
Abstract
Workforce shortages in the health and social care sectors are a relevant issue worldwide. One measure to mitigate workforce shortages is to improve working conditions and workers’ future prospects in order to encourage worker retention. Although studies have examined factors related to organizational turnover, less is known about the factors that lead to occupational turnover intentions. Drawing upon social cognitive career theory, this study examines the reasons behind health and social care workers’ occupational turnover intentions considering emotional exhaustion as an explanatory variable. The participants were 403 health and social care workers who responded to a questionnaire about 4 years after completing their vocational education and training at the upper-secondary level. Structural equation analyses revealed that affective occupational commitment showed the highest negative correlation with occupational turnover intentions. Furthermore, the results suggest that career-related outcome expectations, wellbeing, and supportive working conditions are crucial for designing effective interventions.
Keywords
The shortage of skilled workers is a socially relevant issue in the health and social care fields worldwide (World Health Organization [WHO], 2016) that has been discussed and studied in terms of measures for recruitment and retention of skilled workers even before the COVID-19 pandemic (Organisation for Economic Co-operation and Development [OECD], 2020). In 2030, the number of health workers (physicians, nurses or midwives, and other health workers) is expected to be far below the estimated demand presented by aging populations (Liu et al., 2017). Switzerland and many other countries employ initiatives to promote interest in occupational activities and professional careers in these sectors, and to thereby increase the number of students of these subjects in both the upper-secondary and tertiary levels. Other initiatives have been attempted to meet the demand for a qualified workforce in these sectors by discouraging health and social care workers and professionals from leaving. Moreover, research shows that turnover intention negatively affects the quality, consistency, and stability of human services, and thus has negative implications for clients receiving care (e.g., De Simone et al., 2018; McMullen et al., 2020). The ongoing COVID-19 pandemic has increased work demands and exacerbated stress, particularly for frontline health care workers (Labrague & Santos, 2021), and has further revealed the crucial roles played by nursing and care professionals and the importance of addressing workforce shortages (Labrague & Santos, 2021; OECD, 2020). Overall, these current challenges underscore the urgency of keeping skilled workers in their occupational fields. They also underline the need for a renewed focus on the occupation rather than the organization (Medici et al., 2020), and for the advancement of research that contributes to a better understanding of the causes of occupational turnover in specific fields, both in general and beyond the pandemic.
While the factors related to the loss of qualified staff who intend to move to another organization or company have long been studied, relatively few studies have specifically looked at health and social care workers’ decisions to leave their occupation and change careers (e.g., Fernet et al., 2021; Kim & Stoner, 2008). Among more recent studies that focused on employees’ decisions to leave their occupational or professional field, some have dealt specifically with occupational turnover in both traditional and non-traditional female areas, such as engineering or nursing/healthcare (e.g., Fernet et al., 2021; Fouad et al., 2016). Studies in the health and social care sectors have repeatedly shown that prolonged strain and stress, which can lead to emotional exhaustion and burnout, are important factors in explaining why workers leave their jobs or occupations voluntarily (e.g., Leiter & Maslach, 2009; Van der Heijden et al., 2019). In a recent longitudinal study with participants from a broad range of occupations (Medici et al., 2020), strain was found to be a direct antecedent of occupational change in employment; the authors thus suggested that future studies and theoretical models on occupational change should consider stress as a central predictor of occupational change.
The present study examines health and social care workers’ occupational turnover intentions, drawing upon extended social cognitive career theory (SCCT) framework models (Fouad et al., 2016, 2017; Singh et al., 2013). Moreover, it adds strain, respectively, emotional exhaustion, to which health and social care workers are particularly vulnerable, as an explanatory variable to the theoretical framework. With regard to the target group, the study picks up a research gap through the inclusion of skilled workers from occupational groups without a university degree—that is, skilled assistant staff with a vocational education and training (VET) degree—for which currently scarce international data exist (OECD, 2017). Thus, so far hardly any theoretically sound studies on career development or retention of workforce are available. The results of this study are of high practical relevance, as they will aid in developing effective interventions that prevent the attrition of qualified staff from the health and social care sectors and thus reduce financial, as well as social and societal costs. Furthermore, the results of the present study provide theoretical suggestions for the extension of existing SCCT-based framework models dealing with voluntary occupational turnover.
Social Cognitive Career Theory and Model Predicting Organizational Turnover Intentions
SCCT (e.g., Brown & Lent, 2019; Lent et al., 1994) is an established theoretical framework for studying career choice and development, career self-management, and work satisfaction, and it has served as the basis for a great deal of research in this area. According to SCCT, several cognitive-person variables affect career-related choices and self-management behavior directly. They are: (1) goals and intentions to engage in particular career-relevant actions, (2) self-efficacy beliefs, and (3) outcome expectations, which are the anticipated longer-term consequences of activity engagement. Organizational or social supports and career role models play central roles as contextual factors that shape the development of self-efficacy and outcome beliefs both directly and through learning experiences (e.g., Lent et al., 2016, 2000). SCCT has also been used to study decisions and actions regarding organizational and occupational turnover (e.g., De Simone et al., 2018; Fouad et al., 2016; Singh et al., 2013).
In their model predicting organizational turnover intentions, Singh et al. (2013) integrated SCCT with organizational support and organizational turnover theory (Eisenberger et al., 1986; Hom & Griffeth, 1995) to examine voluntary organizational turnover intentions. They added two key job-related attitudes—job satisfaction and organizational commitment (Blau, 2007)—and organizational support as predictors of organizational turnover intentions to their model. In line with previous research (e.g., Griffeth et al., 2000; Podsakoff et al., 2007) and a more recent study on employee retention in healthcare (Perreira et al., 2018), their results show that women engineers with positive job attitudes (i.e., high organizational commitment) are less at risk of leaving their organization. In addition, Singh et al. (2013) found a direct positive association between social cognitive factors (i.e., self-efficacy beliefs and outcome expectations) and job attitudes and identified their influence on turnover intentions. Furthermore, their results show that organizational support is a source of self-efficacy and outcome expectations, and that both are mediators of the relationships between organizational support and job attitudes.
