
Abstract
Background:
Peritoneal dialysis (PD) can offer more flexibility and independence compared with hemodialysis, yet uptake of PD remains low. Barriers to PD include the fear of dialyzing without medical assistance and uncertainty about recognizing and managing complications. There is increasing use of remote monitoring in automated peritoneal dialysis (APD), but little is known about its acceptability by patients and caregivers. We aimed to describe patients’ and caregivers’ expectations and experiences of remote monitoring for APD.
Methods:
Qualitative study design, using semi-structured face-to-face interviews of patients who either receiving PD or were considered eligible for PD, and their caregivers. Transcripts were analyzed using thematic analysis.
Results:
Of the 34 participants, 27 were patients and the remainder caregivers. Four themes (with subthemes) were identified reducing patient burden (seeking reassurance and shared responsibility, convenience and accuracy); strengthening partnerships in care (empowering knowledge and understanding, increased accountability to dialysis team); improving access to treatment (saving time and money, providing timely care and avoiding hospital); and preserving quality patient–provider interactions (enhancing face-to-face contact, clarifying expectations of access and use of data).
Conclusions:
Remote monitoring may increase patient knowledge about their kidney disease and its treatment, encourage accountability to the clinical team, enhance partnerships with clinicians, and improve access to treatment and timely care. It is also important to ensure that remote monitoring does not replace face-to-face clinical contact with clinicians.
Keywords
Background
Compared with hemodialysis (HD), peritoneal dialysis (PD) has a number of advantages for patients including increased flexibility and freedom and ability to maintain employment. 1 –3 Automated peritoneal dialysis (APD) offers additional advantages than continuous ambulatory peritoneal dialysis (CAPD) including day-time freedom, 4 improved fluid balance, and lower risk of peritonitis. 5,6 Yet, overall, the uptake of PD remains low in most countries. 1
Barriers include patients’ fear of catastrophic events on PD, and perceived lack of medical support, and concerns among clinicians that patients may not be able to monitor or manage complications. 1,2,4 To address these, there has been increasing use of remote monitoring. Remote monitoring is integrated in some APD machines, which allows for electronic transfer of data from APD machines to the PD clinical team who can access treatment data transfer, follow trends in data, and modify dialysis prescriptions and management patients’ dialysis remotely. Studies have shown that RPM in APD is associated with reduced hospitalizations, 7 emergency room visits and unplanned clinic visits, 8 risk of infection, which can result in substantial cost savings. 2 Patients have also reported that RPM increased their confidence to dialyze independently. 9
Although there are a number of studies that support remote monitoring for patients with chronic conditions, 10 there has been limited research of patients’ experiences with remote monitoring on PD. 11 This study aims to describe the perspectives, expectations, and experiences of patients on APD or who are eligible for APD and their caregivers. This may inform strategies to optimize RPM in APD to improve acceptability and uptake and maximize its potential for improving patient satisfaction and outcomes.
Methods
This study is reported according to the COnsolidated criteria for REporting Qualitative research (COREQ) 12 (Supplementary Material 1).
Context
Participant recruitment and selection
Patients who had experience with PD, both with and without remote monitoring, and patients who were acute starts and on HD who were clinically appropriate for PD and their caregivers were eligible to participate. We used purposive sampling to ensure diversity based on demographics and clinical characteristics including dialysis modality (CAPD, APD, and HD). Participants were excluded if they were not eligible for PD, did not speak English, or were able to consent. All participating sites provided ethical approval.
Data collection
Participants were interviewed face-to-face at home or a clinic room based on their preference. The interview guide was developed from review of the literature 10,11 and discussion among the research team. Topics included knowledge, perspectives, and experience of remote monitoring; views on the advantages and disadvantages of remote monitoring; and suggestion for how RPM could support patients receiving PD (Supplementary Material 1). First author (RCW), a nurse practitioner, and author (ND), a PD nurse, both with experience in qualitative research and PD, conducted the interviews. Six patients interviewed were known to either interviewer. Seven invited participants declined to participate two participants because they were unwell and five participants had other commitments or were not interested. Interview times ranged from between 38 min and 64 min. We conducted interviews until data saturation, defined as when no new data emerged. Field notes were taken after each interview. All interviews were recorded and transcribed verbatim.
