
Abstract
Peritoneal dialysis (PD) patients have higher hospitalisation rates than the general population. The hospitalisations are not always related to dialysis issues, and physicians with little or no experience with PD may be responsible for the care of these hospitalised patients. Furthermore, the hospital may not be familiar with or equipped to manage these patients. This review highlights barriers, knowledge gaps and management strategies to guide the care of hospitalised PD patients.
Keywords
Take-home points
Antibiotic prophylaxis is suggested before endoscopy and invasive gynecologic procedures, and these procedures should be carried out without PD fluid in situ. Intraperitoneal antibiotics to treat systemic/extra-abdominal infections can be considered. Although cloudy peritoneal fluid is common in PD-associated peritonitis, broader aetiologies should be entertained. Radiocontrast can be administered cautiously in hospitalised PD patients, if necessary, without significantly affecting residual kidney function. The PD patient undergoing cardiac surgery or hernia repair does not necessarily have to be converted to haemodialysis in the peri-operative period.
Case vignette
Mr F is an 84-year-old man with end-stage kidney disease (ESKD) secondary to ischemic nephropathy. The patient had a peritoneal dialysis (PD) catheter inserted laparoscopically and then he and his wife were trained to perform cycler PD at home. Unfortunately, after 2 years on therapy, he presented to another hospital with acute coronary syndrome, and the decision was made that he needed to undergo surgical coronary revascularisation. The cardiovascular surgeon requested that he be pre-emptively changed to haemodialysis (HD). The nephrology consult service at that hospital agreed and arranged for a central venous catheter (CVC) insertion. On post-op day 3, he developed fever and peripheral leukocytosis. Blood cultures from the CVC demonstrated Serratia marcescens. Mr F had no abdominal pain or tenderness. One litre of dialysate was infused into the peritoneal cavity and dwelled for 4 h. The PD fluid was clear with a normal cell count, but cultures demonstrated S marcescens. The care team assumed this was PD peritonitis, and the PD catheter was removed. As the case above illustrates, patients on PD may come under the care of physicians with little knowledge of this therapy. The patient developed a bloodstream infection that may have resulted from the (unnecessary) placement of the HD catheter. The bacterium entered the peritoneal cavity but did not lead to peritonitis. Mr F. ended up losing his PD catheter unnecessarily.
We will describe some common clinical scenarios where it is important to anticipate that there may be errors or omissions in the management of hospitalised PD patients.
How to prepare for procedures in hospitalised PD patients?
It is essential that the peritoneal cavity is empty of dialysate before the procedure and that phosphate-containing enemas in the bowel preparation for endoscopic procedures are avoided. The use of polyethylene glycol and bisacodyl is advised. 1 In addition, prophylactic antibiotics before the procedure are recommended to diminish the chance of peritonitis. PD patients are at high risk for PD-related peritonitis due to the PD catheter in their abdominal cavity 2 and the ongoing infusion of dialysis fluid with its intrinsic risk of bacterial contamination. PD-peritonitis is a major cause of the transition to intermittent HD 3 and a risk factor for increased mortality. 3
Sources of PD-related peritonitis include trans-visceral migration from the gastrointestinal tract, or genitourinary tract, and haematogenous dissemination in the face of bacteraemia, which may occur during some procedures (as in the patient described above). 2 Prevention of PD-related peritonitis using prophylactic antibiotics during high-risk procedures is one of the strategies that the International Society of Peritoneal Dialysis (ISPD) has suggested. 4 Gastrointestinal procedures, including upper endoscopy and colonoscopy, are potential sources of PD-peritonitis. There is growing literature that colonoscopy increases the risk of peritonitis in the PD population. 5,6 Mucosal disruption and subsequent seeding of the bacteria to the peritoneum is the most frequently proposed mechanism. 6 The most frequent culprit organisms cultured from the peritoneal fluid are from the Enterobacteriaceae family, especially E coli. 7 Nonetheless, in response to the increased risk of peritonitis after colonoscopy, the ISPD recommends prophylactic antibiotics for any PD patient prior to undergoing a colonoscopy without recommending a specific antibiotic choice but cites a single dose of IV ampicillin or oral amoxicillin plus an aminoglycoside, with or without metronidazole, as a potential regimen to cover most culprit organisms. 4 In contrast to colonoscopy, upper endoscopy has limited available data to support the benefits of prophylactic antibiotics. Wu et al. found that upper endoscopies had significantly lower rates of peritonitis compared to other types of endoscopic procedures in PD patients. 8 Another recent retrospective observational study showed peritonitis post gastroscopy is not rare with an incidence of 4%. 9 And the common bacteria were polymicrobial, predominantly gram-negative organisms, similar to lower colonscopy. 7 One-quarter of the reported peritonitis had microorganisms that arise from oral cavity such as streptococci viridians and B-haemolytic streptococci. 10,11 Older age and biopsy during the procedure were associated with higher risk of PD-peritonitis. However, antibiotics pre procedure was associated with a lower incidence of PD-peritonitis. 12 We conclude that PD patients may benefit from prophylactic antibiotics prior to upper endoscopy similar to colonoscopy as illustrated in Table 1, especially high-risk patients such as older patients and those who may need tissue biopsy.
