
Abstract
Several studies have been published in the last decade on the effects of low glucose degradation product (GDP) neutral pH (L-GDP/N-pH) dialysis solutions on peritoneal morphology and function during the long-term PD treatment. Compared to conventional solutions, the impact of these solutions on the morphological and functional alterations of the peritoneal membrane is discussed, including those of effluent proteins that reflect the status of peritoneal tissues. Long-term PD with conventional solutions is associated with the loss of mesothelium, submesothelial and interstitial fibrosis, vasculopathy, and deposition of advanced glycosylation end products (AGEs). L-GDP/N-pH solutions mitigate these alterations, although vasculopathy and AGE deposition are still present. Increased vascular density was found in some studies. Small solute transport increases with PD duration on conventional solutions. Initially, higher values are present on L-GDP/N-pH treatment, but these may be reversible and remain stable with PD duration. Consequently, ultrafiltration (UF) is lower initially but remains stable thereafter. At 5 years, UF and small pore fluid transport are higher, while free water transport decreased only slightly during follow-up. Cancer antigen 125 was initially higher on L-GDP/N-pH solutions, suggesting better mesothelial preservation but decreased during follow-up. Therefore, L-GDP/N-pH solutions may not prevent but reduce and retard the peritoneal alterations induced by continuous exposure to glucose-based dialysis fluids.
Keywords
Introduction
Five-year patient survival in incident PD patients in Europe is similar to that of those on hemodialysis (HD), if not better in intention-to-treat analyses. 1 Yet the dropout rate to HD remains high. After 5 years, only 10% of incident PD patients remain on PD, while this is 25% for HD. 1 Besides death and transplantation, catheter complications and peritonitis are the main reasons for PD discontinuation during the initial years, 2 but thereafter, impaired ultrafiltration (UF) becomes progressively important. 3 The UF decline points to the development of peritoneal membrane changes during prolonged treatment. These morphological and functional membrane alterations have been reviewed in detail. 4 The continuous exposure of the peritoneal tissues to the dialysis solutions is the major culprit of peritoneal remodeling because conventional fluids are composed of extremely high concentrations of glucose, have a low pH, and contain lactate as a buffer substance. Furthermore, they contain glucose degradation products (GDPs) generated during the solution sterilization procedure. A review on GDPs summarized the in vitro data, indicating that glucose with GDPs accelerates the formation of advanced glycosylation end products (AGEs) at a faster rate than glucose alone. 5 Toxic effects of the low pH are probably limited to in vitro and experimental studies because in PD patients, the initial intraperitoneal pH rapidly increases due to dilution with the residual volume after drainage of the previous exchange. 6 However, in some, this initial low pH may manifest as initial pain on infusion of the dialysate.
Around the turn of the millennium, many new PD solutions have been developed that contain glucose as the osmotic agent in the usual concentrations but have reduced GDP content. They all have a higher or normal pH and some have totally or partially replaced lactate with bicarbonate. These dialysis fluids are called low GDP neutral pH (L-GDP/N-pH) solutions. They still have an unaltered glucose content. Less inflow pain with L-GDP/N-pH solutions was established shortly after their introduction. 7 A number of other effects have been summarized in a review, published a decade ago. 8 Strikingly, all studies with a short follow-up duration of maximally 2 years reported higher or increased effluent concentrations of cancer antigen 125 (CA 125), relative to conventional solutions, regardless of the composition of the investigated biocompatible solution. Although the explanation is not fully understood, better preservation of mesothelial cells is one possibility. In contrast, the results of short-term studies with L-GDP/N-pH solutions on fluid and solute transport are equivocal. This is not unexpected, because marked peritoneal remodeling usually takes a number of years to become clinically evident. A number of studies concerning peritoneal alterations in long-term PD patients treated with L-GDP/N-pH dialysis solutions have been published recently. These will be discussed in the following sections using a case history as starting point.
Case history
A 57-year-old female developed kidney failure due to mesangioproliferative glomerulopathy in 1991. She received three kidney transplants in total. The first and second allografts failed due to chronic antibody-mediated rejection, the third one was removed due to thrombotic microangiopathy secondary to chronic hepatitis C. Maintenance immunosuppression included cyclosporin. After the loss of the second and third grafts, she was treated with PD in 2008, altogether for 11 years. Except one mild exit site infection, the patient did well on PD without acute complications or peritonitis. In 2017, Dianeal® was replaced by Physioneal® and icodextrin. Peritoneal function was assessed every 2 years with a 3.86% glucose peeritoneal equilibration test (PET), determination of D/P Na+ after 1 h, and measurement of effluent CA 125 after 4 h. Results are presented in Table 1. D/P creatinine started to increase from 2013 onward, accompanied by lower UF and less sodium sieving. Progressive UF insufficiency was present from 2015. No decrease was found for CA 125. A laparotomy for surgical replacement was performed in August 2019 because of an injury of the external part of the catheter in close proximity to the exit site. The intraoperative findings included a stiff mesentery, mural peritoneal invasions, and a serous effusion around the catheter, necessitating its withdrawal. Postoperative CT scan showed localized peritoneal thickening in less than 20% of peritoneal tissue, accompanied by calcifications in 20%, mild bowel tethering, a pelvic fluid collection, and increased density of abdominal fat (Figure 1(a)). A peritoneal biopsy confirmed thickening of the submesothelial layer, microvasculopathy, and calcifications (Figure 1(b)). A diagnosis of localized encapsulating peritoneal sclerosis (EPS) was made, the patient was transferred to HD and treated with prednisone and tamoxifen.