Data analysis
Author RCW entered transcripts into the software program HyperRESEARCH version 3.7.2 (ResearchWare Inc). This software is designed to manage qualitative data. Analysis was conducted using thematic analysis. 13 RCW coded the transcripts line-by-line, identifying concepts inductively, and grouped similar concepts specific to patient and caregiver expectations, perspectives, and experiences of remote monitoring. Investigator triangulation was performed by two other authors (ND and SCP) who also reviewed the transcripts to ensure all themes captured the range and depth of data. Later, all authors reviewed the preliminary themes to ensure that the findings captured the full breadth and range of data.
Results
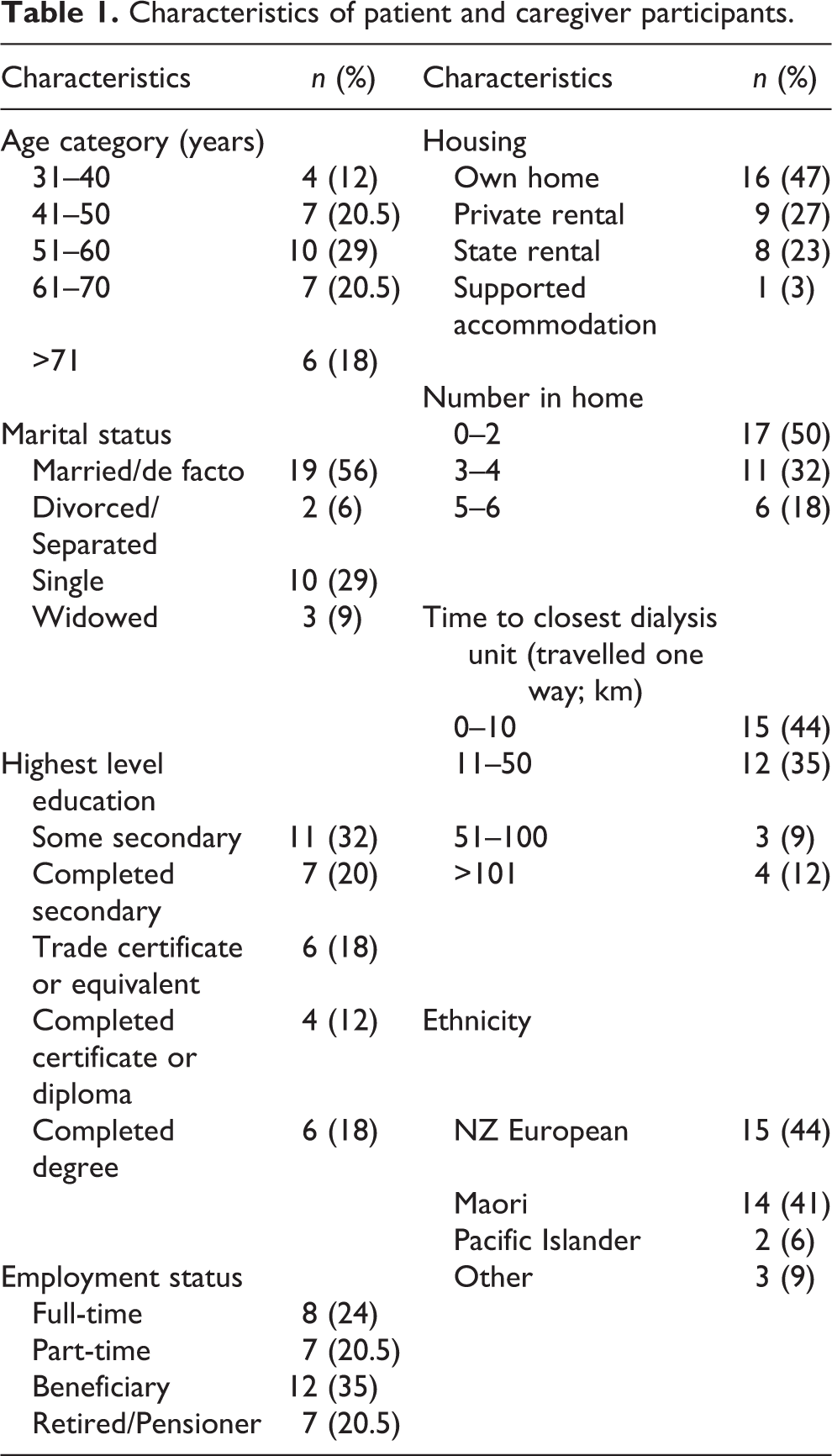
The 34 participants included 15 patients on APD and with experience of RPM, 7 patients on CAPD without experience of RPM, 7 caregivers of patients on APD using remote monitoring, and 5 patients on HD who were suitable for APD but had chosen HD. Participant characteristics are presented in Table 1. The age of participants ranged from 31 years to 76 years. Over half were married; 15 (44%) were in full- or part-time employment and 16 (48%) had vocational or university qualifications.
