
Abstract

Lay summary
The International Society for Peritoneal Dialysis last published a guideline on prescribing peritoneal dialysis (PD) in 2006. This focused on clearance of toxins and used a measure of waste product removal by dialysis using urea as an example. This guideline suggested that a specific quantity of small solute removal was needed to achieve dialysis ‘adequacy’. It is now generally accepted, however, that the well-being of the person on dialysis is related to many different factors and not just removal of specific toxins. This guideline has been written with the focus on the person doing PD. It is proposed that dialysis delivery should be ‘goal-directed’. This involves discussions between the person doing PD and the care team (shared decision-making) to establish care goals for dialysis delivery. The aims of these care goals are (1) to allow the person doing PD to achieve his/her own life goals and (2) to promote the provision of high-quality dialysis care by the dialysis team.
Key recommendations
PD should be prescribed using shared decision-making between the person doing PD and the care team. The aim is to establish realistic care goals that (1) maintain quality of life for the person doing PD as much as possible by enabling them to meet their life goals, (2) minimize symptoms and treatment burden while (3) ensuring high-quality care is provided. The PD prescription should take into account the local country resources, the wishes and lifestyle considerations of people needing treatment, including those of their families/caregivers’, especially if providing assistance in their care. A number of assessments should be used to help ensure the delivery of high-quality PD care.
Patient reported outcome measures – this is a measure of how a person doing PD is experiencing life and his/her feeling of well-being. It should take into account the person’s symptoms, impact of the dialysis regimen on the person’s life, mental health and social circumstances.
Fluid status is an important part of dialysis delivery. Urine output and fluid removed by dialysis both contribute to maintaining good fluid status. Regular assessment of fluid status, including blood pressure and clinical examination, should be part of routine care.
Nutrition status should be assessed regularly through evaluation of the patient’s appetite, clinical examination, body weight measurements and blood tests (potassium, bicarbonate, phosphate, albumin). Dietary intake of potassium, phosphate, sodium, protein, carbohydrate and fat may need to be assessed and adjusted as well.
Removal of toxins. This can be estimated using a calculation called Kt/Vurea and/or creatinine clearance. Both are measures of the amount of dialysis delivered. There is no high-quality evidence regarding the need or benefit associated with the achievement of a specific target value for these measures. The amount of kidney function that continues to remove waste products and the remaining urine volume should be known for all individuals doing PD. Management should focus on preserving this as long as possible. For some people who require dialysis and who are old, frail or have a poor prognosis, there may be a quality of life benefit from a reduced dialysis prescription to minimize the burden of treatment. In low and lower middle-income countries, every effort should be made to conform to the framework of these statements, taking into account resource limitations. The principles of prescribing and assessing delivery of high-quality PD to children are the same as for adults. In all cases, the PD prescription should be designed to meet the medical, mental health social and financial needs of the individual child and family
Background
The International Society for Peritoneal Dialysis (ISPD) last published guidelines on prescribing peritoneal dialysis (PD) in 2006. 1 These focused primarily on targets for small solute removal (Kt/Vurea and creatinine clearance) and ultrafiltration. Even though the recommendations in that guideline started with the statement, ‘Adequacy of dialysis should be interpreted clinically rather than by targeting only solute and fluid removal’, the guideline has often been interpreted as stating that there must be a minimum small solute removal target. Indeed, in some healthcare settings, delivery of PD has focused on achieving the small solute targets suggested in the 2006 guideline without taking into consideration the impact of increasing dialysis exchanges or hours on a cycling machine on a person’s quality of life.
Since 2006, those in need of dialysis have changed considerably with increasing multimorbidity associated with higher proportions of people with diabetes and/or in older age groups. There is therefore increasing realization that dialysis is only one component of care affecting outcomes (see Figure 1).