Changes in parameters of peritoneal water and solute transport assessed by 3.86% glucose PET over the time on peritoneal dialysis.
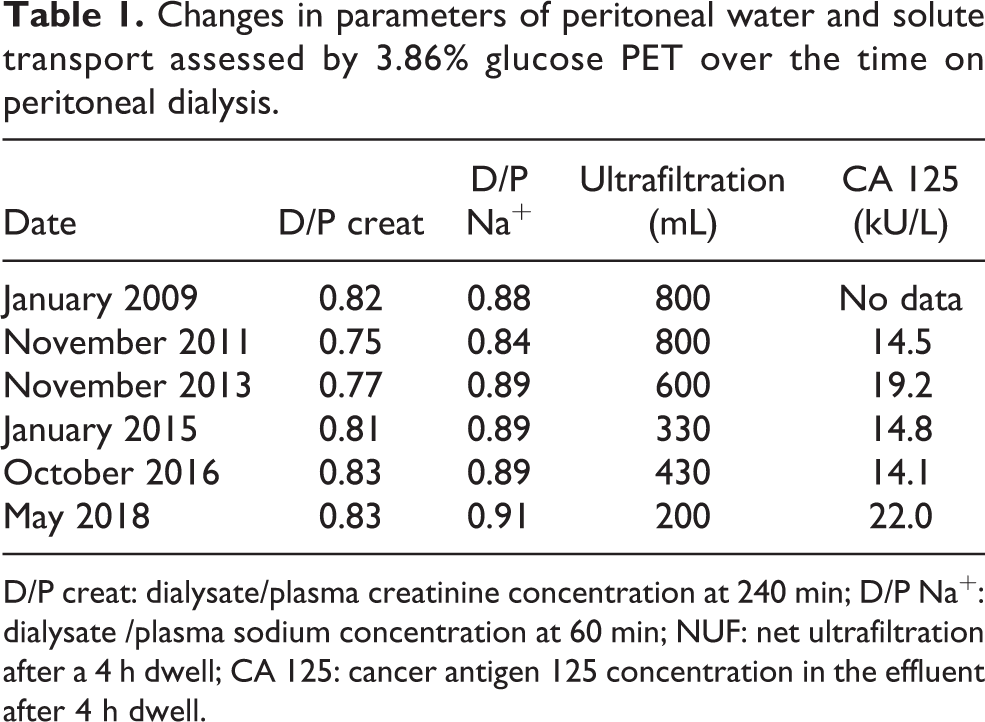
D/P creat: dialysate/plasma creatinine concentration at 240 min; D/P Na+: dialysate /plasma sodium concentration at 60 min; NUF: net ultrafiltration after a 4 h dwell; CA 125: cancer antigen 125 concentration in the effluent after 4 h dwell.
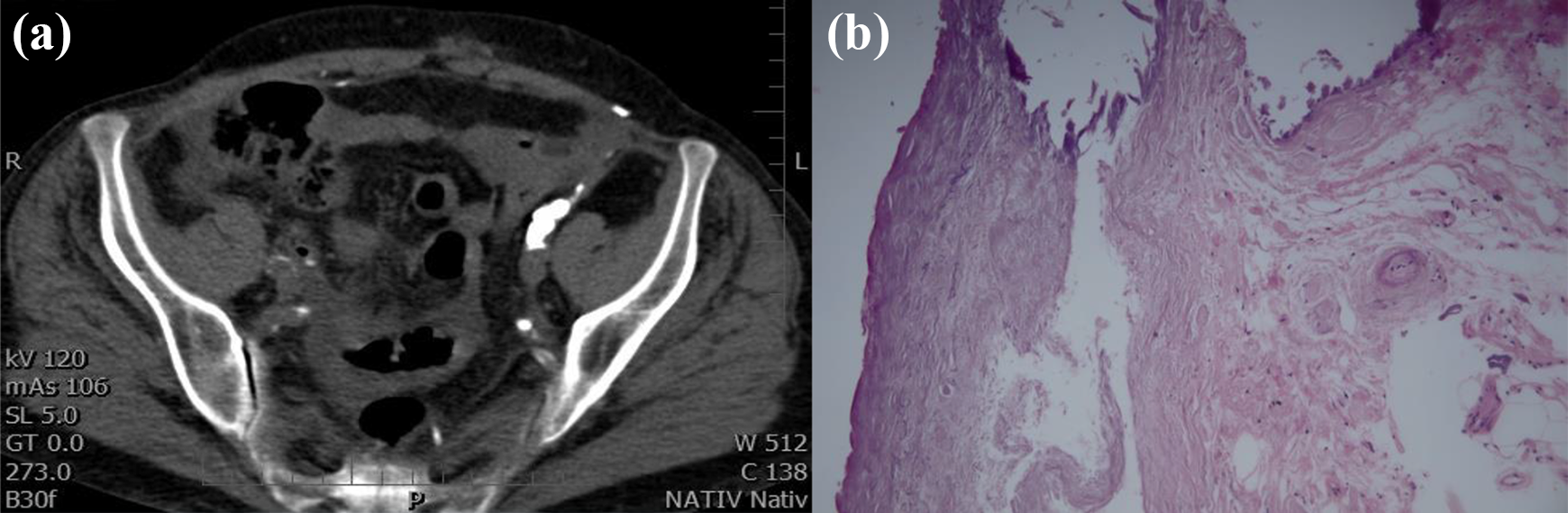
(a) Abdominal CT scan showing irregularly thickened peritoneum with coarse calcifications medial to the caudal portion of the iliopsoas muscle on the left. Discrete fat stranding of mesenterial fat, calcifications in the iliac vessels, and free fluid are present. No signs of bowel obstruction are visible. (b) Hematoxylin-stained peritoneal biopsy showing some mesothelial cells (upper left), submesothelial fibrosclerosis, interstitial fibrosis, calcification on the top and microvasculopathy on the right.
Peritoneal morphology
Until recently, information on the normal structure of peritoneal tissues was based on scarce observations in a small number of individuals. A detailed description of quantitative peritoneal histomorphometry in a large number of children and adults was published in 2016. 