
Abstract
Introduction
Peritoneal dialysis (PD) related infections are a significant obstacle leading to PD discontinuation. Since catheter related infections (CRI), defined as exit site infections and/or tunnel infection, can progress to peritonitis, vigorous efforts are implemented in CRI prevention. Following an increased CRI rate in our institution, partially related to environmental organisms found in water distribution systems, we hypothesized that exit site care that includes prevention of water exposure-related pathogens may reduce CRI.
Methods
In this prospective single center study, we compared a contemporary cohort consisting of PD patients who implemented the modified exit-site care protocol, mainly including water avoidance during shower with stoma bag usage and local Mupirocin ointment against a historical control group before the protocol implementation. The historical cohort was allowed water exposure and used local gentamicin ointment. The primary outcome was the development of a CRI. Secondary outcomes were PD associated peritonitis and infection related outcomes.
Results
There were 55 patients in contemporary cohort and 58 in historical group. The CRI rate was significantly lower in study group (0.11/episodes per patient year [EPP]) compared to control group (0.71 EPP), p < 0.001. A multivariate Cox regression analysis demonstrated a protective effect of being in the contemporary cohort compared to historical group (HR for first CRI = 12.0 95%CI: 4.0–35.7, p < 0.001). Peritonitis rate was significantly lower in contemporary cohort (0.19/EPP) compared to the historical group (0.40/EPP), p = 0.011. Transfer to hemodialysis was significantly lower in contemporary cohort than historical group (7.3% vs 31.0% in contemporary and historical group respectively, HR = 0.2, 95%CI; 0.05–0.6, p = 0.001).
Conclusion
An exit site care protocol that includes water avoidance and local Mupirocin use reduced substantially both CRI and peritonitis rate in patients treated with PD.
Keywords
Introduction
Peritoneal dialysis (PD) is a cost-effective dialysis modality, however, it is underutilized worldwide, as approximately 11% of dialysis patients perform PD globally. 1 Various barriers influence patients’ recruitment and retention. Peritoneal dialysis related infection is an important and preventable cause of catheter loss and PD discontinuation,2,3 therefore vigorous efforts must be implanted to reduce its frequency.
While the primary aim of infection preventive measures is focused on peritonitis rate reduction, prevention of catheter related infection (CRI) is highly important, as both exit-site infection (ESI) and tunnel infection (TI) may migrate and result in catheter-related peritonitis. 4 Different protocols are used for exit-site care, mainly focusing on hand hygiene, exit-site cleaning and application of local antibiotic cream or ointment. 5 There is no consistency in the local antibiotics used, as different studies demonstrated conflicting results, hence the International Society for Peritoneal Dialysis (ISPD) guidelines recommend the use of either Mupirocin or Gentamicin on catheter exit site. 6 Most protocols oppose swimming or bath immersion, but allow shower with running water. 7 Our local exit site care policy has evolved over the years according to causative organisms. In 2016, following a rise in Pseudomonas-related catheter infections, we switched from local Mupirocin to Gentamicin. Subsequently, we noticed an increased ESI rate caused by environmental organisms found in drinking water distribution systems, such as Acinetobacter, Achromobacter and non-tuberculous (atypical) mycobacteria. 8
As a substantial amount of ESI events were driven from drinking water distribution systems, we searched for a method to prevent water exposure to the catheter and exit-site. Additionally, although several studies demonstrated a reduction in ESI episodes caused by gram negative organisms while using Gentamycin as compared to Mupirocin,9,10 since in practice we had experienced many infection episodes caused by gram negative bacteria, including Pseudomonas, we hypothesized that Gentamycin suppressed natural skin flora, leading to growth of environmental and opportunistic organisms, and therefore aimed to narrow the antibiotic range. Therefore, the new exit-site care protocol mainly included the use of a stoma bag to cover the catheter during showering, and a change in antibiotic treatment to Mupirocin. We previously reported short-term results of the protocol implementation, in which we presented a significant reduction in ESI rate after one year. 11 Herein we introduce the results of long term follow up of the novel exit-site care practice.
Methods
This is a prospective single center study, aimed to evaluate outcomes of a novel exit-site care practice on PD related infections. The study was approved by local ethics committee and each participant signed informed consent.
Detailed explanations on study design and exit-site care protocols were published previously. 11 In brief, the study (contemporary) group consisted of PD patients in our dialysis unit between June 2018 and May 2021 who implemented a new exit-site care protocol. They were compared to a historical control group that included all PD patients in our unit between January 2016 and May 2018. Prevalent patients had a 90-day wash out period to avoid bias of bacterial colonization resulting from the historical period exit-site policy. Data was collected prospectively for the contemporary cohort and retrospectively for historical group.
