
Abstract
Background
Although both hemodialysis and continuous ambulatory peritoneal dialysis (CAPD) are covered by national healthcare insurance, 98% of kidney failure disease patients are treated with hemodialysis. This study compared the health-related quality of life (HRQoL) and utility scores of patients receiving hemodialysis and CAPD in Indonesia and determined factors associated with HRQoL and utility scores.
Methods
A cross-sectional study was performed using the Kidney Disease Quality of Life-36 and EQ-5D-5L instruments at six hospitals. Utility scores were presented as SF-6D and EQ-5D scores. Factors associated with the EQ-5D were evaluated using Tobit regressions due to ceiling effects, while the SF-6D and HRQoL were assessed using generalized linear models since the data were not normally distributed.
Results
Among the 613 patients, 76% were treated with hemodialysis. After adjusting for sociodemographic characteristics and clinical parameters, CAPD patients reported better HRQoL compared to hemodialysis patients in terms of the SF-6D (p = .038), mental component summary (p = .020), symptoms (p = .005), and effects of kidney disease (p<.001), but no significant differences were reported in EQ-5D (p = .083), physical component summary (p = .323), burden of kidney disease (p = .111), and kidney summary scores (p = .068). Poorer HRQoL and utility scores were likely experienced by older patients who were male, married, with diabetes, treated in Class A hospitals, and with lower education, hemoglobin, and albumin levels.
Conclusion
In Indonesia, patients treated with CAPD had better HRQoL and utility scores compared to patients undergoing hemodialysis. Therefore, CAPD should be promoted by healthcare professionals as the first treatment option for patients who are eligible for both hemodialysis and CAPD.
Background
Patients with kidney failure disease require a kidney replacement therapy, and it is forecasted that approximately 3.9–7.6 million will need a kidney replacement therapy by 2030. 1 Aside from increasing the length of survival, a kidney replacement therapy is also intended to improve the health-related quality of life (HRQoL) of a patient. 2 In light of HRQoL's crucial role as a predictor of a patient's overall outcomes as confirmed by several studies,3,4 it is important to incorporate HRQoL as an important supplement to clinical outcomes. To improve and optimize the overall treatment for chronic kidney disease, HRQoL assessments can be performed in tandem with symptom monitoring. 5 A focus on the improvement of HRQoL has been associated with improved treatment adherence, enhanced emotional and cognitive functioning, better certain laboratory parameters, reduced hospitalization frequencies, and decreased mortality rates. 6
Hemodialysis and peritoneal dialysis are the most common kidney replacement therapies, 7 although the question of which of the two results in better overall outcomes is inconsistent across scientific literature. Some studies reported that the HRQoL of patients undergoing peritoneal dialysis is better compared to the HRQoL of those undergoing hemodialysis,8,9 while others reported a nonsignificant difference,6,10,11 or even lower HRQoL in patients on peritoneal dialysis than in those on hemodialysis. 12 One past systematic review assessed studies focusing on the HRQoL of patients treated with hemodialysis compared to the HRQoL of those undergoing peritoneal dialysis, but a decisive conclusion and final recommendations could not be reached. 13 Another systematic review indicated no significant difference in HRQoL between patients treated with the two dialysis modalities, 14 while a meta-analysis found that kidney failure patients treated with peritoneal dialysis have better HRQoL in some domains compared to hemodialysis patients. 7 Therefore, additional studies to examine the overall outcomes on HRQoL of patients when treated with hemodialysis compared to the overall outcomes of patients when treated with peritoneal dialysis is absolutely necessary.
In Indonesia, national healthcare insurance covers both hemodialysis and continuous ambulatory peritoneal dialysis (CAPD). A previous societally focused cost-utility analysis study found that administering CAPD in the first instance is more cost-effective than administering hemodialysis for the Indonesian population. 15 Furthermore, CAPD is considered more suitable for Indonesia due to the limited number of hemodialysis facilities available 16 and an uneven distribution of such facilities throughout the country. Nonetheless, the most recent report from the Indonesian Renal Registry indicated that hemodialysis patients still significantly outnumbered CAPD patients. 16 Despite the number of CAPD patients almost doubling from 1376 to 2478 between the years 2013 and 2018, the percentage of the total population receiving kidney replacement therapy decreased from 5.9% to only 1.8%. 16 The introduction of CAPD in Indonesia is encountering various obstacles, such as limited availability of facilities, CAPD's less profitability to hospitals than the profitability offered by hemodialysis, unclear service fees and less incentives for healthcare professionals, physicians’ low motivation to promote CAPD, and inadequate knowledge of CAPD among the public. 17
A previous study compared the HRQoL of hemodialysis and CAPD patients in Indonesia and found no significant difference. However, that study used only a generic HRQoL instrument, compared only the descriptive system, and did not compute the utility score or HRQoL score. 18 The use of a generic instrument is an important concern because many studies report that kidney disease-specific instruments are necessary to properly capture HRQoL sensitivities when comparing different dialysis modalities.19,20 Moreover, there only exist a few studies that evaluated factors affecting the HRQoL of patients with kidney failure disease from South-East Asia, 20 and findings on the HRQoL of patients from Western countries may not be reflective of these patients. 21 Therefore, this study aimed to compare the HRQoL and utility scores of kidney failure disease patients receiving hemodialysis and CAPD, as well as to determine factors associated with HRQoL and utility scores in the Indonesian population.
Methods
A cross-sectional study design was used to measure the HRQoL and utility scores of patients with kidney failure disease undergoing hemodialysis or CAPD. The study was conducted at six hospitals (three Class A hospitals, and three Class B or C hospitals) that provided both hemodialysis and CAPD treatments across four cities in Indonesia. These hospitals were selected to represent both public and private hospitals as well as different hospital classifications. According to the medical services coverage, health facilities are categorized into primary and secondary health facilities. If necessary, patients from primary health facilities may be referred to secondary health facilities for further treatment. Secondary health facilities consist of Class A, B, and C hospitals, among which Class A hospitals are the top hospitals treating more complex cases, providing a wide range of subspecialist services, and equipped with the most advanced facilities. The study procedures, objectives, and ethics were explained to all potential participants. Each participant willing to join the study confirmed consent with a signed informed consent form. All participants were asked to complete a sociodemographic characteristic form and instruments measuring their HRQoL, each provided by a research assistant. Clinical parameters were obtained from participants’ medical records. The report of this study was prepared according to the STROBE guidelines. 22 A checklist of the items is provided in Supplemental Table S1.