9 The density of blood capillaries in adults increased with age, while the endothelial thickness decreased. No effect of age was found for other vascular properties, submesothelial thickness, and lymphatic density.
An inherent problem with the interpretation of morphologic studies in long-term PD patients is their cross-sectional nature. Longitudinal analyses are usually absent except for one study in which 24 incident pediatric patients (prior to PD) and PD patients underwent a follow-up peritoneal biopsy after a median duration of 13 months. 10 Data on follow-up biopsies in long-term adult patients are not available. Six studies on the development of peritoneal alterations in adult patients are summarized in Table 2. Taken together, the morphological analyses show the progressive development of peritoneal remodeling with the duration of PD using conventional dialysis solutions.
Morphologic peritoneal abnormalities in long-term PD patients on conventional dialysis solutions.a
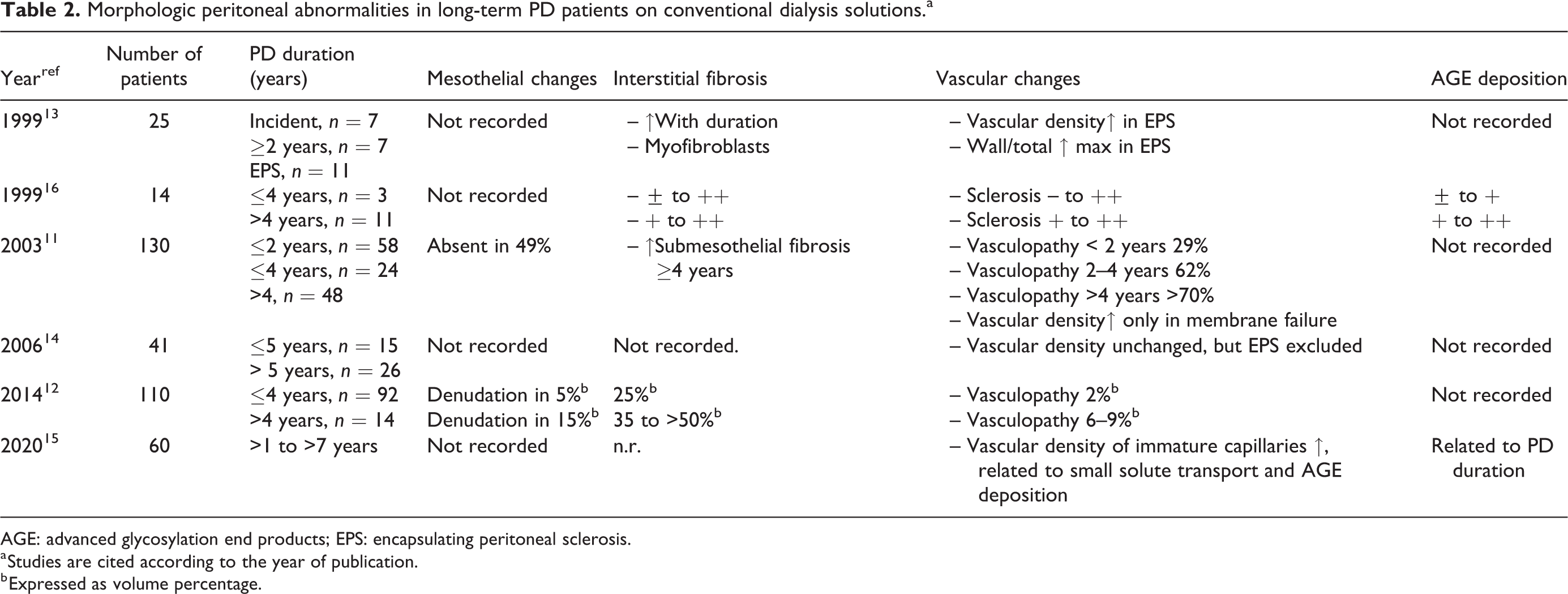
AGE: advanced glycosylation end products; EPS: encapsulating peritoneal sclerosis.