Characteristics of patient and caregiver participants.
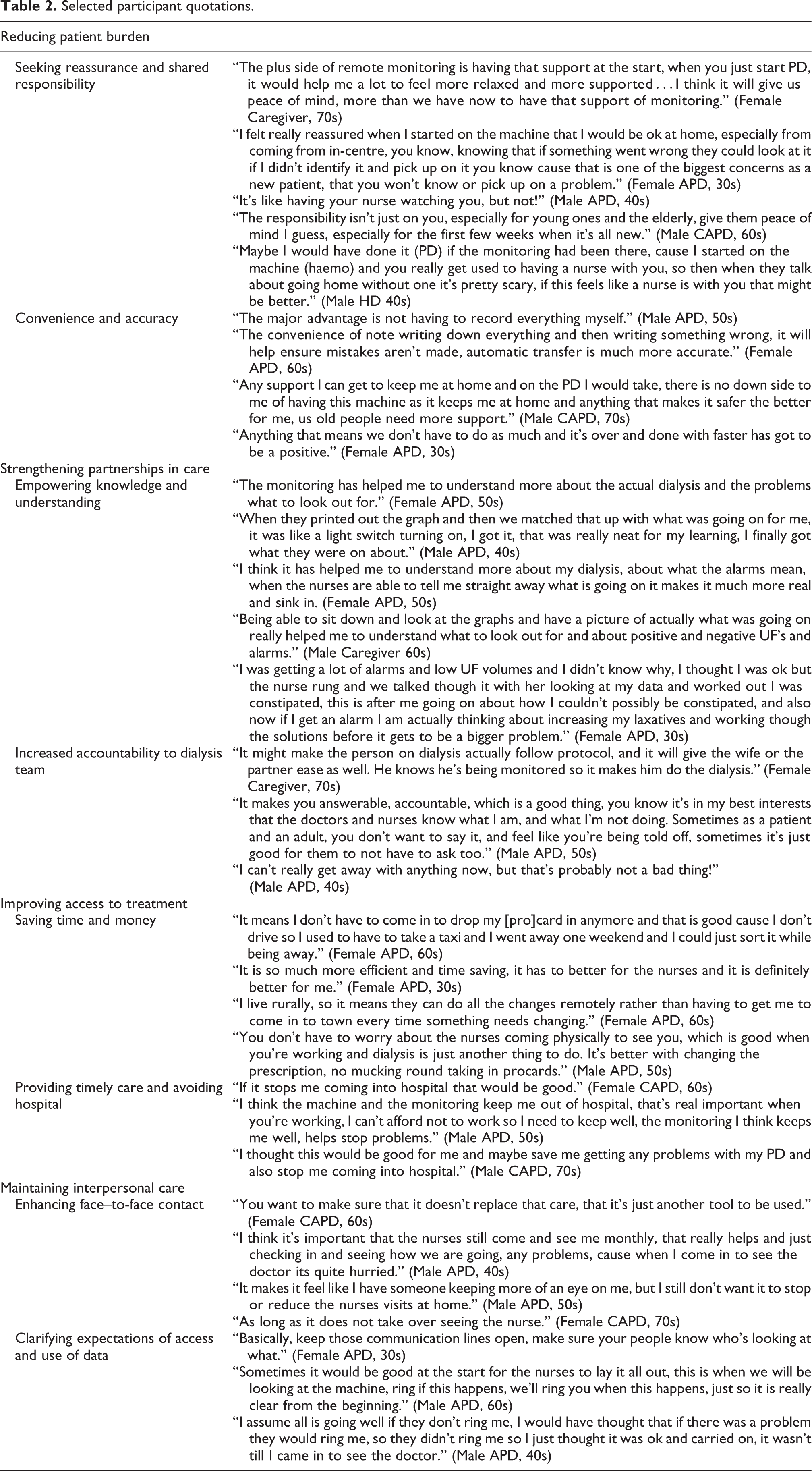
We identified four main themes reducing patient burden, strengthening partnerships in care, improving access to treatment, and preserving quality patient–provider interactions. The respective subthemes are described below. Illustrative quotations are provided in Table 2, and the conceptual links among themes are shown in Figure 1.
Selected participant quotations.
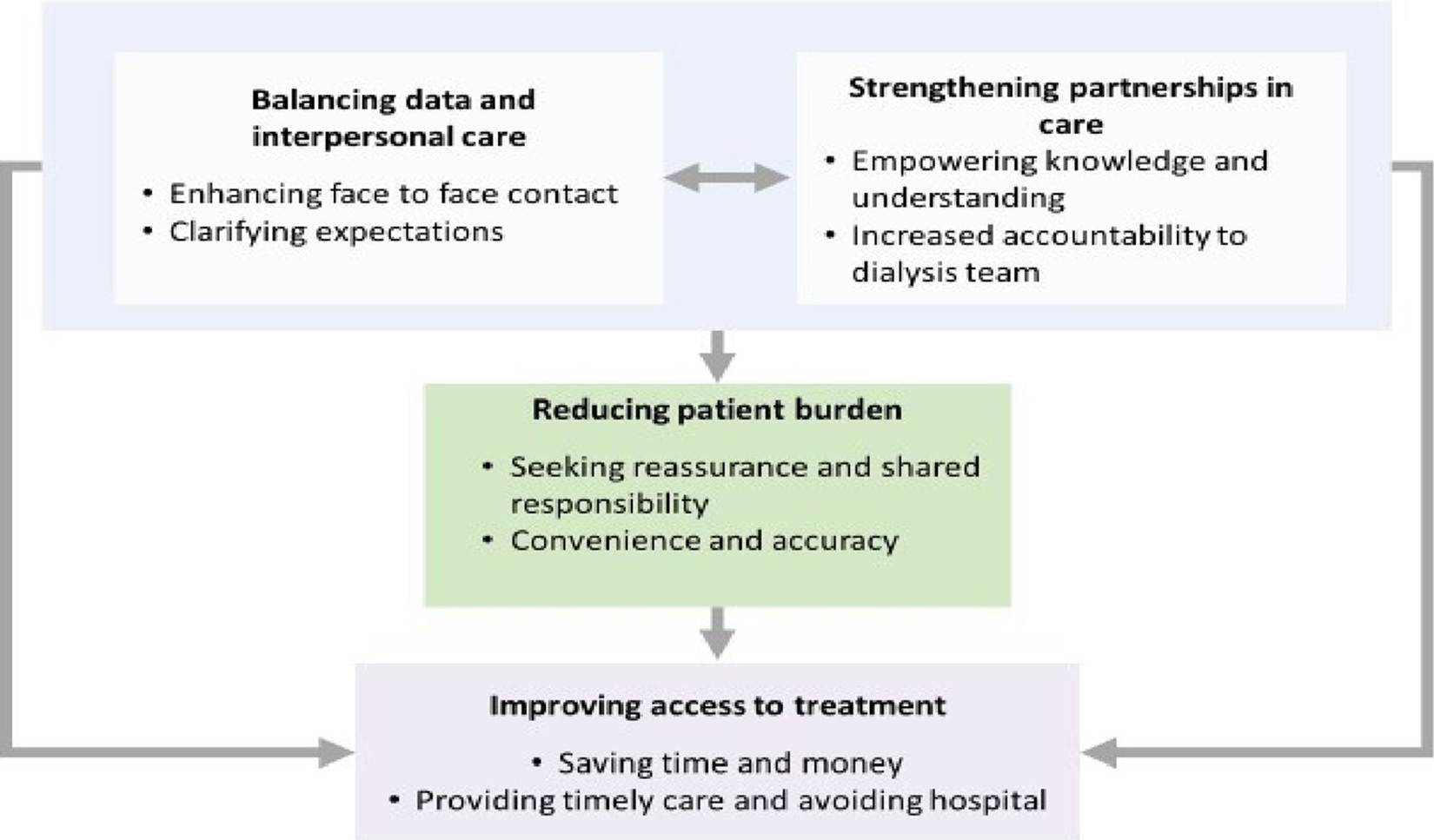
Thematic schema of patients’ and caregivers’ perspectives, expectations, and experiences of remote monitoring in peritoneal dialysis. Note: Remote monitoring assists in knowledge acquisition and improved understanding of the disease and its treatment for patients. Remote monitoring increased patient accountability to the clinical team and enhanced partnerships between patients, caregivers, and clinicians leading to improved access to treatment and timely care, and saving time and money. The reassurance, sense of shared responsibility and convenience and accuracy achieved through remote monitoring helps to reduce some of the burden of independent dialysis. Patients and caregivers, however, cautioned of the importance of maintaining interpersonal care by clarifying expectations through clear communication and using remote monitoring to enhance, not replace face-to-face contacts.