Participants
Research assistants would approach patients either while they were receiving hemodialysis or while they were waiting for a nephrologist for a routine consultation at the CAPD unit of the hospital and take a sample of participants by a convenient sampling technique. All research assistants were trained before data collection on study protocols regarding data collection, how to approach potential participants, and data management. Patients were recruited if they were 18 years of age or older, had been diagnosed with kidney failure disease, and had been undergoing hemodialysis or CAPD for more than 3 months, but patients who refused participation in the study, suffered from mental disorders, or had a difficulty in communication, such as not being able to speak Indonesian or suffering from hearing impairment, would be excluded. The minimum sample size for each of the hemodialysis and CAPD groups was set to be at least 100 in order to enable detection of statistically significant differences in HRQoL and utility scores using an independent two-tailed t-test 23 with 80% power, α set at 0.05, and an expected effect size of 0.4.
Study instruments
Study instruments were used to determine participants’ sociodemographic characteristics, clinical parameters, and HRQoL. Dialysis modality was the independent variable, while HRQoL and utility scores were the dependent variables. Sociodemographic characteristics and clinical parameters were considered as covariates. Sociodemographic characteristics included age, gender, education level, marital status, employment status, and classification of the hospital at which patients were receiving treatment. Clinical parameters included whether the participant was diagnosed with diabetes, comorbidities, dialysis vintage, blood pressure, dialysis adequacy (measured in Kt/V), and albumin, hemoglobin, creatinine, and urea levels. HRQoL and utility scores were measured using the Kidney Disease Quality of Life 36 (KDQOL-36) and EuroQol Five-dimension (EQ-5D) instruments.
Health-related quality of life and utility scores
Several instruments exist to assess HRQoL in kidney failure disease patients, 24 including generic and kidney disease-specific instruments. The EQ-5D is a generic HRQoL measurement tool that generates a single utility score to calculate the quality-adjusted life years from a health economic field perspective, while the KDQOL-36 covers both generic and kidney disease-specific HRQoL measurements.
This study used the Five-level EQ-5D (EQ-5D-5L), consisting of the EQ-5D-5L descriptive system on the first page and a visual analog scale on the second page. 25 The descriptive system comprises five dimensions assessing mobility, self-care, usual activities, pain, and anxiety. Each dimension has five level options from “no problems” to “extreme problems.”
The KDQOL-36 contains 36 items. The first 12 items, referred to as the 12-item Short-form Survey (SF-12), measure the physical component summary (PCS) and mental component summary (MCS) domains, while the remaining 24 items were used to compute three kidney disease-specific domains comprising burden, symptoms, and effects of kidney disease. 26 The kidney summary score (KSS) was calculated by averaging the scores of burden, symptoms, and effects of kidney disease. Each of the PCS, MCS, KSS, burden, symptoms, and effects of kidney disease scores was to range from 0 to 100, and better quality of life was indicated by higher scores. 27 In terms of validity and reliability, psychometric measurements for the Indonesian version of KDQOL-36 were successfully evaluated in Indonesian hemodialysis and peritoneal dialysis patients. 28
The Short-form Six-dimension (SF-6D) and EQ-5D utility scores were determined from the SF-12 and EQ-5D-5L instruments, respectively. The SF-6D utility score was calculated using software developed by the University of Sheffield,29–31 which was approved for use in this study by the University of Sheffield Licensing Team with license number 240ANFM. In order to generate an SF-6D score, we implemented a scoring algorithm based on the US version of the SF-12 since item number 10 of the SF-12 in our study had six possible responses and item number 12 only had five. The EQ-5D utility score was determined according to the value set for the Indonesian population. 32 Both scores for SF-6D and EQ-5D utility were to range from 0 to 1.
Statistical analysis
The sociodemographic characteristics and clinical parameters of patients undergoing hemodialysis and CAPD were compiled and compared using descriptive statistics. Categorical variables were demonstrated as frequencies and percentages, while continuous variables were reported as means and standard deviations. Chi-square tests were used to compare categorical variables in hemodialysis patients and CAPD patients, while for continuous variables, an independent t-test and a Mann–Whitney test were used to compare variables with normal and nonnormal distributions, respectively. Next, the three summary scores (PCS, MCS, and KSS), the three kidney disease-specific domains (burden, symptoms, and effects of kidney disease), and the utility scores (SF-6D and EQ-5D utility scores) of the hemodialysis patient and CAPD patient groups were compared. Differences in HRQoL and utility scores were determined using the Mann-Whitney test, and effect sizes were estimated using Cohen's d. Cohen's d effect sizes were interpreted as small (0.2), medium (0.5), or large (0.8). 33
Based on previous systematic reviews and existing studies,13,19,34,35 we hypothesized that patients on CAPD would have better HRQoL and utility scores than would patients on hemodialysis, especially in the kidney disease-specific domains. In addition, we also hypothesized that patients who were female, older, married, with diabetes, treated in Class A hospitals, and with a longer dialysis vintage, lower education levels, lower levels of hemoglobin and albumin, and a higher Carlson Comorbidity Index value would have poorer HRQoL and utility scores.8,19,20,35,36
The Multiple Imputation by Chained Equations (MICE) algorithm was used to impute missing values before evaluating predictors associated with HRQoL and utility scores. Considering the plausibility of the method as documented by previous studies, 37 MICE became the preferred approach because it takes into account the uncertainty during imputations and can handle variables of different types, such as continuous and binary variables. Dialysis adequacy was excluded during the imputation process since it was not measured for CAPD patients; thus, this missing value was considered missing not at random. Urea levels were also excluded during the imputations since they were found in previous studies to have no relationship with HRQoL or utility scores. 36 In addition, creatinine levels, as well as urea levels, were likely affected by the time of measurements, whether the measurements were conducted before or after dialysis; thus, creatinine levels were also excluded during the imputations. Missing data or values for any other variables were considered missing at random, as MICE requires this assumption to minimize the bias. Imputations were set at 25 times, and visual inspection was used to investigate the density estimates and distribution between observed and imputed values.