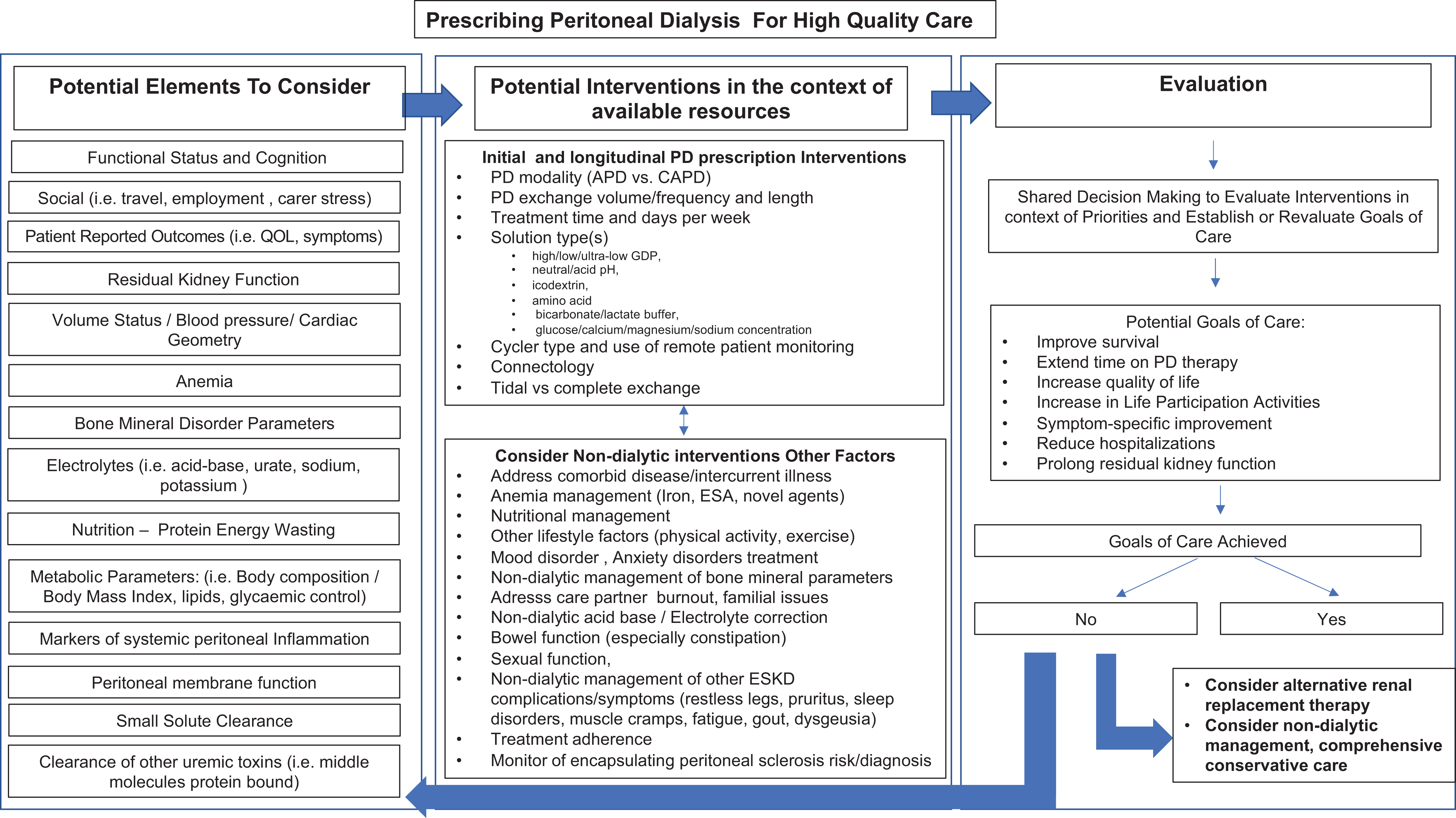
Complexity of care when prescribing high-quality peritoneal dialysis.