Antibiotic prophylaxis and procedures in PD patients.
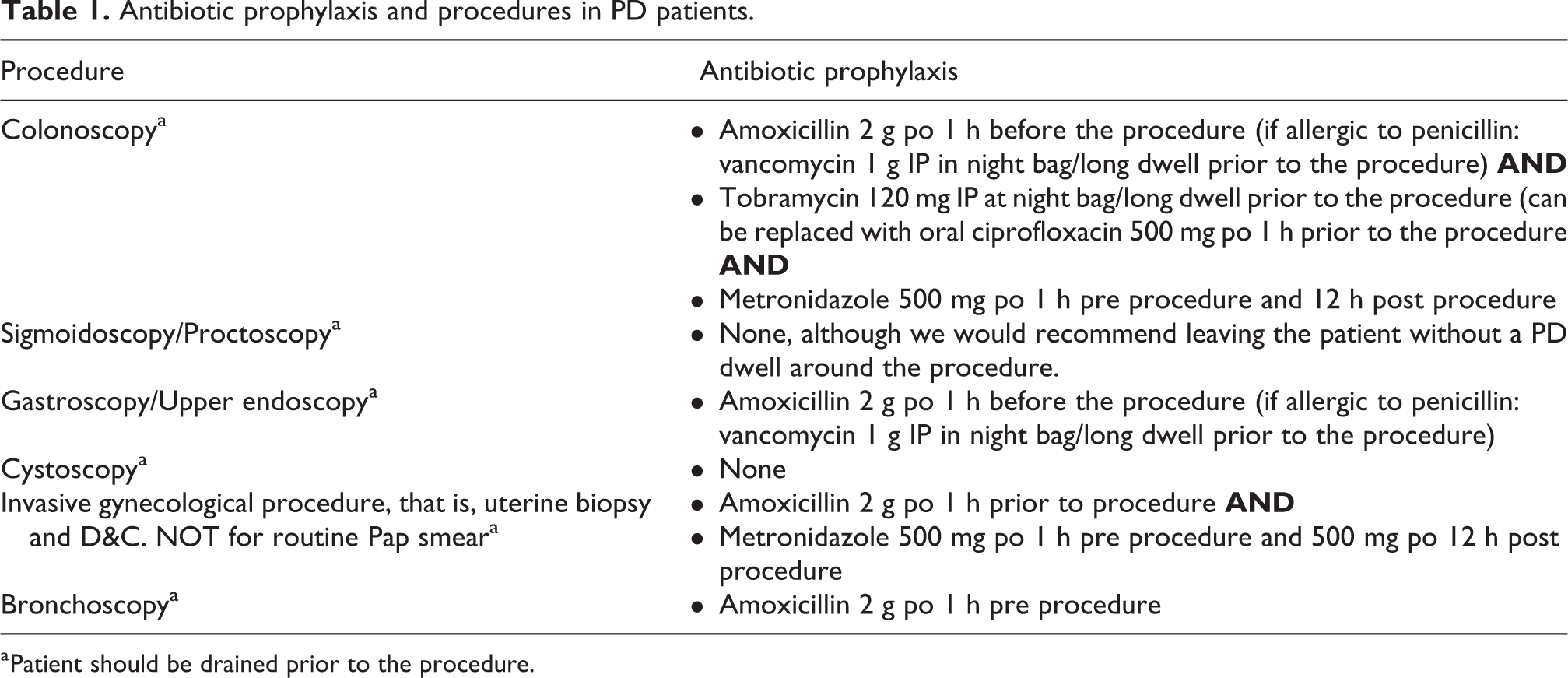
a Patient should be drained prior to the procedure.