Generalized linear models with a gamma distribution and log-link function were applied to evaluate predictors associated with HRQoL (PCS, MCS, KSS, and three kidney disease-specific domains) and utility scores. Multivariate linear regressions were not used since the HRQoL and utility scores were too skewed when evaluated by quantile-quantile plots (Q-Q plots) (Supplemental Figure S1). However, since all previous studies used multivariate linear regressions to evaluate predictors of HRQoL and utility scores in patients on dialysis,19,20,36 we also compared the results of the generalized linear models and multivariate linear regressions. In addition, Tobit regressions were used if HRQoL or utility scores as the dependent variables had ceiling effects. 38 All independent variables, including dialysis modality, sociodemographic characteristics, and clinical parameters, were included in subsequent regression models irrespective of whether the variables were statistically significant in the univariate analysis.
Data were analyzed using R software (version 4.2.1), where p-values below .05 were considered statistically significant. The direction of the association between a variable and HRQoL or utility scores was determined based on the regression coefficient of the variable. Effect size was computed using the effsize package, 39 while MICE method-derived imputations were processed using the MICE package. 40
Results
Participant characteristics
A total of 636 patients were approached by the research assistants, among whom 22 patients (3.5%) refused to participate and 1 patient (0.1%) was excluded due to hearing impairment (Figure 1). In total, data from 613 patients (response rate of 96.4%) were included for data analysis; of those patients, 466 (76%) received hemodialysis and 147 (24%) received CAPD (Table 1).
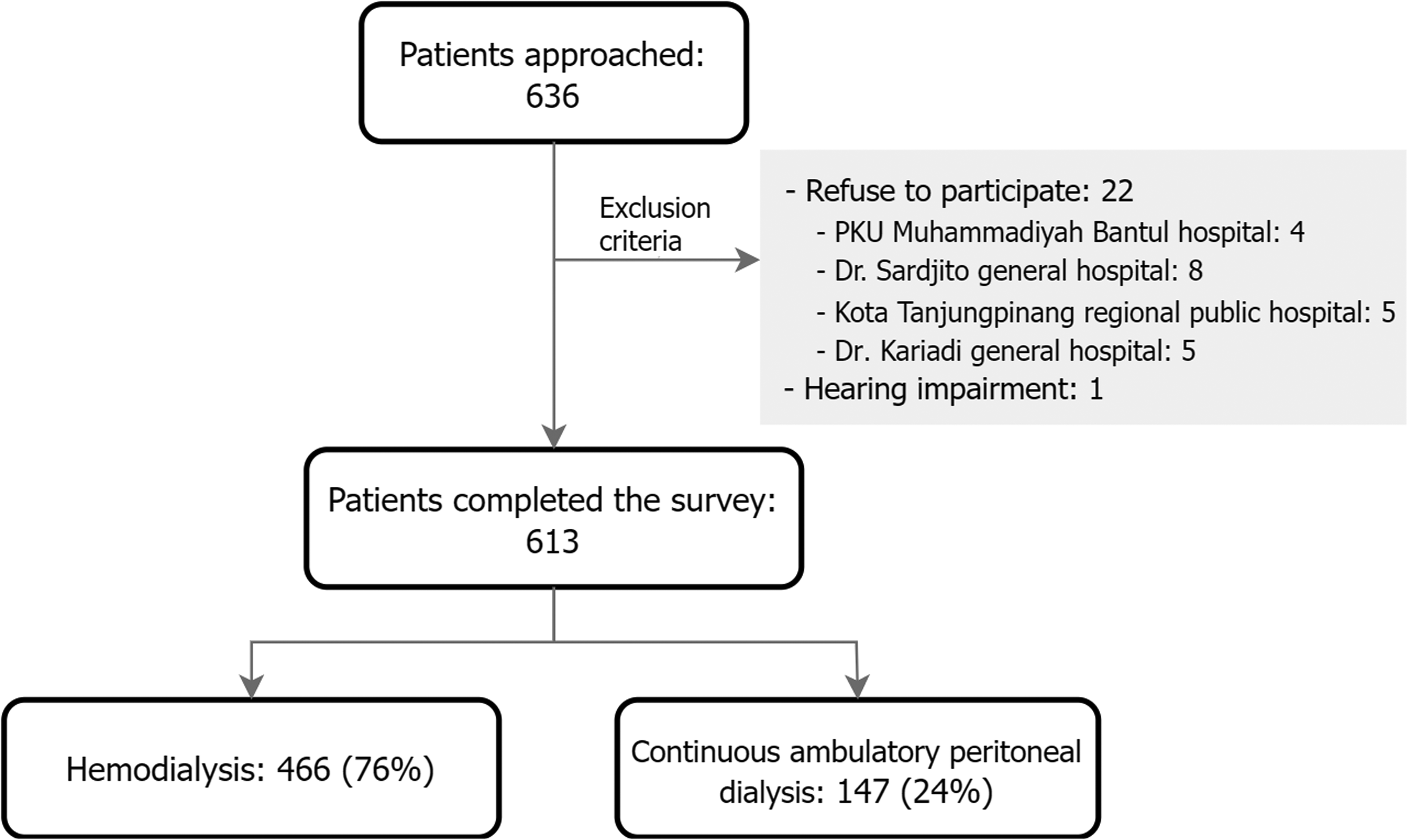
Recruitment process of participants.
Characteristics of hemodialysis and CAPD patients.
