
Abstract
Background:
Urgent-start peritoneal dialysis (PD) carries a similar efficacy and safety profile compared to urgent-start haemodialysis (HD) but is only sparsely applied due to resource issues and concerns of complication risks. Furthermore, few data exist on adverse outcomes associated with central venous catheter (CVC) insertions in urgent-start HD patients. Thus, we sought to compare patient and dialysis-related outcomes in patients undergoing urgent-start PD or HD.
Methods:
All patients initiating urgent-start PD in a tertiary research hospital in 2005–2018 were included in this retrospective, single-centre, comparative study and matched with urgent-start HD patients of similar age and chronic kidney disease aetiology. All urgent-start PDs were initiated within 72 h after catheter insertion, and urgent-start HDs were performed via a CVC. All analyses were performed at 3 months and at 1 year of follow-up, respectively.
Results:
Thirty-three patients who commenced urgent-start PD and 58 matched urgent-start HD control patients were included. Altogether, 26 patients (29%; PD: 36%, HD 24%) died within the 1-year follow-up, and patient survival was similar at 3 months (hazard ratio (HR): 1.15, 95% confidence interval (CI): 0.35–3.81, p = 0.82) and at 1 year of follow-up (HR: 0.64, 95% CI: 0.30–1.39, p = 0.26) between the study groups. There were no differences in the total kidney replacement therapy (KRT)-related infection rate (p = 0.66) or cumulative first-year hospital care days (p = 0.43) between the treatment groups. Altogether, 139 CVCs were inserted during the 1-year follow-up. The number of CVCs per patient was associated with the emergence of blood culture-positive bacteraemia and increased cumulative first-year hospital care days.
Conclusions:
Patient survival, cumulative first-year hospital care days and total KRT-related infection rate at 3 months and 1-year follow-up are similar between urgent-start PD and urgent-start HD patients. Furthermore, CVC insertion rate is associated with incident blood culture-positive bacteraemia and increased cumulative first-year hospital care days.
Introduction
Urgent-start kidney replacement therapy (KRT) remains common in acute kidney injury (AKI) and chronic kidney disease (CKD) patients without prior contact to a nephrology clinic but also in patients under established nephrologist care. 1,2 Urgent-start KRT stands for prompt and emergent initiation of dialysis, peritoneal dialysis (PD) or haemodialysis (HD), after dialysis catheter insertion in a patient with imminent symptomatic kidney failure. Despite rigorous efforts in identifying CKD patients at risk for acute KRT initiation 3 and organising pre-dialysis programmes for patients with gradual kidney function decline, 4,5 KRT is initiated urgently 1,6 in 30–50% of these patients. 7,8 Furthermore, urgent-start KRT is associated with increased mortality compared to elective KRT initiation. 9
Traditionally, the KRT modality of choice has been HD via a central venous catheter (CVC) in patients urgently requiring KRT. However, CVCs have been associated with cardiovascular and infectious complications, increased risk of hospitalisation and mortality compared to arteriovenous fistulas in patients undergoing urgent-start HD or patients undergoing urgent-start PD. 10 –12 Urgent-start PD was defined by Blake and Jain in 2018 as PD initiated 72 h after PD catheter insertion, whereas, initiation between 3 days and 14 days after catheter insertion was denoted early start PD. 13 Multiple studies have demonstrated that PD is a safe and efficient option for urgent-start KRT 14,15 and associated with improved preservation of kidney function, 16 quality of life and lower healthcare costs 17,18 compared to HD. However, outcome data comparing patients undergoing urgent-start PD or HD remain scarce.
Thus, the aim of this retrospective comparative study was to investigate patient and KRT modality-related outcomes in patients undergoing urgent-start PD or urgent-start HD in a tertiary care research hospital. Moreover, this is the first study to our knowledge to explore the CVC insertion rate and associated adverse outcomes in patients initiating urgent-start KRT.
Methods
This retrospective, single-centre, comparative study focused on comparing outcomes of patients initiating urgent-start PD or HD. Altogether, 319 patients initiated PD during the study time frame of 2005–2018. All patients starting PD within 72 h after PD catheter insertion during the study in Turku University Hospital Kidney Center were included, leading to an urgent-start PD cohort of 33 patients.
Next, all patients initiating urgent-start HD (initiation of HD using a CVC within 24 h after insertion) with a CVC along with KRT initiation dates during the same time period were collected from the electronic patient records comprising 222 patients. With an objective of 1:2 matching ratio one or two urgent-start HD controls treated in the intensive care unit (ICU) or Kidney Center of the research hospital from the same time period were manually selected for each of the PD patients blinded for other clinical details and for outcome data of the assessed patients. The urgent-start HD control patients were matched with the urgent-start PD patients by the aetiology of CKD and age (± 5 years). The list of potential urgent-start HD patient match candidates was first screened only for age at the time of KRT initiation and second for CKD aetiology at the earliest mention to find an eligible match for each urgent-start PD patient. For six urgent-start PD patients, however, only one matching urgent-start HD patient was found out of the potential urgent-start HD patients within the research time frame, resulting in a matching ratio of 1:1-2. After the exclusion of 164 matching candidates, an urgent-start HD patient cohort of 58 patients for the urgent-start PD patients was selected. The exclusion criteria for the study included age under 18 years, KRT initiation due to AKI or presence of AKI at the start of KRT, ongoing maintenance KRT and/or a previously prepared vascular access (arteriovenous fistula or graft or a tunnelled catheter).
Patient demographics, disease history, medications, KRT and PD or HD catheter insertion data were manually extracted from the electronic patient records of the research hospital.