Exit site care protocol
In the historical group, exit-site care included a daily shower with a bactericidal cleanser containing chlorhexidine 4%, thereafter cleansing with sterile water and applying local gentamicin 0.1% ointment with sterile gauze dressing. In the contemporary group, water exposure during daily wash was avoided using a stoma bag sealed around the catheter exit-site and containing the tubing. After shower, the exit-site was cleaned with a chlorhexidine 0.5%- alcohol 70% solution and local mupirocin 2% ointment was applied with a sterile gauze cover. The application of a stoma bag over the catheter is demonstrated in Figure 1.
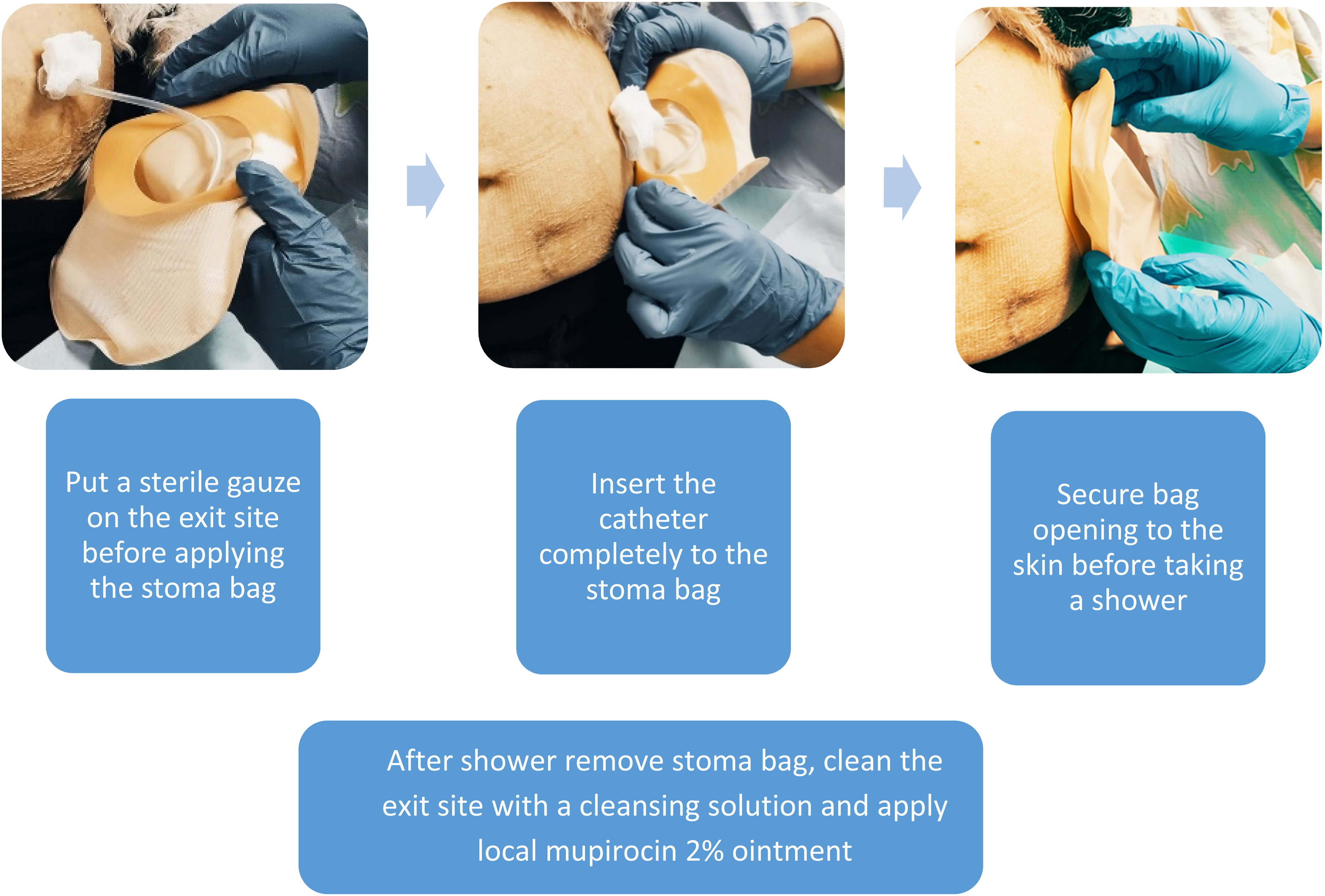
Stoma bag application instructions.
In both groups patients were routinely screened for Staphylococcus aureus nasal carriage before catheter insertion and following episodes of CRI. Positive cases were treated using intranasal Mupirocin ointment 3 times daily for 7 days, combined with a daily shower with Chlorhexidine 4% soap. Eradication was confirmed.
Clinical outcomes
Primary outcome was defined as CRI, including a combination of ESI and tunnel infection. Secondary outcomes were PD associated peritonitis, catheter salvage intervention, transfer to hemodialysis due to infection and 30 days mortality after a peritonitis episode.