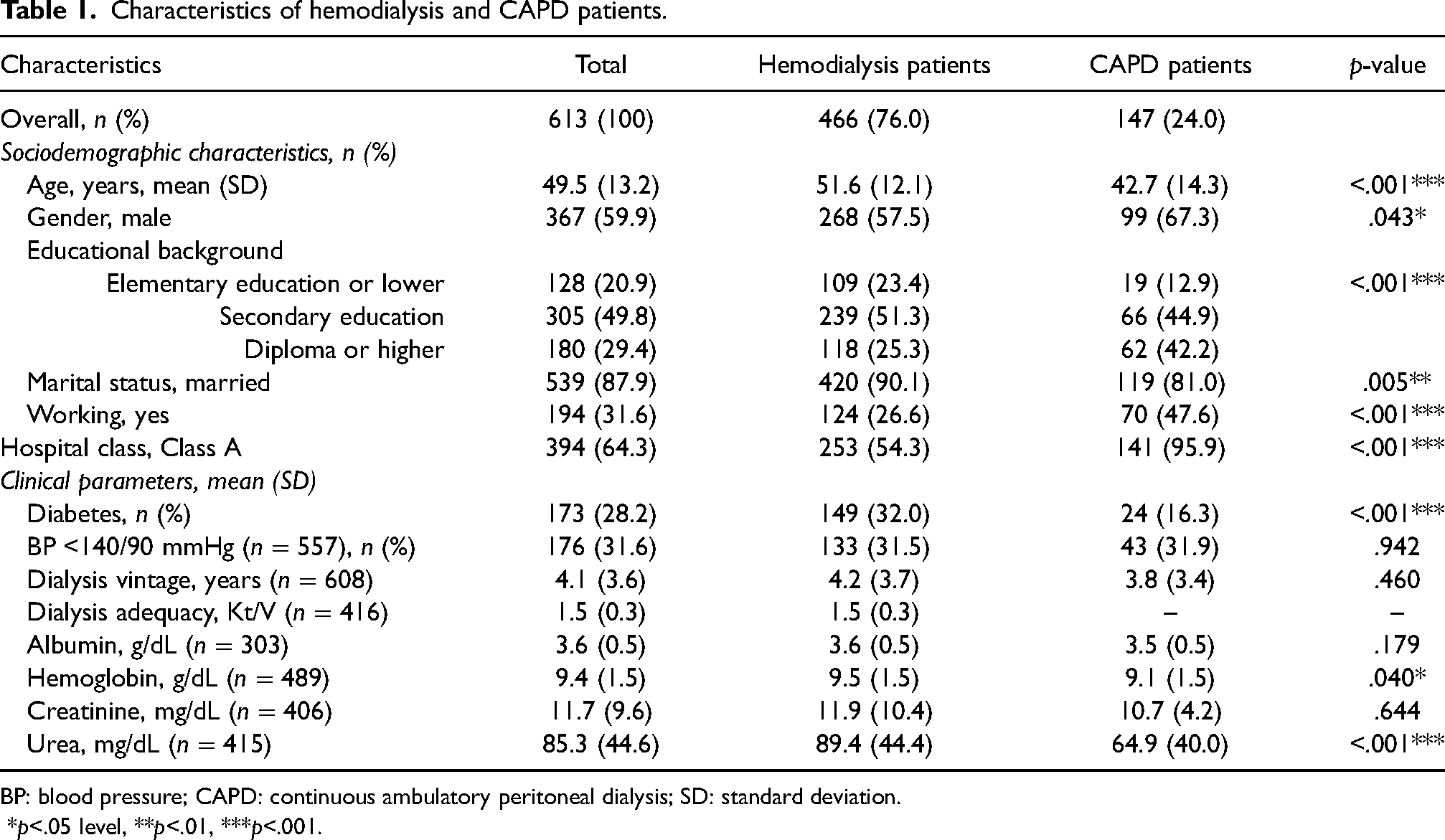
BP: blood pressure; CAPD: continuous ambulatory peritoneal dialysis; SD: standard deviation.
*p<.05 level, **p<.01, ***p<.001.
The average age of participants in the study was approximately 49.5 years (SD = 13.2), and the majority of them were male (59.9%), married (87.9%), unemployed (68.4%), with secondary school as their highest level of education attainment (49.8%), and receiving treatment in Class A hospitals (64.3%). Of patients receiving CAPD, the majority were male (67.3%), younger (average age 42.7 years), holding a higher level of education to that of at least a diploma (42.2%), single (19.0%), employed (47.6%), treated in Class A hospitals (95.9%), and with a lower percentage of diabetes (83.7%) than the percentage among patients on hemodialysis. All sociodemographic characteristic variables were statistically significant when hemodialysis and CAPD patient groups were compared. Meanwhile, for clinical parameters, only the number of participants with diabetes (p<.001), hemoglobin levels (p = .040), and urea levels (p<.001) had significant differences. Dialysis adequacy could not be determined for CAPD patients since the hospitals participating in the study measured dialysis adequacy only for patients treated with hemodialysis.
Based on clinical parameters, seven variables had missing data. Dialysis vintage (0.8%) and blood pressure (9.1%) had missing data of less than 10%, while hemoglobin levels, dialysis adequacy, urea levels, and creatinine levels had missing data of 20.2%, 32.1%, 32.3%, and 33.8%, respectively. Of all the variables with missing data, albumin had the highest missing data, with 50.6%.
HRQoL and utility scores
Table 2 presents a comparison of HRQoL and utility scores between hemodialysis and CAPD patients. In general, the HRQoL of CAPD patients was better than that of hemodialysis patients, with differences notably significant in PCS (p<.001) and effects of kidney disease (p = 0.004). Similarly, the utility scores of CAPD patients were statistically higher in the EQ-5D (p = 0.003) and SF-6D (p = 0.009). Mean HRQoL and utility scores by participants’ characteristics can be found in Supplemental Table S2.
Health-related quality of life and utility scores of hemodialysis and CAPD patients.