In subsequent studies, Fouad et al. (2016, 2017) analyzed predictors of occupational turnover, and therefore unified SCCT with the integrated model of career change (Rhodes & Doering, 1983). They found that women who stayed and women who left the field of engineering differed in their experiences with workplace support (i.e., training and development opportunities, managers’ understanding of the desire to balance work life and family roles). Occupational commitment and turnover intentions emerged as the two key variables that explained continuation in the profession. However, the authors did not find differences in self-efficacy or outcome expectations between individuals who continued in their profession and those who left.
Emotional Exhaustion and Turnover Intentions
Theoretical assumptions about the influence of burnout and the syndrome of emotional exhaustion (Maslach & Jackson, 1981) on commitment and turnover have been confirmed in various studies on career behavior of professionals (e.g., Blau, 2007; Cropanzano et al., 2003; Thanacoody et al., 2014). In turnover theory (e.g., Blau, 2007; Hom & Griffeth, 1995) exhaustion is conceptualized as an antecedent of job-related attitudes (i.e., commitment, satisfaction), which in turn influence turnover perceptions and intentions. The negative relation between organizational or professional turnover intentions and employee attitudes is a consistent research finding across professions and industries (e.g., Lee et al., 2000), and has also been showcased in the SCCT-based framework model by Singh et al. (2013)—namely, for the aspect of organizational commitment, but not for job satisfaction.
Workers in the health and social care sectors, whose work activities involve intensive social contacts and are emotionally demanding, experience high work-related stress (McFadden et al., 2021; Thanacoody et al., 2014) and are at an increased risk of becoming emotionally exhausted and developing burnout, which has become a more acute problem since the beginning of the pandemic (Labrague & Santos, 2021). Research shows that mental health stressors and burnout among nurses are responsible for significant variance in organizational (e.g., De Simone et al., 2018) and occupational turnover intentions (e.g.,Van der Heijden et al., 2019), and similar findings are available for social workers (e.g., Itzick & Kagan, 2017; Kim & Stoner, 2008). Blau (2007) found work exhaustion to be a significant correlate for occupational turnover. For job stress, a negative impact on job-related attitudes, both occupational commitment and work satisfaction, was shown. (Major et al., 2013; Medici et al., 2020). In a study on new graduate nurses (Spence Laschinger & Fida, 2014), emotional exhaustion was proved to be a predictor of career turnover intentions, but not of job turnover intentions. There is empirical evidence that access to need-based job resources (e.g., autonomy, social support, development opportunities) can buffer the effects of demanding job tasks and challenging interactions on strain (e.g., Xanthopoulou et al., 2007) and occupational turnover intentions (Van der Heijden et al., 2018) among healthcare professionals. In a study with nurses, support from supervisors and coworkers was found to foster both occupational commitment and retention and was mediated by autonomous motivation (Fernet et al., 2021). In social occupational work environments too, social support was found to have a positive effect on work motivation, whereby coworkers’ autonomy support was found to be more effective than manager support (Jungert et al., 2021).
Purpose of the Present Study
The current study on career change intentions among health and social care workers extends social cognitive career theory and research in two ways: first, we build upon previous SCCT-based models (Fouad et al., 2016; Lent & Brown, 2013; Singh et al., 2013) to explain occupational (rather than organizational) turnover intentions. Based on Feldman and Ng (2007), we define occupational turnover as a worker’s decision to abandon their current work and look for employment in different occupational fields that requires different skills and routines. Second, in line with empirical findings (e.g., Blau, 2007; Major et al., 2013) and theoretical approaches that distinguish between both a motivational and a health-impairment process when explaining turnover (e.g., Bakker & Demerouti, 2017), we consider emotional exhaustion as a precursor of occupational commitment and turnover intentions (see Figure 1). Extended social cognitive model of occupational turnover intentions.
One main objective of the study is to understand what makes health and social care workers consider leaving their occupational fields 4 years after completing VET and launching a career in the health and social sectors. To do this, we analyze the relationships between the theoretically postulated direct explanatory variables—which include social cognitive factors (i.e., occupational self-efficacy and outcome expectations), job attitudes (i.e., affective occupational commitment), but also wellbeing (i.e., emotional exhaustion)—and their direct and indirect contribution to the prediction of occupational turnover intentions. Concerning job-related attitudes, we confine the focus on workers’ affective occupational commitment. Furthermore, we consider career-related outcome expectations (rather than outcome expectations related to professional tasks) as desired outcomes of intentional career actions with regard to work-related needs (Fouad & Guillen, 2006). Among these needs, experiencing growth and comfort is positively valued and contributes to career and occupational commitment (Major et al., 2013; Meyer et al., 1998; Zhu et al., 2021), and career growth has been explicitly recommended to be included in theoretical frameworks beyond those who usually do so (Weng & Zhu, 2020). Another important goal of the study is to examine workplace support as a source of workers’ occupational self-efficacy, career-related outcome expectations, occupational commitment, and wellbeing. In addition to social support by coworkers (Fouad et al., 2016), we integrate autonomy support from supervisors as another need-based resource into the model. This resource turned out to be the most important type of supportive behavior an organization can provide regarding leadership behavior, and has been shown to influence motivational processes and affect occupational commitment, emotional exhaustion, and turnover intentions (Fernet et al., 2013, 2021; Jungert et al., 2021). We propose the following hypotheses.
High occupational self-efficacy and positive outcome expectations as well as high affective occupational commitment are associated with low occupational turnover intentions. High emotional exhaustion is associated with high occupational turnover intentions.