Peritonitis, ESI or TI were diagnosed according to ISPD guidelines.5,12 Data collected included infection date, the causative organisms and outcomes. In incident patients, infection episodes were calculated if occurred 30 days after Tenckhoff catheter insertion to prevent bias resulting from surgical complications. This criterion corresponds with the ISPD 2022 updated guidelines definition of PD catheter insertion-related peritonitis. 13
Environmental organisms were defined as organisms found in water distribution systems including Pseudomonas, Mycobacteria, fungi, Diphtheroids, Serratia, Proteus, Acinetobacter and Acromobacter infections.14–16 While some of the above organisms can originate from the gastrointestinal system, they are also found in water pipes. Moreover, we do not anticipate to grow enteric bacteria from the catheter exit-site. To answer these controversies, every organism's definition was discussed in-depth with infectious disease specialist to decide which organisms will be defined as environmental.
Catheter salvage intervention consisted of external cuff shaving with exit site diversion for refractory exit site infection, after proving that there is no tunnel / inner cuff involvement using ultrasound.
Statistical analysis
Data is presented as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate for the distribution, for the continuous variables. Data is displayed as number of patients and the percentage in each group for categorical pre- and post-implementation of the new exit-site care policy, while controlling for potential confounders.
Time to infection was analyzed using Kaplan-Meier analysis (Log-Rank test) and Cox regression analysis while adjusting for co-variates including age, diabetes, ischemic heart disease, heart failure, obesity, active cancer, participation in both historical and contemporary groups and PD time included as a time-dependent covariate. Peritonitis and CRI rates were calculated as the number of events divided by the total follow-up time (in years). They were compared by zero inflated Poisson regression analysis. Proportion of patients free of CRI or peritonitis was calculated as the number of patients free from events divided by the total number of patients in the specific group.
The Number Needed to Treat (NNT) was calculated as control event rate minus experimental event rate.
P-value <0.05 was considered statistically significant. All statistical tests were two tailed. IBM SPSS Statistics for Windows, version 28 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses.
Results
A total of 113 patients were included, 58 patients in the historical group and 55 in the contemporary cohort. Twenty patients from the historical group signed informed consent and entered washout period, among them 5 were not included in the statistical analysis (2 cardiovascular death, 2 switched to hemodialysis due to PD related peritonitis and one had a deceased donor kidney transplantation). Thus, the contemporary cohort included 15 crossed-over patients and 40 incident PD patients. There were no cases of active CRI upon transition from the historical group to the contemporary cohort. Mean age was 69.95, 61% were males. Mean follow up time was 13.28 ± 9.5 months in historical and 16.4
Patients baseline characteristics.
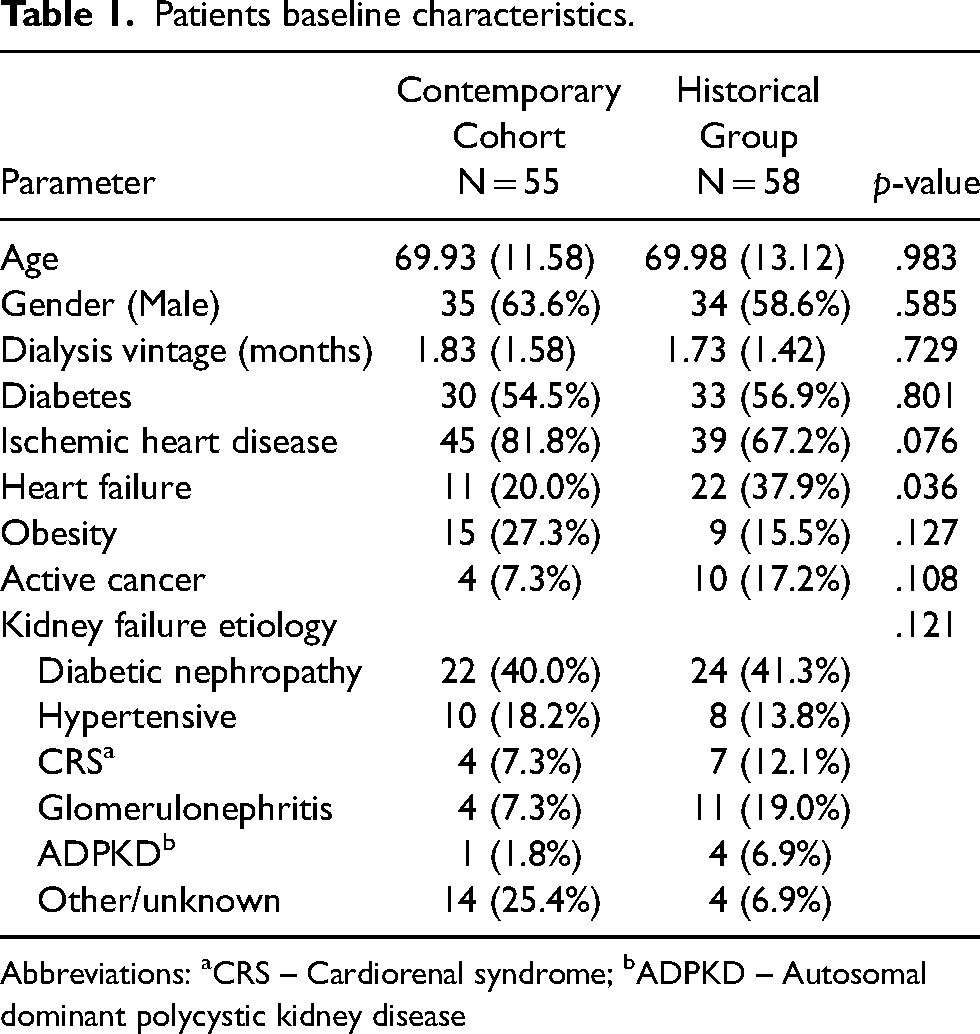
Abbreviations: aCRS – Cardiorenal syndrome; bADPKD – Autosomal dominant polycystic kidney disease
In the contemporary cohort, 3 patients had difficulty handling the stoma bag, which was substituted successfully with a designated belt that protects the catheter from water exposure during shower.