Reducing patient burden
Seeking reassurance and shared responsibility
Some patients felt remote monitoring provided reassurance in case they missed an “important alarm that meant I missed something, and my tube had to be taken out” (Female APD, 60s). This was more apparent in patients who were transitioning to home dialysis and in older patients. Participants who had experienced remote monitoring felt “more relaxed and supported, (be)cause you’ve got that constant help in form of someone seeing your data” (Caregiver APD, 60s), similar to having a “nurse watching you” (Male APD, 60s). This also relieved some pressure of feeling solely responsible for their treatment.
Convenience and accuracy
Some patients appreciated the convenience of RPM because they no longer needed to record their dialysis information manually and the “mundane work that adds to the burden of PD” (Male APD, 50s). Participants also believed automated transfer of data improved the accuracy of data reporting and could have potential for collecting and transferring other data, for example blood pressure, weight, and dialysate strength through remote monitoring.
Strengthening partnerships in care
Empowering knowledge and understanding
Some believed that remote monitoring helped them to understand the technicalities of dialysis and enabled them to manage PD on their own—“a light switch turning on, I got it, that was really neat for my learning, I finally got what they were on about” (Male APD, 40s). Some gained more confidence in knowing “what to look out for” (Female APD, 30s). Being able to discuss their data from RPM with nurses helped patients to feel that they were more involved as active partners in their care.
Increased accountability to dialysis team
Caregivers, in particular, felt that remote monitoring may motivate patients to adhere to their treatments because they knew their data were being transferred to the clinical team and therefore, they were more accountable. Participants reported some assurance in knowing the clinical team could access how much prescribed dialysis was being missed. This eased stress and uneasiness because patients no longer had to “confess how much dialysis I was missing, which is not any easy conversation to start” (Male APD, 50s). For caregivers, this also helped them to be “not seen as the one telling tales on him” (Female Caregiver, 50s).
