
Abstract
In the Democratic Republic of Congo (DRC), acute kidney injury (AKI) contributes to the high rate of child mortality owing to the conjunction of poverty, deficiency of qualified health-care providers in pediatric nephrology, and the lack of pediatric dialysis programs. We aimed to describe the recent experience of the first pediatric acute peritoneal dialysis (PD) program in DRC. This is a retrospective cohort study on epidemiology, clinical features and outcomes of children admitted from January 2018 to January 2019 at the University Hospital of Kinshasa for AKI and treated with PD. This pediatric PD program started by a team of one physician and one nurse who were trained in the local production of PD fluids and bedside catheter insertion technique in Benin Republic. The training was jointly supported by the Flemish Inter-University Council (VLIR) TEAM project and Saving Young Lives (SYL) program of ISN, ISPD, EuroPD, and IPNA. From January 2018 to January 2019, 49 children (aged 4 months–15 years) were admitted for AKI mainly due to severe malaria and sepsis. Dialysis was indicated in 35 of 49 (71.4%), 32 of 35 (91.4%) were treated with PD, two with hemodialysis (HD) in adult ward and one died at admission. Data of the two patients transferred for HD were not available for follow-up. The main indications were uremia and prolonged anuria. Of 32 dialyzed patients, 24 (75%) recovered normal renal function 3 months after discharge. Peritonitis was observed in 2 of 32 (6.2%) patients and the mortality was 18.7%. This promising experience proves that with simple means including use of locally produced dialysis fluids and low peritonitis rates, we can effectively save lives of children suffering from AKI.
Introduction
In the Democratic Republic of Congo (DRC), a country of approximately 80 million inhabitants, half of which are children, acute kidney injury (AKI) is often regarded as death sentence due to the conjunction of the deficiency of qualified health-care providers in pediatric nephrology, poverty, and the lack of a pediatric Renal Replacement Therapy (RRT) program in the country. 1,2 Before 2018, children admitted in the University Hospital of Kinshasa for AKI who required RRT were transferred to Adult Nephrology ward. However, the access to this treatment was very limited due to financial constraints and most of them died. 1 We aimed to establish the first pediatric acute peritoneal dialysis (PD) program in the DRC.
Methods
We conducted a retrospective review of pediatric cases treated for AKI with PD at the Pediatric Nephrology Unit of the University Hospital of Kinshasa from January 2018 to January 2019. Initially, with the joint support of KU Leuven through the Flemish Inter-University Council (VLIR) TEAM project and the Saving Young Lives (SYL), a complementary partnership between international nephrology organizations: International Society of Nephrology (ISN), International Pediatric Nephrology Association (IPNA), European Peritoneal Dialysis (EuroPD), International Society for Peritoneal Dialysis (ISPD), one pediatric resident and one nurse from the Pediatric Nephrology Unit were trained at the University Hospital CNHU-HKM of Cotonou, in Benin. The training covered the main aspects of running a pediatric PD program, especially the bedside PD catheter insertion technique and the local production of PD fluids. After returning from training, since December 2017, the two resource members of the team have in turn trained three other pediatric residents and five nurses.
Eligibility criteria to start PD treatment included prolonged anuria, life-threatening fluid overload, uremic toxicity, severe metabolic acidosis, and refractory hyperkalemia. PD was stopped based on recovery of diuresis, clinical improvement, and normalization of electrolytes disturbances. PD was performed in strict aseptic conditions. Cuffed PD catheters were supplied by SYL program and inserted manually at bedside by trained pediatric residents in the midline, 1–2 cm below the umbilicus after local skin disinfection and instillation of local anesthetics. PD fluids with 1.5%, 2.5%, and 4.25% dextrose solutions were produced locally by mixing lactated ringer’s solution with subsequent addition of 50% glucose following ISPD guidelines for PD treatment of AKI (Table 1). Patients have been treated with standard manual exchanges with the frequency of exchanges depending on the clinical condition of the patient, following ISPD guidelines for PD treatment of AKI. 3 Full renal function recovery was defined by the normalization of creatinine measured during the follow-up, 3 months after the discharge.
Composition of locally made PD fluids.
