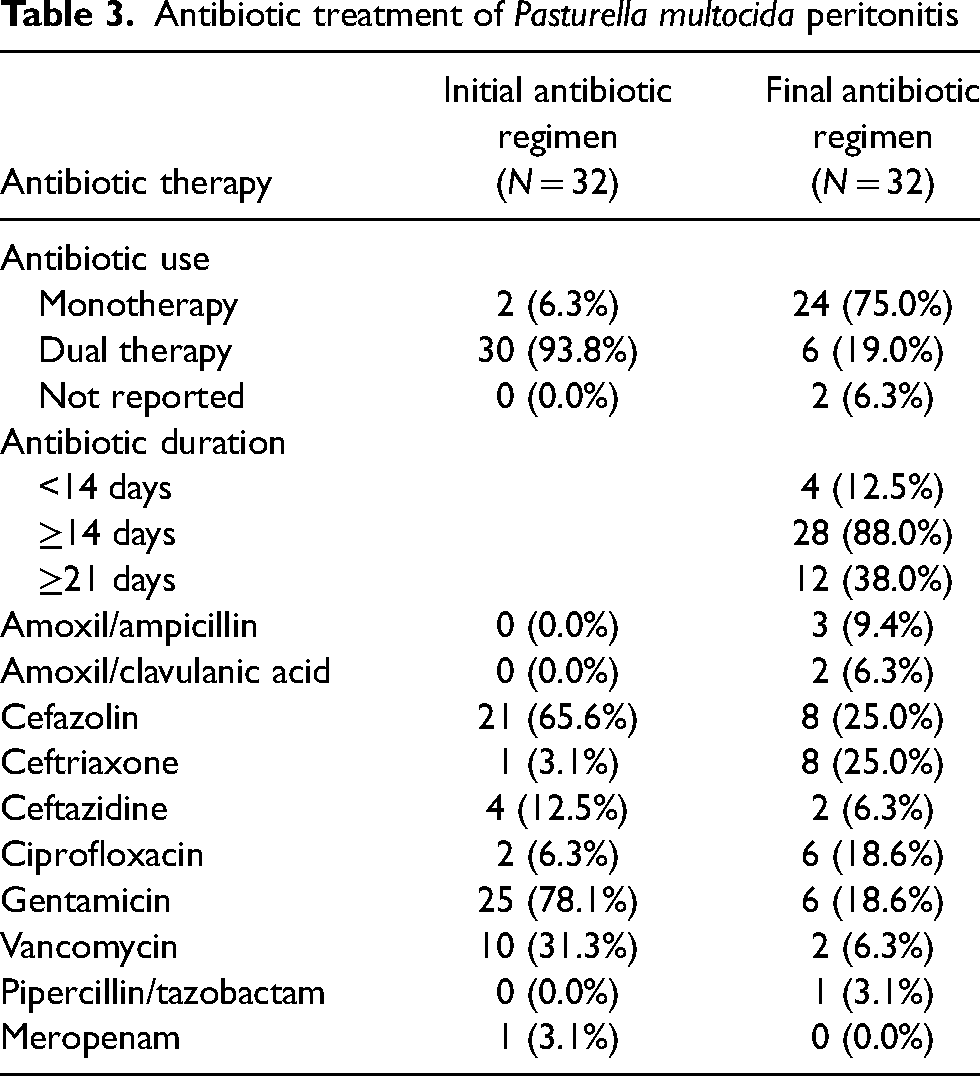
Initial treatment of P. multocida peritonitis consisted of dual antibiotics in 94% (n = 30/32) until culture results were available (Table 3). Final antibiotic regimen was monotherapy in 75% (n = 24/32) including cefazolin (25%), ceftriaxone (25%), ciprofloxacin (19%) or amoxycillin (16%). Treatment duration with antibiotics was for at least 14 days in 88% (n = 28/32) and at least 21 days in 38% (n = 12/32; Supplementary Table 2).
Outcomes were largely favourable with complete medical cure seen in 88% (n = 28/32) with 1 relapse and 3 cases requiring catheter removal and subsequent transfer to HD (Table 2). No deaths were reported within 30 days. Cases of P. multocida peritonitis were more likely to be admitted, with 71.4% required overnight hospital admission (p = 0.039), but for a shorter length of stay than the control population (median 3.0 [IQR 2–5] vs. 5.0 days [IQR 3–10], p = 0.008).