Primary outcome
In the contemporary cohort, 8 CRI episodes were observed in 5 patients, all considered ESI, compared to 44 CRI in 27 patients in the historical group, among them 3 were diagnosed as TI.
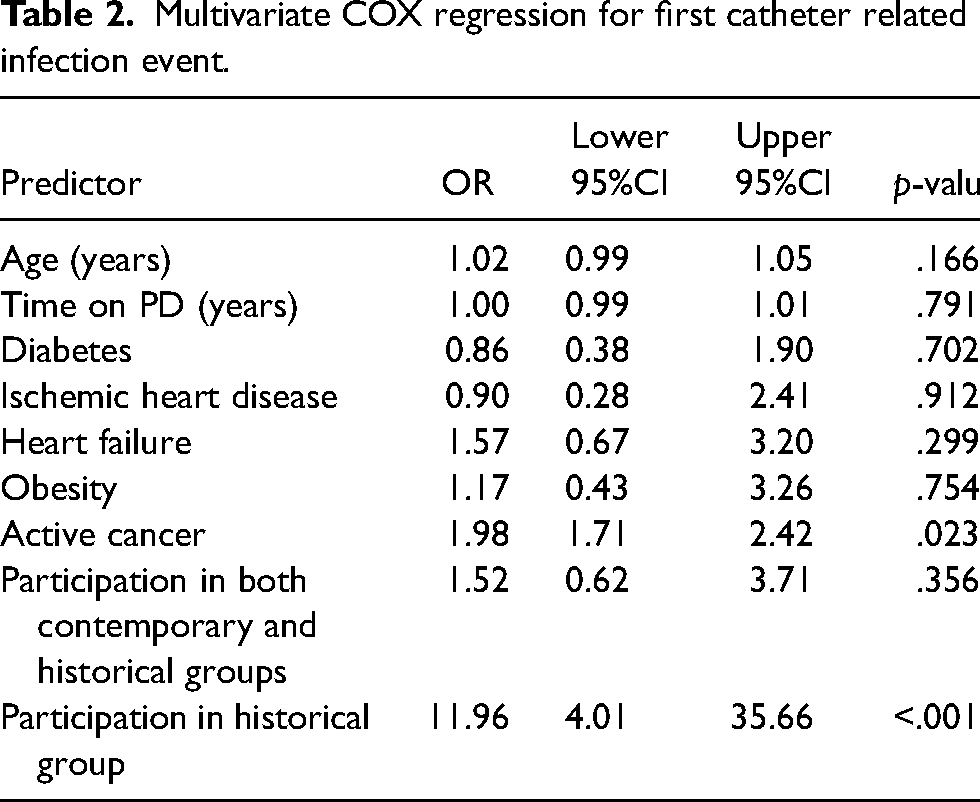
Fifty patients were free of infection at the study group (90.9%) compared to only 31 at the control group (53.4%). The number needed to treat to prevent one case of first infection was 3. Rate of CRI was significantly lower in contemporary cohort (0.11/EPP compared to historical group (0.71/ EPP), p < 0.001 at zero inflated Poisson regression analysis (IRR = 5.0, 95%CI;2.9–8.7). Time to first CRI was significantly longer in the contemporary cohort compared to the control group at Kaplan-Meier log-rank test, χ² (1) = 25.104, p < 0.001 (Figure 2). Univariate Cox regression analysis further demonstrated a substantially higher hazard ratio of experiencing a first CRI event in the control group compared to the contemporary cohort (HR = 8.3, 95%CI: 3.1–21.8, p < 0.001) (Figure 3). The protective effect of being in the contemporary cohort was also confirmed on a multivariate Cox regression analysis (HR for first ESI = 12.0, 95%CI: 4.0–35.7, p < 0.001) even after controlling for confounding factors (Table 2). Active cancer was the only significant covariate predictor of experiencing a first CRI event (HR = 2.0, 95%CI: 1.7–2.4, p = 0.023).