a Studies are cited according to the year of publication.
b Expressed as volume percentage.
Six studies on peritoneal morphology during PD with exposure to L-GDP/N-pH solutions have been published, two of which are in children. 10,17 The latter analyses were done in the same large population and comprised a comparison with nondialyzed children with CKD stage 5 and a follow-up biopsy in 12% of all biopsies. One-third of the patients received PD for more than 2 years and 16% for more than 4 years. Mesothelial thickness was especially decreased in children treated for more than 4 years and peritoneal blood vessel density was higher in children on PD compared to those with CKD5 but without evident progression. Remarkably, the lumen/vessel diameter (L/V) ratio was not different between CKD5 and PD, irrespective of its duration. Previous peritonitis was only associated with increased submesothelial thickness and vascular density compared to controls in patients with a PD duration of at least 4 years. 17
Comparisons between L-GDP/N-pH and conventional solutions were made in adult dialysis populations. 18 –21 These are summarized in Table 3. It can be concluded that all studies in patients treated with L-GDP/N-pH solutions showed better preservation of mesothelial cell integrity, less peritoneal submesothelial thickness, and a reduction of the severity of vasculopathy and AGE deposition, compared with those on conventional fluids. Increased vascular density was present in some but not in all analyses. However, it should be noticed that submesothelial fibrosis, vasculopathy, and AGE deposition still occurred despite the lower GDP content of PD solutions used.
Morphologic differences between long-term treatment with conventional and low ↑GDP neutral pH dialysis solutions.a
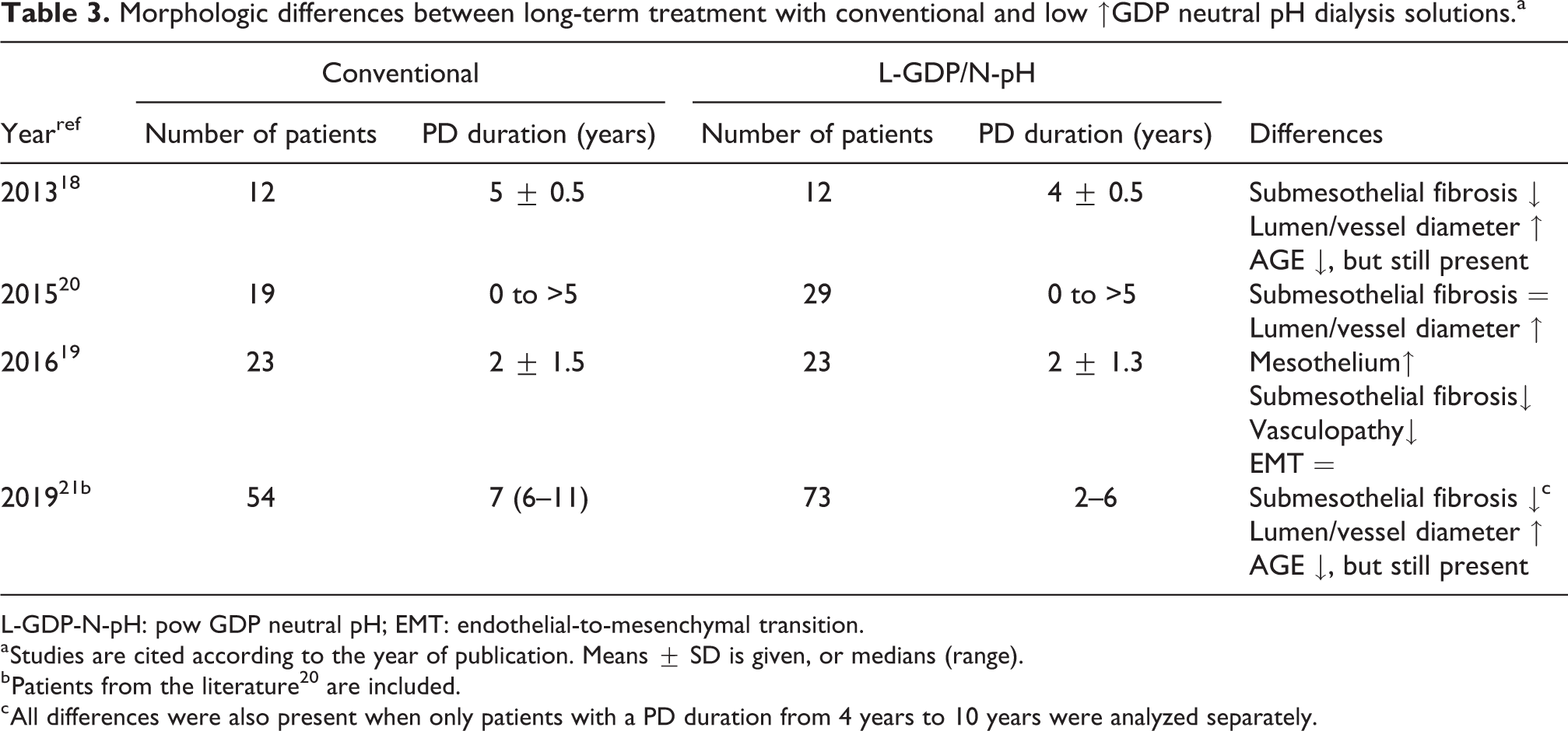
L-GDP-N-pH: pow GDP neutral pH; EMT: endothelial-to-mesenchymal transition.