Multivariable analysis of risk factors for P. multocida peritonitis (Supplementary Table 1) confirmed that patients were more likely to be aged less than 50 (OR = 2.68, 95% CI = 1.03–6.94, p = 0.042) and female (OR = 3.38, 95% CI = 1.48–7.74, p = 0.004). The same analysis revealed that the type of PD used at time of peritonitis was not strongly associated with P. multocida peritonitis, when automated peritoneal dialysis (APD) was compared to continuous ambulatory peritoneal dialysis (CAPD; OR = 1.04, 95% CI = 0.78–1.37, p = 0.81).
Discussion
We present here 32 episodes of P. multocida PD peritonitis and their clinical outcomes. Even with this report, this is a rare cause of PD peritonitis with less than 100 cases reported in the published literature. 8
Outcomes were overall favourable, with no deaths within 30 days and complete cure in 88% of cases reported. Whilst patients with P. multocida peritonitis were more likely to be admitted, they spent less time in hospital than other causes of peritonitis. Patients treated with PD have been shown to have greater quality of life across multiple domains, including physical and social functioning, work status and burden of kidney disease, according to a meta-analysis analysing 21 studies. 9 This highlights the importance of reducing transfer to HD by preventing all causes of PD peritonitis, including P. multocida.
Antibiotic treatment was varied within our study group. 88% received antibiotic therapy for 14 days or more, with 38% received therapy for 21 days or more, demonstrating the severity of this infection. There remains no specific clinical trials that explore efficacy of various antibiotics for peritonitis related to P. multocida, which could represent a future area of exploration. Smaller case studies have recommended gentamicin, ampicillin and penicillin as first-line selections. 10 Compared to our cases, 78.1% of cases were treated empirically with gentamicin, 65.6% with cefazolin and 31.3% with vancomycin. Dual therapy with a combination of one oral/IV antibiotic and one intraperitoneal antibiotic is recommended for empirical therapy, 11 and dual therapy was reported in 93.8% of our P. multocida group.
Whilst demographics were mostly similar between the P. multocida peritonitis cohort and control cohort, the P. multocida peritonitis cohort were younger (median age of 45.5 [IQR 35.0–66.5] years) and a higher proportion of females compared to the control group (71.4% vs. 39.7% female). Literature suggests that sex is not an independent risk factor for poorer outcomes of peritonitis infection. 12 Gadola et al. 13 found the risk factors for peritonitis included age and lack of education programmes and some studies have shown female sex to be associated with lower rates of failure of PD technique. 14
Initial univariate analysis of the data suggested the use of APD technique was significant higher in the P. multocida group compared to the general peritonitis group (78.6% vs. 56.7%, p = 0.025; Supplementary Table 2). However, on multivariable logistical regression analysis revealed no significant difference between the groups (OR = 1.04, 95% CI = 0.78–1.37, p = 0.81; Supplementary Table 1). Use of APD is not associated with a higher risk of peritonitis compared to CAPD within literature, as incidence and mortality has been found to be equivalent between the two 15 and rates of hospitalisation lower with utilisation of APD. 16 An ANZDATA registry study found there was no increased risk of peritonitis between the modalities and comparable peritonitis outcomes. 17 Therefore, our findings were consistent with literature and greater utilisation of APD could not account for the younger age of our P. multocida group, despite the greater daytime flexibility and autonomy offered by APD. 18
Therefore, we considered other potential causes for the demographic data uncovered and analysed other reports of P. multocida peritonitis and their risk factors, raising the suggestion that pet ownership, in particular cats, could be a risk factor for this younger and predominantly female population group. Despite rare reporting, there have been reports of PD peritonitis due to P. multocida where households pets have been directly implicated, 10 with mechanisms of infection suggested including a cat playing with equipment or person touching cat before touching machine. Mu et al. 10 reported 28 cases of P. multocida PD peritonitis in 2020, highlighting appropriate antibiotic therapy for P. multocida infection and suggesting a potential for prevention through severance of infection route via the pet.