High occupational self-efficacy and positive outcome expectations are associated with high affective occupational commitment and low emotional exhaustion.
Social support from close coworkers and autonomy support from supervisors are associated with high occupational self-efficacy and positive outcome expectations as well as high occupational commitment and low emotional exhaustion.
Method
Context of the Study
The current study investigates occupational turnover intentions in the context of the Swiss VET system. In this approach, training is based on an apprenticeship model in which future workers acquire the competencies needed to work in a specific occupation. Most VET programs consist of dual-track approaches: apprentices receive in-company training and, at the same time, attend a vocational school one to 2 days per week over a span of several years (State Secretariat for Education, Research and Innovation [SERI], 2021). The apprenticeship model regulates access to tertiary-level professions, which is achieved in the health and social care sectors primarily through subsequent studies at a university of applied sciences. In Switzerland, two-thirds of youth begin a VET-based apprenticeship (at the upper-secondary level) after compulsory education. In addition, special options have been offered for some years now to adults who wish to obtain a Federal VET Diploma (SERI, 2021).
Participants and Procedure
The participants were a sample of 403 health and social care workers (96% female; M age = 29.5, SD = 9.6) holding a Federal VET Diploma in health care or social care. At the time of the survey in 2015 or 2016, participants had worked in these fields for about 4 years after receiving their Federal VET Diploma. The relatively high mean age of the participants in this study is not surprising, since VET for adults has become particularly popular in the health and social care sectors. The total sample consisted of 206 social care workers (97% female; M age = 31.5, SD = 10.3) and 197 health care workers (94% female; M age = 27.5, SD = 8.4). The vast majority of the participants were native Swiss (social care workers: 81%, health care workers: 75%). At the time of the survey 4 years after completion of VET, 63% of the health care workers and 20% of the social care workers had obtained a formal job-related or university-related qualification at the tertiary level.
Graduate social care workers assist people of different ages and in various facilities in everyday situations. Professionals with a tertiary education in social care work take on team and management tasks in the same area. Fifty-three percent of the 206 participating social care workers were specialized in child care, 27% in care of impaired people, 12% in elderly care, and 4% had generalist training for all three target groups. Most of them (37%) worked in small companies or institutions (between ten and 49 employees), and only 46% of them worked in shifts or on weekends.
Graduate health care workers work in hospitals, homes, and other health and social care facilities. There they take on tasks in nursing, nutrition, and administration. Health care workers differ from qualified nurses in the responsibility they assume and the profile of skills and competencies they have. Half of the 197 participating health care workers worked in the acute care sector, 32% worked in the long-term sector, 8% worked in home care organizations, and 10% worked in another sector. Most health care workers (43%) worked in large companies (250 employees or more), and 92% regularly worked in shifts or on weekends.
An online questionnaire was used to collect the data. Login data (web link, user name, and password) were sent to the individuals’ postal address by the vocational school where they trained. A total of 533 individuals responded to the questionnaire (return rate of 34%). Seventy-six percent of participants were still working in the health and social care sectors (some of them completed further training at the same time), resulting in a final sample of 403 individuals. American Psychological Association ethical standards were followed in the conduct of the study, including with regard to the treatment of human subjects.
Measures
Correlation Matrix and descriptives of the variables included in the structural equation model (see Figure 2).
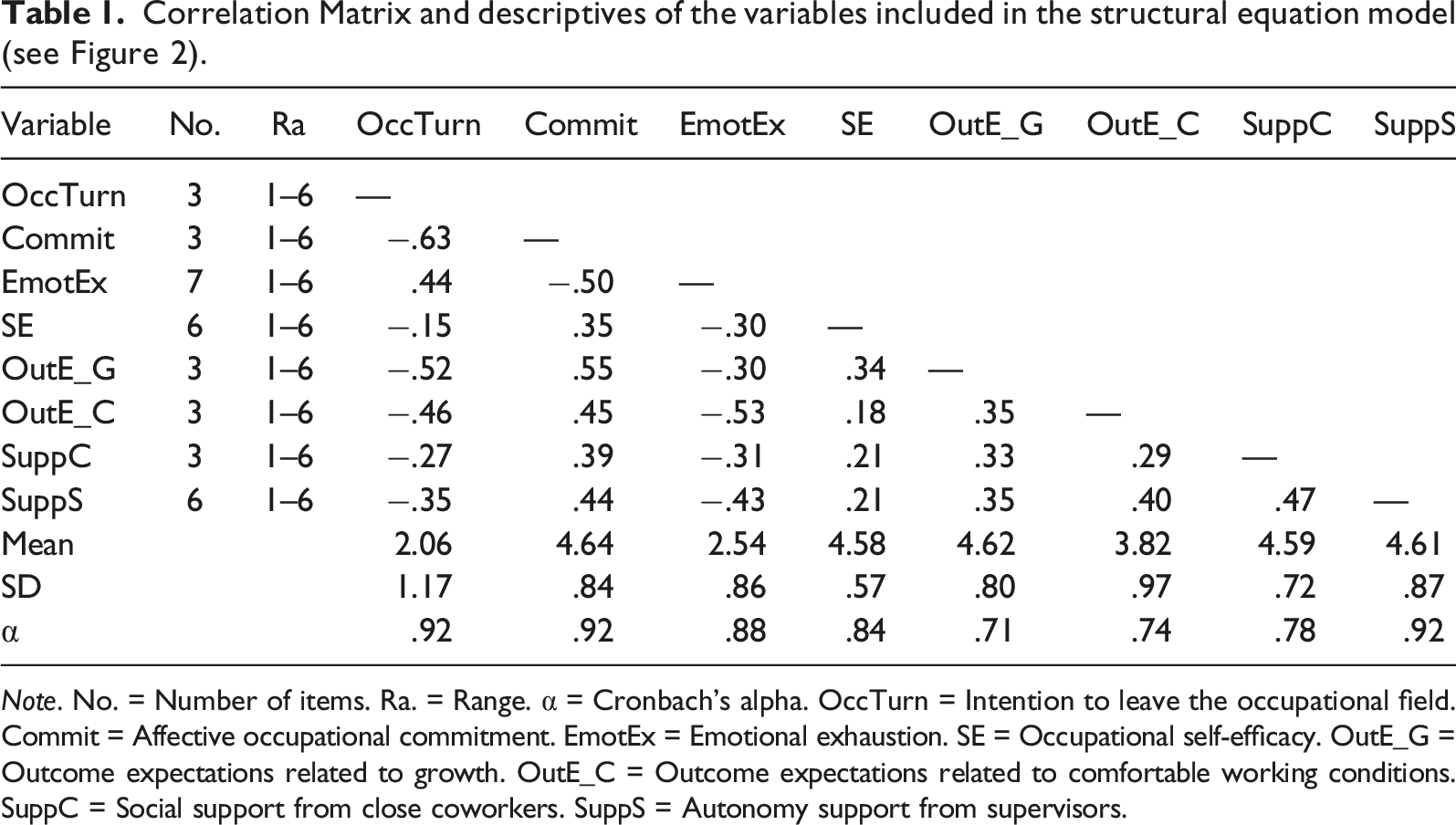
Note. No. = Number of items. Ra. = Range. α = Cronbach’s alpha. OccTurn = Intention to leave the occupational field. Commit = Affective occupational commitment. EmotEx = Emotional exhaustion. SE = Occupational self-efficacy. OutE_G = Outcome expectations related to growth. OutE_C = Outcome expectations related to comfortable working conditions. SuppC = Social support from close coworkers. SuppS = Autonomy support from supervisors.
Intention to Leave the Occupational Field