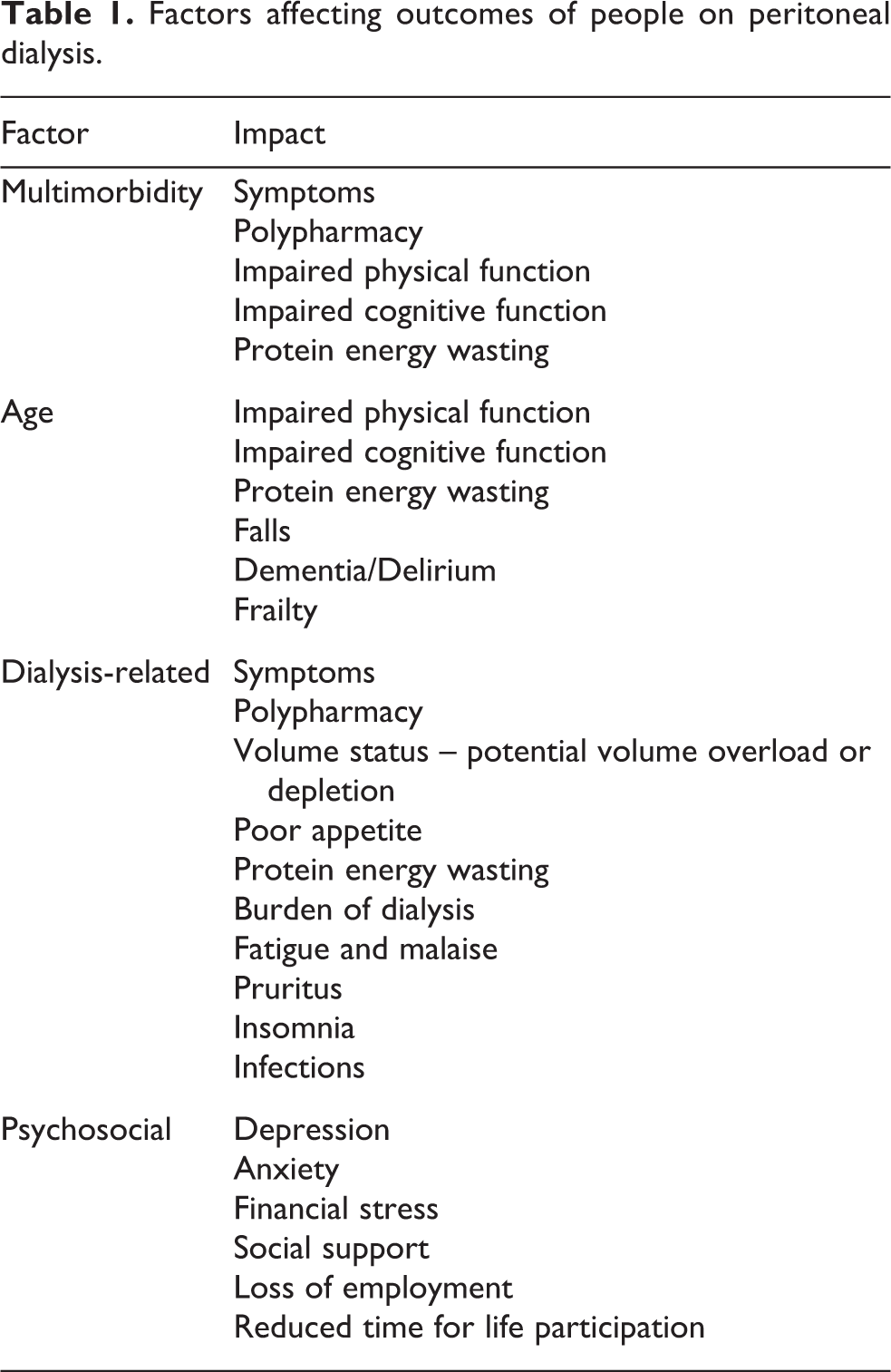
The need for a change in emphasis of care was the focus of discussion at the Kidney Disease Improving Global Outcomes Controversies Conference on Dialysis Initiation, Modality Choice & Prescription in January 2018. At this meeting, it was proposed that there should be a change in terminology from ‘adequate’ dialysis to ‘goal-directed’ dialysis defined as ‘using shared decision-making between the patient and care team to establish realistic care goals that will allow the patient to meet his/her own life goals and allow the clinician to provide individualized, high quality dialyis care’. 2 This approach would require multiple measures and goals to be considered when assessing quality of dialysis, including symptoms, individual experiences and goals, residual kidney function, volume status, biochemical measures, nutritional status, cardiovascular function, small solute clearance and sense of well-being and satisfaction 2 (Table 1).
Factors affecting outcomes of people on peritoneal dialysis.