Improving access to treatment
Saving time and money
The ability for nurses to make changes to the dialysis prescriptions remotely was perceived as both a cost and time saving to patients. This was particularly important for those who were living outside of metropolitan regions, further from dialysis units, or who did not have ready access to transportation. “I don’t have to come in to drop my (pro)card in anymore and that is good cause I don’t drive” (Female APD, 60s). Patients who lived outside metropolitan areas also saw remote monitoring as a way for them to have better access to clinical care and receive similar support to those in the city. For those who were working or had other commitments, remote monitoring reduced unnecessary clinic appointments and time.
Providing timely care and avoiding hospital
For patients, remote monitoring provided timely warnings to prevent complications and hospital admissions. Patients and caregivers who had used remote monitoring described cases when the data had prompted the nurses to contact the patient when they had noticed issues with low drain volumes, alarms or incomplete dialysis cycles, that the patient had not been aware of. Patients reported feeling more confident in contacting the clinical team when they had alarms, as they knew the nurses could match the patients concerns with the remote monitoring data “rather than me just battling on at home wondering what had happened and hoping it didn’t happen again the next night, or cause bigger problems” (Female APD, 40s).
Maintaining interpersonal care
Enhancing face to face contact
Patients were initially concerned that remote monitoring may be used to replace contact with clinicians. They emphasized that remote monitoring should be used to enhance, not replace care. Patients and caregivers valued the nursing visits particularly because this allowed them an opportunity to discuss concerns face to face and directly receive more education and support and did not want these visits reduced or replaced by technology.
Clarifying expectations of access and use of data
Patients and caregivers wanted to understand who was responsible for reviewing their data and at what time intervals it would be viewed so their roles and expectations and that the clinical team were clear. Some patients discussed being confused and concerned when they only were notified there had been a problem after the event. “I assume all is going well if they don’t ring me…they didn’t ring me, so I just thought it was ok and carried on” (Male APD, 40s). Patients and caregivers were open to sharing their PD data and believed that this could “improve the care and prevent problems” (Female CAPD, 60s). The ability to transfer data directly between the home and the hospital was regarded as safe and not “any different from sharing any other information across the hospital” (Female CAPD, 40s).
Discussion
Patients requiring PD believed that remote monitoring enabled them to gain knowledge and understanding, particularly about the technicalities of dialysis and signs and symptoms that may indicate a change in their health. With remote monitoring, patients felt more accountable to the clinical team and through having more understanding and access to data patients particularly felt empowered and a more active partner in their care. RPM was viewed as a way to improve access to treatment and timely care and saved time and cost for patients and caregivers. Participants felt remote monitoring provided more reassurance and a sense of shared responsibility and thus alleviated stress and pressure. Collectively, these were thought to alleviate, to some extent, the burden of PD. However, there were some concerns that remote monitoring may diminish face-to-face interaction with clinicians and participants wanted a clear understanding of how and when they would be communicated with regarding the RPM data.
Older patients and caregivers emphasized the importance of reassurance of being able to share responsibility for PD and to be able to be safe on PD at home. For some patients who were on HD at the time of the study, they acknowledge that these fears were the reasons for choosing HD instead of PD. Caregivers viewed that increased accountability of patients to the clinical team through remote monitoring helped to relieve some of their burden and responsibility, which in turn benefitted the patient–caregiver relationship. This is relevant given that this may be attributed to conflict and breakdown of relationships. 14 –16
It is well established that patients contemplating and performing home dialysis have concerns around safety, isolation, and support. 1,2,17,18 Addressing the patient and caregiver preference for increased support may help to allay these concerns and support patients to choose and maintain PD. Similar to another study in patients receiving HD, 11 our study has identified that remote monitoring improves patients’ sense of security and safety in dialyzing independently and gives patients and caregivers reassurance and confidence. Patients have suggested the need for more nursing support to help them choose and maintain PD; 2,4 however, this may not be possible in many settings due to resource constraints. Thus, remote monitoring potentially offers an alternative and less costly way to both the patient and the health system to support patients to feel confident and reassured that they are safe on dialysis at home.