Health and social care workers’ occupational turnover intentions were measured using a modified version of the 3-item Career Withdrawal Cognitions scale (Blau, 1989) that was translated into German by a professional translator (note: we did not use the back-translation method). A sample item is “I intend to look for a different field of employment.” The original response scale was a five-point scale (1 = Very unlikely to 5 = Very likely), and the author reported an internal consistency of α = .84. Work by Blau et al. (2003) on the career patterns of recently graduated medical technologists has supported the discriminant validity of professional withdrawal cognitions versus organizational withdrawal cognitions at two measurement times (r = .67 and r =. .58). Blau et al. (2003) reported an internal consistency of α = .87 and α = .91 for their professional withdrawal cognitions three-item measure. Additionally, professional commitment as a work-related attitude had a strong negative relationship to subsequent professional withdrawal cognitions (r = −.42), demonstrating the construct validity of the Career Withdrawal Cognitions scale.
Occupational Commitment
To measure health and social care workers’ occupational commitment, we used the 6-item Affective Occupational Commitment scale from the standardized COMMIT questionnaire that was developed and tested on a norm sample of 11,119 individuals from 39 organizations by Felfe and Franke (2012), recording item responses originally on a five-point scale (1 = Disagree to 5 = Agree). This German-language adaptation and further development of the occupational commitment scale from Meyer et al. (1993) is one of six subscales that was systematically developed and psychometrically validated (Schilling, 2014). The COMMIT subscale Affective Occupational Commitment shows very good internal consistency of α = .91 (Felfe et al., 2002). A sample item is (originally in German): “I am proud to be in this profession.”
Emotional Exhaustion
Participants rated statements concerning the degree to which they feel depleted of energy and drained of sensation and responded using the 7-item Emotional Exhaustion subscale from MBI-D (Büssing & Perrar, 1992), a German version of Maslach and Jackson’s (1984) instrument for assessing burnout among health professionals. The original response scale was a seven-point scale (1 = Strongly disagree to 7 = Strongly agree). The psychometric properties of the instrument were tested with 449 male and female West German nurses and nursing students (Büssing & Perrar, 1992). The validity of the German subscale on emotional exhaustion could be confirmed. It showed a very good internal consistency of α = .91, and the criteria for convergent validity that was tested with five relevant scales (psychosomatic complaints, irritability/stress, burnout measure subscales) lay between r = .40 and r = .55. A sample item is “I feel burned out from my work.”
Occupational Self-Efficacy
Participants’ occupational self-efficacy was measured using a 6-item German short version (Rigotti et al., 2008) of the Occupational Self-Efficacy scale (Schyns & von Collani, 2002). Structural and construct validity was assessed across five countries (including Germany). The reliability coefficients were between α = .85 (Belgium) and α = .90 (Great Britain) and supported a good internal consistency. Across the five countries, substantial partial correlations could be found between occupational self-efficacy and job satisfaction (r = .17 for Germany and r = .46 for Sweden) as well as (except for Great Britain) commitment (r = .16 for Spain and r = .39 for Sweden). The original response scale was a seven-point scale (1 = strongly disagree to 7 = strongly agree). A sample item is “When I am confronted with a problem in my job, I can usually find several solutions.”
Career-Related Outcome Expectations
Participants were asked to rate their outcome expectations, if they were to continue working in the health and social care sectors, regarding both (a) professional growth and (b) comfortable working conditions using a 3-item scale for both components. To measure individuals’ outcome expectations, we selected and adapted items from Meyer et al.’s (1998) Work Value and Work Experience inventory, namely, from the component Comfort and Security as well as Competence and Growth. The authors tested their inventory on the basis of two studies with a total sample of 522 university graduates, and both components showed good internal consistency (Study 1: α = .65 and α = .83, Study 2: α = .73 and α = .84). A professional translator translated the items into German. In their study, participants were asked to indicate how characteristic each of a set of descriptors was of their jobs (1 = not at all characteristic to 5 = extremely characteristic), including aspects of growth and comfort. In this study, this inventory was used to assess expectations of whether workers would continue working in their fields. The following are sample items: “[If I continue working in the health care field] I can continuously develop my knowledge and skills” (growth), and “[If I continue working in the social care field] I have ample leisure time/time for private life” (comfortable working conditions).
