
Abstract
Introduction:
Peritoneal dialysis (PD) remains underutilised and unplanned start of dialysis further diminishes the likelihood of patients starting on PD, although outcomes are equal to haemodialysis (HD).
Methods:
A survey was sent to members of EuroPD and regional societies presenting a case vignette of a 48-year-old woman not previously known to the nephrology department and who arrives at the emergency department with established end-stage kidney disease (unplanned start), asking which dialysis modality would most likely be chosen at their respective centre. We assessed associations between the modality choices for this case vignette and centre characteristics and PD-related practices.
Results:
Of 575 respondents, 32.8%, 32.2% and 35.0% indicated they would start unplanned PD, unplanned HD or unplanned HD with intention to educate patient on PD later, respectively. Likelihood for unplanned start of PD was only associated with quality of structure of the pre-dialysis program. Structure of pre-dialysis education program, PD program in general, likelihood to provide education on PD to unplanned starters, good collaboration with the PD access team and taking initiatives to enhance home-based therapies increased the likelihood unplanned patients would end up on PD.
Conclusions:
Well-structured pre-dialysis education on PD as a modality, good connections to dedicated PD catheter placement teams and additional initiatives to enhance home-based therapies are key to grow PD programs. Centres motivated to grow their PD programs seem to find solutions to do so.
Keywords
Introduction
Treatment with peritoneal dialysis (PD) as a first line modality for management of end-stage kidney disease (ESKD) has many advantages 1 : better preservation of residual kidney function 2 and future vascular access, better post-transplantation outcomes, 3 better patient empowerment and lower intrusiveness. 4 Outcomes on PD versus haemodialysis (HD) are equal in large registries for all relevant subgroups, 5 and the majority of professionals active in kidney replacement therapy (KRT) would for themselves opt for a home-based therapy. 6 Nevertheless, in reality, the majority of ESKD patients are still treated with in-centre HD. 5
Many barriers to the growth of PD programs have been forwarded. 7 PD is in most healthcare structures more economic than HD, which might reflect on the income of the provider 8,9,10 Changes in reimbursement strategies can be linked to upsurges in PD uptake, as seen in the United States. 11,12
Unplanned start of dialysis is also associated with a lower likelihood to start PD 13 –15 a risk factor for short and longer period outcomes in terms of mortality and opportunity for transplantation . 15,16 Nevertheless, starting unplanned patients on PD is feasible, 16 can lead to outcomes that are not different from those starting on HD in the same setting 17 and can avoid a substantial number of patients starting KRT on a central venous line. Lower uptake of PD is also attributed to lack of patient education and free choice, 18 –20 conditions which are more likely to be present in unplanned patients. 20 However, education on PD and homebased therapies can increase PD incidence, even in the setting of the unplanned starter. 21 Furthermore, many PD programs report problems to achieve and maintain functioning peritoneal access, especially in the unplanned patients. 22 Unfavourable social circumstances 23 and bias in healthcare workers and patients 9,13 are also factors negatively impacting uptake of PD in general.
It is conceivable that all these individual factors known to be associated with PD uptake find a common ground in true motivation to grow the PD program as reflected in the organisational aspects of nephrology services. 24 Working on individual parts, for example, setting up assisted PD programs to tackle frailty as a barrier to PD, 23 probably are rather a reflection of motivation to grow PD than an independent cause of PD growth. 25 Identification of this common ground is thus important, as interventions aiming at this aspect would be most effective in improving PD incidence and prevalence. We hypothesize that the intrinsic dedication of the PD team might be the most important factor in achieving reasonable PD incidence and prevalence. 25
To dissect this hypothesis, in this survey, we first assessed the likelihood to start unplanned patients on PD and the factors that are associated with the inclination to do so. Secondly, we explored the association between centre practices and different organisational aspects of access management practices.
Methods
Study design
An online survey developed by the EuroPD Future Leadership Initiative was sent to nephrologists, nephrologists in training and dialysis nurses in Europe. The survey was developed based on a systematic review and a three-round Delphi process within the group, accomplished during two face-to-face meetings in 2019 with all group members. In the survey, the following topics as potential explanations for differences in uptake of PD were discussed: unplanned start PD, assisted care programs, access placement policy, pre-dialysis education in planned and unplanned patients, motivation to grow PD program and centre size. The final complete survey consisted of 56 questions (Online Appendix 1). Questions addressed professional background, country of employment, centre type and size; presence of structured programs for all dialysis modalities; provision of education; presence of a dedicated team; reimbursement of PD versus HD and impact on income of nephrologists; aspects of home dialysis, as the proportion of incident and prevalent patients on home dialysis, assistance for patients on home dialysis and placement of PD catheters.