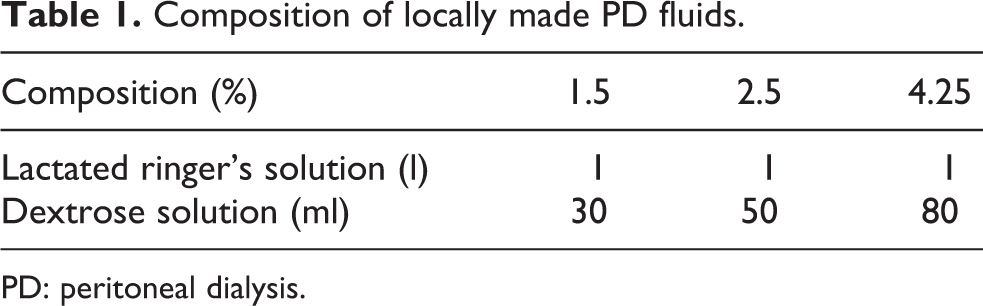
PD: peritoneal dialysis.
Results
From January 2018 to January 2019, a total of 1036 patients were admitted in the emergency unit, of whom 143 (13.8%) were new cases of kidney disease, 49 (4.7%) had AKI. Dialysis was indicated in 35 of 49 (71.4%): 32 of 35 (91.4%) patients were treated with PD, 2 were transferred to the adult HD program and 1 child died before having started PD treatment. Data from two patients transferred for HD treatment were not available for follow-up. In the present study, we described epidemiological data, clinical features, and outcomes of 32 children who underwent PD treatment.
Clinical and biochemical characteristics of dialyzed patients
There were 21 boys (65.6%) and 11 girls (34.4%), the male-to-female ratio was 1.9:1 with a median age of 7 years (4 months–15 years). The median duration of disease was 9 days (4–120 days). At presentation, predominant clinical features of patients were decreased urine output (n = 21, 65.6%), coma and/or convulsions (n = 15, 46.8%), and body swelling (n = 6, 18.7%). The other presenting features were pallor (n = 4, 12.5%), hemorrhagic diathesis (n = 3, 9.4%), and jaundice (n = 1, 3.1%). Biochemical characteristics at presentation widely varied from one patient to another. All patients had elevated serum creatinine with an average of 7.94 ± 4.37 mg/dL. Serum urea and kalemia were 222.34 ± 93.81 mg/dL and 5.10 ± 1.39 mEq/L, respectively. The average of natremia was 133.38 ± 11.18 mEq/L and hemoglobin 7.89 ± 3.31 g/dL. Figure 1 shows the main causes of AKI and indications for initiating PD.
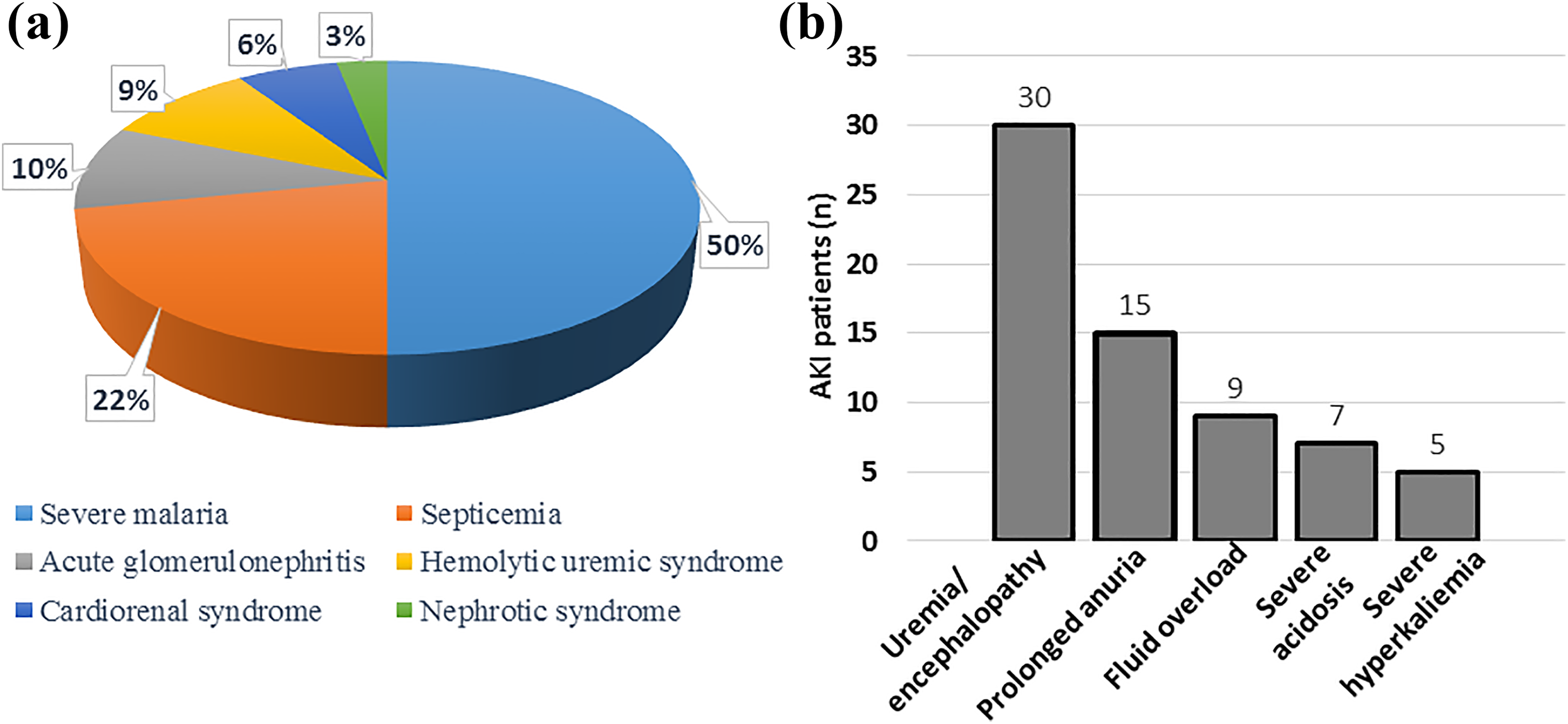
Clinical characteristics of dialyzed patients. (a) Main causes of AKI diagnosed among dialyzed patients. (b) Main indications for initiating PD treatment in children admitted with AKI: number on the top of each column represents the number of patients for each indication. To note that some patients had more than one indication. AKI: acute kidney injury; PD: peritoneal dialysis.