Social Support From Close Coworkers
Participants rated the degree to which they felt supported by close coworkers using a 4-item scale adapted from the Social support from close colleagues scale (Van der Heijden, 2003), recording item responses on a six-point scale and with an internal consistency of α = .74. A professional translator translated the items into German. A sample item is “Are your close coworkers in general ready to help you with the performance of your tasks?” The scale was also used and psychometrically validated with more than 38,000 nurses in 10 European countries (Kümmerling et al., 2003). The internal consistency proved to be good in all countries and ranged from α = .72 (Belgium and Poland) to α = .79 (Germany and Great Britain).
Autonomy Support From Supervisor
We measured autonomy support from the supervisor using a 6-item German version (Nickenig, 2014) of the Autonomy Support from Supervisor subscale of The Work Climate Questionnaire (Baard et al., 2004). Nickenig (2014) tested the German version of the scale on the basis of a survey of 151 employees of the Leibniz Institute of Agricultural Engineering (α = .91). A sample item is “My supervisor listens to how I would like to do things.” The original response scale was a five-point scale (1 = strongly disagree to 5 = strongly agree). Baard et al. (2004) found perceptions of managerial autonomy support to be positively correlated with employees’ intrinsic needs satisfaction (including satisfaction of the need for autonomy, r = .32, p < .05), which in turn predicted their performance and psychological adjustment, thus confirming its validity.
Model Specification
We performed multivariate regression analyses using the multigroup structural equation modeling (SEM) in MPlus Version 7 (Muthén & Muthén, 1998–2015). We used maximum likelihood estimations with robust standard errors (MLR estimator). Full information maximum likelihood (FIML) was used to specify the model so that cases with missing values on predictors were included. Figure 2 shows the estimated model. Given the size of the model and the study’s sample size, all variables were included in the model as manifest (i.e., observed) variables. For each scale, we averaged the scores across relevant items, with higher scores reflecting a greater expression of the variable (e.g., greater intention to leave the occupational field, greater affective occupational commitment). Table 1 provides the correlation matrix for this model and displays the number of items, the range, the (estimated) mean and standard deviation, and Cronbach’s alpha for each variable. We included age (at the time of the survey, in years) as a control variable in the model by regressing workers’ intention to leave the occupational field on age. We also tested the indirect effects of emotional exhaustion, social cognitive factors, and organizational support on health and social care workers’ intention to leave the occupational field. Predictors of professionals’ intention to leave their occupational field, controlling for age. N = 403. Note. Standardized model parameters are shown. Dotted paths are not significant at the .05 level. R
2
for health care group is in parentheses. Two path coefficients (occupational self-efficacy → outcome expectations related to growth and autonomy support from supervisor → outcome expectations related to comfortable working conditions) significantly differ between the groups, β for health care group is in parentheses. There is no significant association between the control variable and social support from close colleagues and autonomy support from the supervisor (not displayed in Figure 2). Indirect associations are not displayed in Figure 2.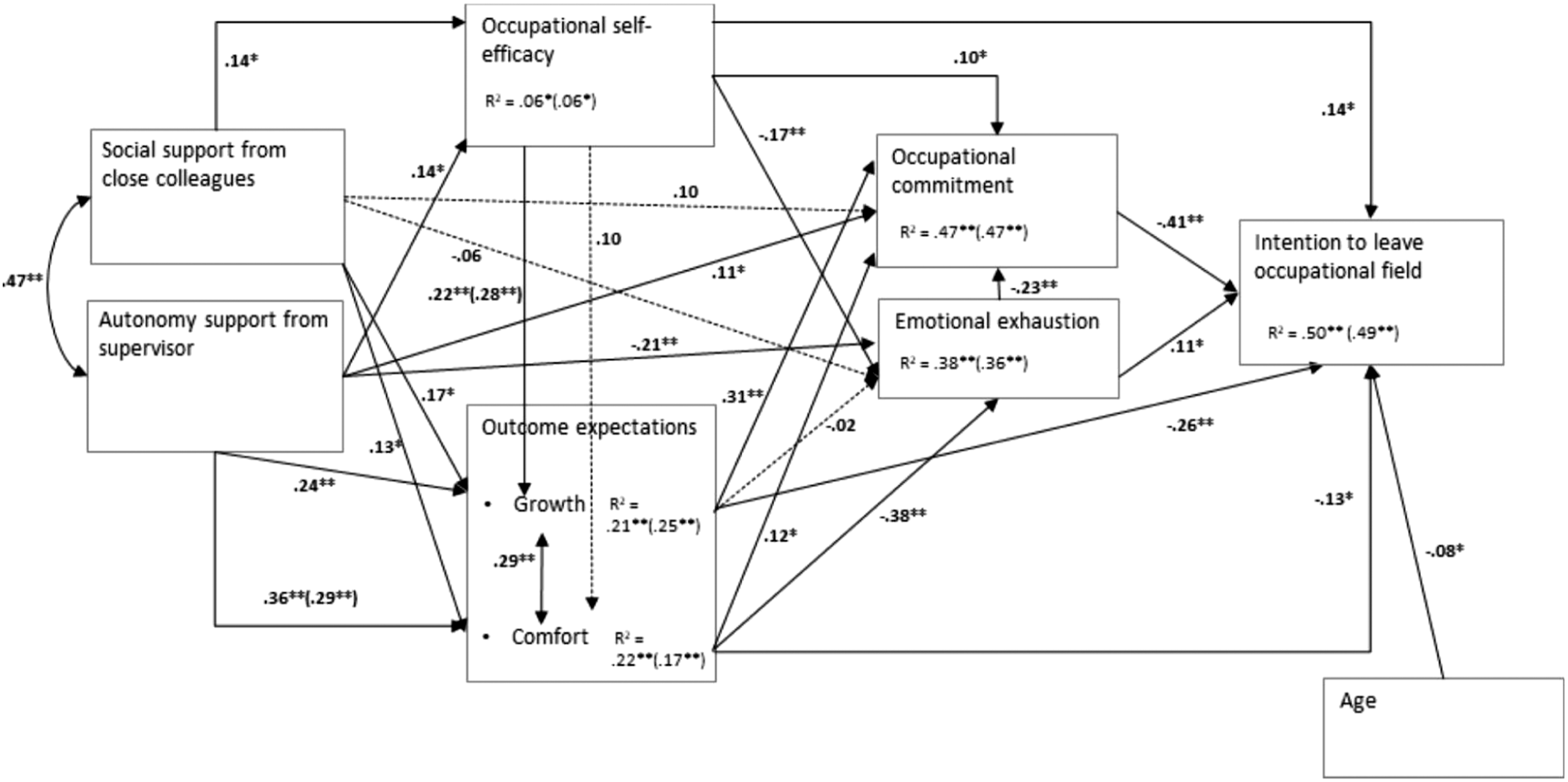