Finally, the survey offered several case vignettes on different topics. For the current article, we analysed the case vignette posing the situation of ‘a 48-year-old woman not previously known to your unit who presents at your emergency department. Diagnosis of established end stage renal disease is made’. Respondents were asked to rank the likelihood of the following possible options for management of the patient in their institution in order of probability (4: most probable, 1: least probable): the patient will start on HD by a central venous line; the patient will start on HD by a central venous line and AV access will be planned; the patient will start on HD by a central venous catheter, and different KRT modalities, including PD, will be discussed for follow-up treatment; the patient will receive a PD catheter and PD will be started within 48 h. To analyse the impact of centre characteristics and practices on ‘unplanned start’, the three first options were lumped together in the further analysis as ‘unplanned HD’ versus ‘unplanned PD’ (dichotomic analysis). We also performed an analysis in which the two first options were lumped together as ‘unplanned HD’, versus either unplanned HD but intention to educate for other modalities and versus unplanned PD (three groups). In this way, we hoped to better appreciate the (potentially) different impact of being PD minded in general versus be inclined for unplanned PD in specific.
The survey was developed in SurveyMonkey and mailed to all EuroPD members for distribution across Europe via their colleagues and national nephrology societies. Participation was voluntary and anonymous, so we could not determine a response rate. Respondents could submit the survey between 11 December 2019 and 15 January 2020. The survey study was approved by the Ethical Committee of the Ghent University Hospital (EC 2019/1972).
Statistical analysis
Answers regarding the following variables were grouped into a limited number of categories: centre type (non-academic vs. academic), centre size (<50, 50–100, 100–200 or >200 patients). Likelihood that chronic kidney disease or unplanned patients would receive education on kidney function/kidney failure/PD/home HD/in-centre HD (Likert-type scale) impact on the income of the nephrologist of reimbursement of PD as compared to in-centre HD (eight categories converted into three categories) and the proportion of incident (intended modality in the first 3 months) and prevalent home dialysis patients (expressed as categorical variable <10%, 10–20%, 20–30%, >30%). Descriptive statistics were used to present an overview of professional background, centre characteristics and organisational factors.
The univariable association between centre characteristics, PD practices and organisational factors on the one hand and likelihood of opting for unplanned PD modality start in the vignette (dependent variable) on the other hand was explored by Chi-square analysis for the categorical and by one-way analysis of variance for the ordinal variables.
Descriptive statistics were used to present an overview of financial factors as the perceived profitability of PD (i.e. the sum of reimbursement and disposable costs) and the perceived impact of the distribution between KRT modalities (i.e. PD, home HD, in-centre HD, kidney transplantation) on the income of nephrologists.
All statistical analyses were performed with SPSS Statistics version 25 (SPPS, Chicago, Illinois, USA).
Results
Characteristics of respondents and their centres
In total, 628 respondents completed the survey. Of these, 53 were from countries outside Europe, these were excluded, so 575 respondents were included in the final cohort. Details for the respondents according to their different countries of origin are reported in Table 1. In the overall cohort, respondents were nephrologists with more than 10 years of experience (53%), nephrologists with less than 10 years of experience (32.7%), nephrologists in training (9.0%), nurses (4.5%) or administrative heads of the nephrology units (1%). Fifty percent of the respondents are active in a non-academic centre, while centre size (i.e. the total number of dialysis patients) varied between <50 patients (9.6%), 50–100 (32.0%), 100–200 (39.1%) and >200 patients (19.3%).
Characteristics of respondents according to country.
