
Abstract
The practice and clinical outcomes of peritoneal dialysis (PD) have demonstrated significant improvement over the past 20 years. The aim of this review is to increase awareness and update healthcare professionals on current PD practice, especially with respect to patient and technique survival, patient modality selection, pathways onto PD, understanding patient experience of care and use prior to kidney transplantation. These improvements have been impacted, at least in part, by greater emphasis on shared decision-making in dialysis modality selection, the use of advanced laparoscopic techniques for PD catheter implantation, developments in PD connecting systems, glucose-sparing strategies, and modernising technology in managing automated PD patients remotely. Evidence-based clinical guidelines such as those prepared by national and international societies such as the International Society of PD have contributed to improved PD practice underpinned by a recognition of the place of continuous quality improvement processes.
Keywords
Introduction
Although peritoneal dialysis (PD) was initially developed to treat acute kidney injury in the first part of the 20th century it was not until 1962 that the first programme of long-term PD was established, the same year in which a machine was developed for automated PD (APD). The Tenckhoff catheter, introduced in 1968, enabled the establishment of the first continuous ambulatory PD (CAPD) programme based in Toronto in 1978. 1,2
PD was initially delivered using two one-litre glass bottles with a long disposable transfer set, 3 with each exchange involving a large number of steps. The high risk of infections (typically one every three months), inadequate clearance of small solutes and deterioration of peritoneum resulting in ultrafiltration failure adversely impacted the reputation of CAPD and this was compounded by an association with encapsulating peritoneal sclerosis. 4 The causes of these poor outcomes were due to a combination of factors including limited experience with the modality, inadequate approaches to prescription, lack of policies and procedures for infection control, poor pre- and post-catheter insertion care, a lack of understanding of the role of prophylactic antibiotics, inadequate education and training of medical and nursing staff and patients, and lack of adoption or inadequate implementation of the evidence-based clinical guidelines such as those prepared by the International Society of PD (ISPD).
The implementation of a “First PD” policy, as in Thailand and Hong Kong, where PD is used as the first treatment modality for appropriate kidney failure patients, resulted in significant increase in the PD take-on rate in those countries. 5 This policy was primarily driven by increasing costs of dialysis, lack of space for in-centre haemodialysis (HD) and a goal to provide effective therapies with improved outcomes. Likewise, “PD-Favoured” policies (e.g. USA, Canada, Mexico, Spain, China and India), where government policy on dialysis encourages the use of PD as the treatment choice while removing any existing disincentives, and a Home Dialysis-First (e.g. Australia, New Zealand and Finland), where PD or home HD is used as the first treatment modality, usually as a complimentary strategy, all contributed to increased PD take-on rates. 6 The penetration rate in Hong Kong reached more than 70%, 7 and the technique and patient survival have significantly improved in Thailand. In 2016, patient survival rate was 83% at 1 year, and 54% at 5 years, and technique survival rates (censored for death and kidney transplantation) were 95% at 1 year and 81% at 5 years. 5
PD has multiple benefits including better preservation of vascular access and residual kidney function, and as a home-based treatment, patients on PD benefit from reduced requirement to travel to centres and reduced risk of transmission of infectious diseases including respiratory viruses (e.g. Covid-19) or blood borne viruses. Improvements in practice and clinical outcomes of PD over the last 20 years have led to the current success of the therapy resulting in a renewed interest in this modality. The purpose of this review is to increase awareness and to update healthcare professionals on current PD practice, with particular focus on patient and technique survival, patient modality selection, pathways onto PD, understanding patient experience of care and its place prior to kidney transplantation.
Clinical outcomes
Relative mortality
In the early days of the therapy, the overall survival for patients treated with PD was inferior to HD 8,9 – however that has changed in recent decades so that outcomes are at least equal between the modalities, with a possible advantage for PD over the first 1–2 years of therapy 10,11 (Table 1). Greater improvement in survival was noted among patients treated with PD relative to HD at all follow-up periods in a United States Renal Data System (USRDS) analysis of three 3-year cohorts (1996–1998, 1999–2001 and 2002–2004). 12 These results were supported by evidence from Canada from 1990 to 2004, 13,14 Korea from 2004 to 2015, 15 Taiwan from 1997 to 2006, 16 Australia and New Zealand from 1998 to 2012 17 and Denmark from 1990 to 2010. 18
Studies showing better survival rate during the early years on PD.