To test whether the model is valid across occupations, we performed a multigroup comparison in three steps. First, an unconstrained model was estimated, in which all parameters were allowed to vary across the two groups of workers, which indicated a good fit [χ2 (14) = 29.853, p < 0.01, CFI =. 980, RMSEA = . 075, SRMR = . 031]. Second, all parameters were constrained to equality across the groups to obtain the fully constrained model, which yielded a poor model fit [χ2 (61) = 149.630, p < 0.01, CFI = . 885, RMSEA = . 085, SRMR =. 131]. The results of difference testing using the MLR chi-square confirmed that the fit of the unconstrained model was significantly better than that of the fully constrained model [χ2 (47) = 118.877, p < 0.01]. Third, the equality constraint with the largest modification index in the fully constrained model was released to obtain a partially constrained model. The partially constrained model was compared to the unconstrained model. We repeated the last step until no significant chi-square test difference between comparative models was found. In the best fit model [χ2 (59) = 87.843, p < 0.01, CFI =. 963, RMSEA =. 049, SRMR =. 109], equality constraints on two path coefficients were released (occupational self-efficacy → outcome expectations related to growth, autonomy support from supervisor → outcome expectations related to comfortable working conditions), indicating significant differences in these two path coefficients across the groups. The following descriptive measures were used to assess model fit (Browne & Cudeck, 1993; Hu & Bentler, 1998): comparative fit index (CFI; values above 0.95 indicate a good model fit) and root mean square error of approximation (RMSEA; values below 0.06 indicate a good model fit, and values below 0.08 are still adequate), and standardized root mean square residual (SRMR; values below 0.08 indicate a good model fit). The chi-square test of model fit was used to test the null hypothesis that the proposed model fits exactly in the population, which is a very strict assumption (i.e., the p-value of this test is often significant).
Results
Explaining the Variability in Workers’ Intention to Leave Their Occupational Field
Preliminary analyses, including descriptive statistics, revealed that health and social care workers’ occupational turnover intentions were rather low (M = 2.05, SD = 1.17, see Table 1). Based on the results, about 9% of the individuals who still work in health and social care 4 years after completing VET (N = 403) do strongly or do rather intend to leave the sector.
The multigroup analysis revealed no significant differences between the group of social care workers and the group of health care workers, except for two path coefficients in the model displayed in Figure 2 (occupational self-efficacy → outcome expectations related to growth and autonomy support from supervisor → outcome expectations related to comfortable working conditions), resulting in a small difference in the total explained variance in workers’ intention to leave the occupational field across the groups. It was 50% in the group of social care workers and 49% in the group of health care workers. The SEM results show that, as expected (H1), higher affective occupational commitment (β = −.41) and positive outcome expectations (growth: β = −.26, comfortable working conditions: β = −.13) were associated with lower occupational turnover intentions. However, contrary to expectations (H1), workers’ occupational turnover intentions were higher when they reported experiencing higher occupational self-efficacy (β = .14). Furthermore, as expected (H1), turnover intentions were higher when they reported feelings of emotional exhaustion (β = .11). Workers’ emotional exhaustion was negatively related to their affective occupational commitment (β = −.23). Outcome expectations with regard to growth as well as with regard to comfortable working conditions were positively correlated (r = .29). We found small age-related differences in workers’ occupational turnover intentions: they were lower with increasing age (β = −.08).
Total indirect effects of emotional exhaustion, social cognitive factors, and organizational supports on health and social care workers’ intention to leave their occupational field.