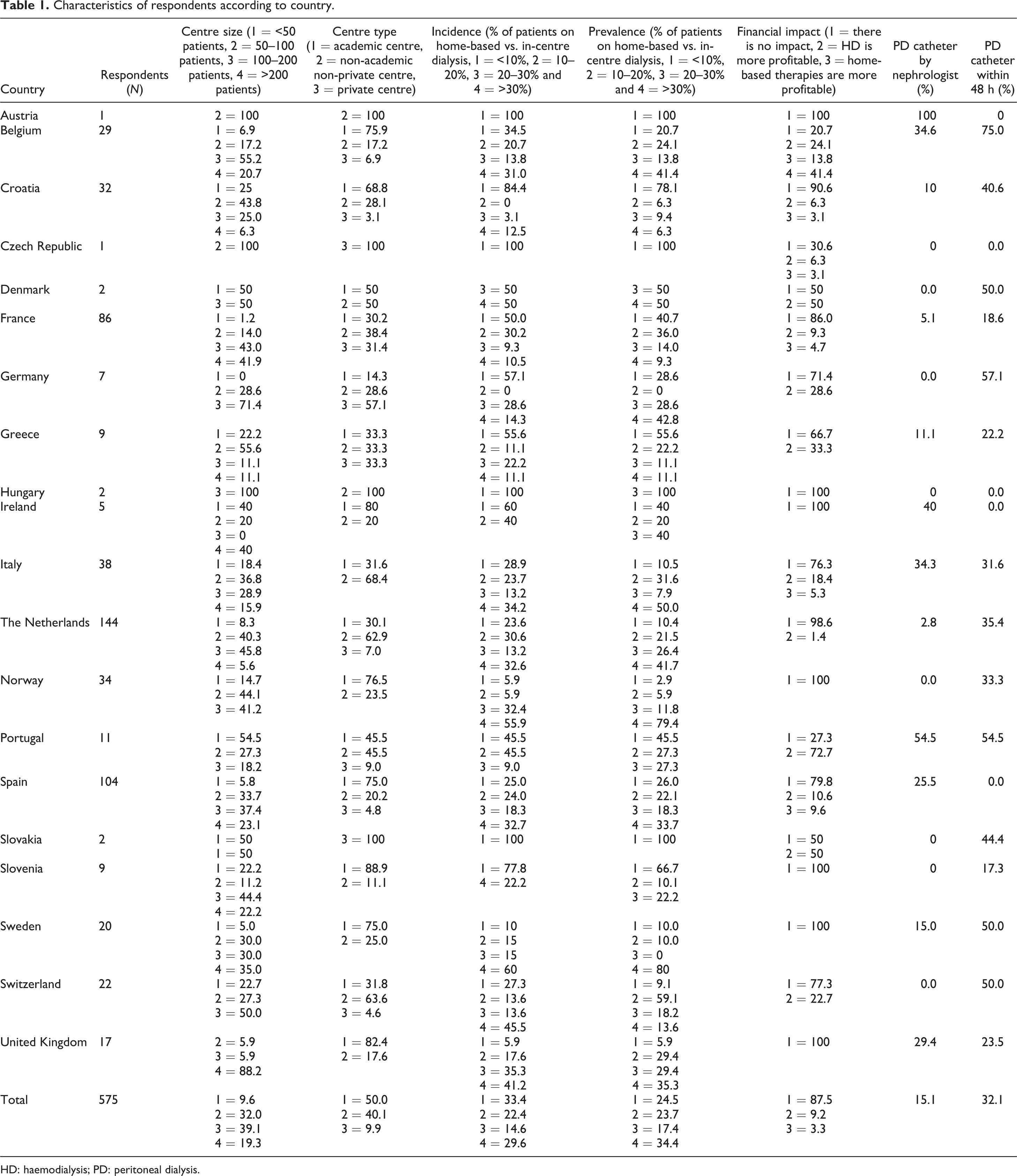
HD: haemodialysis; PD: peritoneal dialysis.
The proportion of incident patients starting home-based therapies versus HD also varied among respondents between <10% of patients (33.4% of respondents), 10–20% of patients (22.4% of respondents), 20–30% of patients (14.6% of respondents) and >30% of patients (29.6% of respondents). Similarly, the proportion of prevalent home-based therapies versus HD patients also varied from less than 10% of patients (24.5% of respondents) to 10–20% of patients (23.7%), 20–30% of patients (17.4%) and more than 30% of patients (34.4%).
Collaboration agreements with other units were reported to be established for management of PD catheter-related issues (41.5%), management of presumed encapsulating peritoneal sclerosis (16%), infectious complications (28.4%), training and education (23.1%) or for clinical case discussions (28.4%). Respondents further indicated their centre had a quality assessment program in place for PD catheter follow up (56.4%), monitoring of presumed encapsulating peritoneal sclerosis (19.6%), infectious complications (61.5%), training and education (41.2%), survival (41.2%) and for technique success (38.3%).
Thirty-five percent of all respondents indicated they did not know the profitability of PD or home-based therapy in their centre. In total, 85% perceived that the mix of modalities (home based vs. in centre) did not influence their income.
Respondents were more likely to report their centre had done special initiatives to grow home-based therapies, a proxy to solicit their inclination for home-based therapies, if they also reported having a well-structured pre-dialysis education program (p < 0.001), a well-structured PD program (p < 0.001), ability to have a PD catheter placed within 48 h (p = 0.04) and a high likelihood of PD education in patients needing to start unplanned dialysis (p < 0.001).
Centre characteristics and practices of respondents according to dichotomic analysis of the vignette on unplanned start
Table 2 depicts centre characteristics and practices according to the answer on the vignette ‘unplanned PD vs. unplanned HD’. Pre-dialysis education (p = 0.06), assisted PD program (p = 0.04) and having a nephrologist who can place a PD catheter (p = 0.04) were associated with starting the vignette patient with unplanned PD.