a Studies are cited according to the year of publication. Means ± SD is given, or medians (range).
b Patients from the literature 20 are included.
c All differences were also present when only patients with a PD duration from 4 years to 10 years were analyzed separately.
Time course of peritoneal solute and fluid transport
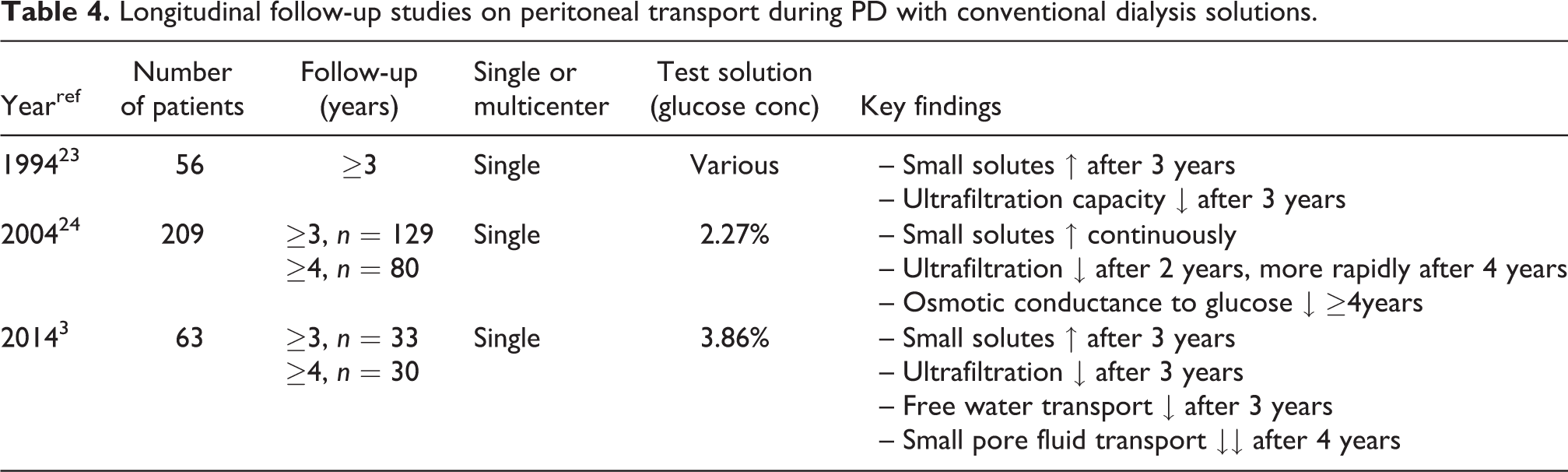
In contrast to morphological studies, longitudinal follow-up of peritoneal solute transport parameters is possible when standardized dialysis dwells and dialysate tonicity are used. Most attention has traditionally been given to small solutes like creatinine and urea. Their transfer from the microcirculation to the dialysate is mainly by diffusion through small interendothelial pores and therefore by the number of perfused peritoneal microvessels, often summarized as the effective peritoneal surface area. 22 Three longitudinal studies have been published on the time course of small solute transport during PD with conventional dialysis solutions, as summarized in Table 4. 3,23,24 They all showed an increase of D/P creatinine or its mass transfer area coefficient (MTAC) after a follow-up of 2–3 years, pointing to an enlargement of the effective peritoneal surface area. This enlargement also influences the absorption of dialysate glucose into the circulation, leading to a rapid disappearance of the crystalloid osmotic gradient. No evidence exists that the diffusion of small solutes is directly influenced by the mesothelial layer or by fibrotic interstitial changes.
Longitudinal follow-up studies on peritoneal transport during PD with conventional dialysis solutions.