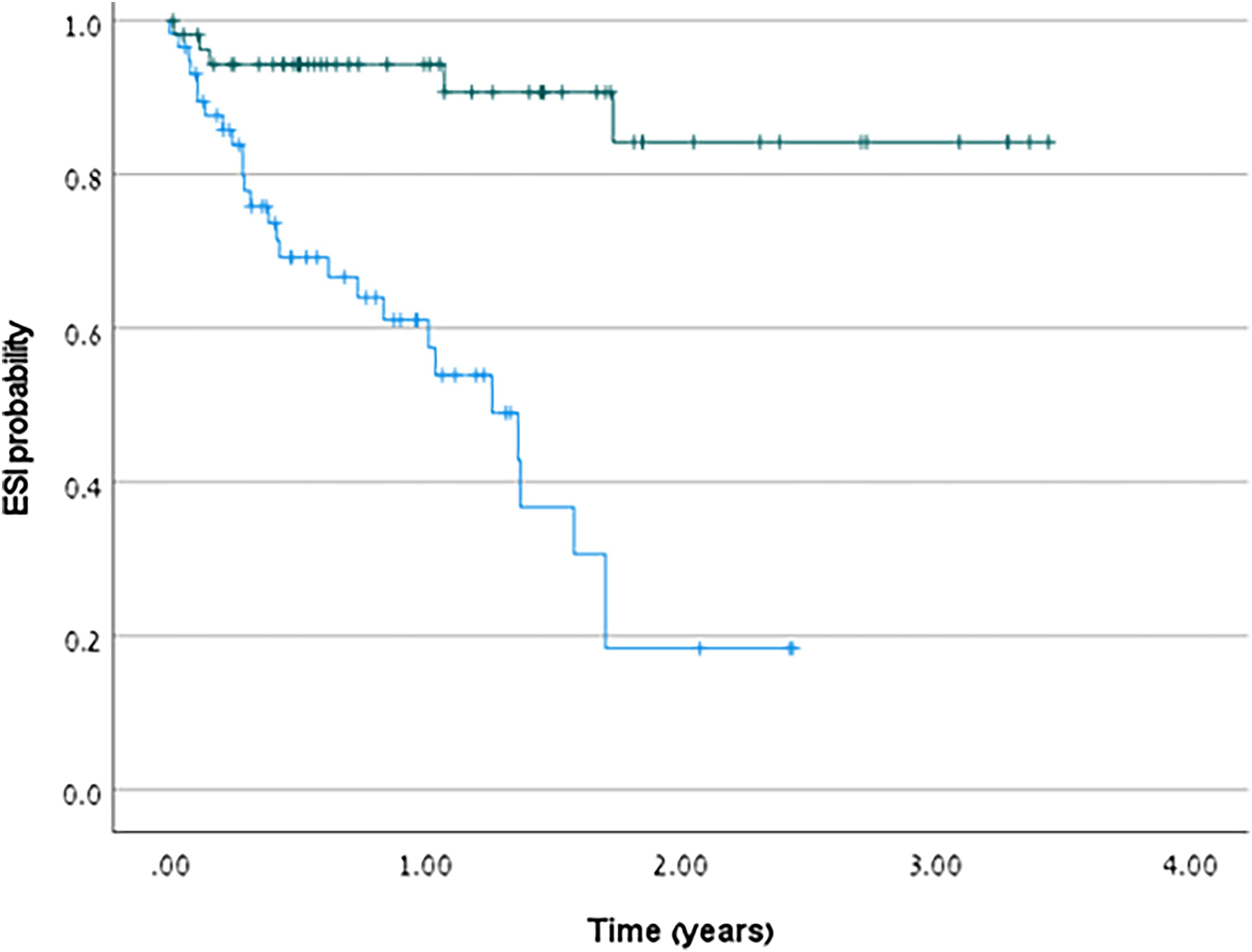
Kaplan Meier curve for first catheter related infection episode.