Complications
Complications of PD were reported in 6 of 32 (18.7%) children. Peritonitis occurred in 2 of 32 (6.2%), catheter obstruction in 2 of 32 (6.2%), hemorrhagic effluent in 1 of 32 (3.1%), and catheter leakage in 1 of 32 (3.1%). Catheter obstruction by fibrin clot was treated by flushing PD catheter with heparin before continuing the dialysis. PD was stopped in one case of catheter leakage because of the risk of peritonitis.
Outcomes and mortality
The median duration of PD treatment was 7 days (1–19 days). After PD treatment, creatinine control was performed 3 months after discharge and full recovery of renal function was observed in 24 of 32 (75%) children. Of the 32 dialyzed patients 6 (18.7%) died. Most of those patients, referred late, presented with a critical condition at admission.
Discussion
Access to PD treatment
In this study, almost all patients (> 90%) who required dialysis had access to the treatment. Access to PD was much higher than previously reported by Aloni et al. (26.6%) in the same hospital. 1 In the current PD program, catheter insertion was performed at bedside by a pediatric senior resident. This significantly reduced time and costs required to initiate PD. Before the establishment of this pediatric PD program, the catheter was inserted surgically in the operating theater under general anesthesia. There was only one surgeon in the hospital who was in charge of this procedure. In addition to dialysis fees, the parents had to cope with the cost of surgery and anesthesia. All these constraints contributed to limited access to PD treatment in the majority of patients. The bedside PD catheter insertion and local production of PD fluids have significantly reduced the cost of PD treatment and made it affordable for most patients.