Transcapillary ultrafiltration (TCUF) is the main determinant of net UF, that is, the difference between the drained and the instilled dialysate volume. TCUF of water with dissolved solutes occurs by interendothelial pores, small pore fluid transport (SPFT), which is largely dependent on the hydrostatic pressure gradient. 25 In addition, water without solutes leaves the circulation by the intraendothelial water channel aquaporin-1 (AQP-1). 26,27 This free water transport (FWT) is dependent on the crystalloid osmotic pressure gradient. FWT explains the decrease of the dialysate sodium concentration by dilution, the so-called sodium sieving, 28 which can be used in clinical practice for assessment of FWT. 29 Calculating the sodium clearance allows simultaneous assessment of SPFT. 30
The first longitudinal study on the time course of fluid transport published in 1994 showed a progressive decline of net UF after 3 years on PD. 23 This was related to an increase of the D/P or MTAC creatinine, suggesting a rapid disappearance of the crystalloid osmotic gradient. Shortly thereafter, similar results were published in prospective studies from Japan 31 and the UK; the latter in a large number of incident PD patients. 32 The longitudinal studies on peritoneal transport are summarized in Table 4. The inverse relationship between net UF and D/P creatinine is different in long-term patients because the decrease in net UF was more than one would anticipated bases on an increase in D/P creatinine alone. 24 This phenomenon has been interpreted as an impaired osmotic conductance to glucose but may in retrospect also have been caused by a reduction in FWT. A separate prospective longitudinal analysis of the time course of SPFT and FWT confirmed this assumption because both decreased after 3–4 years on PD. 3
All studies cited above were performed with conventional dialysis solutions. Based on the results of the first randomized trial done in prevalent PD patients, no important differences in fluid and small solute transport were found between the patients treated with L-GDP/N-pH and those with conventional solutions. 33 This first study was followed by a number of others, summarized in a study from central Europe, 34 which either showed no differences in the transport of small solutes and net UF or somewhat lower net UF values in patients treated with L-GDP/N-pH solutions during short-term follow-up. The multicenter randomized clinical trial balANZ in almost 200 incident PD patients with a follow-up of 2 years showed stability of D/P creatinine and net UF in those randomized to the L-GDP/N-pH solution, while D/P creatinine increased and net UF decreased in the controls. 35
A more pathophysiologic approach with special emphasis on the initial 3 months of treatment in incident CAPD patients and a crossover design after 6 weeks allowed further insights into the early effects of a dialysis regimen, consisting of a combination of one icodextrin-based solution for the long dwell combined with one amino acid-based and two L-GDP/N-pH glucose-based solutions (NEPP). 36 The NEPP treatment was associated with higher values of D/P creatinine compared to the controls and higher effluent levels of dialysate CA 125, interleukin-6 (IL-6), and vascular endothelial growth factor. The results of plasma concentrations of GDPs were variable, 37 while C-reactive protein concentrations showed no consistent results. 38 Although unlikely, a contribution of the amino acid exchange to the observed differences cannot be excluded with certainty. 39 Recently, two large studies were published on changes in peritoneal transport during long-term follow-up for more than 4 years. 40,41 The results of these and the balANZ study are summarized in Table 5. The initially lower UF reported in the study from The Netherlands 41 confirmed the results of the NEPP study 36 and those of a previous study from Canada. 42 This effect lasted up to 3 years. Thereafter, the MTAC creatinine increased 2.7 mL/min/year and glucose absorption 4.6% per year in the conventional group, which coincided with a marked decrease in sodium sieving and FWT. Both parameters remained stable in the L-GDP/N-pH group. SPFT showed a gradual decrease during the first 4 years in both groups. Peritonitis induced a decrease of TCUF after 2 years in the conventional group, which was absent in the patients on L-GDP/N-pH solutions. No effect of peritonitis on other transport parameters was found in the two patient groups.
Longitudinal follow-up studies on peritoneal transport in incident PD patients comparing conventional with low GDP neutral pH dialysis solutions.