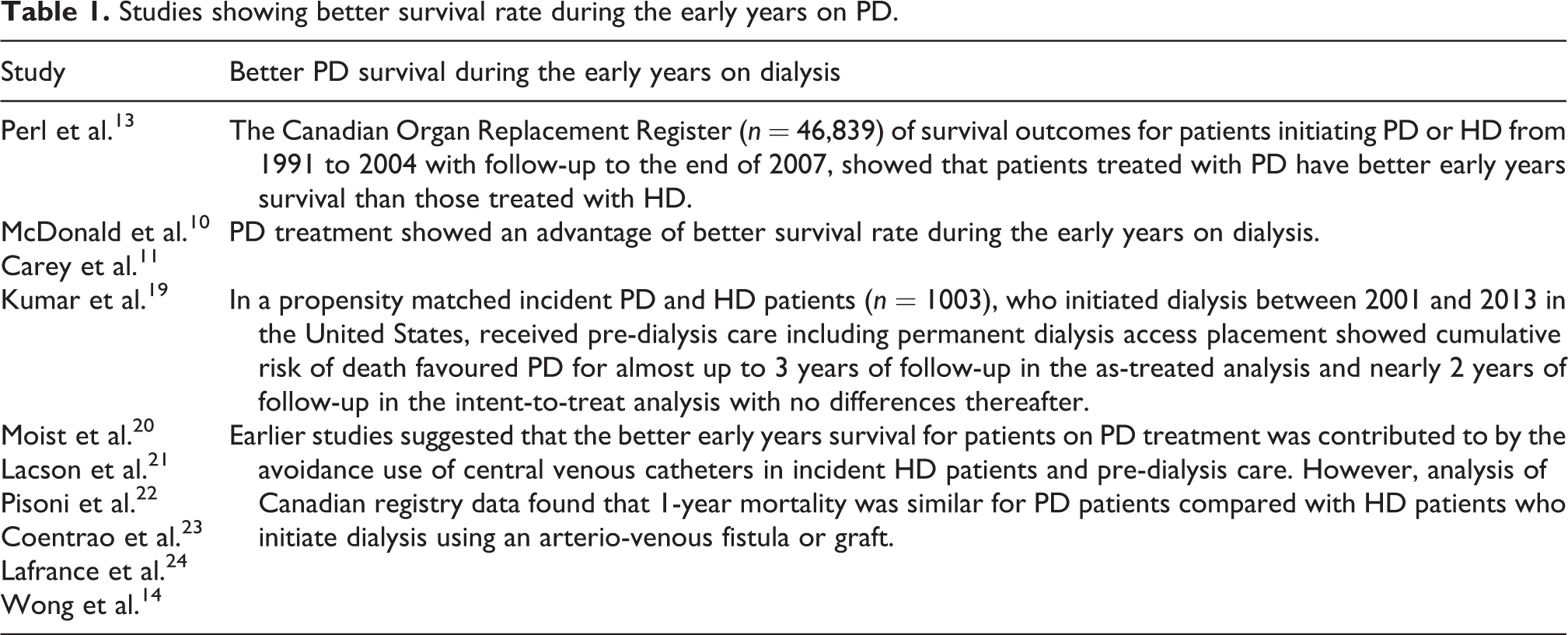
However, since randomised controlled trials of dialysis modality choice have not proven practicable available data is from registries or large cohort studies. These are subject to bias by indication – since for example sicker patients, or those presenting late requiring dialysis, were more likely to receive HD than PD. To add to this has been the adverse effect on HD outcomes of the use of cuffed dialysis lines with the associated risk of bacteraemia. Complex statistical techniques have been used to reduce the impact bias on the outcome of registry studies by adjusting for a range of covariates leading to the conclusion that long-term survival is similar between PD and HD. 12,25 –27
Quality of life
The ability to undertake usual activities for those receiving PD has been prioritised as an important outcome for patients, care givers and healthcare professionals 28 and contributes to quality of life (QoL). Existing QoL instruments vary in their characteristics, content and validation in the assessment of life participation and further work is ongoing to establish a core patient-reported outcome measure to assess life participation in patients receiving PD. 29
Multiple studies have assessed QoL among patients on PD, one of the earliest being the Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD) that followed 230 incident dialysis patients over 18 months measuring QoL using the SF-36, and reporting, a consistently favourable effect of HD on physical QL over time compared with PD, whereas mental QoL values remained similar. 30 A recent systematic review and meta-analysis concluded that patients treated with PD had better generic health-related QoL measured by SF-36 and EQ-5D than HD patients with particular advantages in the subdomains of physical functioning, role limitations due to emotional problems and burden of kidney disease. 31 There is some evidence of better QoL for APD than CAPD 32,33 and although this was not confirmed in NECOSAD. 34
The Frail and Elderly Patient Outcomes on Dialysis (FEPOD) multicentre observational study, which compared the QoL and physical function of older patients with end-stage kidney disease among 129 patients receiving assisted PD matched to 122 patients on HD, demonstrated higher treatment satisfaction score on assisted PD, 35,36 whereas older (>65 years) patients reported significantly better QoL than younger patients. 37 This is important since the Annual Renal Data of the USRDS showed since 2010 a progressive increase in the uptake of PD modality in older age group (65–74 and ≥75). 38
Covid-19 infection
The Covid-19 pandemic had a hugely deleterious effect on kidney patients with high hospitalisation and mortality for those who contracted the illness and major disruption of routine care including transplantation and access surgery. 39 The high transmission rate between patients at dialysis centres required the adoption of stringent infection control measures including during transportation between home and the dialysis centre as well as creating a strong argument for managing patients in the community if possible. Home-based dialysis enabled patients to self-isolate more effectively avoiding the increased risk of exposure to Covid-19 associated with frequent travel to the clinic and the risk of exposure while dialysing.