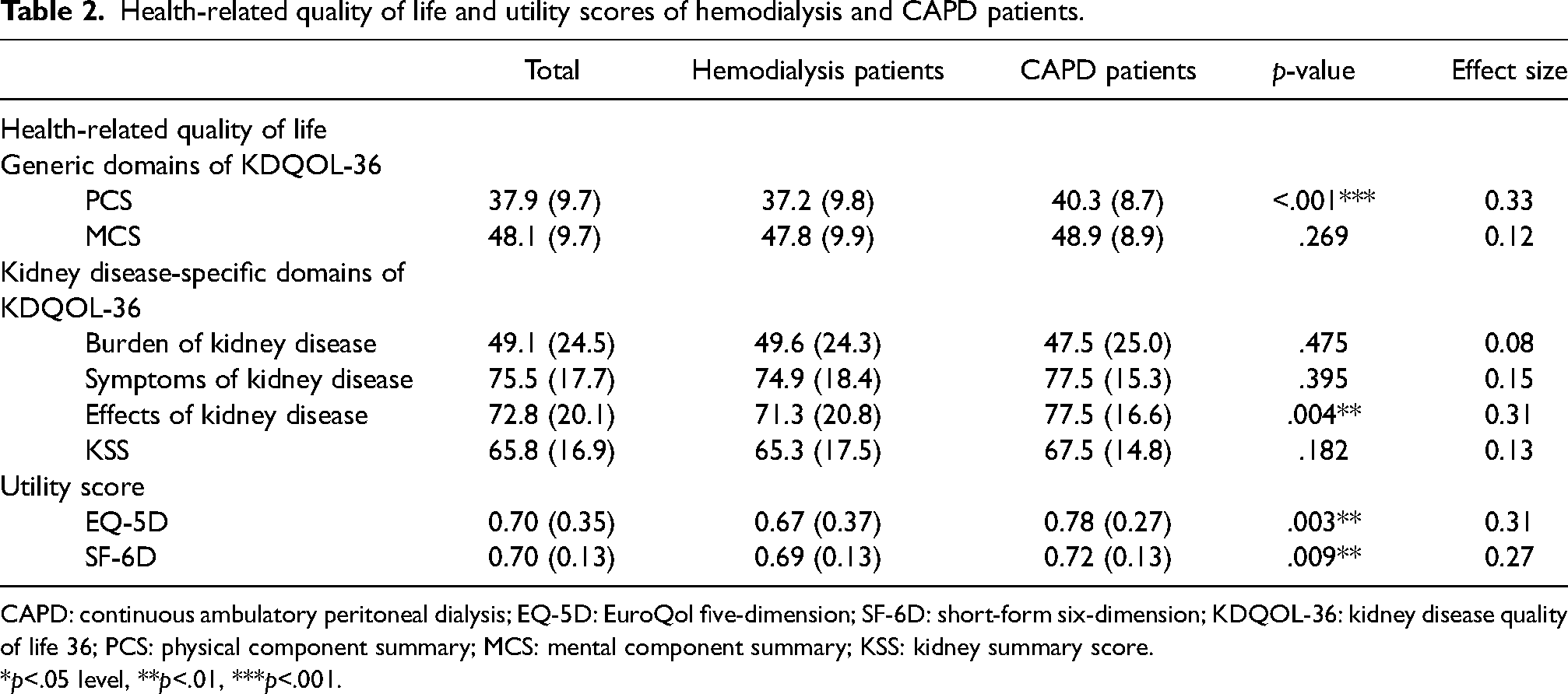
CAPD: continuous ambulatory peritoneal dialysis; EQ-5D: EuroQol five-dimension; SF-6D: short-form six-dimension; KDQOL-36: kidney disease quality of life 36; PCS: physical component summary; MCS: mental component summary; KSS: kidney summary score.
*p<.05 level, **p<.01, ***p<.001.
Effect sizes were higher than 0.3 in the EQ-5D utility score (d = 0.31), PCS (d = 0.33), and effects of kidney disease (d = 0.31), while the SF-6D utility score had an effect size of 0.27. These effect sizes were only considered small differences. Other HRQoL domains, such as MCS, KSS, burden, and symptoms of kidney disease, had effect sizes lower than 0.2.
Predictors of HRQoL and utility scores
Tables 3 and 4 display the results of the regression analysis. Predictors for EQ-5D utility scores were analyzed by using a Tobit regression since 26.1% of participants had utility scores equal to 1, while other analyses were conducted using generalized linear models. After introducing sociodemographic characteristics and clinical parameters into the model, CAPD patients reported better HRQoL over the HRQoL of hemodialysis patients in terms of SF-6D (p = .038), MCS (p = .020), symptoms (p = .005), and effects of kidney disease (p<.001). The comparison of results between generalized linear models and multivariate linear regressions is displayed in Supplemental Table S3.