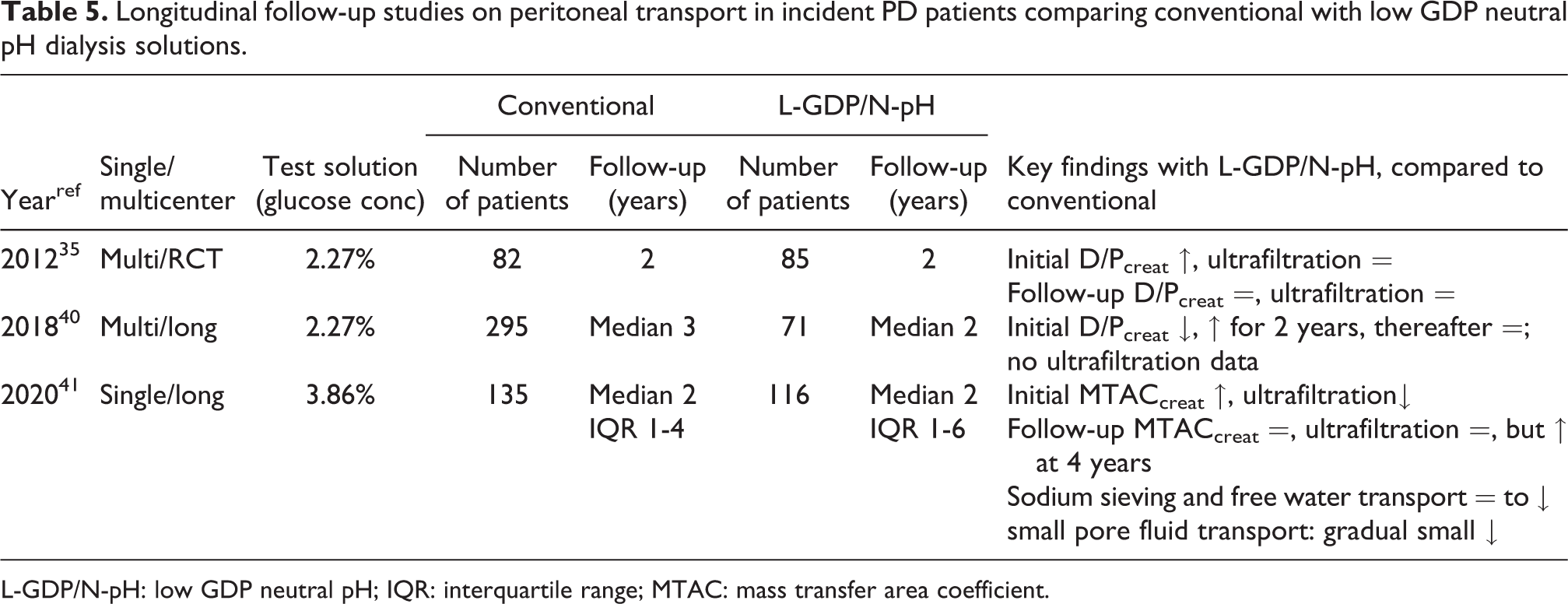
L-GDP/N-pH: low GDP neutral pH; IQR: interquartile range; MTAC: mass transfer area coefficient.
Taken together, long-term PD with conventional dialysis solutions leads to an increase of the effective peritoneal surface area and impaired UF. The latter is partly due to a decrease in FWT, caused by a rapid disappearance of the glucose-induced crystalloid osmotic pressure gradient, but also by a reduction of SPFT, possibly due to a decreased hydrostatic pressure gradient as a consequence of vasculopathy. 43 Peritonitis episodes may modify some of the effects of exposure. 40,41,44 In contrast, the long-term changes in small solute transport and FWT were minor with L-GDP/N-pH solutions and independent of peritonitis, although SPFT still declined with time. It is speculative if the latter is caused by vascular deposition of AGEs, leading to narrowing of vascular lumina. The initially higher small solute transport rates were not reported in all studies, possibly due to heterogeneity of the population investigated. Initially, higher solute transport rates observed with L-GDP/N-pH solutions have been postulated to be due to higher production rates of vasoactive mediators due to less inhibition of peritoneal cell functions, as has been shown in vitro. 45
Peritoneal effluent biomarkers
Peritoneal effluent after drainage of the dialysis solution contains proteins and peptides that may reflect the health and integrity of peritoneal tissues. Longitudinal data are available for CA 125, IL-6, and plasminogen activator inhibitor type 1 (PAI-1). All three can be measured as proteins in effluent and as the expression of their transcripts in effluent cells. 46 The current knowledge on all three has been reviewed recently. 47 Associations between the above-mentioned markers and peritoneal transport are discussed below, and associations with peritoneal morphology are not available.
Dialysate CA 125 originates from mesothelial cells and its dialysate appearance rate is related to its gene (MUC 16) expression in effluent cells. Peritonitis causes a moderate transient increase lasting over days. 48 Effluent CA 125 decreases with PD duration, 49 which corresponds to the mesothelial denudation described in morphological analyses. 11,12 Treatment with L-GDP/N-pH dialysis solutions is associated with higher effluent CA 125 levels than with conventional ones during a maximal follow-up of 2 years. 50 –52 However, unpublished observations (Coester AM. PhD Thesis, University of Amsterdam, 2010) suggest that CA 125 also shows a decrease with dialysis duration using L-GDP/N-pH fluids only.
The dialysate concentrations of IL-6 are often higher than in the circulation due to local production by peritoneal cells. However, no upregulation of its gene could be detected in peritoneal cells, while no relationship was present between gene expression and effluent concentrations. 42,43 The combination of this finding, together with the high intraindividual variability of effluent IL-6 which averages 28%, 53 suggests that local intraperitoneal factors are important determinants of its concentration. Transport from the circulation will also contribute. Therefore, the relationships reported in cross-sectional studies between small solute transport and dialysate IL-6 are all biased by mathematical coupling. 54 This is present because peritoneal transport affects both dialysate small solute and effluent IL-6 concentrations. An increasing trend for IL-6 has been reported during the first 2 years of the treatment. 53,55,56 The results of using L-GDP/N-pH solution in the first month of PD on effluent IL-6 are not uniform. Higher levels were reported in the NEPP study, 36 but no difference was present in the Global Fluid Study. 40 Therefore, no evidence is currently available that effluent IL-6 is influenced by the amount of GDPs in the dialysis solution.