KRT initiation criteria and modalities
Urgent-start KRT was initiated according to the Kidney Disease Improving Global Outcomes guidelines criteria including severe refractory hyperkalaemia (potassium ≥6 mmol/L) or metabolic acidosis (pH ≤7.2 or bicarbonate ≤12 mmol/L) or volume overload (dyspnoea in the presence of oliguria, severe swellings and thoracic X-ray findings consistent with pulmonary fluid congestion confirmed by the attending radiologist). 19 Furthermore, prompt uncontrolled uremic symptoms such as nausea, fatigue or loss of appetite were considered acceptable criteria for KRT initiation. The primary reason for KRT initiation was collected and categorised into two groups: KRT start due to volume overload or metabolic/uremic (hyperkalaemia, metabolic acidosis or uremic symptoms) disturbances.
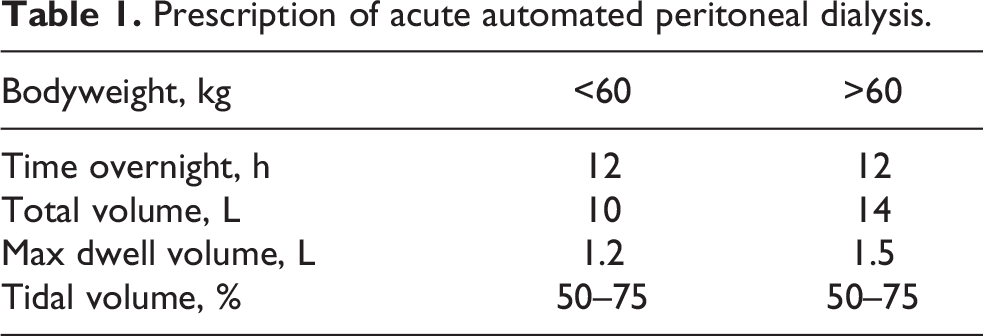
PD catheters were implanted by mini-laparotomy, and fluid flow was tested perioperatively. All PD patients received preoperative oral cephalexin for infection prophylaxis. All operations were performed in an operating room, and strict hygiene standards were followed. Both continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis (APD) were applied as needed. Acute APD programme was performed according to a protocol described by Povlsen and Ivarsen 20 (Table 1). Urgent-start CAPD was initiated by using reduced volume nightly icodextrin solution as a monotherapy or in addition to daytime dwells with glucose-based PD fluids. All the urgent-start PD patients were hospitalised at the time of KRT initiation for careful monitoring and patient education.
Prescription of acute automated peritoneal dialysis.
CVCs for urgent-start HD were operated by anaesthesiologist, and all operations were performed in an operation room or post-anaesthesia care unit. Surgery-level hygiene standards were followed. Urgent-start HD was performed via a tunnelled or non-tunnelled CVC with 2.5–5 h treatment duration, blood flow rates 170–250 mL/min and dialysate flow rate of 500 mL/min. Low-molecular-weight heparin anticoagulation was dosed depending on the clinical condition of the patient and the running number of the HD treatment.
The choice of KRT modality was left at the discretion of the attending clinician.
Outcome measures and definitions
Primary outcomes of the study were patient survival at 3 and at 12 months of follow-up. Secondary study outcomes included cumulative first-year hospital care days, PD modality survival (defined as not switching to another modality from the initial urgent-start KRT modality throughout the follow-up) and KRT-related infectious complications (PD or HD catheter exit-site infection (ESI), PD associated peritonitis or blood culture-positive bacteraemia) at 3-month and 12-month follow-up. PD peritonitis and blood culture-positive bacteraemia were denoted as severe KRT-related infections.
PD ESI and PD peritonitis were defined according to the International Society for Peritoneal Dialysis guidelines (Online Supplementary Material). 21 Blood culture-positive bacteraemia was denoted as bacterial growth in the blood culture with coincident clinical signs of infection. Severe KRT-related infection was defined as the occurrence of blood culture-positive bacteraemia or PD peritonitis and KRT-related ESI as the occurrence of PD ESI or HD ESI. Any KRT-related infection was defined as any of the following: PD peritonitis, blood culture-positive bacteraemia, PD ESI or HD ESI.
PD catheter and CVC insertion rates were defined as cumulative total number of respective insertions performed.
Ethics
All studies were in accordance with the ethical standards of the institutional and/or national research committee at which the studies were conducted and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The study received approval (reference number T138/2016) from the Medical Ethics Committee of the Hospital District of Southwest Finland. Due to the observational nature of the registry study, informed consent was not required.
Statistics
Categorical variables were summarised with counts and percentages and continuous variables with mean or median (inter-quartile range, IQR) or range (minimum and maximum). The normality in continuous variables was tested with the Kolmogorov–Smirnov and Shapiro–Wilk tests.
The groups (urgent-start PD versus urgent-start HD) were compared with one-way analysis of variance (continuous variables) or Fisher’s exact test (categorical variables). Logarithmic transformation was performed to C-reactive protein (CRP), creatinine and estimated glomerular filtration rate (eGFR) to achieve assumptions of normality. Normality assumption was checked with studentised residuals.
Cumulative first-year hospital care days were compared between the groups using the Wilcoxon rank-sum test. Hospital care days between number of CVC insertions were compared with the Kruskal–Wallis test. Association between hospitalisation days (ln transformed) and CRP (ln transformed) and albumin was analysed using linear regression model.