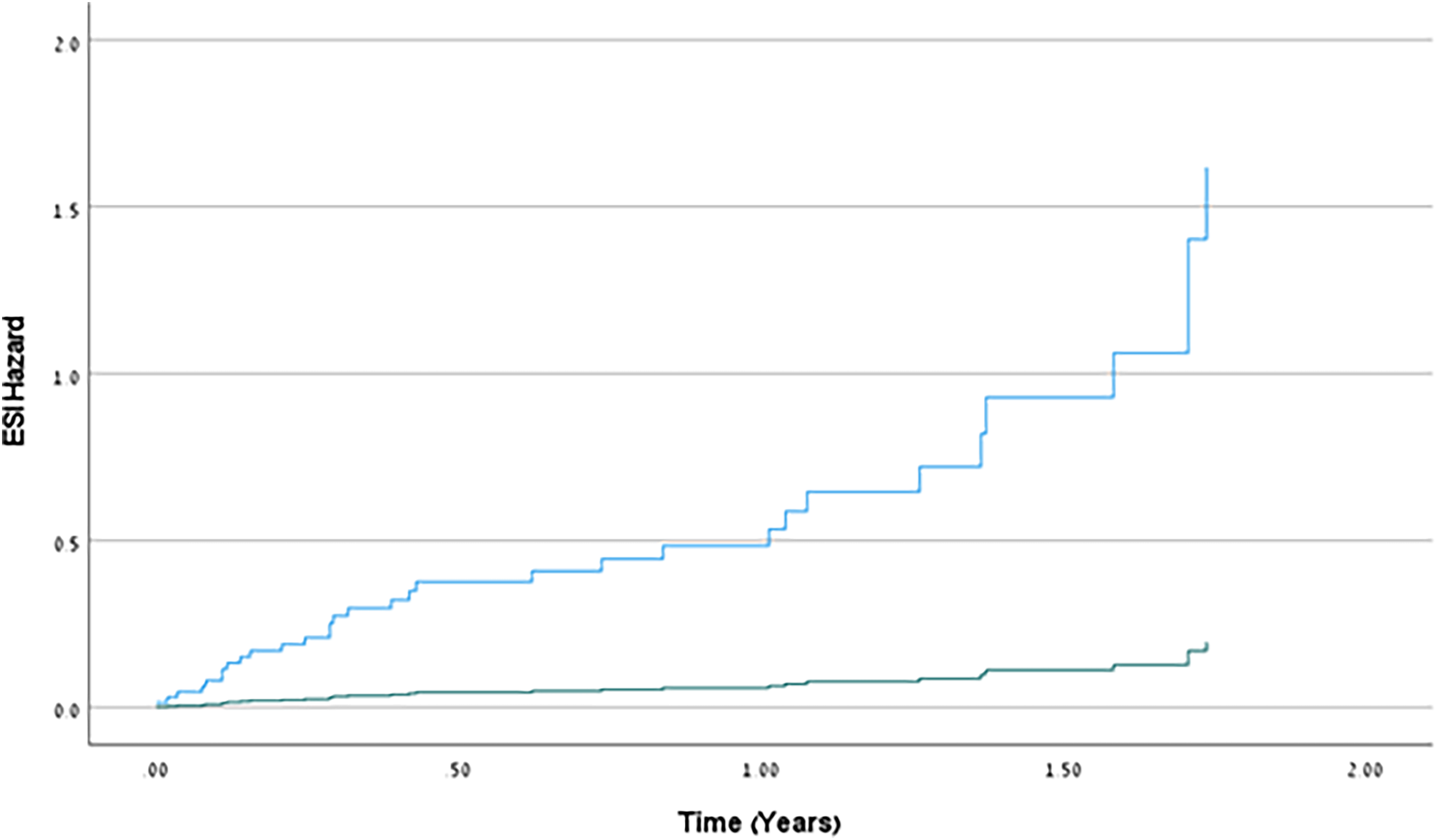
Hazzard function for first catheter related infection episode.
Multivariate COX regression for first catheter related infection event.
The causative organisms are presented in Table 3. Environmental organism accounted for 4 CRI episodes in the contemporary group (50%), as opposed to 32 CRI episodes in the historical group (72.7%), however, differences didn't reach statistical significance, χ² (1) = 1.64, p = 0.20.
Characteristics of catheter infection and peritonitis in the cohort.