Causes of AKI
All patients in the present study had community-acquired AKI: severe malaria, mainly BWF, and sepsis. This is consistent with data reported in other African countries as presented in Table 2. Because of malaria and/or ingestion of amino alcohols such as quinine, BWF emerges as a frequent form of severe malaria and a common cause of AKI in the DRC and in many other African countries. 1,5,9
Comparative overview of clinical characteristics and outcomes of patients treated with PD in seven different sites in Africa.a
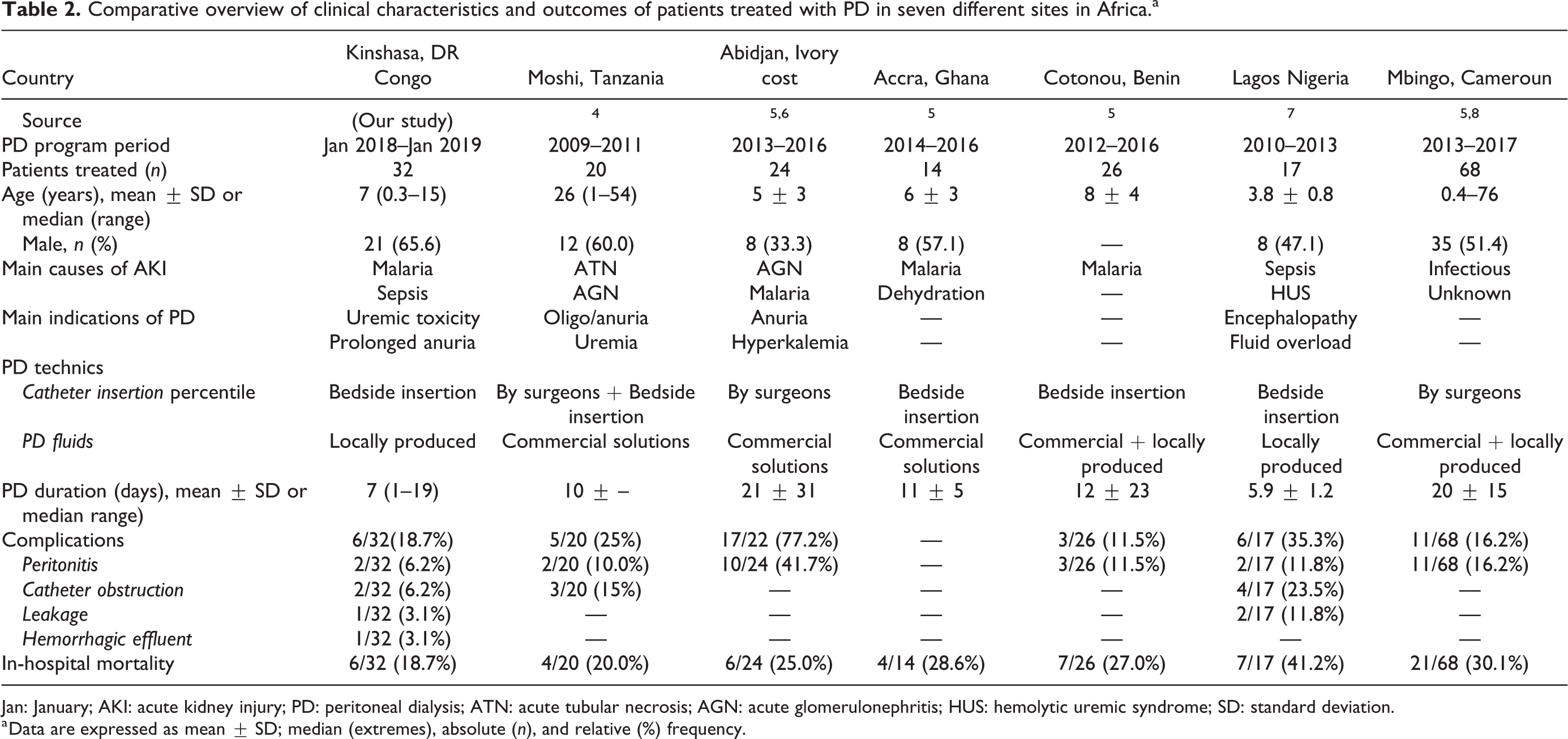
Jan: January; AKI: acute kidney injury; PD: peritoneal dialysis; ATN: acute tubular necrosis; AGN: acute glomerulonephritis; HUS: hemolytic uremic syndrome; SD: standard deviation.
a Data are expressed as mean ± SD; median (extremes), absolute (n), and relative (%) frequency.