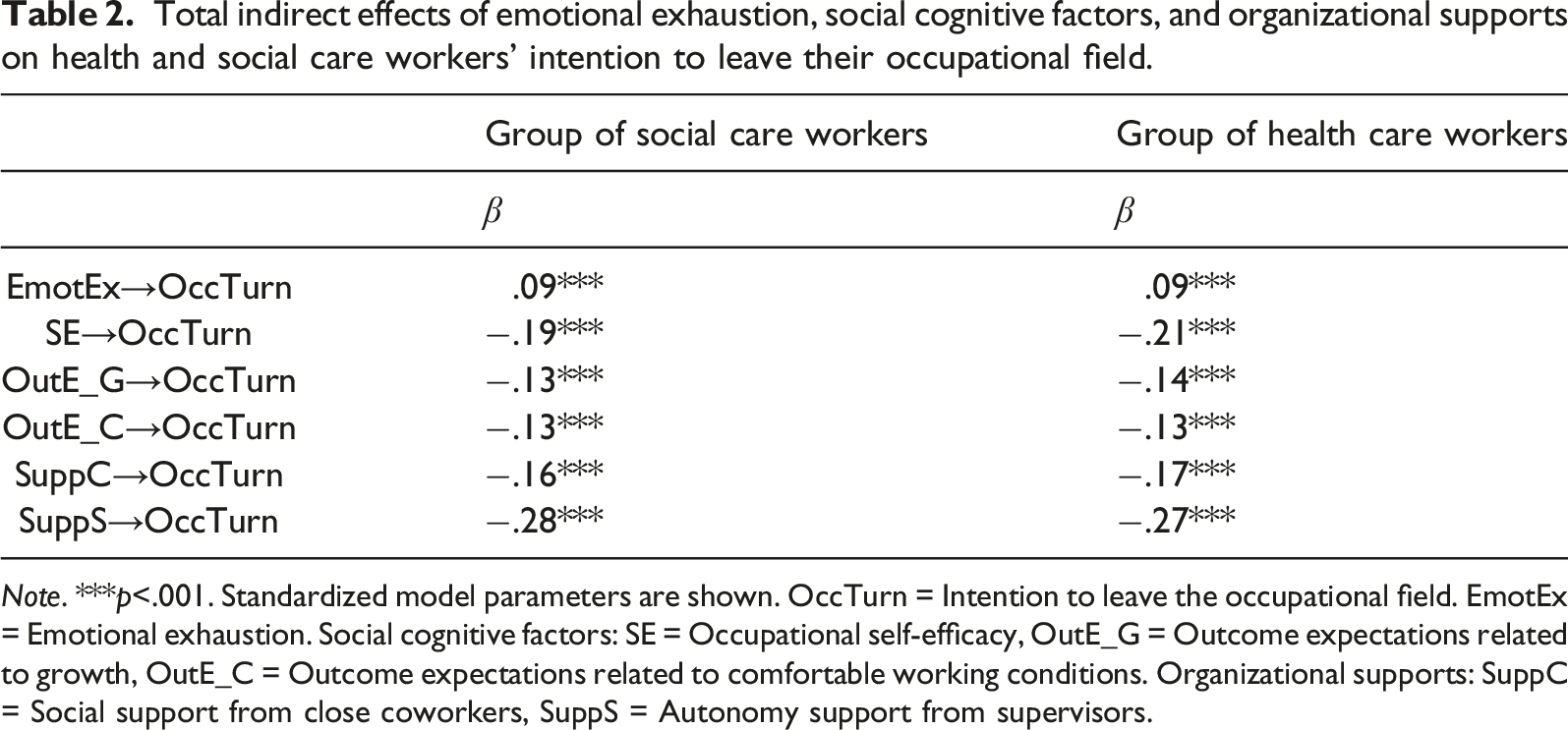
Note. ***p<.001. Standardized model parameters are shown. OccTurn = Intention to leave the occupational field. EmotEx = Emotional exhaustion. Social cognitive factors: SE = Occupational self-efficacy, OutE_G = Outcome expectations related to growth, OutE_C = Outcome expectations related to comfortable working conditions. Organizational supports: SuppC = Social support from close coworkers, SuppS = Autonomy support from supervisors.
Associations Between Social Cognitive Factors, Job Attitudes, and Wellbeing
The results show that, as expected (H2), health and social care workers with higher occupational self-efficacy (β = .10) and positive outcome expectations (growth: β = .33, comfortable working conditions: β = .12) reported higher occupational commitment. Furthermore, occupational self-efficacy (β = −.17) and positive outcome expectations related to comfortable working conditions (β = −.38) were negatively associated with emotional exhaustion. Thus, as expected (H2), individuals reported feeling less exhausted when they perceived themselves to be self-efficacious and when they anticipated positive outcomes related to comfortable working conditions. We observed a slight trend indicating that positive outcome expectations related to growth were also negatively associated with emotional exhaustion; however, this association was not statistically significant (β = −.02). Finally, we found a positive association between occupational self-efficacy and outcome expectations related to growth. The results of a multigroup comparison show that this association was stronger in the health care group (β = .28) than in the social care group (β = .22). The association between occupational self-efficacy and outcome expectations related to comfortable working conditions was not significant (β = .10). The model shown in Figure 2 was able to explain 47% of the total variance in health and social care workers’ occupational commitment. The total explained variance in their emotional exhaustion was 38% in the group of social care workers and 36% in the group of health care workers.
Positive Influences of Support From Close Coworkers and Supervisors
Autonomy support from supervisors was found to be a source of self-efficacy (β = .14) and positive outcome expectations with regard to growth (β = .24) as well as with regard to comfortable working conditions (H3), albeit to a different degree in the two groups. The association between autonomy support from supervisors and positive outcome expectations with regard to comfortable working conditions was stronger in the social care group (β = .36) than in the health care group (β = .29). Autonomy support from supervisors was also found to be a source of occupational commitment (β = .11) and wellbeing (H3). That is, individuals who reported that their supervisor listens to them and provides them with choices and options also reported feeling less exhausted (β = −.21).
Positive associations were also found between social support from close coworkers and occupational self-efficacy (β = .14) as well as outcome expectations related to growth (β = .17) and comfortable working conditions (β = .13, see H3). However, the associations between social support from close coworkers and occupational commitment (β = .10), and between social support from close coworkers and emotional exhaustion (β = −.06) were not significant. We found a medium positive correlation between social support from close coworkers and social support from supervisors (r = .47, Cohen, 1988). The model shown in Figure 2 could explain 21% of the total variance in social care workers’ outcome expectations related to growth, 22% of that in their outcome expectations related to comfortable working conditions, and 6% of that in their occupational self-efficacy. In the health care group, the model could explain 25% of the total variance in workers’ outcome expectations with regard to growth, 17% of that in their outcome expectations with regard to comfortable working conditions, and 6% of that in their occupational self-efficacy.