This goal-directed approach concurs with the findings from the Standardised Outcomes in Nephrology – PD initiative (https://songinitiative.org/projects/song-pd/), which identified core outcomes for PD chosen by patients, caregivers and healthcare professionals. 3 These core outcomes were PD infection, cardiovascular disease, mortality, PD failure and life participation. 4 There is no evidence that small solute clearance on its own directly affects these core outcome measures, except for a small proportion of individuals in whom transfer from PD to HD has been attributed to insufficient small solute removal. 5,6 Otherwise, PD infection and cardiovascular disease have already been addressed by recent ISPD guidelines. 7 –10
Given these changes in clinical emphasis, the Guideline Committee of the ISPD invited a group of globally representative nephrologists to compose new practice recommendations for prescribing high-quality, goal-directed PD. These recommendations are summarized in this article with the underlying thought processes and/or evidence in the accompanying manuscripts in this PDI supplement. Evidence has been graded using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system for classification of the level of certainty of the evidence and grade of recommendations in clinical guideline reports. 11,12 Within each recommendation, the strength of the recommendation is indicated as Level 1 (We recommend), Level 2 (We suggest) or not graded, and the certainty of the supporting evidence is shown as A (high certainty), B (moderate certainty), C (low certainty) or D (very low certainty). We have taken the position to label statements with low certainty evidence (2C, 2D) as practice points
Headline recommendations
The aim of high-quality goal-directed dialysis is to provide the best health outcome possible for an individual on PD in terms of maintaining their clinical well-being, quality of life, ability to meet life goals and at the same time minimize treatment burden. The following headline recommendations are derived from the accompanying papers PD should be prescribed using shared decision-making between the person doing PD/ their caregivers and the care team with the aim of achieving realistic care goals to maximize quality of life and satisfaction for the individual, minimize their symptoms and provide high quality care (
Blake PG and Brown EA. Person-centered peritoneal dialysis prescription and the role of shared decision making. Perit Dial Int 40(3): 302–309.
PD can be prescribed in a variety of ways and should take into account local resources, the person’s wishes regarding lifestyle and the family’s/caregivers’ wishes if they are providing assistance (
Wang AY-M, Zhao J, Bieber B, et al. on behalf of PDOPPS dialysis prescription and fluid management working group. International comparison of peritoneal dialysis prescriptions from the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS). Perit Dial Int 40(3): 301–319.
High-quality PD prescription should be guided by a number of assessments encompassing the person’s well-being and life participation, volume status, nutritional status, anaemia management, small solute removal and bone and mineral management. 3.1 Health-related quality of life The person’s perception of their health-related quality of life should be assessed routinely. This should take into account assessment of symptoms, the impact of dialysis treatment prescription on life participation and psychosocial status. Appropriate adjustments in care should be made based on these assessments (
Finkelstein FO and Foo MWY. Health-related quality of life and adequacy of dialysis for the individual maintained on peritoneal dialysis. Perit Dial Int 40(3): 270–273.
3.2 Volume status High-quality PD prescription should aim to achieve and maintain clinical euvolaemia taking residual kidney function and its preservation into account, so that both fluid removal from peritoneal ultrafiltration and urine output are considered and residual kidney function is not compromised ( Blood pressure should be included as one of the key objective parameters in assessing quality of PD prescription. However, there is currently no evidence for a specific blood pressure target in PD ( Regular assessment of volume status including blood pressure and clinical examination should be part of the routine clinical care (
Wang AY-M, Dong J, Xu X, et al. Volume management as a key dimension of a high-quality PD prescription. Perit Dial Int 40(3): 282–292.
3.3 Nutritional status Nutritional status should be regularly assessed and monitored with attention to appetite and dietary protein intake to maintain a normal nutrition status with restriction of phosphorus, sodium and potassium as indicated ( Biochemical plasma markers including potassium, bicarbonate, albumin, phosphate should be regularly measured as markers of nutrition (
Glavinovic T, Hurst H, Hutchison A, et al. Prescribing high-quality peritoneal dialysis: moving beyond urea clearance. Perit Dial Int 40(3): 293–301.
3.4 Small solute clearance Small solute clearance should be routinely measured using Kt/Vurea or creatinine clearance to provide a quantitative measure of the amount of dialysis delivered. This can guide the amount of dialysis prescribed, while recognizing the limitations of accuracy of these measurements in individuals ( There is no specific clearance target that guarantees sufficient dialysis for an individual. Increasing small solute clearance to a Kt/V The presence of residual kidney function at the start of PD may enable individuals to start on a low dose prescription that may be increased incrementally as residual kidney function declines or as clinically indicated. This may allow patients more time for life participation, less treatment burden and better quality of life ( If symptoms, nutrition and volume are all controlled, no PD prescription change is needed for the sole purpose of reaching an arbitrary clearance target (
Boudville N and Moraes TP. 2005 Guidelines on targets for solute and fluid removal in adults being treated with chronic peritoneal dialysis: 2019 Update of the literature and revision of recommendations. Perit Dial Int 40(3): 254–260.
Davies SJ and Finkelstein FO. Accuracy of the estimation of V and the implications this has when applying Kt/Vurea for measuring dialysis dose in peritoneal dialysis. Perit Dial Int 40(3): 261–269.