Our results indicate that remote monitoring can empower patients and caregivers by increasing their knowledge and understanding of chronic kidney disease and dialysis. Specifically, participants were more likely to understand fluid balance, titration of medications, and consequently be more active self-managers. Patient education and self-management are fundamental aspects of PD care; however, rates of nonconcordance have been reported in up to 85% in medication adherence and 53% for dialysis exchanges. 19 Poor self-management and inadequate knowledge are associated with reduced quality of life, higher symptom burden, and outcomes. 20 Remote monitoring has potential to improve patient reported outcomes and may also support clinician recommendation and encouragement of PD. 21
Clinicians experienced with remote monitoring in PD have also noted that it can improve access to care by enabling decision-making based on real-time clinical data, adherence to dialysis, and relieving time and financial burdens. 22 Clinicians who use remote monitoring may make more proactive adjustments of dialysis prescriptions for the patients, resulting in fewer clinic visits for patients in their first six months of therapy, 23 compared with those who do not use this technology. Studies have also found that remote monitoring enabled nurses to be more proactive in patient care, rather than being reactive, which reduced the frequency and duration of clinic visits. 24
We suggested that future research evaluating remote monitoring interventions assess cost-effectiveness, quality of life, and clinical outcomes in patients on APD. This would need to include consideration of patient out of pocket costs, hospital admission, and health-care utilization. It may also be worthwhile comparing the out of pocket costs between urban and rural patients.
In our study, we included reasonably diverse patients with and without direct experience of remote monitoring. We achieved data saturation, and through member checking and investigator triangulation, we can confirm that the findings reflect the full range and depth of the data collected. However, there are some potential limitations. The study was conducted in New Zealand, a country with a higher than average rate of PD; therefore, the transferability of the findings to countries with low rates of PD may be limited. Also, only English-speaking patients and caregivers were included.
Remote monitoring may improve knowledge acquisition and understanding of kidney disease and its treatment in patients on APD. It may also encourage patient accountability to the clinical team and enhance patient–clinician partnerships, leading to improved access to treatment and timely care, potentially saving both patient and provider time and money. It is also important, however, that remote monitoring enhances rather than replaces face-to-face clinical contact with clinicians.
Supplemental material
Supp_mat_1 - Patients’ and caregivers’ expectations and experiences of remote monitoring for peritoneal dialysis: A qualitative interview study
Supp_mat_1 for Patients’ and caregivers’ expectations and experiences of remote monitoring for peritoneal dialysis: A qualitative interview study by Rachael C Walker, Allison Tong, Kirsten Howard, Natasha Darby and Suetonia C Palmer in Peritoneal Dialysis International
Supplemental material
Supp_mat_2 - Patients’ and caregivers’ expectations and experiences of remote monitoring for peritoneal dialysis: A qualitative interview study
Supp_mat_2 for Patients’ and caregivers’ expectations and experiences of remote monitoring for peritoneal dialysis: A qualitative interview study by Rachael C Walker, Allison Tong, Kirsten Howard, Natasha Darby and Suetonia C Palmer in Peritoneal Dialysis International
Footnotes
Acknowledgements
The authors thank the people who participated in this study and the units who assisted in patient recruitment.
Author contributions
RCW researched literature, conceived the study, and wrote the first draft of the manuscript. All authors were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We have read and understood Peritoneal Dialysis International’s policy on conflicts of interest disclosure and declare the following interests Dr Walker was supported by a Baxter Clinical Evidence Research Council Grant to conduct this study. The funder of this study had no role in the study design or data analysis.
Ethical approval
Ethical approval for this study was obtained from the Health and Disability Ethics Committees—Low Risk Waiver, Canterbury District Health Board, Localities Committee (RO# 18088), and Hawke’s Bay District Health Board, Localities Committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article This study was supported by a Baxter Clinical Evidence Research Council Grant.
Informed consent to participate
Written informed consent was obtained from all subjects before the study.
Informed consent to publish
Written informed consent was obtained from the participants for their anonymized information to be published in this article.
Trial registration
Australian New Zealand Clinical Trials Registry—ACTRN12617001617358.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.