Characteristics according to selected modality in case vignette on unplanned start.
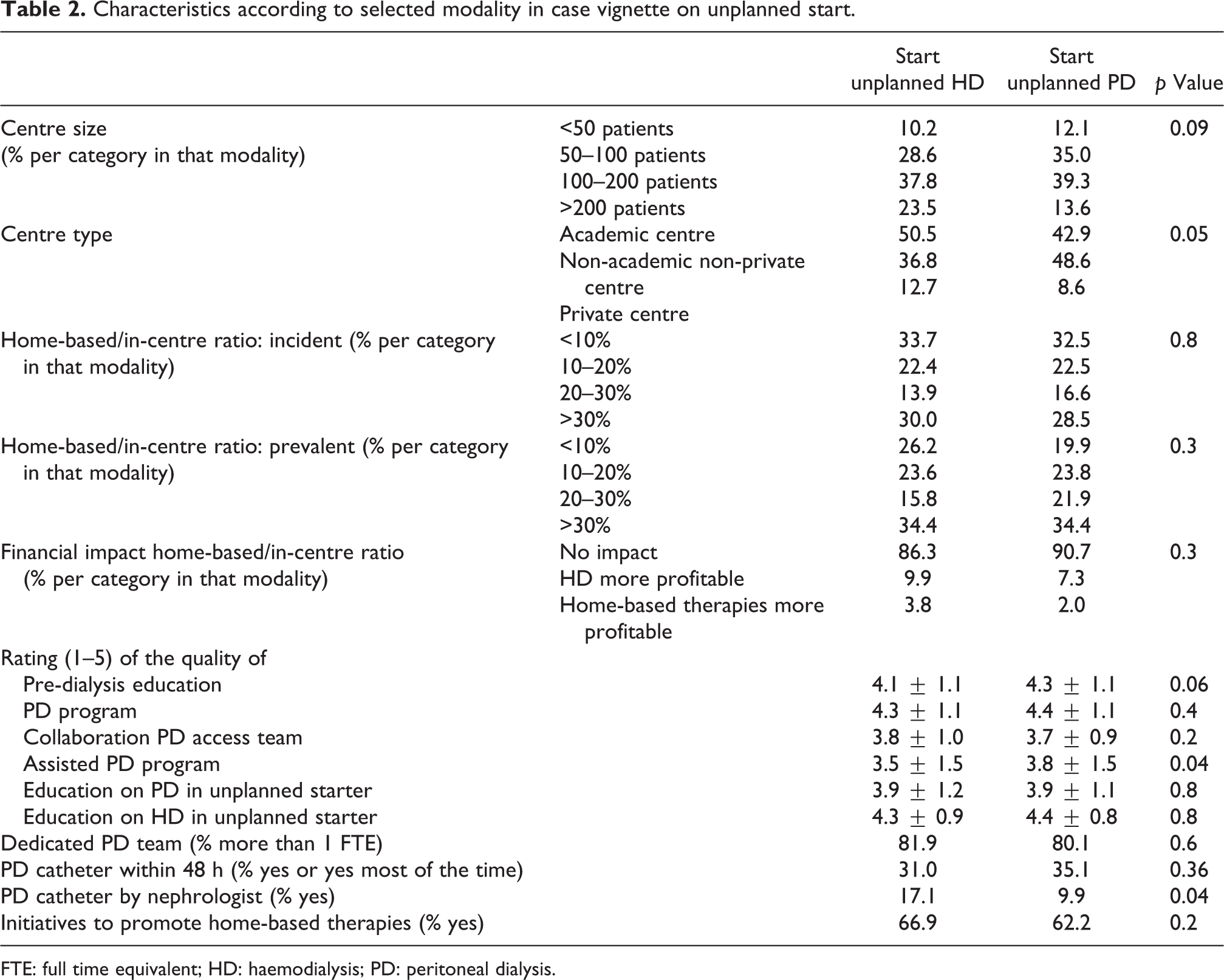
FTE: full time equivalent; HD: haemodialysis; PD: peritoneal dialysis.
Associations between centre characteristics and practices and inclination to start unplanned PD in the case vignette (three-group analysis)
Unplanned HD (34.9%), unplanned HD with a plan for education on PD (32.2%) and unplanned start PD (32.8%) were reported as the most likely modality choice in an unplanned patient as described in the vignette and as least likely option by 24.9, 17.6 and 47.5% of respondents, respectively.