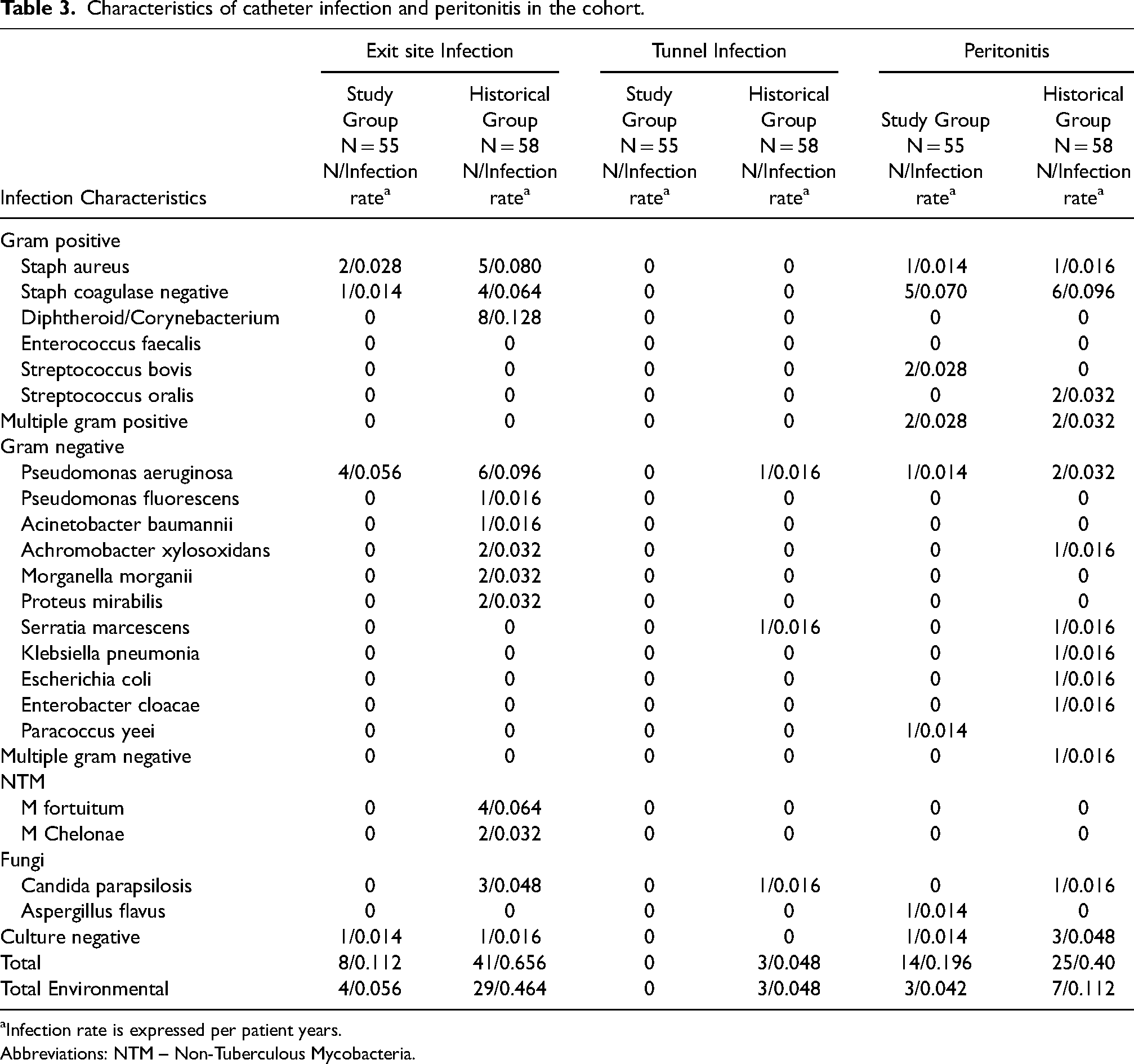
Infection rate is expressed per patient years.
Abbreviations: NTM – Non-Tuberculous Mycobacteria.
Secondary outcomes
Peritonitis
One patient in the historical group developed PD catheter insertion-related peritonitis that was excluded from the analysis, compared to none in the contemporary cohort.
In the contemporary cohort, 14 peritonitis episodes were observed in 13 patients, compared to 25 in 20 patients in the historical period. Two episodes in the contemporary cohort were defined as catheter-related peritonitis compared to 5 in historical group. Peritonitis rate was significantly lower in study group (0.19/EPP) compared to control group (0.40/ EPP), p = 0.011 at zero inflated Poisson regression analysis (IRR = 1.9, 95%CI;1.2–3.3).
There was no difference in incidence of peritonitis caused by environmental organisms between groups. Environmental organisms accounted for 3 peritonitis events in contemporary cohort (21.4%) and 7 in the historical group (30.4%) (χ² (1) = 0.36, p = 0.55) (Table 3).
Kaplan-Meier log-rank test (χ² (1) = 2.32, p = 0.128) and univariate Cox regression (HR = 1.1, 95%CI; 0.5–2.3, p = 0.776) did not detect a statistically significant difference in time to first peritonitis between the groups.
Other outcomes
Hazzard Ratio for transfer to hemodialysis was significantly lower in contemporary cohort than historical (N = 4, 7.3%, N = 18, 31.0%respectively, HR = 0.2, 95%CI; 0.05–0.6, p = 0.001). Reasons for infection associated PD discontinuation in contemporary cohort were isolated peritonitis in one patient, catheter related peritonitis in 2 patients and recurrent ESI events caused by inability for self-care in one patient. Transfer to hemodialysis due to PD related infections in historical group resulted from peritonitis in 6 cases (5 catheter related peritonitis and one due to isolated peritonitis), refractory ESI in 10 patients and repeated ESI episodes in 2 patients.
Five patients in the historical group had catheter salvage intervention compared to none in contemporary cohort.
There was one episode of peritonitis related 30-days mortality in the historical group, and none in contemporary cohort.
Discussion
Implementation of the new exit-site care protocol, which mainly includes water avoidance and Mupirocin ointment, resulted in a significant reduction in CRI rate in individuals receiving PD, accompanied by a concomitant decrease in peritonitis episodes.