Furthermore, the association between survival over 1 year and hospitalisation days was tested using Cox’s proportional hazard model. Patient survival between urgent-start PD and HD patients was explored with the log-rank test (illustrated with a Kaplan–Meier plot) and further with Cox’s proportional hazards model. All Cox’s proportional hazard analyses were further explored with multivariable adjustment by including sex and Charlson Comorbidity Index (CCI) as covariates. Furthermore, a sensitivity analysis was performed regarding the association between 12-month survival and hospitalisation days by excluding the patients (n = 8 (9%)) that perished during the first 14 days of care from the univariate Cox proportional hazards analysis.
p Values less than 0.05 (two-tailed) were considered as statistically significant. The analyses for this paper were performed using SAS software, version 9.4, of the SAS System for Windows (SAS Institute Inc., Cary, North Carolina, USA) and IBM SPSS Statistics software version 26.0 (IBM SPSS Inc., Armonk, NY, USA) as appropriate.
Results
Baseline and KRT characteristics
Altogether 33 urgent-start PD patients and 58 urgent-start HD patients were included in the study. Baseline characteristics of the patients are presented in Table 2. The patients were matched according to the CKD aetiology and age (mean difference between urgent-start PD patients and urgent-start HD controls was 3.4 years). Furthermore, no significant differences between the study groups in relation to CCI, sex, body mass index or eGFR at the time of KRT initiation were observed (Table 2). Mean age of the patients was 60 (range 26–89) years, 77% were male and the primary cause of CKD was diabetes in 60 (66%) patients. The description of baseline characteristics and 12-month survival in the included and excluded urgent-start HD patients are summarised in Online Supplemental Table S1.
Baseline characteristics of the study patients and pre-dialysis programme, late referral and primary reason for urgent-start KRT.a
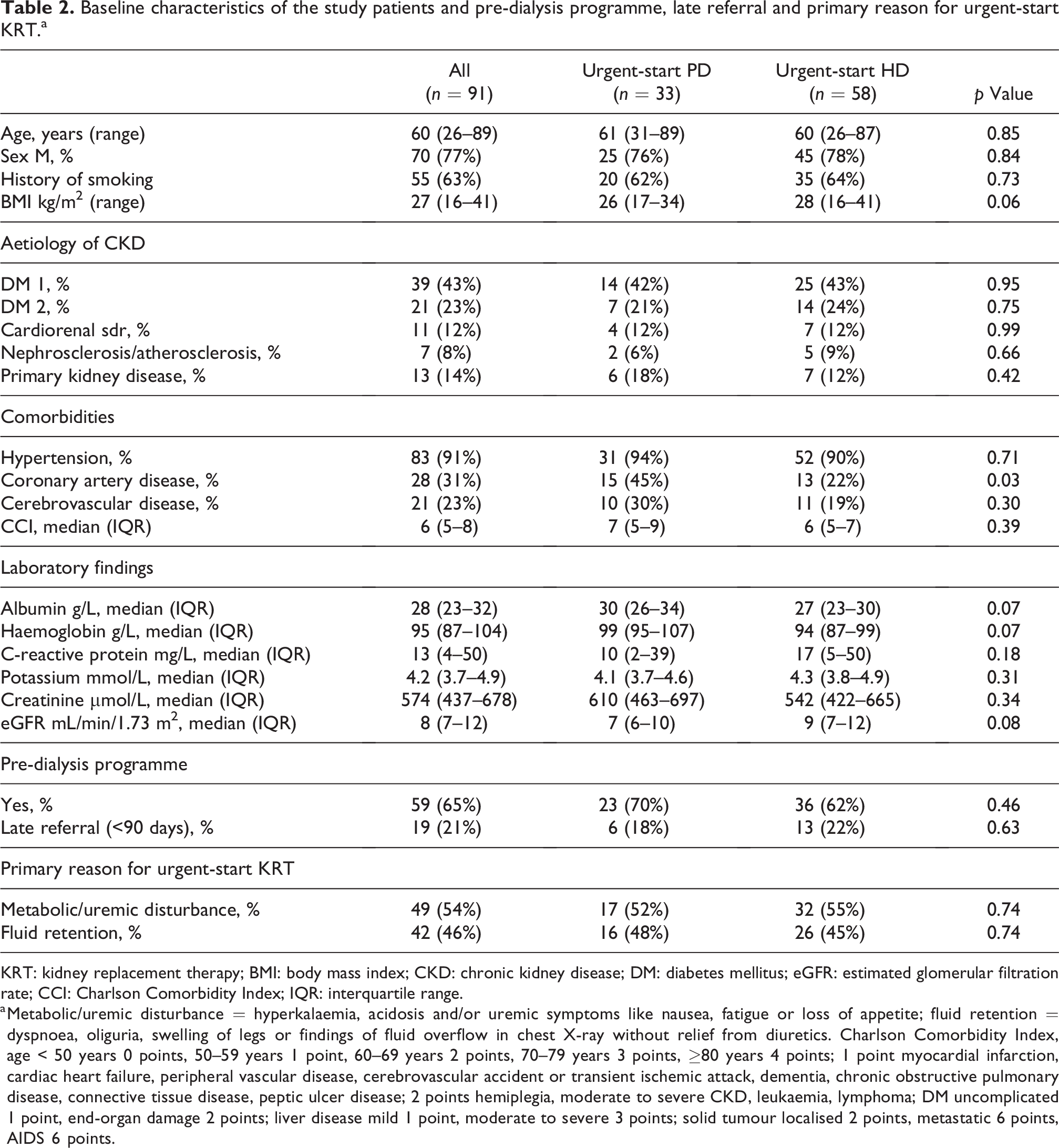
KRT: kidney replacement therapy; BMI: body mass index; CKD: chronic kidney disease; DM: diabetes mellitus; eGFR: estimated glomerular filtration rate; CCI: Charlson Comorbidity Index; IQR: interquartile range.
a Metabolic/uremic disturbance = hyperkalaemia, acidosis and/or uremic symptoms like nausea, fatigue or loss of appetite; fluid retention = dyspnoea, oliguria, swelling of legs or findings of fluid overflow in chest X-ray without relief from diuretics. Charlson Comorbidity Index, age < 50 years 0 points, 50–59 years 1 point, 60–69 years 2 points, 70–79 years 3 points, ≥80 years 4 points; 1 point myocardial infarction, cardiac heart failure, peripheral vascular disease, cerebrovascular accident or transient ischemic attack, dementia, chronic obstructive pulmonary disease, connective tissue disease, peptic ulcer disease; 2 points hemiplegia, moderate to severe CKD, leukaemia, lymphoma; DM uncomplicated 1 point, end-organ damage 2 points; liver disease mild 1 point, moderate to severe 3 points; solid tumour localised 2 points, metastatic 6 points, AIDS 6 points.