The ANZDATA Peritonitis Registry does not record data on possible exposure to pets and pet ownership, which could elucidate this potential link and could be considered in future data collection and research. A national survey found that 27% of people in Australia own a cat and that pet ownership was more common in younger age demographics, as high as 70% in 18- to 24-year-olds and 66% in 40- to 54-year-olds. 19 The same study reported pet ownership to be more common in females (at 64% compared to 42% in males), similarly, Mueller et al. 20 suggested that cat ownership is slightly more prevalent in females at 52.8% compared to 47.2% in males. This demographic is consistent with the population observed in our study group and highlights an important potential area for future prevention of infection. Consideration of this potential exposure risk provides an opportunity for harm prevention, as individuals can be warned of these risks and make changes to keep pets away from this equipment. These risks should be emphasised during patient education on use of the PD machinery and should highlight the multiple observed routes of infection where pets can contribute. This should include pets interacting with PD machine when not in use, pets compromising the dialysis tubing and touching the pet before using the PD machine causing contamination. 10 Advice could include keeping pets away from machinery even when not in use and careful hand hygiene prior to use.
This study is limited by a small sample size due to the rarity of P. multocida as a cause of PD peritonitis, which limits the strength of the study and capacity for multivariate analysis. The ANZDATA registry analysis did not encompass all peritonitis risk factors, including exposure to household pets. A focus on a single cause of pet-related peritonitis is likely to underestimate its impact, this is a limitation of our study and data set.
In conclusion, whilst the incidence of PD peritonitis due to P. multocida is low, there were at least 28 people affected in Australia over the 13-year period between 2011 and 2023. This condition could largely be prevented by ensuring domestic animals do not have access to the catheter or APD equipment, subsequently, this number could be lower and potentially zero. Despite largely favourable outcomes, most patients required a hospital admission and a prolonged course of antibiotics, demonstrating the severity of the infection. Peritonitis remains the leading cause of transition to HD in patients undergoing PD 21 as observed in two patients included in this study. As HD is associated with a reduced quality of life, 22 every attempt should be made to mitigate the risk of peritonitis in these patients, including education regarding the risk that household pets pose to the development of PD-associated peritonitis. Given the potentially significant risks, education about the possible hazards of domestic animals should be included in all training for home PD to prevent these harms.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608241292477 - Supplemental material for Peritoneal dialysis-related peritonitis due to Pasteurella multocida in Australia
Supplemental material, sj-docx-1-ptd-10.1177_08968608241292477 for Peritoneal dialysis-related peritonitis due to Pasteurella multocida in Australia by Isabelle Ingham, Erin Jose, James Burgess, Laura Cuthbertson and Matthew D. Jose in Peritoneal Dialysis International
Supplemental Material
sj-docx-2-ptd-10.1177_08968608241292477 - Supplemental material for Peritoneal dialysis-related peritonitis due to Pasteurella multocida in Australia
Supplemental material, sj-docx-2-ptd-10.1177_08968608241292477 for Peritoneal dialysis-related peritonitis due to Pasteurella multocida in Australia by Isabelle Ingham, Erin Jose, James Burgess, Laura Cuthbertson and Matthew D. Jose in Peritoneal Dialysis International
Footnotes
Acknowledgements
The data reported here have been supplied by the Australia and New Zealand Dialysis and Transplant Registry. The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the Australia and New Zealand Dialysis and Transplant Registry.
Author contributions
All authors have contributed significantly to the writing of and agree with the content of the manuscript. Author contributions in keeping with the latest guidelines of the International Committee of Medical Journal Editors are as follows:
Isabelle Ingham: Design, acquisition and interpretation of the work, revised the manuscript critically for important intellectual content. Erin Jose: Design, acquisition and interpretation of the work, drafted the manuscript. James Burgess: Design, acquisition and interpretation of the work, revised the manuscript critically for important intellectual content. Laura Cuthbertson: Design, acquisition and interpretation of the work, revised the manuscript critically for important intellectual content. Matthew D Jose: Conception, design, acquisition, analysis and interpretation of the work, revised the manuscript critically for important intellectual content.
All authors have reviewed and approved the final manuscript for submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Specific informed consent including voluntary, written consent and approval to publish was obtained from the patient described above in the case report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.