Rate of CRI in the study group complied with 2023 updated ISPD guidelines recommendation for less than 0.40 episodes per patient year. 6 It decreased significantly from 0.71 episodes per patient year in the historical group to 0.11 episodes in contemporary cohort. While infection risk can be reduced through several measures such as appropriate catheter insertion and design, patient education etc., the current study focused on components of exit site care. Two major modifications were performed in our exit site care protocol: avoiding water exposure and local antibiotic change from Gentamicin to Mupirocin. Although a meta-analysis demonstrated 57% reduction in ESI and 41% reduction in peritonitis when using local Mupirocin versus placebo or no treatment, 17 a randomized controlled trial compared local Mupirocin to Gentamicin and demonstrated greater efficacy of Gentamicin in ESI prevention. 9 Throughout the years studies identified conflicting results.10,18,19 Therefore, ISPD guidelines concluded that the comparative efficacies of Mupirocin and Gentamicin are uncertain and could not recommend one over the other. 6 Considering this data, we speculate that the local antibiotic change could not fully explain the significant reduction in CRI rate and that water avoidance was an important component. In the control period the use of gentamicin cream, that has a broader antibiotic spectrum, might have contributed to local suppression of indigenous skin flora, resulting increased susceptibility for colonization and subsequent infection by opportunistic premise plumbing pathogens. 20 Opportunistic plumbing pathogens are environmental microorganisms found in water distribution systems. They share common characteristics such as biofilm formation, growth under low-nutrient conditions, disinfectant resistance and thermal tolerance, allowing adapted growth and colonization of domestic water systems.20,21 Microbes can detach from the biofilm and cause infection in vulnerable populations such as immune-compromised individuals, elderly and newborns. These pathogens may adhere to the surface of medical implants, form biofilm and subsequently cause implantable device-related infections that are extremely difficult to eradicate.20,22 As PD catheter is a medical implant, it is therefore prone to biofilm formation and infection. In the current study, water avoidance decreased CRI episodes significantly, probably by reducing opportunistic pathogens exposure. Water avoidance may be less relevant in areas of high-quality municipal water, but highly important in countries with poor water quality.
Prevention of exit site bacterial colonization and infection is a well-recognized method to reduce peritonitis risk, as catheter infection may lead to catheter-related peritonitis. 23 As PD associated peritonitis confers substantial morbidity and mortality, there is an unmet need for better strategies for peritonitis prevention. 13 Although there was no statistically significant difference in environmental organisms related peritonitis, our novel exit-site protocol decreased peritonitis rate considerably. Stoma-bag use is associated with additional costs. A daily shower results in an additional amount of 80 US dollars monthly, according to local prices. Since the number needed to treat was 3 patients to prevent one case of first CRI, we find this protocol cost-effective. Accordingly, we recommend considering implementing the protocol in units with a high catheter infection rate or in areas with poor water quality.
Apart from increased peritonitis risk, catheter infection is associated with additional hazardous complications including exposure to antibiotic treatment with its associated risks. Refractory catheter infection may lead to surgical interventions and can result in unplanned transfer to hemodialysis. 6 CRI was an important cause for PD discontinuation before intervention and improved significantly thereafter.
The study has several limitations. It is a single center non-randomized study. Although patients in the study group were followed prospectively, control group data was collected retrospectively. However, since PD related infections rate is an important quality measure in dialysis units, data was accurately and completely documented without missing data.
Additionally, the new protocol included two major components – avoidance of water exposure and change of antibiotic cream and it is impossible to know if one or both changes were responsible. Another minor modification in exit site care protocol was different local antiseptic used. Various factors can influence infection risk in PD patients, for instance appropriate catheter insertion and design, patient education etc; which can be another limitation. However, our PD team was the same in the historical group and contemporary group, and catheter insertion technique did not change. Patient's training program was also similar in terms of hand hygiene, maintaining aseptic workspace, number of trainings before starting PD independently, etc. The only change in patient's education was regarding the new protocol of exit-site care.
Despite the limitations above, we believe the significant reduction in infection rate we have experienced while following this protocol encourages further randomized controlled trials to validate our findings, specifically looking for the impact of exit site water avoidance.
Conclusions
An exit site care protocol that includes measures to avoid water exposure of the catheter and local Mupirocin ointment significantly reduces both CRI and peritonitis rate in patients treated with PD.
Footnotes
Acknowledgements
We thank our dedicated dialysis nurses Inna Faukman and Rachila Badbalayev for patient education. We thank institute's stoma nurse Maya Shriki for advice and support.
Authorship
HS and OK researched literature and conceived the study. HS and OK were involved in protocol development, gaining ethical approval and patient recruitment. HS, OK, EH and AG were involved in data acquisition and analysis. HS and OK wrote the draft of the manuscript. DS and AW helped in supervision and mentorship. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by Tel Aviv Sourasky ethics committee, approval reference number 0077-18-TLV.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Written informed consent was obtained from all subjects before the study.