Various genitourinary procedures have been reported to cause peritonitis, including cystoscopy, diagnostic hysteroscopies, endometrial polypectomies, endometrial curettages, cervical conizations, and both intrauterine device implantations and removal. 13,14 The most frequent reported organisms include gram-negative bacilli, enterococcus and streptococci. 15 Due to the concern for peritonitis, the ISPD 2022 guidelines recommend antibiotic prophylaxis in all patients undergoing invasive gynecologic procedures. They suggest the same antibiotic regimen as that for colonoscopies (Table 1). 4 We conclude that prophylactic antibiotics are needed prior to invasive gynecological procedures. This recommendation does not include Pap smears.
Why do we prescribe oral antifungal prophylaxis in the hospitalised PD patient who is on antibiotics?
Fungal peritonitis is a serious complication in patients on PD. 16 It accounts for 2–12% of all episodes of peritonitis, 17 and is associated with significant morbidity and mortality. 16 Therefore, prevention of fungal peritonitis is essential. Many hospitalised patients receive antibiotics that can alter the bowel flora and lead to the yeast overgrowth in the gastrointestinal tract. 18 Two randomised trials showed reduction of incidence of fungal peritonitis with antifungal prophylaxis. 19,20 Lo et al. studied the use of oral nystatin 500,000 units four times per day versus placebo during use of antibiotics, whatever the indication. 19 Restrepo et al. studied fluconazole 200 mg every 48 h versus placebo when patients were receiving antibiotics for peritonitis. 20 The 2022 ISPD guidelines recommend antifungal prophylaxis be co-prescribed whenever PD patients receive antibiotics, regardless of the indication. 4
Should we hold the PD temporarily in hospitalised PD patients who are admitted with colitis or any abdominal pathology?
In general, any patient with intra-abdominal infection/inflammation including pancreatitis, cholangitis, colitis and diverticulitis may be at increased risk of translocation of organisms across the bowel wall into the peritoneal cavity, which can lead to peritonitis. Early diagnosis and treatment to control the abdominal inflammation is critical. There are no data on whether holding PD temporarily decreases the risk of enteric peritonitis insofar as bacterial entry into an empty peritoneal cavity may be better dealt with by innate immune defences. 21 The decision of holding the PD temporarily should be based on multiple factors including the severity of the colitis, clinical stability, the metabolic derangement, volume status and the residual kidney function (RKF). If a patient has severe abdominal inflammation and adequate RKF, holding PD for as long as 72 h could be considered. Furthermore, in this clinical setting, the patient typically is not eating and drinking well and is also losing fluid and electrolytes through the GI tract. Holding the PD should not preclude the administration of IP antibiotics with dwell of 6 h if needed to treat the intra-abdominal infection/inflammation, followed by keeping the patient dry the rest of the day. Finally, because of altered pancreatic enzymes in PD patients, including interference with the amylase assay in patients using icodextrin, diagnosing pancreatitis is challenging and difficult to distinguish from peritonitis. 22 The treatment is the same as in patients who are not receiving PD.
Can we prescribe intraperitoneal antibiotics to treat systemic/extraperitoneal infections in hospitalised PD patients?
Intraperitoneal (IP) administration of antibiotic is the treatment of choice for peritonitis in PD patients. 23 Depending on the antibiotic pharmacokinetics and the permeability of the peritoneal membrane, significant plasma concentration of the antibiotics can be achieved with the IP administration. 24 –26 Successful treatment of pacemaker infection with IP administration of Daptomycin has been reported. 27 IP administration of antibiotics may present a feasible route of antibiotic administration. This route would obviate the need for a peripherally inserted central catheter (PICC) line with its own attendant risk of bacteraemia, especially in infections needing a long course of antibiotics such as osteomyelitis and infective endocarditis. Measurement of serum concentrations and dose adjustments to maintain therapeutic, non-toxic concentrations is possible and meaningful in this context. Also, some patients may have significant gastrointestinal intolerance to oral antibiotics, so the IP route is an attractive option. The major drawback is that blood levels of cephalosporins are not easily monitored, and if this class of agents is necessary (as opposed to, for example, vancomycin), the intravenous route may be necessary for serious infections such as endocarditis. We encourage the reader to consult the latest ISPD 2022 guidelines on the choice and dosing of IP antibiotics. 4
Is it safe to expose hospitalised PD patients to intravenous contrast or gadolinium? If so, what are the precautions?