In the urgent-start PD group, APD was started in 28 (85%) and CAPD in five (15%) patients, and the initial vascular access in the urgent-start HD group was a non-tunnelled CVC in 41 (71%) and a tunnelled CVC in 17 (29%) patients. The median time for starting PD after catheter insertion was 0 days (IQR 0–1 days). Urgent-start HD was initiated in the ICU for 7 (12%) patients.
Primary and KRT modality outcomes
Patient flow, switches between KRT modalities, mortality and transplantations at different time points during follow-up are depicted in Figure 1. Altogether, 26 patients (29%) died within the 12-month follow-up. There were no differences in patient survival in patients receiving urgent-start PD compared to urgent-start HD at 3 months (hazard ratio (HR): 1.15, 95% CI: 0.35–3.81, p = 0.82) or at 1 year of follow-up (HR: 0.64, 95% CI: 0.30–1.39, p = 0.26) in Cox proportional hazards analysis, and the results did not change when the analyses were adjusted by sex, and CCI as covariates (HR: 1.55 95% CI: 0.45–5.27, p = 0.49 (3-month follow-up] and HR: 0.73, 95% CI: 0.33–1.58, p = 0.42 (12-month follow-up)).
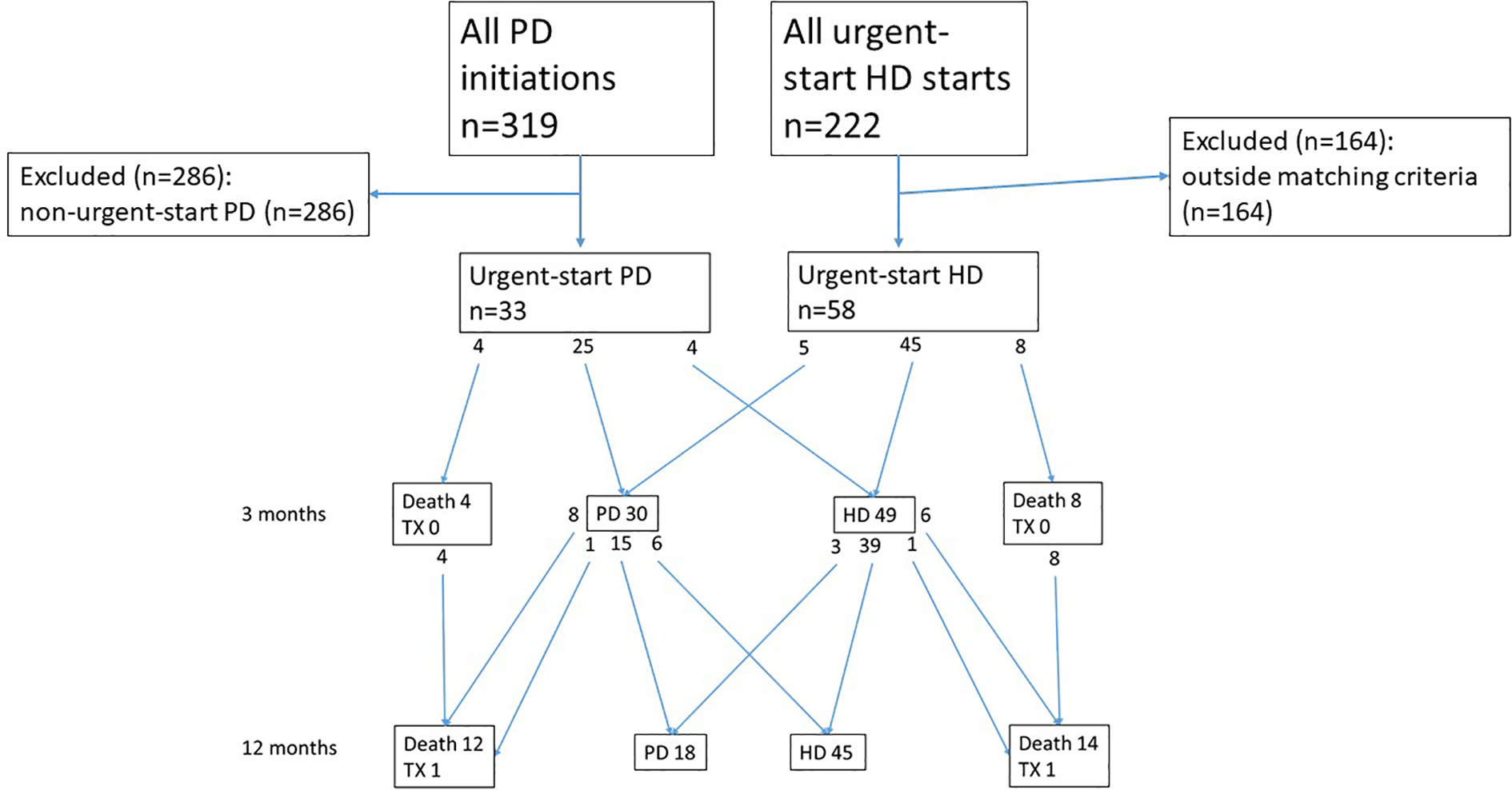
Patient flow, switches between modalities, mortality and transplantations throughout the study.