The reduced infection risk associated with home therapies was reported from the Lombardy region where the infection rate was 8% in HD patients compared to 1% in patients on PD treatment. 40 These trends were confirmed by studies from the United Kingdom, Canada, Spain and France. 41 –43 In the United Kingdom, the mortality rate from Covid-19 was more than twice among those who received HD in-centres compared with those on home-based dialysis during the first wave of the pandemic. 44 The ERA-EDTA Registry reported that the mortality in dialysis patients and kidney transplant recipients infected with Covid-19 across Europe was 20% on average, though it reached 30% in Spain, Switzerland and Netherlands. 45
PD as a bridge to kidney transplantation
There is evidence for the impact of prior dialysis modality on kidney transplant outcomes. A systematic literature review and meta-analysis of 16 studies assessed post-transplant mortality, graft survival or delayed graft function in patients receiving HD or PD pre-transplant showed that patients who received pre-transplant PD had significantly reduced early graft dysfunction than pre-transplant HD. 46 Similar findings were observed in a separate meta-analysis of 12 studies, where pre-transplant PD was significantly associated with lower 5-year mortality post-transplant compared with HD, and while there was no significant difference in the graft survival rate, pre-transplant PD patients was associated with a lower incidence of delayed graft function. 47
Approaches impacting modern PD
The patient pathway onto PD
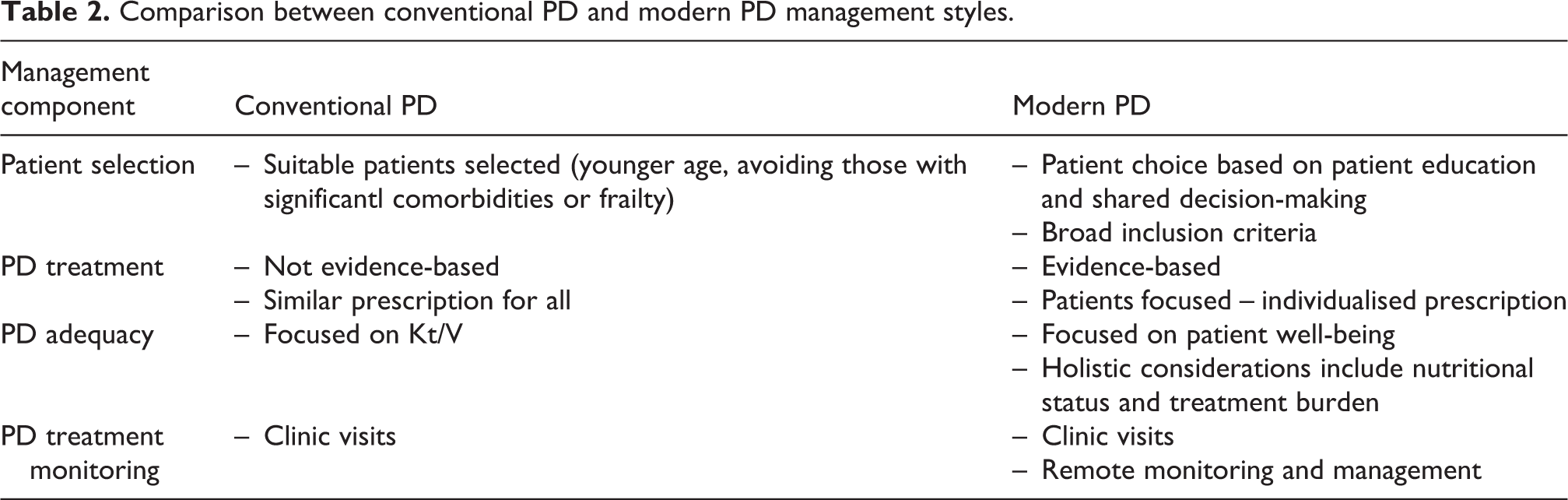
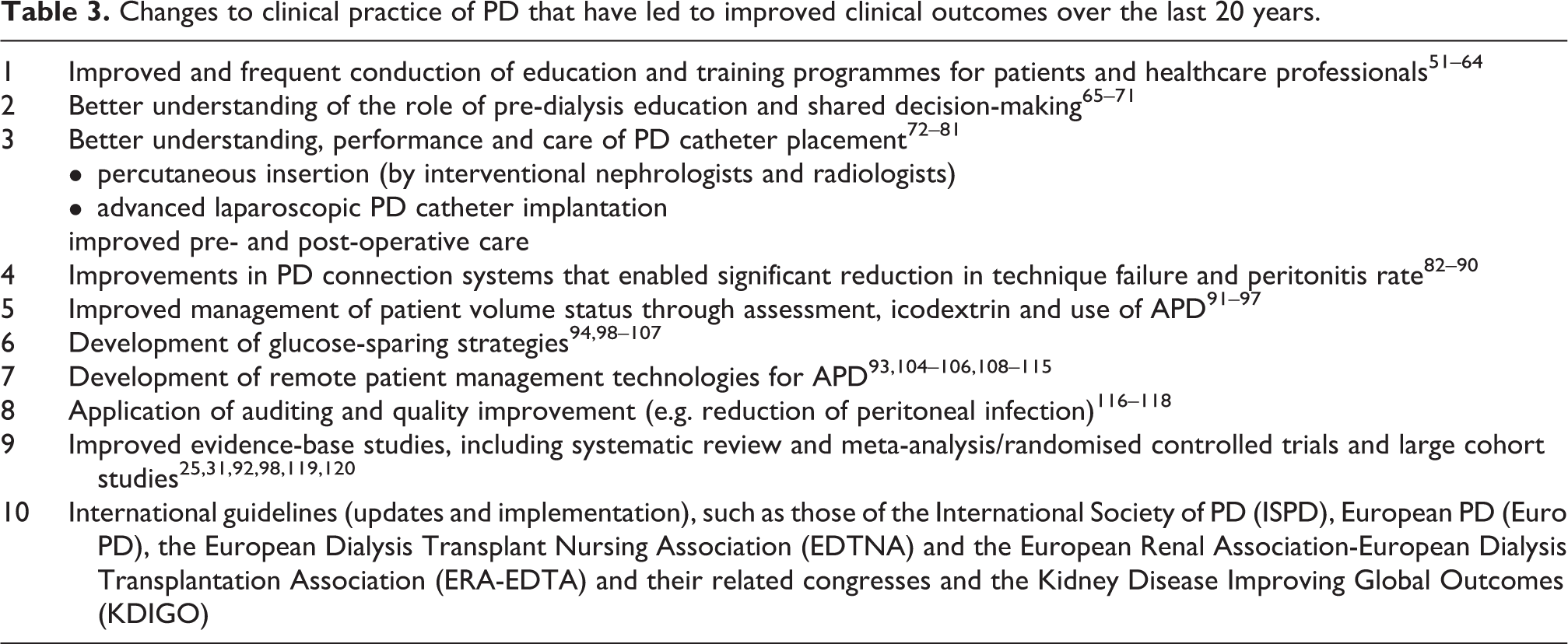
In recent years, there has been better understanding of the processes that enable the establishment of a patient onto PD and how that differs from conventional PD (Table 2). This is important because an understanding of the barriers that there are to commencing a patient on PD allows consideration of steps required to overcome them 48 (Table 3). These include identification of all potential PD candidates, systematic assessment for eligibility and offering PD to those who are, supporting the choice of PD as a therapy, timely PD catheter insertion and the commencement of PD. 49 Importantly, this requires to be underpinned by a process of iterative patient education. 49,50
Comparison between conventional PD and modern PD management styles.
Changes to clinical practice of PD that have led to improved clinical outcomes over the last 20 years.