RKF remains important in ESKD patients. 28 It contributes significantly on overall patient’s health, volume control, phosphate control and the clearance of middle molecules. 28 It has been observed that the presence of RKF in PD patients is associated with better survival, nutritional status and quality of life. 29 The data about the toxicity of intravenous contrast and its effect on the RKF are conflicting. 30,31 In a cohort of PD patients, contrast exposure did not adversely affect the RKF after 1 month. 31 We recommend using a different diagnostic study, if possible, to avoid exposure to radiocontrast dye. However, if another option is not feasible, the contrast should be used cautiously, and consideration should be given to preventive measures before contrast exposure. The preventive measures include volume expansion, 32 N-acetyl cysteine 33 and the use of iso-osmolar contrast at the lowest possible dose. Although the evidence of the benefit of prophylactic N-acetyl cysteine is inconsistent, we still use it as it has little intrinsic risk compared to the significant adverse impact of losing RKF. However, this practice may have a burden on nursing care, and it may delay an urgent procedure requiring contrast. Moreover, the PD prescription can be adjusted as needed to ensure that patient is euvolaemic pre contrast and not volume depleted. Otherwise, there is no evidence for adjusting the PD prescription just to dialyse the contrast.
Regarding the safety of exposure to gadolinium, it had been reported that dialysis patients who were exposed to the older magnetic resonance gadolinium agents had a 3–7% risk of gadolinium-associated nephrogenic systemic fibrosis (NSF). 34 With the newer gadolinium agents, the risk of NSF is exceedingly low and there is no evidence to support switching PD patients to HD to avoid the low risk of NSF. 35
Cloudy PD fluid in hospitalised PD patients is not always infection, so what does it mean?
The most common cause of cloudy peritoneal dialysate is infectious peritonitis. 36 However, this diagnosis is established by the presence of two of the following: Clinical features consistent with peritonitis such as abdominal pain or cloudy PD effluent, dialysis effluent white cell count >100 with >50% neutrophils, and positive dialysis effluent culture.
There are several non-infectious causes of cloudy peritoneal fluids need to be considered when the criteria of infectious peritonitis is not met. 37 Some of the causes are benign and resolve spontaneously, and others need prompt recognition and treatment. 37 One of benign causes of cloudy PD fluid commonly encountered in hospitalised PD patients is having the fluid left in the peritoneum for a day or two or that the fluid was sampled after a prolonged period of peritoneal rest or ‘dry’ abdomen. While the total peritoneal white count may be elevated, these are predominantly monocytes, the percentage of neutrophils in the fluid from a very long-dwelling dialysate or dry abdomen is small, certainly <50%. Another commonly encountered cause is a presumed allergy to medication such as antibiotics. 38 It usually resolves spontaneously with stopping the offending medication and in some cases may need antihistamine and prednisone. 39 Moreover, an eosinophilic reaction to the PD catheter has been reported and is not rare. 40,41 It ranges from mild peripheral blood eosinophilia in asymptomatic patients to severe eosinophilic peritonitis where the eosinophil count constitutes about 30%. 40,41 Also, presence of air in the abdominal cavity (pneumoperitoneum) can cause eosinophilic peritonitis because connections in hospitalised patients may not be made properly, resulting in inadvertent introduction of air.
Who carries out PD for hospitalised PD patients? The patient, caregiver, healthcare team (medical doctor, nurse)?
Performing the PD during hospitalisation depends on multiple factors such as the patient’s stability, who usually does the PD at home, the reason for the admission, the cognitive status of the patient, the availability of resources and the availability of a confident well-trained healthcare team at the hospital where the patient is admitted. Ideally, In the PD-providing hospitals, the healthcare team should carry out the PD for the hospitalised PD patients. If patient is admitted to non-PD-providing hospitals, it is reasonable for the patient who is on established PD at home, capable and is knowledgeable to carry on their PD during hospitalisation. Also, the trained family member who is willing to perform PD for the hospitalised patients is an alternative option. We should avoid switching PD patients unnecessarily to intermittent haemodialysis (IHD) as this transition carries with it the risk intrinsic to insertion of a CVC and a theoretical risk of losing the RKF. 42 Some hospitals are more comfortable with cycler-based PD, and there should be little hesitation to alter the PD modality between continuous ambulatory peritoneal dialysis (CAPD) and cycler during hospitalisation if it keeps the patient on PD. Unfortunately, there may be medicolegal or policy reasons why a hospital may not permit a patient or a family member to carry out the PD.