Blake PG, Dong J and Davies SJ. Incremental peritoneal dialysis. Perit Dial Int 40(3): 320–326.
Residual kidney function should be determined for all individuals doing PD and management should focus on preserving this function (
Chen CH, Perl J and Teitelbaum I. Prescribing high-quality peritoneal dialysis: The role of preserving residual kidney function. Perit Dial Int 40(3): 274–281.
For some individuals, particularly those who are old, frail or have a poor prognosis, there may be a quality of life benefit from a modified dialysis prescription to minimize the burden of treatment (
Brown EA and Hurst H. Delivering peritoneal dialysis for the multimorbid, frail and palliative patient. Perit Dial Int 40(3): 327–332.
In low and lower middle-income countries or regions, every effort should be made to conform to the framework of these statements, taking into account resource limitations (
Liew A. Prescribing peritoneal dialysis and achieving good quality dialysis in low and low-middle income countries. Perit Dial Int 40(3): 341–348.
The principles of prescribing and assessing delivery of high-quality PD to children are the same as for adults. In all cases, the PD prescription should be designed to meet the medical, psychosocial and financial needs of the child and their family (
Warady BA, Schaefer F, Bagga A, et al. Prescribing peritoneal dialysis for high quality care in children. Perit Dial Int 40(3): 333–340.
Key points from literature review
These recommendations include sections on delivering PD to children and prescribing PD in lower income countries, so that they are relevant for all people doing PD. The discussions of the ISPD work group focused on the need for person-centred care with an emphasis on dialysis-related factors that impact on individual well-being, PD delivery approaches that have evolved since 2006 (incremental PD, PD delivery to older and frail individuals) and the problems associated with interpreting Kt/V. The summary points and key recommendations from each paper are summarized in Table 2.
Summary of key points.
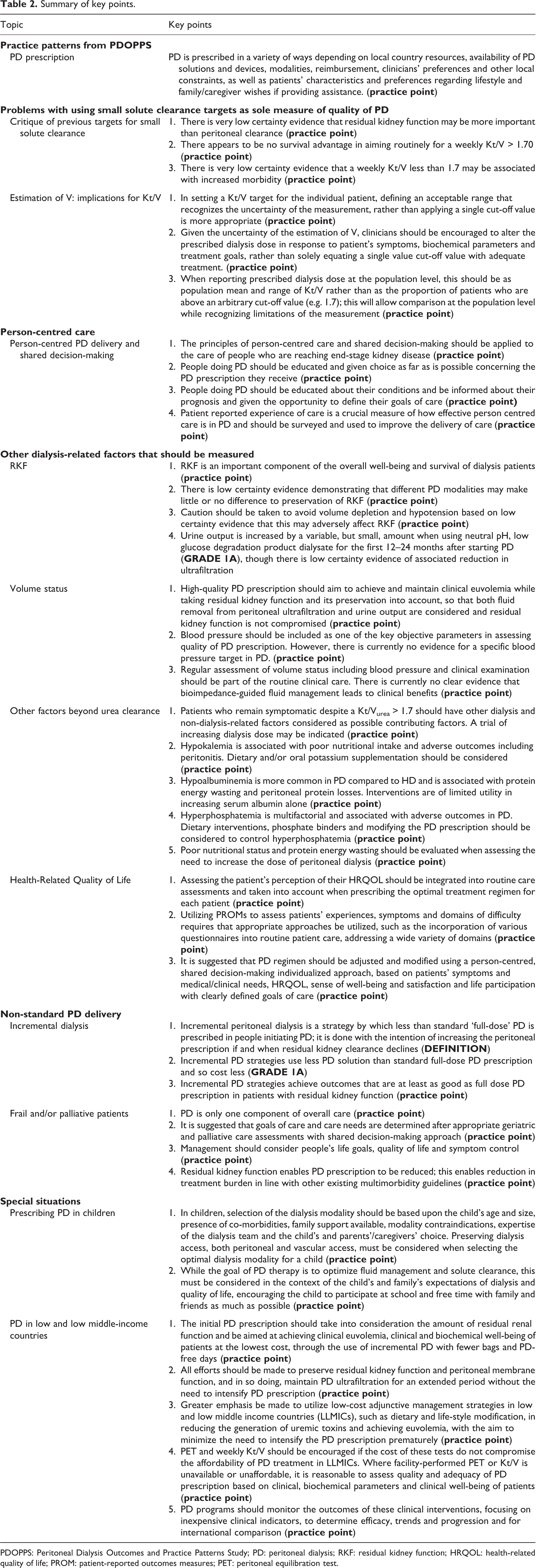
PDOPPS: Peritoneal Dialysis Outcomes and Practice Patterns Study; PD: peritoneal dialysis; RKF: residual kidney function; HRQOL: health-related quality of life; PROM: patient-reported outcomes measures; PET: peritoneal equilibration test.