Patient suitability for PD
In a prospective study of 1303 patients with chronic kidney disease (CKD), stages 3 and 4 conducted at seven North American nephrology practices 78% (95% CI: 75.6–80.1%) were considered to be medically and psychosocially suitable to undertake PD as a dialysis modality compared with 95% for HD and 53% or transplantation. 121 Absolute contraindications to PD are limited to those who have lost peritoneal membrane function, have abdominal defects or abnormalities that prevent effective fluid and solute removal or increase the risk of infection, or where the patient and caregiver are either unable or unwilling to perform the therapy. 121,122
Although there has been a signal from registry studies of poorer outcomes for older female diabetic patients on PD compared with HD, this was not the case in a propensity adjusted meta-analysis of 17 cohort studies. 25,123 A nationwide prospective cohort from Korea investigated whether glycaemic control had a modifying effect on mortality between HD and PD in incident dialysis patients with diabetes. In the group with good glycaemic control (HbA1C less than 8.0%), there was a significant (p = 0.021) survival advantage of PD, not seen in the poor glycaemic control group, suggesting that glycaemic control might, at least in part, contribute to better survival of PD in incident dialysis patients with diabetes. 91
Shared decision-making
Patients with advanced CKD are required to make an important choice related to their care that involve uncertainties that can impact on survival and QoL. Shared decision-making (SDM) describes a person-centred approach in which the patient and their treating physician work together to develop a collaborative appreciation of the patient’s situation, needs and goals, incorporating best available medical research evidence while avoiding biases and conflicts of interest. 65 This is particularly relevant when it comes to modality selection. The three talk model of SDM has been comprises: (1) the Team Talk where dialysis education is given, options are discussed and patient priorities and goals explored; (2) the Option Talk where the trade-offs of benefits and harms are given for each modality with time for the patient to weigh up which options best suit their preferences; and (3) the decision talk in which the patient decision is made and evaluated. 66,124
Patient engagement and empowerment in the clinical consultation enables the choice of treatments suitable for their clinical condition, based on their own lifestyle and social circumstances. 67 SDM improves patient satisfaction and confidence in decision-making. 68 Patients who engage in SDM perceive dialysis more positively, and without SDM there greater potential for regret. 69 It is enabled by providing the potential dialysis patient with sufficient information on their condition and the renal replacement therapy (RRT) options. This is followed by discussing the needs and priorities of the patient and the supportive medical advice of the treating physician of best modality, based on patient’s values. Decision aids have a particular role in enabling the patient and their family members to work systematically through the options aligning attributes of treatment to personal preferences. 70
Education and training
Implementation of effective structured dialysis educational programmes are key to enable patient access to self-care dialysis modalities 51,52 with up to 40–60% of potential patients enrolled in such programmes choosing PD and improved outcomes. 53 –55,125 Despite this, there is evidence that kidney dialysis education programmes are significantly under used. 126 A systematic multidisciplinary renal team approach is necessary to prepare for RRT, provide education about the condition, the different available options of RRT and training required to enable supported self-care where appropriate. 127 Multidisciplinary team-based pre-dialysis care comprising nephrologists, nurses, dieticians, social workers and psychologist is associated with superior outcomes to that provided by a solo nephrologist across a range of key domains including hospitalisation, all-cause mortality and temporary catheterisation. 56 The renal team is required to be well-trained and should have adequate exposure to social, psychological and medical concepts of CKD, the specific needs of these patients at different stages of their disease and indications and advantages of different modalities of RRT. 57 –59 The participation of family members is important since understanding the long-term nature of the disease and its demanding nature is a vital for those who are considering contributing to care and support and for developing strategies for resilience.
Pre-dialysis education and training usually requires 1–2 hours per month for 3–6 months (three sessions may be enough), starting 12–18 months before like dialysis inception. Sessions might include some or even all of the following: (a) explanations including questions and answer sessions with nephrologists in either large group (classroom sessions) or small groups, (b) detailed interviews and assessments by pre-dialysis nurses, (c) educational videos, (d) person-to-person meetings, (e) multidisciplinary team meetings, (f) visits to HD and PD units and (g) booklets/brochures. 60 The Nursing Liaison Committee of the ISPD has undertaken a review of PD training programmes around the world and developed a syllabus for PD training to help PD nurses train patients and caregivers based on a consensus of training programme reviews, utilising current theories and principles of adult education. 61,62
Unplanned start
Late referral to the nephrologist (<3 months before initiation of dialysis) is associated with suboptimal dialysis initiation and deprives patients of the opportunity for adequate control of complications of CKD and measures that may slow down the deterioration of renal function and possibly avoid or reduce the risk of cardiovascular morbidity and mortality. 51,63,128 –130 Furthermore, patients presenting unplanned for dialysis not only have less chance of selection of self-care dialysis modality 55 and are more likely to require temporary percutaneous catheter insertion. 131
However, suboptimal dialysis start also occurs in patients known to nephrologist. A study from Toronto reported that suboptimal start defined as initiation as an inpatient and/or with a central venous catheter occurred in 56.4% of patients followed by a nephrologist for >12 months prior to the initiation of dialysis. 132 In a recent study in the Nordic Countries, suboptimal dialysis initiation occurred in 42% of all dialysis starts and was associated with hypoalbuminaemia, comorbidity and a faster rate of eGFR loss. 133 Temporary central venous catheters are associated with an increased risk of luminal thrombosis, infection, inadequate blood flow rates and central venous stenosis. 134,135 Tunnelled catheters have been associated with a 39% increased risk of death. 136
In-hospital education for unplanned start patients requiring acute dialysis initiation increased home dialysis adoption from a baseline of 13% up to 35% (49 patients selected PD and 22 selected HD), suggesting that acute educational intervention may influence dialysis modality selection. 137 These findings were supported by another retrospective study which indicated that 55% of patients enrolled in a pre-dialysis education programme chose self-care (home PD and HD) dialysis. 55
Urgent start PD enables patients with advanced CKD who unexpectedly need dialysis due to uraemia or fluid overload to be treated with PD rather than HD. 138 There are multiple reports of this approach in the literature including comparisons with urgent start HD that have reported lower complication rates for PD. 139,140 Unplanned start with PD was associated with a lower requirement for vascular access procedures and had a 1-year technique survival of 79%. 141 A Cochrane systematic review concluded that when compared with HD initiated using a central venous catheter, urgent start PD may reduce the risk of bacteraemia and had uncertain effects on other complications of dialysis, technique and patient survival. 142 This approach requires coordination at a programme level of several components including timely catheter placement, availability of a social worker or nurse to counsel the patient their family to facilitate SDM, and the ability to provide early PD training. 138 Teaching a patient who is uremic may take longer than usual – training nurses may have to make frequent home visits and assisted home PD by visiting nurses during this initial period is valuable.