Out of the baseline characteristics older age (HR: 1.04, 95% CI: 1.01–1.07, p = 0.01) and higher CCI (HR: 1.39, 95% CI: 1.12–1.72, p < 0.01) were associated with mortality at 1-year follow-up in univariate Cox proportional hazards analyses. The cause of death was cardiovascular in 19 (73% of the deceased), infection in six (23%) and malignancy in one patient (4%).
At 3-month follow-up, 25 (76%) and 45 (78%) patients initiating urgent-start PD or urgent-start HD had persisted with the initial KRT modality, and there was no difference between the groups (p = 0.72). The corresponding numbers at 1-year follow-up were 15 (45%) and 40 (69%) for the urgent-start PD and HD groups, respectively, and no difference between the groups was observed (p = 0.07).
Infectious complications and cumulative first-year hospital care days
Altogether, 11 (33%) and 19 (58%) patients in the urgent-start PD group and 25 (43%) and 38 (66%) in the urgent-start HD group were observed with at least one KRT-related infection (PD or HD ESI or PD peritonitis or blood culture-positive bacteraemia) at 3 months or 12 months of follow-up, respectively, and no difference between the study groups was observed (p > 0.30 for both comparisons).
There was a difference in the rate of blood culture-positive bacteraemia (3 (9%) vs. 22 (38%)), PD peritonitis (8 (24%) vs. 3 (5%)), PD ESI (15 (45%) vs. 3 (5%)) and HD ESI (2 (6%) vs. 21 (36%)) between urgent-start PD and urgent-start HD groups at 12-month follow-up, respectively (p < 0.05 for all comparisons). However, there was no difference in the occurrence of severe KRT-related infections (10 (30%) vs. 24 (41%), p = 0.37) or KRT-related ESIs (16 (48%) vs. 24 (41%), p = 0.52) between urgent-start PD and urgent-start HD patients at 12-month follow-up. Finally, the total number of patients with any KRT-related infections was 18 (55%) and 35 (60%) in the urgent-start PD and HD groups (p = 0.66), respectively (Table 3). Numerical data on the total number of KRT-related infections reported as total counts and counts per patient year are summarised in Table 3.
Number of patients with KRT-related infections or PD leaks and cumulative total number of KRT-related infections reported as counts and per patient year.a
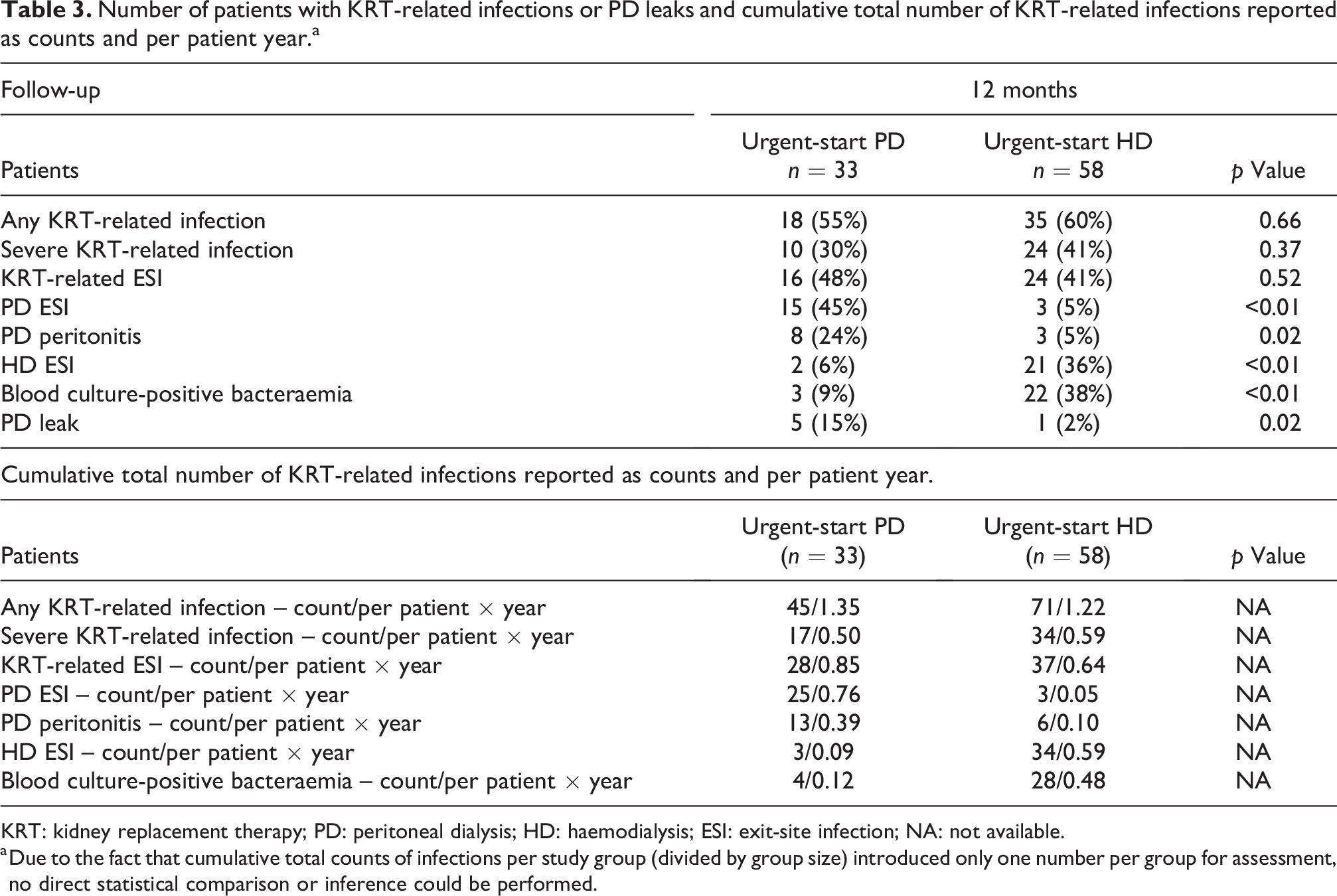
KRT: kidney replacement therapy; PD: peritoneal dialysis; HD: haemodialysis; ESI: exit-site infection; NA: not available.
a Due to the fact that cumulative total counts of infections per study group (divided by group size) introduced only one number per group for assessment, no direct statistical comparison or inference could be performed.