The more respondents perceived their pre-dialysis education program (Figure 1: panel A) and their PD program to be well structured (Figure 1: panel B), it was less likely that the patient from the vignette would start unplanned HD and more likely she would start PD (p = 0.001 and p = 0.005). The same pattern could be seen for a good collaboration with the PD catheter placement team (Figure 1: panel C) and the likelihood that the case vignette patient would receive unplanned education on PD (Figure 1: panel D, p = 0.01 and p = 0.001, respectively). The financial impact of the balance between home-based and in-centre dialysis appeared to be not associated with the acute modality choice in the case vignette patient (Figure 2: panel A, p = 0.3). Having done initiatives to promote home-based therapies did not impact the choice for unplanned PD but decreased the odds that patient would end up on HD, as it especially increased the odds of starting unplanned HD with the intention to educate on PD (Figure 2: panel B, p = 0.006). Whether or not placement of a PD catheter is likely within 48 h did not impact the choice for unplanned start PD
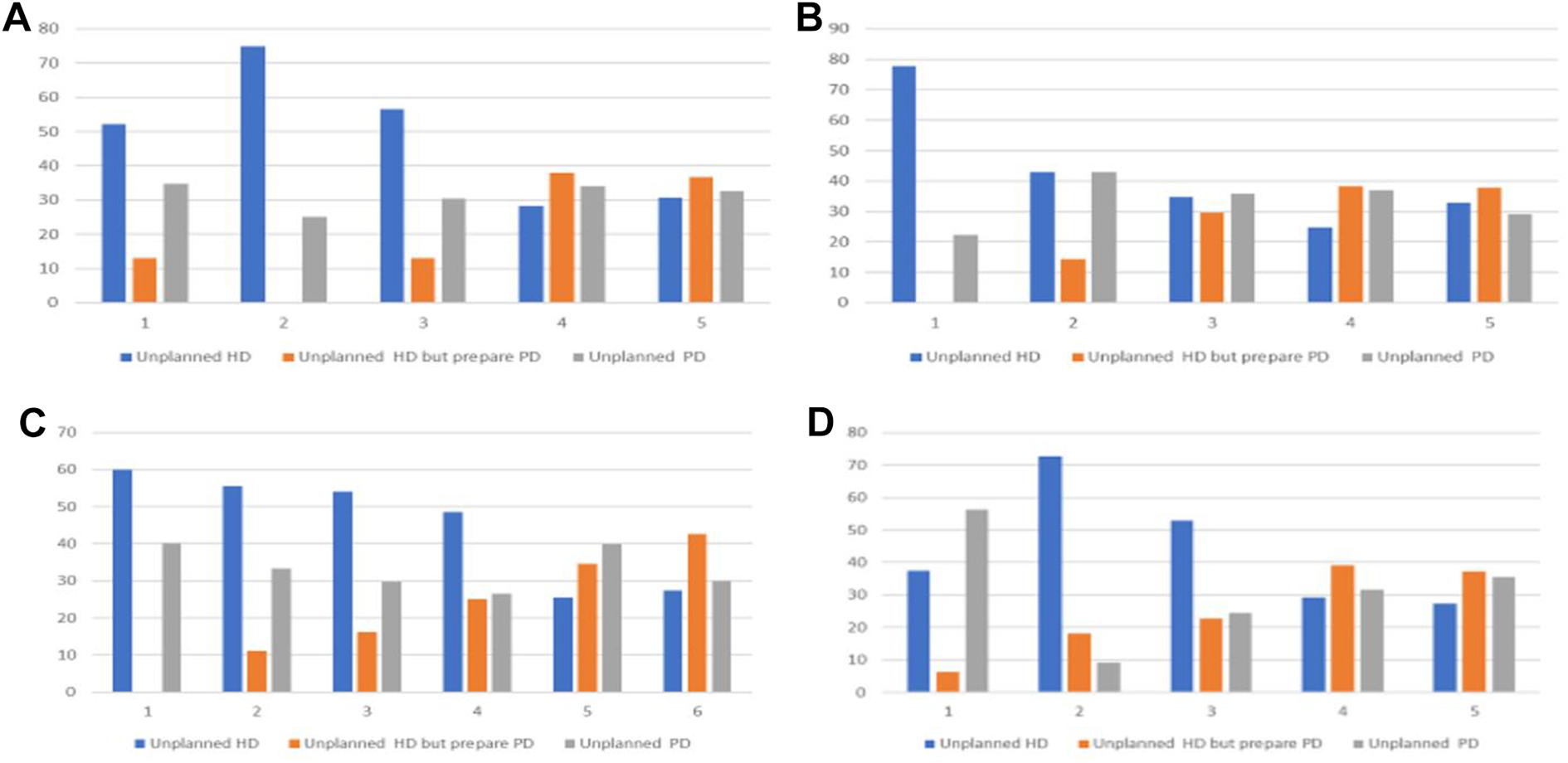
Panel (A): How well structured is your pre-dialysis education program? X-axis: how well structured is your pre-dialysis education program from (1) not at all to (>5) very well structured; p = 0.001 Chi-square; Y-axis: % of respondents in that category. Panel (B): How well structured is your PD program? X-axis: how well structured is your PD program from (1) not at all to (>5) very well structured; p = 0.005 Chi-square; Y-axis: % of respondents in that category. Panel (C): How good do rate your relationship with the PD access placement team? X-axis: how good do you rate collaboration with the PD access placement team from (1) very poor (>6) very good; p = 0.01 Chi-square; Y-axis: percentage of respondents in that category. Panel (D): How many of unplanned patients will receive education on PD? X-axis: how many of unplanned patients will receive education on PD: (1) no patient to (>5) all patients; p = 0.001 Chi-square; Y-axis: % of patients in that category.