Predictors of utility scores and generic domains in hemodialysis and CAPD patients
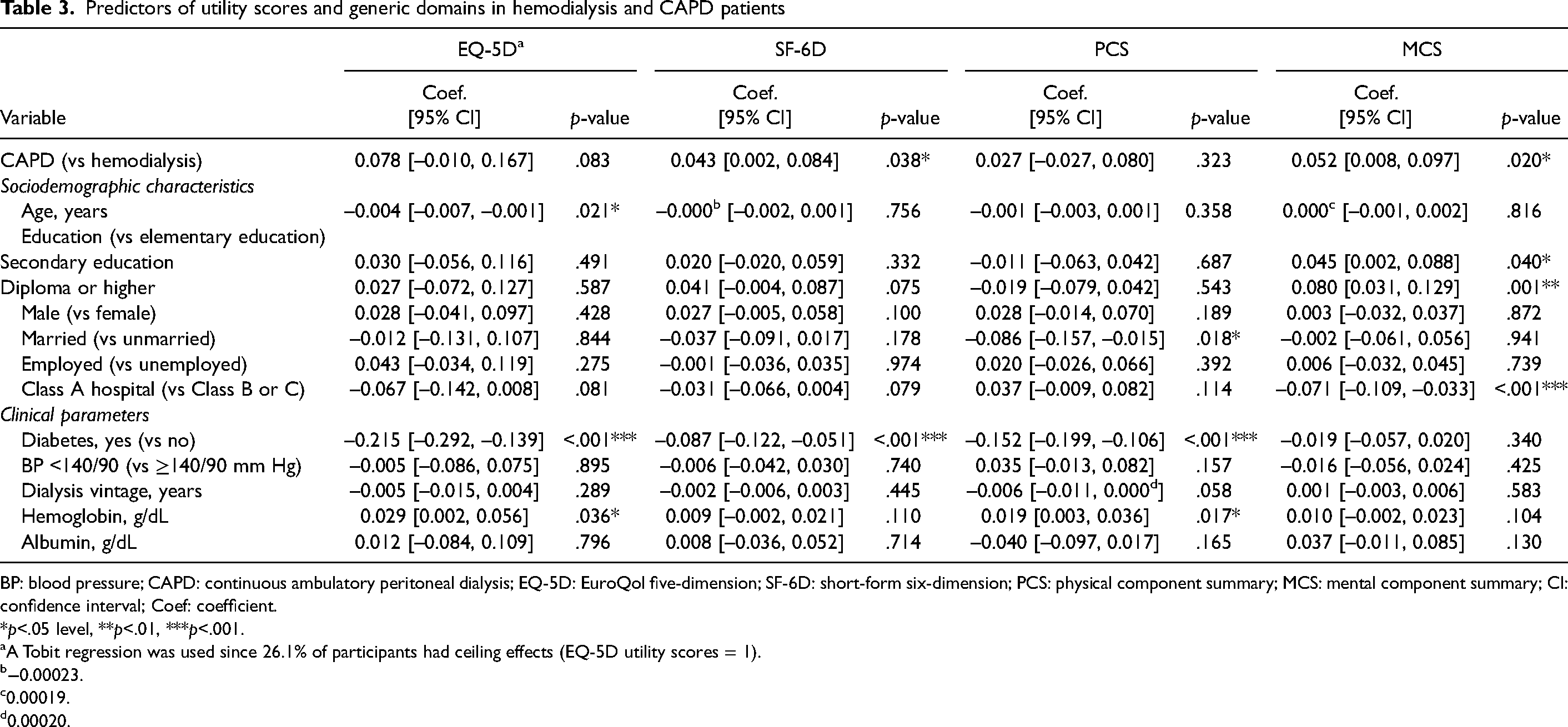
BP: blood pressure; CAPD: continuous ambulatory peritoneal dialysis; EQ-5D: EuroQol five-dimension; SF-6D: short-form six-dimension; PCS: physical component summary; MCS: mental component summary; CI: confidence interval; Coef: coefficient.
*p<.05 level, **p<.01, ***p<.001.
A Tobit regression was used since 26.1% of participants had ceiling effects (EQ-5D utility scores = 1).
−0.00023.
0.00019.
0.00020.
Predictors of kidney disease-specific domains of KDQOL-36 in hemodialysis and CAPD patients.
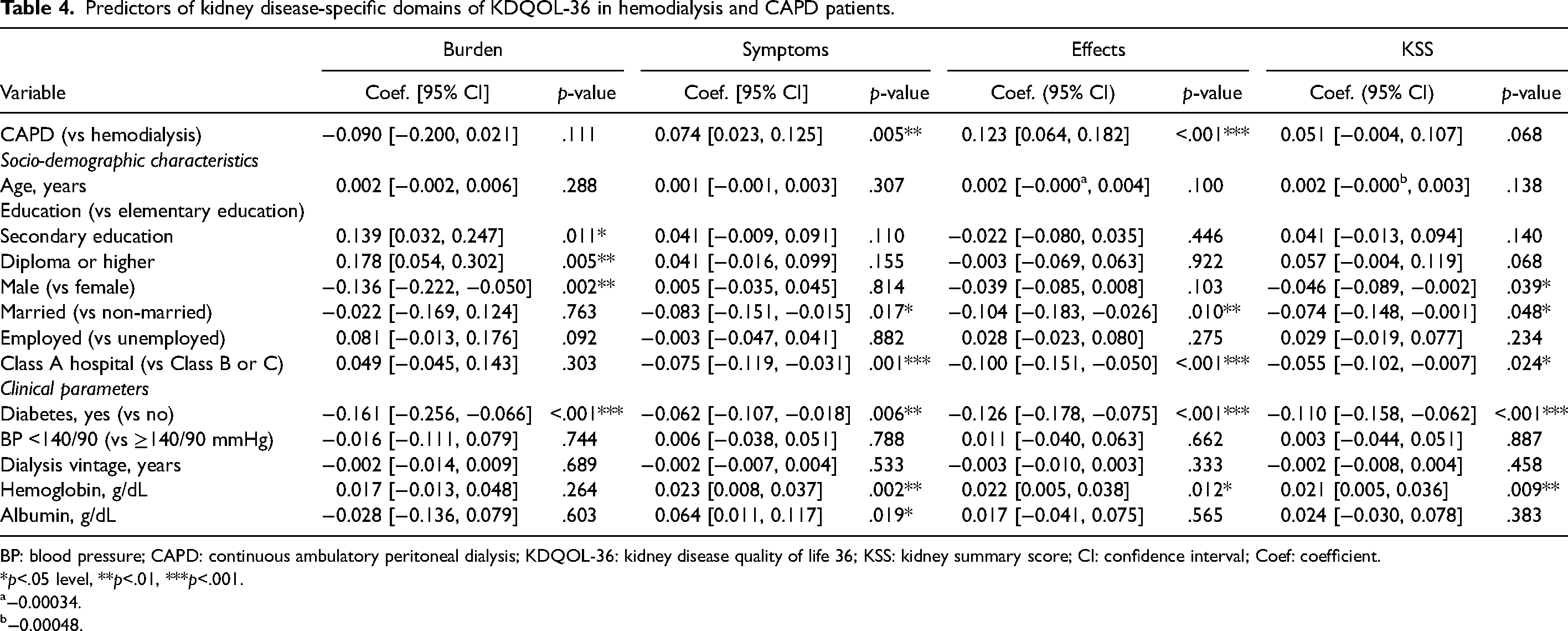
BP: blood pressure; CAPD: continuous ambulatory peritoneal dialysis; KDQOL-36: kidney disease quality of life 36; KSS: kidney summary score; CI: confidence interval; Coef: coefficient.
*p<.05 level, **p<.01, ***p<.001.
−0.00034.
−0.00048.
Supplemental Figure S2 compares effects of kidney disease for hemodialysis and CAPD patients. Almost in all items, CAPD patients reported being less bothered with the effects of kidney disease in daily life. The largest differences were found in the fluid restriction, dietary intake, and dependency on medical staff items, measuring 31%, 20%, and 10%, respectively.