Clinical use of recommendations
Which dialysis solution?
Peritoneal Diaysis Outcomes and Practice Patterns Study (PDOPPS) data
13
showed significant variations in the use of different strengths of hypertonic glucose PD solutions, icodextrin and neutral pH, low glucose degradation product (GDP) solutions depending on availability and reimbursement policies in different countries. Longer follow-up is needed to determine the association between the use of these solutions and patient outcomes. The ISPD cardiovascular guideline published in 2015
9
recently reviewed the evidence regarding icodextrin, neutral pH and low GDP solutions; this has been updated by a Cochrane review published in 2018.
14
Once-daily icodextrin should be considered as an alternative to hypertonic glucose solutions for long dwells in people doing PD who are experiencing difficulties maintaining euvolemia due to insufficient peritoneal ultrafiltration, taking into account the individual’s peritoneal transport state ( Use of neutral pH, low GDP PD solutions improves preservation of residual kidney function and urine output (
Identification of individuals who are ‘failing to thrive’
When prescribing person-centred high-quality PD, a challenge is to identify individuals who would benefit from an increase in dialysis prescription or change in dialysis modality while recognizing that some individuals are reluctant to do so. Furthermore, there may be limitations to dialysis delivery imposed by local healthcare structures and resources. It is therefore important that all units develop some local structures to identify individuals who are failing to thrive on PD and to recognize the symptoms, clinical features and biochemical markers that would support an increase in dialysis prescription or change in dialysis modality. Methods that could be used by care teams are suggested in Table 3.
Methods of recognising ‘failing to thrive’ patients on PD.
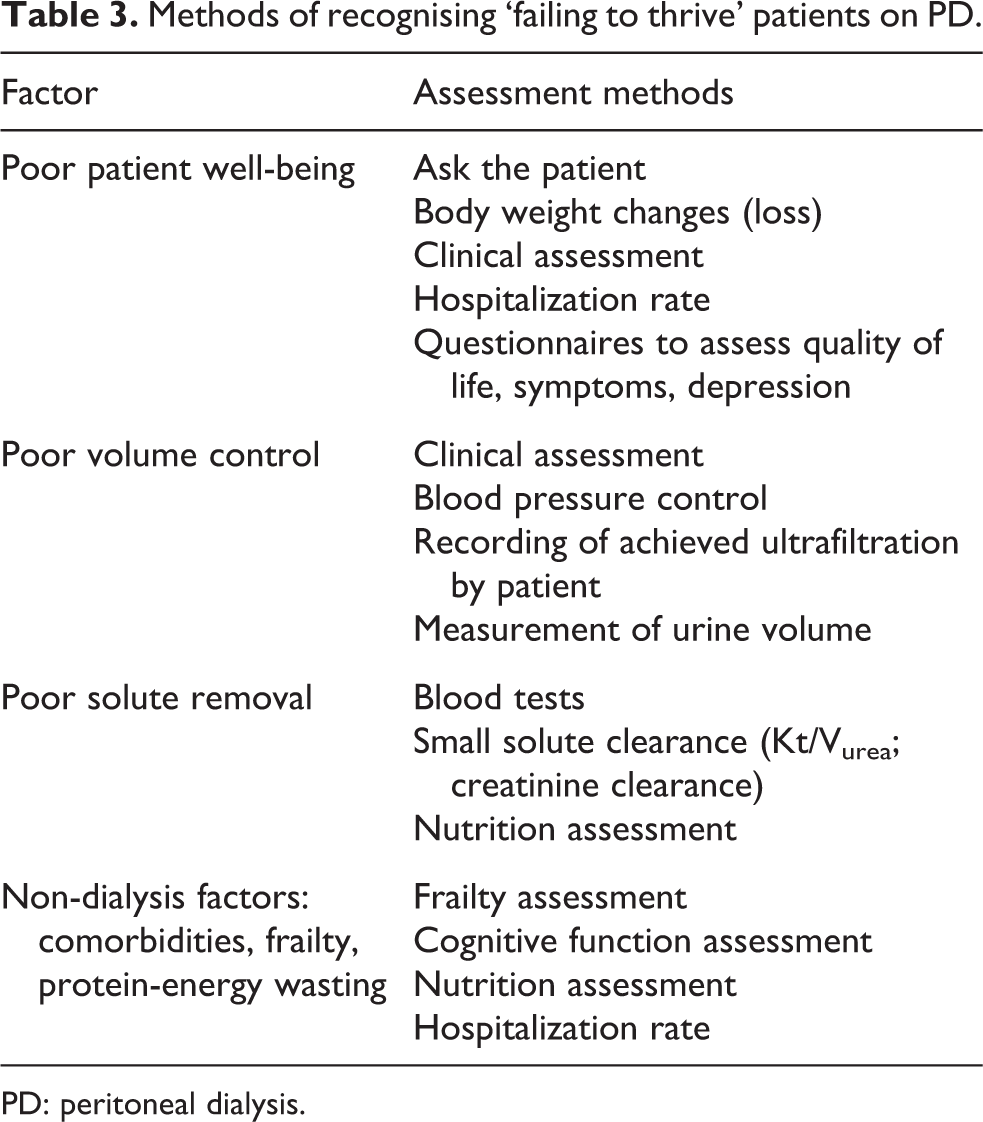
PD: peritoneal dialysis.
The frequency of use of individual methods will depend on local healthcare resources, but it is recommended that all units develop some method of recognizing patients who have symptoms or clinical features and biochemical markers indicating failure to thrive (
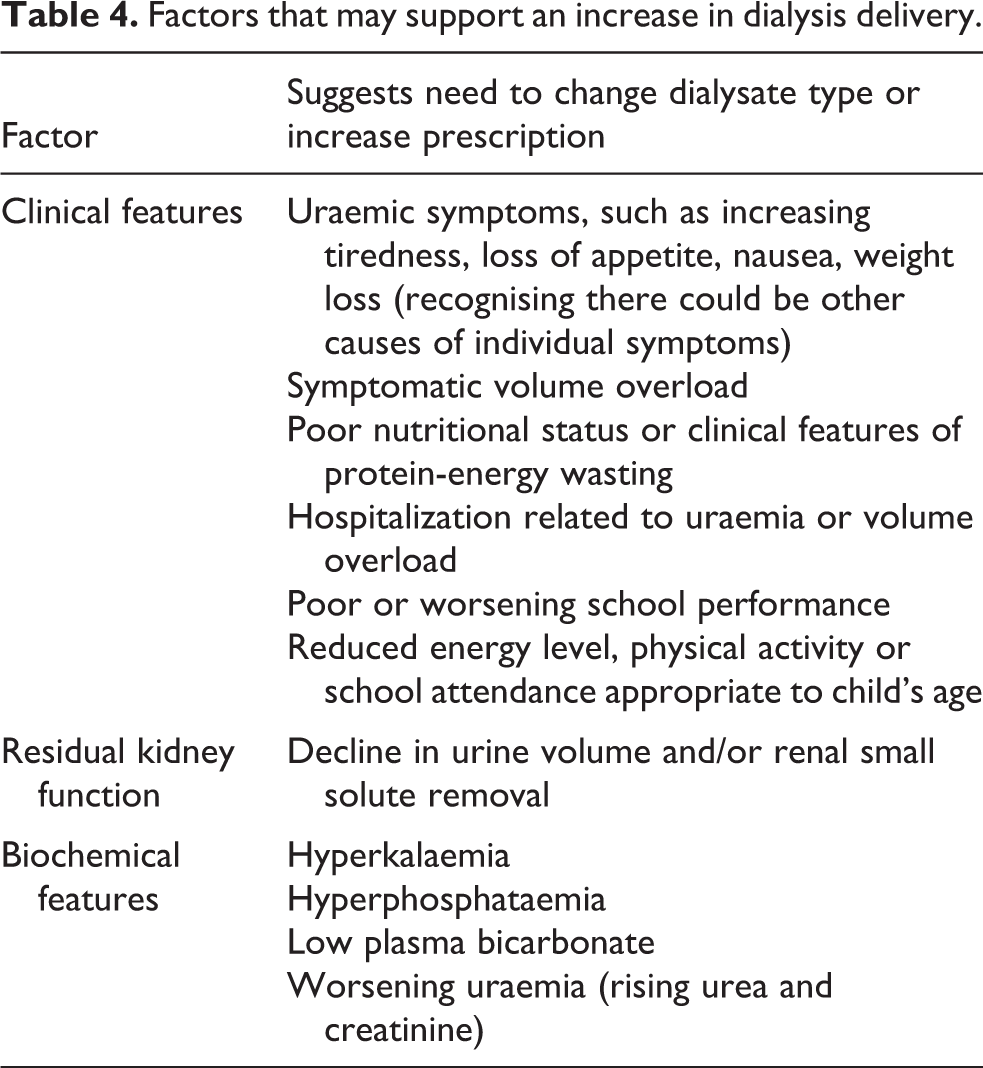
A person’s symptoms, clinical features and biochemical markers that would support an increase in dialysis prescription are shown in Table 4. We suggest that more than one of these should be present given the inherent inaccuracies in measuring small solute clearance and the potential multiple causes of a single ‘uraemic’ symptom or biochemical abnormality
Factors that may support an increase in dialysis delivery.