Do I have to switch hospitalised PD patients to HD post abdominal surgeries, post hernia repair or after cardiac surgery?
Switching a PD patient undergoing elective hernia repair to interim HD is usually not necessary. 43 Shah et al. reviewed the feasibility of undergoing hernia repair in PD patients without switching temporarily to HD. 43 This was a single-centre retrospective study from our centre that included 50 PD patients, 42 of them on CAPD and the rest on continuous cycler peritoneal dialysis (CCPD). Twenty-five patients had an umbilical hernia, eighteen patients an inguinal hernia, five patients’ incisional hernia and two patients had epigastric hernia. None of the patients needed conversion to HD around the hernia repair. 43 They were on their regular PD prescription until the morning of the operation, drained their effluent before surgery, then remained off dialysis for 48 h postoperatively and were closely monitored clinically and with blood work. 43 The PD was gradually restarted with a low fill volume 1–1.5 L and up-titrated slowly as needed up to 4 weeks postoperatively, when they resumed their original prescription. 43 The average total follow-up was 33 months, and no hyperkalaemia or PD-leakage was noted and there was no early recurrence of hernia. 43,44 Several factors are important in deciding which PD patient will need HD bridging after the hernia repair. These include the use of a mesh and its location, (whether it is IP or totally extraperitoneal), and the presence of RKF. If the location of the mesh is IP, it is better to avoid using the PD for several weeks to allow the healing and mesothelial covering of the mesh to prevent the risk of bacteria infecting the mesh. Also, holding PD without the need to bridge to HD can be achieved easily if patient has adequate RKF (perhaps 5 ml/min or more). In our program, we routinely repair hernias without switching to HD. The exceptions would include those who are anuric and those who had the complication of incarcerated or strangulated bowel from the hernia. In the latter instance, there is at least a theoretical risk that enteric bacteria may leak across the compromised bowel.
Management of PD patients after cardiac surgery remains a source of conflict among nephrologists, intensivists and cardiac surgeons. One of the concerns among the intensivists is the effect of the peritoneal fluids in increasing the intrabdominal pressure, which can affect the respiratory haemodynamics and ventilation requirements; another concern that the PD does not provide sufficient ultrafiltration to achieve euvolaemia in such vulnerable patients post cardiac surgery. Continuing PD post-cardiac surgery has several advantages: fewer resources are needed, and it minimises the risk of vascular access-related bacteraemia, which is essential, especially in patients with a recent heart valve replacement. The ultrafiltration achieved by using high concentration PD solution of 4.25% is the same as that produced by 24 h of continuous kidney replacement therapy. Kumar et al. studied the outcomes of PD versus HD after cardiac surgery. 45 They looked at the 30-day mortality as the primary outcome of the study, which was the same in HD and PD patients at 11% and 10%, respectively, and no difference in the 2-year survival between the two groups. 45 The approximate length of stay in the cardiac surgical unit was significantly shorter in PD patients (2 days vs 4 days, p = 0.05), although the total length of the hospital stay did not differ. 45 PD is effective as HD after cardiac surgery and haemodynamically tolerable in patients who are haemodynamically unstable. CCPD can be performed for 24 h or more in the ICU if necessary. Occasionally, the dialysis fluid has been noted to drain out of a chest tube or sternotomy postoperatively, in which case there has probably been some operative communication with the peritoneal cavity. In these instances, we recommend temporarily switching to HD
In contrast to the above, there are situations where holding the PD or switching temporarily to IHD should be considered. The setting is often a surgical issue within the abdominal cavity where there may again be a risk of leak of bacteria into the peritoneal cavity. Examples include hospitalised PD patients with abdominal infections such as cholecystitis, diverticulitis, ischemic colitis or appendicitis. PD should of course be held if the patient needs laparotomy.
What are some PD-related nursing considerations in caring for hospitalised PD patients?