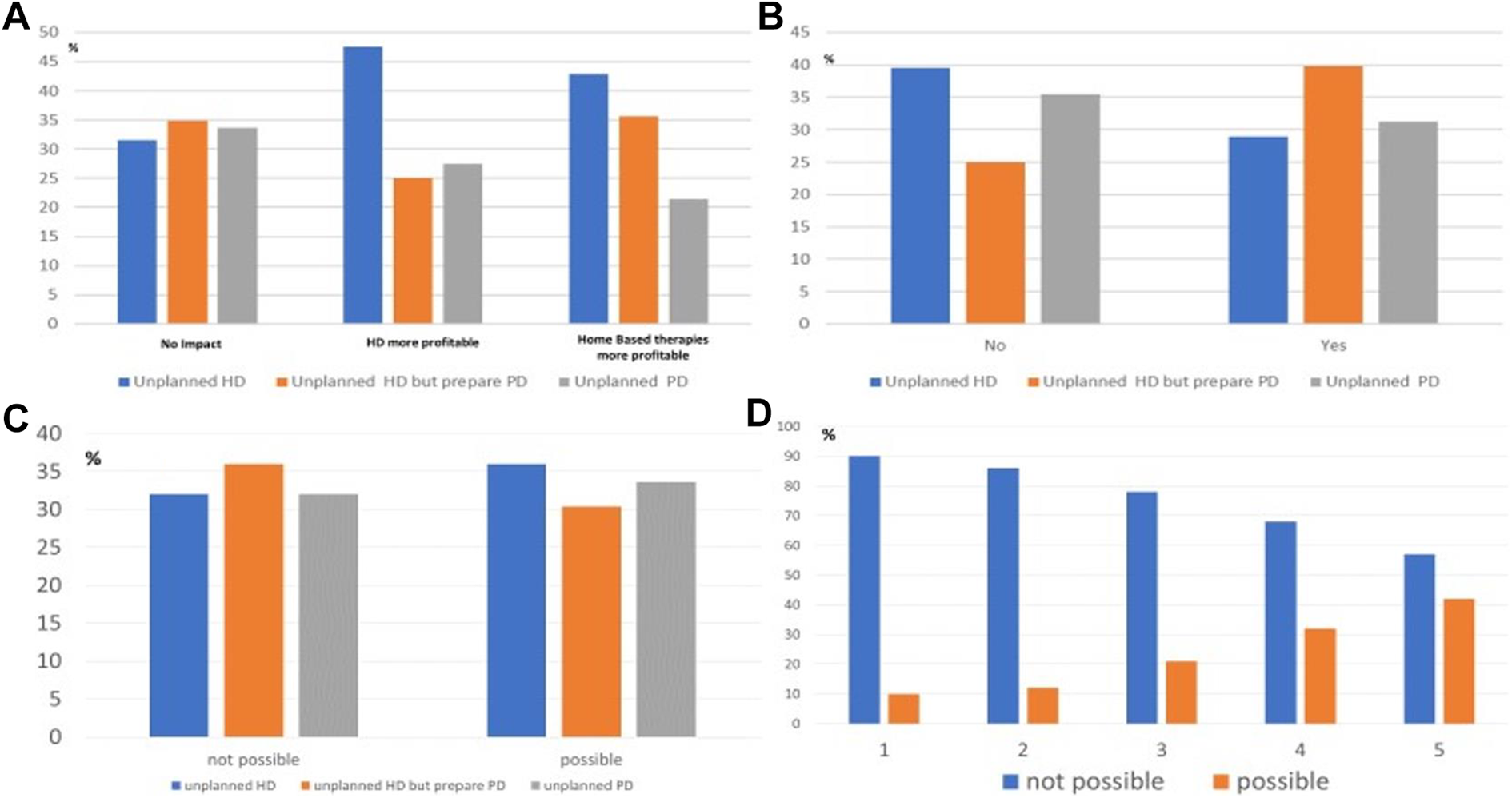
Panel (A): Effect of financial impact of home-based versus in-centre dialysis. X-axis: how does the modality mix influence the income of the nephrology team: p = 0.3 Chi-square. Y-axis: % of the respondents in that category. Panel (B): Impact of initiative to promote home-based therapies. No versus yes: p = 0.006 Chi-square; Y-axis: % of respondents in that category. Panel (C): PD catheter can be placed within 48 h. Not possible versus possible: p = 0.5 Chi-square; Y-axis: % of respondents in that category. Panel (D): Rating of collaboration with PD catheter placement team by respondents who indicate that PD catheter placement is versus is not possible within 48 h. X-axis: rating of collaboration with PD catheter placement team; not possible versus possible: p = 0.01 Chi-square, Y-axis: % of respondents in that category.