Median time to first any KRT-related infection was 62 (range 7–262) days in the urgent-start PD group and 52 (range 0–298) days in the urgent-start HD group, and there was no difference between the groups (p = 0.76).
None of the infection outcomes were associated with mortality at 3-month follow-up. No association between severe KRT-related infection or PD ESI, and mortality was detected at 12-month follow-up. However, the occurrence of HD ESI (p < 0.01) and KRT-related ESI (p < 0.01) were inversely associated with mortality at 12-month follow-up.
The cumulative hospitalisation care days for both study groups are depicted in Figure 2. No differences were observed in the cumulative hospital care days between the study groups at 3 months (p = 0.91) or 1 year of follow-up (p = 0.43) (Figure 2).
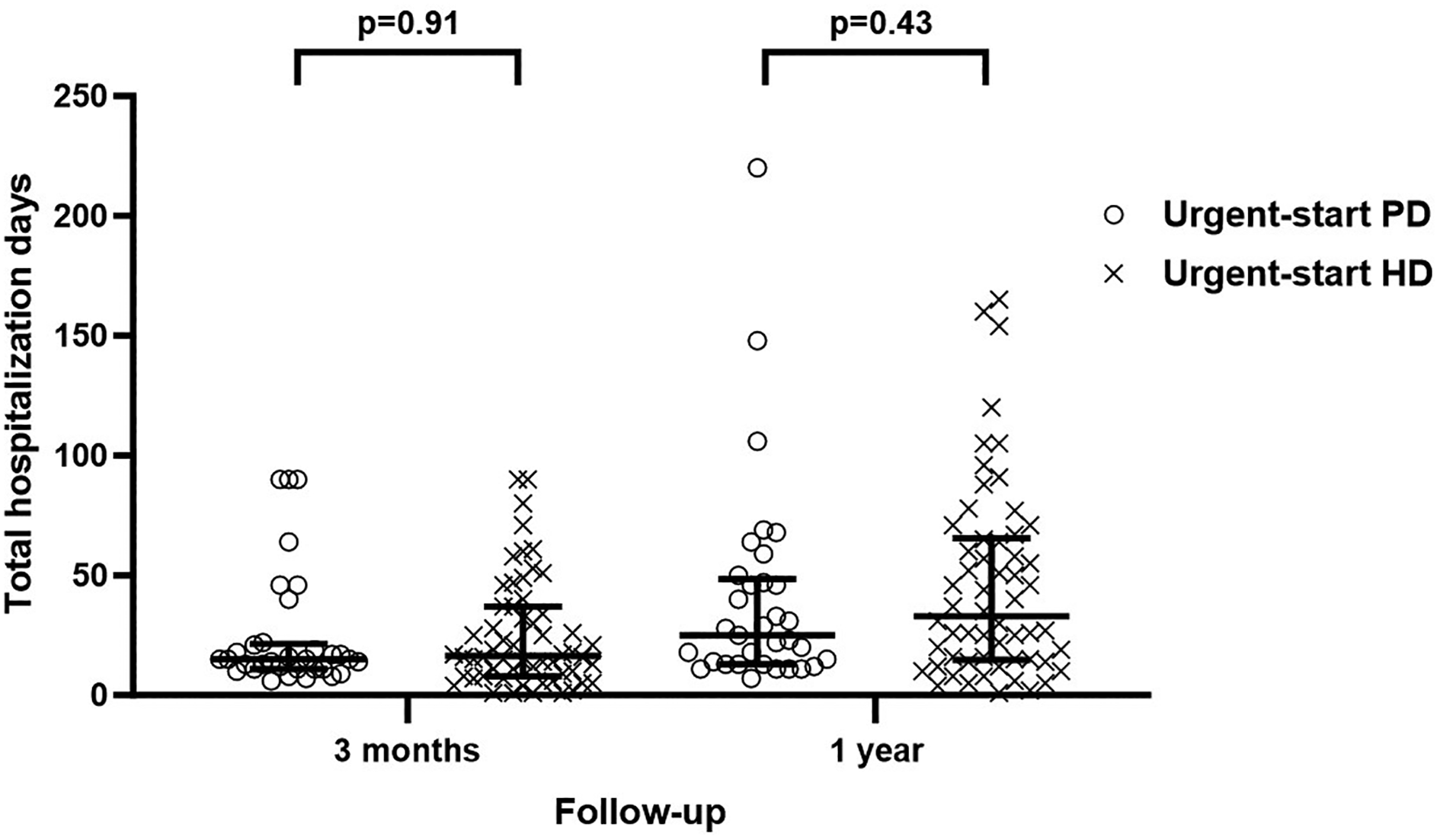
Hospital care in days in the urgent-start PD and HD group at 3 months and 12 months of the follow-up.
Baseline CRP was positively (p = 0.05) and albumin inversely (p = 0.01) associated with cumulative first-year hospital care days in univariate linear regression analyses.