Involvement of people on PD with guideline
Differences in healthcare resources and the heterogeneity in PD technology, dialysis solutions availability and holistic kidney care for people treated with dialysis have made it difficult to have them involved at the guideline development stage. The first version of this article was sent to people doing PD from the various countries represented by members of the guideline group. Feedback was given by 22 people on peritoneal dialysis or caregivers from 8 countries on 5 continents and will be presented as a separate accompanying paper. We have incorporated their wish that ‘person’ is preferable to ‘patient’ in the revision of this manuscript. We have also co-written a lay summary with a UK group of people on dialysis with the key contributor listed as an author.
Corbett RW, Goodlet G, MacLaren B, et al. International Society for Peritoneal Dialysis Practice Recommendations: The view of the person who is doing or who has done PD. Perit Dial Int 40(3): 349–354.
Implementation
It is not possible to embed an implementation plan into an international guideline as the process will vary from country to country depending on healthcare systems and resource availability. We recommend strongly that people doing peritoneal dialysis are involved with national, regional and local implementation plans based on this guideline.
Summary
Delivery of high-quality, goal-directed peritoneal dialysis requires a person-centred, individualized shared decision-making approach with tailoring of the prescription to the person’s well-being, lifestyle and quality of life with adjustments dependent on residual kidney function, volume status and dialytic solute removal and to minimize treatment burden. Given the minimal high-quality evidence for the recommendations, it is essential to conduct further research with questions prioritized by healthcare providers and individuals with kidney disease.
Supplemental Material
Supplemental Material, sj-pdf-1-ptd-10.1177_0896860819895364 - International Society for Peritoneal Dialysis practice recommendations: Prescribing high-quality goal-directed peritoneal dialysis
Supplemental Material, sj-pdf-1-ptd-10.1177_0896860819895364 for International Society for Peritoneal Dialysis practice recommendations: Prescribing high-quality goal-directed peritoneal dialysis by Edwina A Brown, Peter G Blake, Neil Boudville, Simon Davies, Javier de Arteaga, Jie Dong, Fred Finkelstein, Marjorie Foo, Helen Hurst, David W Johnson, Mark Johnson, Adrian Liew, Thyago Moraes, Jeff Perl, Rukshana Shroff, Isaac Teitelbaum, Angela Yee-Moon Wang and Bradley Warady in Peritoneal Dialysis International
Supplemental Material
Supplemental Material, sj-pdf-2-ptd-10.1177_0896860819895364 - International Society for Peritoneal Dialysis practice recommendations: Prescribing high-quality goal-directed peritoneal dialysis
Supplemental Material, sj-pdf-2-ptd-10.1177_0896860819895364 for International Society for Peritoneal Dialysis practice recommendations: Prescribing high-quality goal-directed peritoneal dialysis by Edwina A Brown, Peter G Blake, Neil Boudville, Simon Davies, Javier de Arteaga, Jie Dong, Fred Finkelstein, Marjorie Foo, Helen Hurst, David W Johnson, Mark Johnson, Adrian Liew, Thyago Moraes, Jeff Perl, Rukshana Shroff, Isaac Teitelbaum, Angela Yee-Moon Wang and Bradley Warady in Peritoneal Dialysis International
Footnotes
Declaration of conflicting interests
The author(s) disclosed the following conflicts of interest with respect to the research, authorship, and/or publication of this article: EA Brown received speaker fee for Baxter Healthcare UK Advisory board for Baxter Healthcare UK, LiberDi, AWAK.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.