Complications during PD treatment
The frequency of complications during PD treatment in the present study was 18.7%. The peritonitis occurred in 6.2% of the cases. As shown in Table 2, this frequency is lower than those reported in previous studies from Africa, particularly where surgical catheter insertion and/or commercial PD fluids were used. Likewise in Cameroon, Palmer et al. found that there was no difference in the rate of peritonitis and mortality between patients who have been dialyzed by commercial versus locally made solutions. 8 The infection was a big challenge when we were establishing this first PD program, given the unfortunate experience of using locally produced fluids attempted long before by the adult nephrology in the University Hospital of Kinshasa. To meet this challenge, strict aseptic measures have been followed during the implementation of the current pediatric PD program: newly refurbished and constantly maintained infrastructure, clear protocol of asepsis starting from the insertion of the PD catheter to PD sessions has to be respected by all medical and paramedical staff.
Outcomes
In the present study, more than 70% of dialyzed children recovered renal function in a setting where many of these children may have died without access to PD. An estimated in-hospital mortality of 18.5% has been reported. This observed mortality rate is lower than that previously reported in the same hospital 1 and those reported in other African countries (Table 2). However, as discussed above, all deceased patients were admitted in advanced stage of kidney failure and in a moribund state.
This situation may be explained by several factors including the lack of adequate knowledge and appropriate tools for an early and correct diagnosis of AKI, the long distance to travel for patients coming from the neighboring provinces, the financial constraints, and some cultural beliefs. This again raises the issue of late transfer as a major risk factor of the AKI-related mortality. To efficiently address these preventable deaths, in addition to rigorous aseptic measures, repeated education campaigns in communities and frequent training in peripheral hospitals need to be implemented. Beyond all, in order to significantly contribute to the reduction of AKI-related child mortality in the DRC, this promising experience of acute PD program should be spread across different provinces of the country.
Challenges, opportunities, and recommendations
The results obtained over 12 months of this pediatric PD program are reassuring. However, some limitations and challenges were encountered. The major challenge is the lack of financial commitment from the government. Parents are responsible to pay for the dialysis and all laboratory tests. Ignorance is also one of the challenges to face. Indeed, many parents in our society believe that kidney disease cannot affect children since the kidney is a genital organ of the adult male. To address the financial constraints, a mini laboratory has been installed within the program. The funds generated by this laboratory and those from parents able to pay the costs of PD, allow to support the poorest, and to ensure the sustainability of the program. Furthermore, the association created by the patients suffering from kidney diseases and parents of children having suffered from kidney disease, works in collaboration with the Congolese Society of Nephrology, significantly participates and supports our program. One of its goals is to morally and financially support children suffering from kidney disease and their parents. They organize meetings to exchange experience and provide financial contribution in case of necessity. However, the successful implementation of PD program in low-income countries requires unwavering commitment and a creative and ambitious mind. Strategies to raise awareness of community and regional health-care providers in early recognition and reference of patients with AKI are essential to efficiently address AKI-related preventable deaths. Furthermore, the preliminary results obtained should be used to get the financial commitment of the government, essential for the sustainability of the program.
Conclusion
This experience joins those from other PD sites in Africa proving that with simple means we can effectively save lives of children suffering from AKI and reveals the importance of internal cooperation between teams working in resource-limited countries within Africa with the support of high-income countries outside of Africa, specifically Europe as in this case. The ultimate goal is to extend this experience across the country and to neighboring countries in order to efficiently contribute to the 0by25 objective of the ISN.
Footnotes
Acknowledgments
The authors thank Drs Francis Lalya and Marie Sophie Ghuysen for their valuable contribution to the training of the team of Kinshasa. They also express their gratitude to Dr Betukumesu Dieumerci, Mrs Bibiche Kabedi, and Ms Oyindamola Adebayo for their contribution to the data acquisition and the revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Flemish Inter-University Council (VLIR) and Inter-Faculty Developmental Council (IRO) of KU Leuven. EL is supported by F.W.O. Vlaanderen, grant 1801110N. FOA is supported by F.W.O. Vlaanderen, grant 12Q9917N.