Total cumulative first-year hospital care days were not associated with mortality during the 12 months of follow-up (HR: 0.99, 95% CI: 0.99–1.01, p = 0.44) in univariate Cox proportional hazards analysis. The results did not change in a sensitivity analysis excluding patients (n = 8 (9%)) that perished during the first 14 days of care (p = 0.13) or in a multivariable Cox model adjusted for sex and CCI in the whole cohort (HR: 0.99, 95% CI: 0.98–1.00, p = 0.12).
PD and CVC catheter insertions and associated outcomes
Altogether, 44 PD catheters were inserted in the study cohort including five catheters for five patients in the urgent-start HD group who switched to PD during the 12-month follow-up. Out of the 44 PD catheters, 6 were re-insertions in the urgent-start PD group. The PD catheter insertion rate was not associated with any of the measured outcomes in the study. PD leaks were infrequent, and no difference in the occurrence of PD leaks was observed between the groups (Table 3).
In total, 139 CVCs were inserted in the study cohort, and 7 patients in the urgent-start PD group received a total of 16 CVCs within the 12-month follow-up. Furthermore, the amount of CVC re-insertions was 65 in the urgent-start HD group. The total number of CVC insertions was not associated with mortality at 3 months (p = 0.10), whereas an inverse association between CVC insertions and mortality at 12-month (p = 0.02) follow-up was observed. The results remained similar in a separate analysis assessing the effect of late CVC re-insertions on mortality when the patients (n = 8 (9%)) who died within the first 14 days of follow-up were excluded from the analyses (data not shown).
The number of CVC insertions was positively associated with the risk of blood culture-positive bacteraemia (p < 0.01), severe KRT-related infection (p < 0.01) and the risk of HD ESI (p < 0.01) at 12-month follow-up. The number of CVC insertions was not associated with the risk of PD peritonitis (p = 0.67), KRT-related ESI (p = 0.09) or PD ESI (p = 0.13).
The CVC insertions rate was positively but non-linearly associated with cumulative hospital days at 3-month follow-up (p = 0.04) and 1-year follow-up (p < 0.01). The mean cumulative hospital days in patients receiving only one CVC was 38 and 36 days, whereas the patients who received 5 CVCs were admitted for a mean of 68 and 81 days at 3 months and 1-year follow-up for the urgent-start PD and HD group, respectively.
Discussion
In this retrospective comparative study exploring clinical outcomes in patients initiating urgent-start KRT, we demonstrated comparable patient survival, cumulative first-year hospital care days and total KRT-related infection rate at 3 months and 1-year follow-up between urgent-start PD and urgent-start HD. However, the number of CVC insertions in patients initiating urgent-start HD was eight-fold compared to urgent-start PD patients, and the number of CVC insertions was associated with the risk of blood culture-positive bacteraemia and HD ESI as well as increased cumulative fist-year hospital care days.
Patient survival was similar in patients receiving urgent-start PD or HD in our study, and our results are in line with prior data. Mortality in urgent-start PD and HD patients has ranged between 30% and –42% at 6 months and 17% and 21% at 12-month follow-up in prior studies. 22,23 However, the definition of urgent-start PD in prior studies has varied extensively and been in contrast with the previously established and widely accepted criteria employed in our study, making thereby comparison with our current results difficult. 13 Dias et al. 24 compared 93 patients receiving urgent-start PD initiated according to established criteria (PD initiation within 72 h of PD catheter insertion) by Blake et al. 13 with 91 urgent-start HD patients in a similar setting to our study. Total 1-year mortality was 24.4%, a slightly lower rate than in our study, and 19% of patients receiving urgent-start PD and 30% of those receiving urgent-start HD had deceased at 1-year follow-up. Total patient survival time was comparable between the study groups similar to our results. The numerically higher 1-year mortality in our study might be partly explained by the higher prevalence of diabetes as two-thirds of patients had diabetic kidney disease (DKD) while DKD was observed in one-third of the patients in the study by Dias et al. 24 Moreover, the indication for KRT initiation was fluid retention in every fourth patient in the report by Dias et al., while half of the patients in our study were observed with severe fluid retention at the start of KRT, possibly explaining excess mortality. 24 –26
We observed no association between total or severe KRT-related infection rate or cumulative first-year hospital care days and mortality. However, a lower rate of HD ESIs or CVC insertions were associated with a higher risk of death in this study. This might be explained by selection bias as patients who perished early after KRT initiation had less time and, thus fewer opportunities for CVC insertions and therefore less HD ESIs. In prior studies age, 22 low serum potassium and albumin 27 have been associated with mortality in urgent-start PD and HD patients. In the large study by Dias et al., higher age, CCI, baseline eGFR and lower baseline plasma albumin and haemoglobin as well as KRT-related ESIs were associated with mortality. 24 Older age and higher CCI were associated with mortality in our study, whereas any of the tested laboratory parameters were not. Altogether, our findings are in line with prior studies in relation to mortality and associated variables.