Aside from actual dialysis modality, sociodemographic characteristics and clinical parameters had an effect on HRQoL and utility scores (Tables 3 and 4). Compared to patients with an education of no higher than elementary school, patients with higher education levels had significantly better HRQoL in terms of MCS and burden of kidney disease. Patients who were married had lower PCS (p = .018), KSS (p = .048), symptoms (p = .017), and effects of kidney disease (p = .010) scores compared to those who were unmarried. Overall, patients treated in Class A hospitals had significantly lower MCS (p<.001), KSS (p = .024), symptoms (p = .001), and effects of kidney disease (p<.001) scores compared to patients treated in Class B or C hospitals. History of diabetes was associated with significantly lower HRQoL and utility scores, except for a nonsignificant difference in MCS (p = .340). Patients with lower hemoglobin levels scored significantly lower in EQ-5D (p = .036), PCS (p = .017), KSS (p = .009), symptoms (p = .002), and effects of kidney disease (p = .012). Male patients had lower scores in KSS (p = .039) and burden of kidney disease (p = .002). In addition, older patients had lower EQ-5D utility scores (p = .021), and patients with higher albumin levels scored higher in symptoms of kidney disease (p = .019).
Discussion
This study was the first to compare HRQoL and utility scores in kidney failure disease patients undergoing hemodialysis and CAPD in Indonesia using both generic and disease-specific instruments. A primary finding was that CAPD patients had better HRQoL in terms of SF-6D, MCS, symptoms, and effects of kidney disease after adjusting for sociodemographic characteristics and clinical parameters. Moreover, poorer HRQoL and utility scores were likely experienced by older patients who were male, married, with diabetes, treated in Class A hospitals, and with lower education, hemoglobin, and albumin levels.
CAPD patients have more flexibility compared to hemodialysis patients, in which case they can perform dialysis in more comfortable places at home, leading to better HRQoL. 41 Based on patients’ perspectives in our study, CAPD was the preferred dialysis modality to hemodialysis. This is in line with previous studies that found better HRQoL in CAPD patients in terms of SF-6D, 36 PCS, 36 effects of kidney disease,13,19 and KSS, 20 while other studies found no significant differences.34,42 A previous study conducted in Indonesia showed the opposite findings from our study, reporting no difference in HRQoL. 18 However, this particular study only made use of a generic HRQoL instrument, and the conclusion made was based solely on a descriptive system pertaining to the five dimensions of the EQ-5D without actually calculating utility scores. 18 Therefore, our study, which applied both generic and kidney disease-specific instruments, is expected to better represent the HRQoL and utility scores of patients undergoing hemodialysis and CAPD in Indonesia.
In our study, CAPD patients reported not only fewer effects of kidney disease in daily life, mainly due to lesser restrictions in fluid and dietary intake, but also less dependence on medical staff compared to hemodialysis patients. This information might be useful for eligible patients when deciding on whether to choose CAPD or hemodialysis. A previous study exploring the decision-making process involving different dialysis modalities in Japan showed that dietary and food restrictions were, from patients’ perspective, the main disadvantages of hemodialysis. 43 Considering that CAPD is performed on a daily basis, patients on CAPD do not store as much potassium, sodium, and fluid in their bodies as they would if receiving hemodialysis and, as a result, they do not need to strictly regiment their fluid and potassium intake. 44 However, it is recommended that CAPD patients increase their protein intake to a higher level than patients undergoing hemodialysis would take due to protein loss during the fluid exchange. 45
Patients undergoing dialysis who were male, older, married, with a lower educational level, with a history of diabetes, lower in hemoglobin and albumin levels, and treated in Class A hospitals were at greatest risk for presenting poorer HRQoL and utility scores. Therefore, more attention needs to be paid to these patients. Patients treated in Class A hospitals are expected to have lower HRQoL than patients treated in Class B or C hospitals as Indonesia uses an upward referral system based on disease criticality, with Class A hospitals treating the most severe of conditions. Married patients expressed gratitude for the support that they received from their spouse but at the same time felt guilty for being a burden on their spouse,19,46 making them demonstrate lower HRQoL compared to unmarried patients. In addition, married patients in our study were older on average, while age had a negative correlation with HRQoL. 47 In our study, male patients had poorer HRQoL than did female patients, although other studies confirmed that females have poorer HRQoL.19,36 This could be the case since males in Indonesia typically bear greater responsibility for meeting their families’ needs, while dialysis treatment limits their ability to fulfill such crucial responsibility, exacerbating the burden of kidney disease on them. Patients with longer dialysis vintage also require management of chronic complications associated with kidney failure disease, such as mineral bone disorder, in order to avoid further impairment. However, in our study, dialysis vintage had no association with HRQoL and utility scores, as shown in another study. 47
This study supports the finding that CAPD patients have better HRQoL and utility scores. Therefore, it is important that CAPD be actively promoted as an alternative dialysis modality moving forward. This finding can serve as additional evidence guiding nephrologists when advising patients on dialysis modality suitability and/or selection. It should be noted that patients who elect for peritoneal dialysis are usually more involved in the decision-making process compared to hemodialysis patients. 48 Therefore, there rises a need to provide better education for healthcare professionals on the benefits of CAPD in order to ensure patients are able to make a more informed decision on dialysis modality selection. Previous studies have also documented that the decision-making process for dialysis modality selection is also influenced by a patient's family. 43 Therefore, considering the burden that dialysis treatment may present to family members, and to ensure that they are properly informed to contribute to the decision-making process, healthcare professionals need to also ensure that these affected parties are educated on the benefits of CAPD. Nevertheless, a recent study reported a challenge to implementing this decision-making process since approximately 90% of new patients are referred to nephrologists late, leading to limited available time for choosing the type of dialysis and predialysis treatment to apply. 49
Promisingly, the Indonesian Ministry of Health is expected to increase patient access to CAPD services throughout regions where the numbers of kidney failure disease patients are relatively small as commissioning hemodialysis units at hospitals for small patient numbers is not cost-effective. 50 At this time, hemodialysis patients are required to travel three to four times a week to neighboring cities to receive routine treatment; thus, CAPD treatment will be more cost- and time-efficient for these patients as it does not require weekly visits to dialysis units. 50 To reduce the burden of people on dialysis, the Indonesian government is also encouraged to consider implementing early screening for chronic kidney disease, especially in patients with diabetes, since a recent systematic review has reported that screening for chronic kidney disease is a cost-effective intervention. 51
Among the strengths of this study is its inclusion of a broad range of participants from four public and two private hospitals across four different provinces, encompassing all major hospital classifications. Another strength is that HRQoL and utility scores were calculated using kidney disease-specific in addition to generic instruments. Despite these notable strengths, there are some limitations that need to be acknowledged. The first limitation is that dialysis adequacy could not be included in regression models as data for dialysis adequacy only existed for hemodialysis patients. Although previous studies and systematic review found that dialysis adequacy is not strongly associated with HRQoL,19,20,52 Yang et al. (2018) speculated that dialysis adequacy might instead adversely affect HRQoL in patients treated with peritoneal dialysis. 47 In addition, due to limited data, we were unable to determine the Charlson Comorbidity Index and only considered diabetes as a comorbidity. The last limitation is that this study applied a cross-sectional study design, so causation between variables and HRQoL or utility scores could not be determined. Therefore, we suggest that any future research be performed using a prospective research design.