PD catheter implantation
The establishment of high quality, growing PD programmes relies on timely PD catheter insertion with minimal complications and this has been supported through the establishment of registries that collect information about catheter insertion techniques, complications and outcomes. 72,73 Randomised controlled evidence does not support an advantage for one of the core techniques of percutaneous, laparoscopic or open surgery insertion techniques over another. 74,75 The ‘advanced’ laparoscopic technique facilitates visualisation of the peritoneal cavity for adhesions and hernias and enables a number of adjunctive techniques such as rectus sheath tunnelling to reduce the risk of catheter migration, adhesiolysis and omentopexy, where the redundant omentum is anchored to the anterior abdominal wall of the upper abdomen. 75 –79 Systematic review and meta-analysis of cohort studies of advanced laparoscopy in comparison with basic laparoscopy and open surgery reported significant reductions in catheter obstruction and migration, as well as better 1- and 2-year catheter survival compared to open surgery. 80
Percutaneous PD catheter insertion (commonly supported using ultrasound or fluoroscopy) remains a vital technique, especially in acute/urgent initiation of dialysis. 143,144 During Covid-19 surges where operating theatre capacity was limited, percutaneous insertion required less infrastructure including personnel and operating theatre time. A pragmatic and commonly adopted approach is to use the percutaneous approach for suitable patients, reserving the advanced laparoscopic technique for patients with significant prior abdominal surgery, where there is catheter dysfunction or a second tube is required. 145 –147
Assisted PD
Assisted PD describes support in the home for patients who are unable to perform the therapy by themselves, for example in frail individuals who may have barriers to self-care, and it can therefore increase the number of people eligible for PD. Oliver et al. studied 134 incident chronic dialysis patients (median age 73) and found 81% of patients had at least one medical or social condition, which was a potential barrier to self-care PD. 148 Each barrier reduced the probability of being eligible for PD by 26% (odds ratio 0.74, per condition, p < 0.02) adjusted for age, sex, pre-dialysis care, in-patient start and availability of home care. Of the 22 assisted patients, 15 required chronic support, 5 graduated to self-care and 2 started with self-care but later required assistance. Adverse events were similar between assisted PD and traditional modalities.
Assisted PD can be achieved by trained staff or family members and is available in many European countries, 149 Canada and Australia using healthcare workers and many Middle Eastern, Asian and South American countries using extended family members or domestic help. In Europe and Canada, it is usually delivered as assisted APD, although in France is usually assisted CAPD. Despite increased cost of providing assistance in PD, it may be less expensive than in-centre HD in Western Europe and Canada. 150 Patient and technique survival rates on assisted PD are similar to those of self-care PD. In France, the French Peritoneal Dialysis Registry (RDPLF) showed that the median survival for those requiring nurse assistance (80% of cohort) is 24 months, 151 which is very similar to 75+ age group (mostly treated by HD) in the United Kingdom renal registry data. 152 Data from the RDPLF also show that, overall, the risk of peritonitis is not increased in older patients and actually lower in those who have nurse assistance. 153 The recently published baseline data from the FEPOD Study suggest that QoL is similar on assisted PD and in-centre HD, although satisfaction with treatment is higher on assisted PD (reviewed in Brown and Wilkie 154 ).