Nurses working in hospital wards that do not usually have PD patients may not be familiar with both the PD equipment and with procedures related to the modality. For example, nurses must be aware of the presence of the catheter tunnel in the subcutaneous tissue and familiar with the catheter, transfer set and catheter tunnel. Many of these patients receive regular subcutaneous injections during hospitalisation. With this training they can avoid the site of the PD tunnel for subcutaneous injections, thereby avoiding the risk of accidentally pricking the subcutaneous part of the catheter. There have been circumstances where nurses have confused the PD catheter for a feeding tube and infused G-feeds into the peritoneal cavity. It may be helpful to label the different tubes to avoid this error. Also, the nurses should be educated if they notice any wetness around the catheter to notify the team for consideration of antibiotic prophylaxis for wet contamination to prevent the risk of peritonitis. 4 Protocols should be available to address both wet and dry contamination. These protocols may help to prevent peritonitis following an accidental contamination.
Care workers charged with exit site cleaning and dressing change should have familiarity with the procedure and not place undue stress or tourniquet on the catheter at the exit site. The same applies to carrying out the PD-exchanges, hospital nurses who are unfamiliar with PD must have training before doing exchanges for a patient. Moreover, to reduce the chance of catheter dysfunction, bowel movements should be monitored to avoid the development of constipation.
Finally, there have been circumstances where the conversion from a Fresenius PD transfer set to a Baxter transfer set depends on what resources are available. Protocols on how to do this conversion should be available, and, before discharge, the home PD unit should be aware of this conversion to be able to restore equipment compatible to the home setup.
Can we add any medication to the PD fluids in hospitalised PD patients, if so, which medications can be added and how?
Electrolyte disorders such as hypokalaemia are frequently encountered in hospitalised patients. IP potassium replacement is safe and can be considered as an alternative option to oral or intravenous potassium replacement in hospitalised PD patients. 46 Other medications that can be administered IP are antibiotics, which commonly administered by this route in peritonitis treatment but can also be considered for other infections, particularly if venous access for parenteral administration is limited. Also, IP heparin is indicated if fibrin is present in the bags, for slow PD catheter drainage and for peritonitis. 4 Of note, IP heparin does not usually cause anticoagulation because it is not readily absorbed across the peritoneal cavity. 47 However, it should never be used in a patient with heparin-induced thrombocytopenia. Administering any agent in the PD fluids should be done by well-trained nurses to avoid the risk of contamination. Apart from the heparin, and antibiotics, administering the medications through the IP route is not advisable, unless there is no other option.
Can we use PD to manage life-threatening hyperkalaemia in hospitalised PD patients?
Hyperkalaemia is an uncommon electrolyte abnormality in patients on long-term PD. When it does occur, HD is considered to be the optimal dialysis choice to manage it, although there is limited evidence. While the amount of potassium removed per unit time is greater in HD, consideration must be given in the urgent/emergent setting to the time necessary to establish a usable vascular access and the time necessary to assemble an HD nurse and machine to perform the dialysis (assuming HD is available in the hospital).
Successful treatment of life-threatening hyperkalaemia with frequent manual PD exchanges and automated PD with 24 h cycler has been reported. 48,49 We consider PD a feasible way to manage life-threatening hyperkalaemia, especially in facilities that do not have access to HD. In addition to dialysis, of course, other therapies should be started to reduce the serum potassium.
How do adjust the PD prescription to optimise the volume management in hospitalised PD patients?
Cardiovascular diseases including heart failure are common causes of hospitalisation in chronic dialysis patients. 50 There is often a pressure to switch PD patients to HD to manage acute pulmonary oedema, and this is usually not necessary. There have been many reports of successful management of acute heart failure with PD. 51 We recommend using frequent short manual PD exchanges with hypertonic PD solutions. Consecutive dwells of 4.25% dialysate with 4-h dwells will usually result in successful ultrafiltration of litres of fluid. Furthermore, as discussed with the management of urgent/emergent hyperkalaemia, a change to HD would entail necessary delay to establish vascular access and machine setup.
Footnotes
Author contributions
RBA wrote the first draft of the manuscript, JMB wrote the case vignette and both authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RBA declares that there is no conflict of interest; JMB is Speaker and Consultant: Baxter Healthcare and DaVita Healthcare Partners.
Ethical approval
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RBA is sponsored by King Saud University, Riyadh, Saudi Arabia.