Discussion
Unplanned start of dialysis remains a frequent condition around the world. 26 There is emerging evidence that the outcome of patients with an unplanned start of dialysis is comparable for those starting on PD versus HD. 17 In our study, starting unplanned patients on PD was not associated with any centre characteristic except having a good structured pre-dialysis and assisted PD program. As it is hard to see how these could directly influence unplanned start of PD, we hypothesize these are markers of inclination of the team to grow PD in general. This can better be appreciated when the odds that an unplanned patient will end up on PD are modelled rather than directly unplanned PD start. In such analysis, parameters associated with more inclination to use home-based therapies, such as having taken initiatives to grow home-based therapies, having a well-structured PD and pre-dialysis education program and a high likelihood an unplanned patient will receive education on PD decrease the odds that unplanned patients will start and remain on HD.
While there are reports of increased PD use and availability with changed payment policies, 12 patients starting unplanned dialysis still have a higher likelihood to end up on HD, especially with a central temporary catheter. 26 Previous studies suggest that the combination of poor pre-dialysis education, inadequate education on different dialysis modalities for unplanned starters as well as logistical problems related to urgent PD catheter placement may explain the lower likelihood for unplanned patients to start PD. 25,27 Furthermore, in the current survey, we found that in routine circumstances, PD catheter placement was likely to take more than 48 h in two of the three respondents, with variations among countries (Table 1). This was, however, not reflected in the inclination to opt for an unplanned PD start. Moreover, the likelihood to get a PD catheter placed within 48 h was positively associated with the quality of the collaboration with the PD access team, an essential, albeit insufficient requirement for successful unplanned PD. This suggests a hypothesis that simply having the option for urgent PD access placement alone does not result in more unplanned PD, though this needs to be combined with whole-program strategic initiatives and good collaboration with the PD access team.
Centres having an interventional nephrologist able to place a bedside PD catheter remain an exception. One might anticipate that it would favour choice for PD in unplanned patients, but this was not the case in this survey. Either the nephrologists may not be available for urgent PD catheter placement or it is easier obtained otherwise, due to good collaboration with the PD access team. Nephrologists may consider a bedside (blind) catheter placement less suitable for urgent start of PD, due to risk for leakage, while a metanalysis by Tullavardhana et al. found percutaneous PD placement as effective and safe as surgical technique in suitable patients. 28
Education on different aspects of kidney disease and different kidney replacement modalities is an important aspect of the care for patients with ESKD. Certain transition clinics involving multidisciplinary care with the goal to ‘start dialysis in the right patient at the right time with a working access and the patient involved and satisfied with the decision’ has been suggested. 27 A multidisciplinary team with a specialised nurse, dietician, social worker, physiotherapist and possibly access surgeon to support the patient in between the visits to the nephrologist. 27 A recent metanalysis found multidisciplinary care to reduce mortality, estimated Glomerular Filtration Rate (eGFR) decline and risk for dialysis start with an acute central catheter. 29 Previous reports have indicated that pre-dialysis education is associated with higher likelihood of PD as an initial modality and may empower the patient to choose self-care modalities. 20,30,31 Consequently, if patients do not receive adequate education on dialysis modality choice, considered a driver of low PD uptake, this corresponds to HD patients not remembering ever to have received information on alternative treatment options. In our survey, having a good pre-dialysis education program was strongly associated with the inclination to start PD in an unplanned patient, directly on PD or with a bridging on HD. Allegedly attention to patient education results in a more sustainable modality choice on average, thus ensuring a stable growth of the PD program as a whole, irrespective of the fact that it does not result in an increase of unplanned PD. 32 It is conceivable that, despite best of intentions, education in the early acute stage, when patients are too overwhelmed, is not effective and might even scare patients away from home-based therapies. Our data indicate that though patient education does not increase unplanned PD start, it decreases the number of unplanned patients starting and remaining on HD. Previous studies demonstrate that in-hospital education programs to prevalent acute HD starters were effective to transfer patients to home therapy, home HD or PD. 21 Providing such education on modality choice to unplanned patients does impact both the PD incidence, and PD prevalence, 33 while education on modality choices after stabilisation of the patient might result in patients making more sustainable choices.