Technical developments contributing to modern PD
PD connection systems
PD is reliant on the integrity of the plastic tube systems that connect the catheter to the bags of dialysate to enable the infusion of dialysate into the peritoneal cavity and subsequent drainage of effluent. These connection systems have evolved overtime through a straight connection system used a piece of tubing and a ‘spike’ or a luer lock device, requiring a new connection at each exchange with the empty bag being rolled up and remaining attached until the next exchange when the process is repeated to the most recent development of a twin bag (double bag) system. In this system a Y-connection with the fresh dialysis solution bag is manufactured as a single unit and therefore patient has one less connection procedure to perform. At the same time the patient is able to perform ‘flush before fill’ in which the Y-connection system is flushed for any remnant bacteria with fresh dialysis solution which is drained into the drainage bag, before introducing the fresh dialysis solution is infused into the peritoneal cavity. 82 –84 A Cochrane systematic review of 12 eligible trials with a total of 991 randomised patients, showed that the Y-set and twin bag systems were superior to conventional spike systems in preventing CAPD peritonitis. 85 The importance of delivery systems for PD was underlined by an ANZDATA registry report covering the period of 1995 and 2014 that after multivariable adjustment demonstrated 10% lower rate of technique failure and 22% lower rate of peritonitis for 13438 patients using Baxter systems compared with 2848 using Fresenius and 289 using Gambro. There was an important era effect with a 32% lower technique failure in the 2010–2014 cohort compared with 1995–1999. 86
Glucose-sparing strategies
Despite the effectiveness of glucose as an osmotic agent for PD there have been longstanding concerns around its metabolic effects (e.g. hyperglycaemia and increased insulin resistance – especially in diabetic patients, and hyperlipidaemia), cardiovascular disease, and changes in the characteristics of peritoneal membrane leading over time to a reduction in ultrafiltration. The introduction in the 1990s of icodextrin as a glucose-sparing osmotic agent had a favourable impact on PD clinical outcomes. A Cochrane Systematic Review compared icodextrin with conventional PD solution in 13 studies (1291 participants) reporting with moderate certainty evidence that icodextrin reduced episodes of uncontrolled fluid overload by 70% (RR = 0.30; 95% CI = 0.15–0.59) and augmented ultrafiltration by an average of about 450 ml/day (95% CI = 289.28–607.80) without compromising residual renal function or urine output. 119 More recently, a systematic review of 19 randomised clinical trials (enrolled 1693 participants), icodextrin was associated with improved ultrafiltration reflected by fewer episodes of fluid overload, overall reduction in glucose exposure and absorption and decreased mortality risk by 51% (odds ratio 0.49; 95% CI = 0.24–1.00) compared to glucose-only PD-based solutions. 92
APD and remote patient management
The popularity of APD modality has considerably increased over the past few years, with its use being between 40% and 60% of PD in most European countries and in the United States increasing from 47% in 2000 to 80% in 2015. In Canada, APD accounted for 64% and 71% of patients on PD in 2009 and 2018 respectively, with similar penetrance in Australia and New Zealand. However there considerably lower utilisation of APD in countries with developing healthcare systems (reviewed in Roumeliotis et al. 155 ).
The increase in APD use is explained by improved design and usability of cyclers, the ability to monitor and manage PD patients remotely, life-style benefits of reducing the use of day time exchanges (e.g. studying and employment), beneficial impact on ultrafiltration, lower intraperitoneal pressures, decreased mechanical complications and possibly lower peritonitis rates. 156 Its utility was confirmed for anuric patients in the European Automated Peritoneal Dialysis Outcome study. 157
The remote monitoring system (RMPD Sharesource) devised by Baxter enables patients being treated with APD to have therapy related information shared electronically using cloud-based connectivity with their healthcare team and permits certain adjustments in the therapy to be performed remotely. The value of this approach is that the healthcare team can review the progress of therapy virtually and make proactive decisions to resolve problems that may be developing. Key among the advantages is the ability to see treatment cycles on the APD machine in order to assess the function of the PD catheter, to problem solve and respond to difficulties. Changes in blood pressure and patient weight give indicators of fluid status that enable pro-active actions to avoid episodes of fluid overload or dehydration. Adjusting the prescription remotely allows for responses to problems to be implemented immediately by the healthcare team without the need for the patient to attend the clinic or for the nurse to visit the patient’s home. The healthcare team are able to monitor patient adherence to the prescription, important since reduced adherence can have deleterious consequences.