By the end of follow-up, over half of the patients receiving urgent-start PD or HD were observed with at least one KRT-related infection, and there were no differences between the study groups. Furthermore, there were no differences in the combined severe KRT-related infection or ESI rate between the KRT modalities. However, the risk of blood culture-positive bacteraemia, the KRT-related infection with the worst prognosis, 28 was markedly higher in urgent-start HD patients compared to urgent-start PD patients. This is probably explained by the higher number of CVC insertions in the urgent-start HD patients, as CVC insertions were associated with the risk of blood culture-positive bacteraemia in our study, and similar associations have been observed in previous studies. 11,29 Furthermore, Jin et al. 27 observed that 3.1% in urgent-start PD and 13.4% in urgent-start HD patients developed bacteraemia within the first 30 days after catheter insertion. Moreover, Dias et al. reported catheter-related bacteraemia in 7.5% and 24.1% of patients receiving urgent-start PD and HD, respectively, at 1-year follow-up. 24 The blood culture-positive bacteraemia rate in our study appears to be higher than in prior studies. 22 We hypothesise that this observation results from the high prevalence of factors previously shown to be associated with the risk of blood culture-positive bacteraemia and CVC-related ESIs such as diabetes, atherosclerotic disease and dialysis start as an inpatient as in our cohort. 30,31
Our study is the first to assess the total number of first-year CVC insertions in patients initiating urgent-start PD or HD. The CVC insertion rate was considerably high. As we observed an association between CVC insertions and the risk of blood culture-positive bacteraemia, the high number of CVCs possibly explains the high blood culture-positive bacteraemia rate in our study. Despite the fact that total KRT-related infection rate was similar between the study groups, it might be reasonable to favour urgent-start PD over HD in some patients at increased risk for infection, as bacteraemia rate in these patients appears lower and blood culture-positive bacteraemia is associated with poorer patient outcomes than other KRT-related infections. 11,32 Furthermore, CVC insertion rate was positively associated with cumulative first-year hospital care days in this study. However, patients initiating urgent-start HD did not have a higher cumulative first-year hospital care days compared to urgent-start PD patients (Figure 2), and this finding was in line with Dias et al. 24 A possible explanation is the fact that patient initiating urgent-start PD were all hospitalised at the beginning of treatment balancing the excess admissions associated with CVC insertions, as each CVC insertion was performed in the research hospital. Nevertheless, Karpinski et al. demonstrated a 24% lower rate of hospitalisation in urgent-start PD patients compared to those initiating urgent-start HD via a CVC. 33 Importantly, the on-going global shortage of hospital beds and experienced nurses underscore the need to avoid needless hospitalisations. 34 The initiation of urgent-start PD is somewhat more laborious and requires set special protocols and keen communications within and outside the nephrology clinic to yield favourable outcomes compared to the more commonly practiced urgent-start HD. The identification of suitable patients is also crucial and can prove difficult in the setting of severe illness and associated kidney dysfunction. Typically, the initiation of urgent-start PD is not reasonable in critically ill and severely hemodynamically unstable patients, and recent intra-abdominal surgery is a common contraindication. Nevertheless, the favouring of PD as the urgent-start KRT modality in suitable patients may enhance the adoption of home dialysis, leading to decreased utilisation of hospital resources and facilities, lower healthcare costs as well as improved quality of life compared to in-centre HD. 18,35
The rate of PD peritonitis was in line with prior data, 23,36 and half of the urgent-start PD patients were observed with a PD ESI at 1 year of the follow-up. Diabetes and poor glycaemic control are known risk factors for PD ESI, and DKD was the most common aetiology of CKD in our study. 37 None of the PD-related infections were associated with patient outcomes in this study. Furthermore, urgent-start PD has been associated with the need for fewer dialysis access-related procedures than urgent-start HD patients. 38 Fewer procedures are associated with lower healthcare costs, 18,39 improved quality of life and intuitively fewer infections as suggested in our study.
Limitations
This study has all the limitations of a retrospective study. The sample size was somewhat limited, and the retrospective comparative setting could be at risk for selection bias. Furthermore, not all urgent-start PD patients were able to be matched in a 1:2 ratio with an eligible urgent-start HD match, and the matching criteria may have left room for bias. Thus, only groupwise comparisons in place of matched pairs analyses could be performed. However, all the patients were extensively studied, and the urgent-start PD and HD patients were carefully matched with no difference in the baseline characteristics. Furthermore, during the control selection process, the HD control candidates were blinded for other clinical and outcome data of the assessed patients. Moreover, there was no difference in the 12-month survival of baseline comorbidities between included and excluded urgent-start HD patients. Nevertheless, the risk of some residual confounding has to be taken into account when interpreting the results of the present article. Compared to most prior studies, urgent-start PD was performed according to commonly accepted established criteria. 13 Our current study is the first to carefully measure the CVC insertion rate and demonstrate the associations between the number of CVC insertions and patient outcomes in the urgent-start KRT setting. Despite the structural limitations of this study, our findings are intuitive and plausible, and we believe these data can help guide future research.
Conclusions
In this study, we demonstrate comparable patient survival, cumulative first-year hospital care days and total KRT-related infection rate at 3 months and 1-year follow-up in patients initiating urgent-start PD and urgent-start HD. Furthermore, our data show that the number of CVC insertions during the first year after urgently initiated KRT is associated with the risk of blood culture-positive bacteraemia and increased cumulative hospitalisation days.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608241244939 - Survival, cumulative hospital days and infectious complications in urgent-start PD compared with urgent-start HD
Supplemental Material, sj-docx-1-ptd-10.1177_08968608241244939 for Survival, cumulative hospital days and infectious complications in urgent-start PD compared with urgent-start HD by Jonna Virtanen, Maija Heiro, Niina Koivuviita, Eliisa Löyttyniemi, Mikko J Järvisalo, Risto Tertti, Kaj Metsärinne and Tapio Hellman in Peritoneal Dialysis International
Footnotes
Acknowledgement
None.
Author contributions
JV, MH, NK, MJJ, RT and KM designed the study, and JV and MH were responsible for the data collection. EL and TH performed the statistical analysis. JV drafted the manuscript. JV, MH, NK, EL, MJJ, RT, KM and TH revised the manuscript.
Data availability statement
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study received approval (reference number T138/2016) from the Medical Ethics Committee of the Hospital District of Southwest Finland.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Finska Läkaresällskapet and the Perklén Foundation, Helsinki, Finland.
Informed consent
None.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.