PAI-1 is the most promising effluent biomarker. Its appearance rate is related to the expression of the SERPINE 1 gene in effluent cells. 42,43 PAI-1 is involved in various fibrosing processes by inhibition of fibrinolysis. Transport from the circulation accounts for about one-fourth of the effluent concentration, the reminder is locally produced. Among others, PAI-1 production is stimulated by high glucose concentrations. 57 The SERPINE 1 gene expression by effluent cells was mildly increased in PD patients after 2 years. 42 Effluent PAI-1 in PD patients on a L-GDP/N-pH dialysis solution was related to FWT and showed an increase with dialysis duration, irrespective of whether conventional or L-GDP/N-pH dialysis fluids were used. 42,58 Furthermore, dialysate PAI-1 is a predictor of EPS. 59
L-GDP/N-pH solutions and EPS
EPS is a rare but very serious complication of long-term PD. The discrepancy between the incidence of severe fibrosis and EPS is the reason that a second hit, for example, a peritonitis episode, has been suggested for the development of the clinical picture of EPS with bowel obstruction. 60 The importance of a second hit is illustrated in the development of EPS in two patients on L-GDP/N-pH solutions, one already after 1 year on PD after severe peritonitis, the other following abdominal surgery. 61 Yet it is impossible to identify the second hit in all EPS patients. The condition is macroscopically characterized by thick fibrous bands and extensive adhesions. Light microscopy shows extensive interstitial sclerosing type fibrosis often with myofibroblasts 13 and an abundance of collagen fibers. 62 Relationships have been found between myofibroblasts, the deposition of collagen IV, and vascular density. 13 UF failure is almost always present, especially due to impaired FWT, 62,63 despite normal AQP-1 expression. 62 This marked decrease in FWT, which is also observed in long-term PD on conventional solutions, is probably caused by the development of interstitial fibrosis. 64 The pathophysiological mechanism is still speculative. However, the reduction in submesothelial fibrosis during the treatment with L-GDP/N-pH solutions, which was found in almost all morphological studies and the stability of FWT in the patients on L-GDP/N-pH therapy, suggest a cause/effect relationship. This has been confirmed by clinical observations. The center of one of the authors (RTK) abandoned conventional dialysis solutions completely in 2004. This had a marked effect on EPS incidence, which was 3.5 per 1000 patient-years, 65 to almost zero 66 with the exception of one patient with Alport syndrome, which is a collagen IV disease. 67 Since then, almost all dialysis centers in The Netherlands switched to L-GDP/N-pH solutions. In time, this was associated with a marked reduction of EPS. 68 Similar associations have been reported from Japan 69 and Germany. 70 Therefore, it can be concluded that the main advantage of PD with L-GDP/N-pH dialysis solutions may be the reduction and delay of functional and morphologic alterations, but not complete obliteration, that can occur in long-term PD, possibly preventing EPS.
Lessons from the case history and concluding remarks
The patient developed some decrease in sodium sieving during follow-up and a slight decrease of effluent CA 125 on conventional solutions. However, the sensitivity of CA 125 to predict EPS is only 63%. 59 The switch to L-GDP/N-pH solutions after 8 years of PD on conventional fluids had no effect on peritoneal fluid and solute transport but was associated with some increase in CA 125, while some mesothelial cells were still present. Lubrication of peritoneal tissues is the most important function of the mesothelium, preventing the formation of adhesions. This may explain why the patient had no symptoms of bowel obstruction, despite the other microscopic findings. The L-GDP/N-pH solutions were not associated with regression of fibrosis and vasculopathy in this patient but the switch to these possibly prevented important morbidity. These findings are in accordance with results of an RCT, 71 a systematic review and meta-analysis 72 and a Cochrane analysis, 73 that all failed to show an effect of L-GDP/N-pH solutions on mortality and technique survival. But none of these included a detailed analysis of the effects on peritoneal morphology and the time course of peritoneal function with regard to UF and small solute transport, including biomarkers in peritoneal effluent. It can be concluded from the current analysis that indicating L-GDP/N-pH dialysis solutions as biocompatible solutions is incorrect, because they still induce peritoneal alterations although less severe and after prolonged treatment. Such delay can be very important for individual patients. In the absence of side effects, the use of L-GDP/N-pH solutions may be preferable over conventional dialysis fluids, but for both solution types, reducing the peritoneal exposure to high glucose concentrations is important.
Footnotes
Acknowledgments
None.
Authorship
All authors agree with the sequence of authors.
Informed consent to participate
All authors provide consent.
Informed consent to publish
All authors agree with submission in its present form.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
None.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.