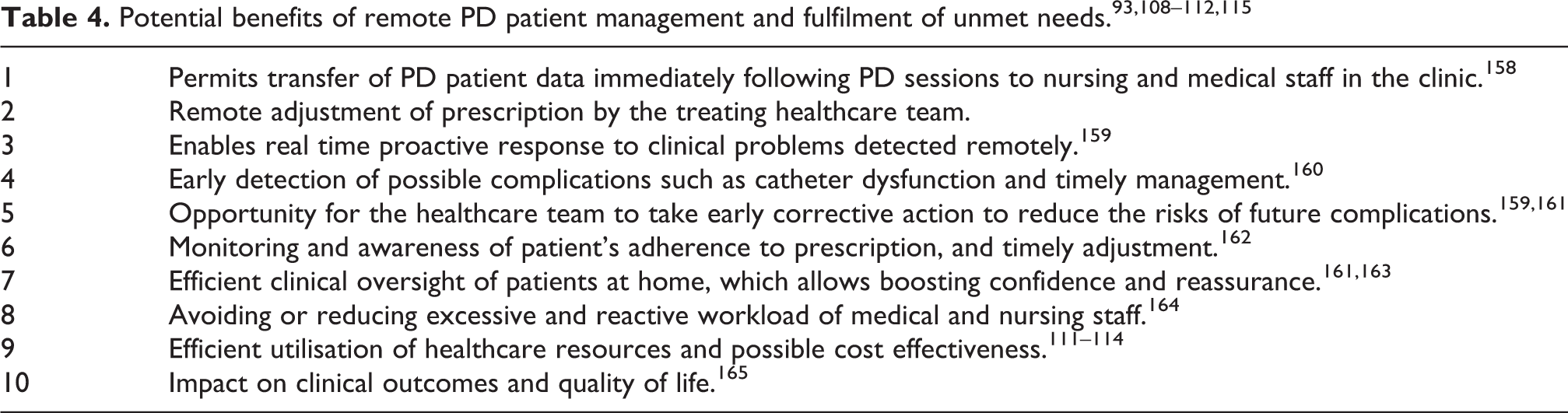
A range of benefits have been reported for RMPD (Table 4), including better monitoring and management of adherence of PD patients to their prescription. It was reported to enhance patient-focused care in qualitative semi-structured studies based on interviews with nephrologists and dialysis nurses across nine dialysis units in New Zealand. 108 An observational study reported time savings for the treating physicians and nurses following remote APD management combined with reductions in visits per patient per year, and night alarms per patient per month. 109 A qualitative study of patients and caregivers from the same group concluded that RMPD may increase patient knowledge about their kidney disease and its treatment, encourage accountability to the clinical team, enhance partnerships with clinicians, and improve access to treatment and timely care. However patients were clear that they did not want RMPD to replace face-to-face clinical contact with clinicians. 110
A retrospective study conducted in Colombia between 2016 and 2018 reported a significant beneficial impact of RMPD patient management on the reduction of technique failure. 93 The same group had reported significantly reduced hospitalisation in an earlier study. 111 These outcomes were due to better adherence to PD prescription, improved ultrafiltration, better blood pressure control, early detection of catheter dysfunction, timely modification of the treatment, reduction in the frequency of visits to the clinic, and enhanced communications between the patient and the clinical team. In addition, simulations studies have reported cost reductions and improved resource utilisation following implementation of RMPD. 112 –114 The value of RMPD was reported during the Covid-19 pandemic from Italy where it supported continuation of care of PD patients 115 and it has been included in recommendations that responded to the pandemic from international nephrological societies. There remain, however, a range of challenges that require better evaluation including best approaches to implementation, means to overcome difficulties with internet connection in some locations, data management, patient anxieties and the ability of patients to see their data.
Quality improvement and the role of evidence-based guidelines
A central part of the improvement in the quality of PD care over the last 20 years has been the systematic incorporation of evidence into clinical guidance that has been made available internationally and translated into several languages. These are available through regional and international societies such as the ISPD and have particularly focused on the prevention and management of infection, the placement of PD access and the prescription of person centred PD. 75,94,166 Evidence has come from large international cohort studies such as the Peritoneal Dialysis Outcome and Practice Patterns Study (PDOPPS), 167 national registries, as well as a limited number of randomised controlled trials. The availability of clinical guidelines and efforts to facilitate adherence to these guidelines can result in improvement of clinical outcome. For example, the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS) across 170 centres caring for more than 11,000 patients in Australia/New Zealand (ANZ), Canada, Thailand, Japan, the UK and the USA showed variation in PD-related infection prevention and treatment strategies across countries with limited uptake of ISPD guideline recommendations for example in prescribing intravenous antibiotics prior to PD catheter insertion and the application of topical mupirocin/aminoglycoside as part of exit site care. 168 It is only through establishing the link between practice and outcomes and highlighting important variations that the quality of care can continue to improve.
Conclusion
The modern application of PD is supported by consistent improvement in the overall mortality rate, better survival rate during the early years on dialysis and achievement of similar long-term survival rate to HD. QoL advantages for PD have been consistently reported and it is a valuable option for older patients with reduced illness intrusion, and for diabetic patients with survival advantages for those with controlled diabetes. Used before transplant, PD may offer lower delayed graft dysfunction rates when compared with HD. PD outcomes have benefited from pre-dialysis education and training for potential PD patients, unplanned urgent start programmes, SDM, improved catheter insertion techniques, better connection systems, low-glucose strategies and remote patient management. International guidelines and conferences have been playing a major role in improving the PD clinical outcomes. Finally, PD treatment had particular advantages during the Covid-19 pandemic, where there was a particular role for remote management.
Footnotes
Acknowledgements
None.
Author contributions
Both authors contributed equally to the preparation and writing of this review.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AK is Baxter Head of Medical Affairs – Renal Care, Middle East & Africa. MW has received honoraria for educational presentations from Baxter, Fresenius medical care and acted as a consultant to Triomed AB. He has received a research grant from Baxter.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Not applicable.
Informed consent to publish
The authors consent to publication.