Centre size, in our study, was not associated with likelihood of starting unplanned PD. Healthcare workers need to be confident in their treatment advice, since clinician bias could be a modifiable factor to augment PD rates. 13 Centres with few PD patients offer limited opportunities to gain experience, while sufficient exposure to PD-related problems and collaboration are important aspects contributing to generate such confidence. Not surprisingly, patients in high-volume centres have reduced risk for technical failure. 33 Collaboration protocols between centres might be a solution but could prove difficult in a setting of privatised healthcare. In our survey, collaboration between centres for PD-related issues was only moderate, such initiatives should probably be encouraged.
Financial implications of modality choice on the income of the nephrology team were in this survey not associated with unplanned start of PD, possibly due to the stronger than average motivation for home-based therapies of respondents. An overwhelming majority (87%) indicated that modality selection does not impact their financial income. Furthermore, it can be imagined that also for financial considerations, a non-negative incentive for home-based therapies is an essential, but insufficient requirement to grow home-based programs.
Strengths and limitations
The survey was widely distributed, and the response number was high providing important information on factors affecting the inclination on starting PD in an unplanned patient. However, due to the anonymous character of the survey, we are not capable of calculating response rate. Furthermore, we might have captured perceptions of care rather than true practices. It is likely that respondents who completed the survey are more PD-minded than the average nephrologist. It is unclear in how far the respondents are representative for the nephrology landscape in their region. However, in this explorative survey, we were more interested in hypothesis generating qualitative probing, than aiming to provide accurate numbers of practices in certain regions. Therefore, we consider representativeness not as essential. Furthermore, we provided detailed data on the respondents per region to allow the reader to assess representability. The survey was quite long, and response rate of questions therefore drops, not unexpectedly from zero % for the first half to 20–25% in the last 10% of the questionnaire. We did effort to take this potential bias into account in the interpretation of the results, so that unwarranted conclusions are avoided. We do however conclude that underlying true motivation to grow the PD program remains valid and more important than often quoted barriers such as unplanned start of PD or catheter placement issues. It is unlikely that just solving the barriers would increase the inclination to start PD.
Conclusion
Well-structured pre-dialysis education on PD as a modality, good connections to dedicated PD catheter placement teams and additional initiatives to enhance home-based therapies are key to grow PD programs. Centres motivated to grow their PD program seem to find solutions to do so.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608211034988 - Barriers and opportunities to increase PD incidence and prevalence: Lessons from a European Survey
Supplemental Material, sj-docx-1-ptd-10.1177_08968608211034988 for Barriers and opportunities to increase PD incidence and prevalence: Lessons from a European Survey by Ulrika Hahn Lundström, Alferso C Abrahams, Jennifer Allen, Karmela Altabas, Clémence Béchade, Felix Burkhalter, Anne-Lorraine Clause, Richard W Corbett, Gabriele Eden, Karlien François, Louis de Laforcade, Mark Lambie, Heike Martin, Jernej Pajek, Vincenzo Panuccio, Silvia Ros-Ruiz, Dominik Steubl, Almudena Vega, Ewa Wojtaszek, Ariane Zaloszyc, Simon J Davies, Wim Van Biesen and Helga Gudmundsdottir in Peritoneal Dialysis International
Footnotes
Acknowledgements
We would like to thank all healthcare professionals from nephrological units across Europe who completed the survey.
Author contributions
Conception (all) UHL, AA, JA, KA, CB, FB, A-LC, RWC, GE, KF, LL, ML, HM, JP, VP, SRR, DS, AV, EW, AZ, SD, WVB and HG developed and distributed the survey. WVB collected the data and did statistical analysis. WVB, UHL and HG analysed and interpreted the data. UHL, WVB and HG wrote the first version, drafted and revised the paper. All authors critically revised and provided intellectual content of critical importance to edit the manuscript and approved the final version to be published.
Declaration of conflicting interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article: UHL has received consultancy and speaker fees from Baxter Healthcare. WVB received travel grants and honoraria for educational sessions from Baxter Healthcare and Fresenius Medical Care. HG has received speaker fees from Baxter Healthcare and Fresenius Medical Care. All outside the submitted work.
Ethical approval
The survey study was approved by the Ethical Committee of the Ghent University Hospital (EC 2019/1972).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The meetings leading to the preparation of the survey were supported by an unrestricted grant of EuroPD.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.