Conclusion
Patients treated with CAPD had better HRQoL and higher utility scores when compared to patients treated with hemodialysis. Based on this finding, it is suggested that CAPD be promoted by healthcare professionals and that patients eligible for both hemodialysis and CAPD be offered CAPD as the first treatment option. Moreover, patients who are male, married, older, with a history of diabetes, with lower education, hemoglobin, and albumin levels, and treated in Class A hospitals should receive the most attention.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608241285969 - Supplemental material for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia
Supplemental material, sj-docx-1-ptd-10.1177_08968608241285969 for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia by M Rifqi Rokhman, Yulia Wardhani, Dwi Lestari Partiningrum, Barkah Djaka Purwanto, Ika Ratna Hidayati, Arofa Idha, Jarir At Thobari, Maarten J Postma, Cornelis Boersma and Jurjen van der Schans in Peritoneal Dialysis International
Supplemental Material
sj-docx-2-ptd-10.1177_08968608241285969 - Supplemental material for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia
Supplemental material, sj-docx-2-ptd-10.1177_08968608241285969 for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia by M Rifqi Rokhman, Yulia Wardhani, Dwi Lestari Partiningrum, Barkah Djaka Purwanto, Ika Ratna Hidayati, Arofa Idha, Jarir At Thobari, Maarten J Postma, Cornelis Boersma and Jurjen van der Schans in Peritoneal Dialysis International
Supplemental Material
sj-docx-3-ptd-10.1177_08968608241285969 - Supplemental material for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia
Supplemental material, sj-docx-3-ptd-10.1177_08968608241285969 for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia by M Rifqi Rokhman, Yulia Wardhani, Dwi Lestari Partiningrum, Barkah Djaka Purwanto, Ika Ratna Hidayati, Arofa Idha, Jarir At Thobari, Maarten J Postma, Cornelis Boersma and Jurjen van der Schans in Peritoneal Dialysis International
Supplemental Material
sj-docx-4-ptd-10.1177_08968608241285969 - Supplemental material for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia
Supplemental material, sj-docx-4-ptd-10.1177_08968608241285969 for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia by M Rifqi Rokhman, Yulia Wardhani, Dwi Lestari Partiningrum, Barkah Djaka Purwanto, Ika Ratna Hidayati, Arofa Idha, Jarir At Thobari, Maarten J Postma, Cornelis Boersma and Jurjen van der Schans in Peritoneal Dialysis International
Supplemental Material
sj-docx-5-ptd-10.1177_08968608241285969 - Supplemental material for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia
Supplemental material, sj-docx-5-ptd-10.1177_08968608241285969 for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia by M Rifqi Rokhman, Yulia Wardhani, Dwi Lestari Partiningrum, Barkah Djaka Purwanto, Ika Ratna Hidayati, Arofa Idha, Jarir At Thobari, Maarten J Postma, Cornelis Boersma and Jurjen van der Schans in Peritoneal Dialysis International
Supplemental Material
sj-xlsx-6-ptd-10.1177_08968608241285969 - Supplemental material for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia
Supplemental material, sj-xlsx-6-ptd-10.1177_08968608241285969 for Comparing health-related quality of life and utility scores of patients undergoing hemodialysis and continuous ambulatory peritoneal dialysis in Indonesia by M Rifqi Rokhman, Yulia Wardhani, Dwi Lestari Partiningrum, Barkah Djaka Purwanto, Ika Ratna Hidayati, Arofa Idha, Jarir At Thobari, Maarten J Postma, Cornelis Boersma and Jurjen van der Schans in Peritoneal Dialysis International
Footnotes
Acknowledgments
We acknowledge the help of all the participants and research assistants, especially Faradiba, Shahiroh Haulaini, Arly Tania Putri, Dian Pita Sabella, and Januari Erik Pratama.
Author contributions
MRR, YW, DLP, BDP, IRH, and AI carried out the data collection. MRR drafted the manuscript. MRR, JAT, CB, JvdS, and MJP contributed to the data analysis and interpretation. All authors were involved in the conceptualization and design, provided input, and read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MJP and CB reported grants and honoraria from various pharmaceutical companies. However, all grants and honoraria were fully unrelated to this specific study. The other authors declare that they have no competing interests related to this specific study and topic.
Ethical approval
The study was approved by the Medical and Health Research Ethics Committee (MHREC), Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada–Dr Sardjito General Hospital with document numbers KE/FK/0952/EC/2020 (dated 27 August 2020) and KE/FK/1000/EC/2021 (dated 3 August 2021). The KDQOL instrument from RAND Healthcare is a public document, while the EQ-5D-5L instrument was used with permission from the EuroQol research group with registration number 42861.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Lembaga Pengelola Dana Pendidikan (Grant No. PRJ-1/LPDP.3/2019).
Informed consent to participate
Written informed consent was obtained from all subjects before the study.
Informed consent to publish
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Availability of data and materials
The dataset of this article is available online as a supplementary material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.