Discussion
The main contribution of this study is a better understanding of variables associated with health and social care workers’ voluntary turnover intentions drawing upon SCCT-based theoretical framework models of career self-management and career change (Lent & Brown, 2013; Fouad et al., 2016, 2017; Singh et al., 2013). The current study not only applies Singh et al.’s (2013) SCCT model to occupational turnover intentions and a traditionally female area of work, but also extends it by integrating emotional exhaustion as an explanatory variable. Even though the relationship between emotional exhaustion and turnover is well researched (e.g., Blau, 2007; Leiter & Maslach, 2009) and health and social care workers are at increased risk of becoming emotionally exhausted and developing burnout (e.g., Itzick & Kagan, 2017; Van der Heijden et al., 2019), this variable has not been included in SCCT career change models before.
The first important finding of this study is that affective occupational commitment showed the highest negative correlation with workers’ intention to leave the health and social care sectors. This is in line with findings from Fouad et al. (2016), who found occupational commitment to be a key explanatory variable for career continuation in a chosen field. The finding also corroborates H1. The newly added explanatory variable emotional exhaustion was, as expected (H1), positively, though weakly, related to occupational turnover intentions (e.g., Blau, 2007; Cropanzano et al., 2003). In accordance with findings from other occupational fields (Major et al., 2013), our results show that emotional exhaustion also indirectly influences workers’ occupational turnover intentions, mediated by occupational commitment (Cropanzano et al., 2003). These results support the current claim (Medici et al., 2020) to consider strain as a focal predictor of career change. We also found significant associations between occupational turnover intentions and outcome expectations related to growth and, to a lesser extent, outcome expectations related to comfortable working conditions as well as occupational self-efficacy. Contrary to expectations, the direct association between occupational self-efficacy and occupational turnover intentions was positive. That is, workers’ intention to leave their occupational field was higher when they reported experiencing higher occupational self-efficacy. However, consistent with studies that identified overall work attitudes and engagement as mediators of the influence of self-efficacy beliefs on turnover intentions (Park & Jung, 2015; Singh et al., 2013), the total indirect effect from occupational self-efficacy on the intention to leave the occupational field was negative. This is an indication that self-efficacy beliefs enable adaptive behavior: on the one hand, by buffering stress (Rigotti et al., 2008), they can strengthen commitment and intention to stay. On the other hand, beliefs of one’s own efficacy can also motivate a career change if commitment declines and the prospects for further advancement in the chosen occupation are unfavorable.
A second important finding is that, among the predictors considered in the model, workers’ expectations related to development opportunities (growth) when pursuing their careers showed the strongest positive association with affective occupational commitment, and outcome expectations related to the availability of time for leisure activities and personal life (comfort) when pursuing their careers showed the strongest negative association with emotional exhaustion. According to SCCT, outcome expectations reflect specific learning experiences. Our results indicate that enabling positive experiences with regard to work–life balance already at the start of the career is particularly important for workers’ wellbeing and motivation to continue their careers in a sector with irregular working hours and weekend shifts. In the health and social care sectors, where skilled workers are in short supply and which are currently also heavily burdened by the ongoing pandemic, this finding takes on additional weight. In line with previous findings (Bakker & Demerouti, 2017; Fouad et al., 2016), positive experiences related to growth/advancement opportunities in the career entry phase, strengthen the anticipation of corresponding outcomes of future working conditions (Brown & Lent, 2019). Compared to anticipated outcomes with regard to work–life balance, outcomes with regard to growth have a greater impact on workers occupational commitment, and on occupational turnover intentions. The results reveal the importance of outcome beliefs and the learning experiences behind them for the career development process. With regard to the theoretical implications of the study, our results support findings that the motivational process and the health-impairment process do not run independently (Bakker & Demerouti, 2017), but that stress is an additional factor in the network of social cognitive predictors that weakens commitment and, via this pathway, promotes the likelihood of career change.
A third noteworthy finding is that, in line with hypothesis 3, autonomy support from the supervisor was positively associated with workers’ career-related outcome expectations, occupational self-efficacy, and occupational commitment, and was negatively associated with emotional exhaustion. This variable also showed an indirect negative association with turnover intentions. We additionally found positive associations between social support from close coworkers and both outcome expectations as well as occupational self-efficacy. However, contrary to expectations, social support from close coworkers was not significantly related to emotional exhaustion and occupational commitment; it thus probably unfolds its effect exclusively through its indirect influence on turnover, mediated by self-efficacy and outcome expectations beliefs. One interpretation of this finding is that autonomy support from the supervisor gives health and social care workers a certain amount of room to maneuver and thereby a sense of self-determination, which can have a positive effect on their health and wellbeing, as well as on their emotional attachment to the occupation. Overall, our study emphasizes the importance of supportive managerial behaviors and support from close work colleagues (Jungert et al., 2021) and affirms the findings of the underlying model (Singh et al., 2013) on the role of workplace support. The results are also consistent with the well-documented findings on the positive effect of an autonomy-supportive work environment, or perceived autonomy, on motivational factors and the wellbeing of employees (Fernet et al., 2013). In contrast, close coworkers are not in the same position to provide room to maneuver, and their assistance is rather limited to direct support in performing, reflecting on, and relieving work tasks, as well as to compassion. They lack the competencies for a sustainable impact on structural working conditions and formal requirements. The results suggest that, unlike with direct supervisors, close coworkers are not perceived as representatives of the organization that provides the structural framework for professional practice. However, through their willingness to help and assist, they can provide positive (competence) experiences for their colleagues and positively influence their colleagues’ expectations to perform well at work tasks. To sum up, our results suggest that Singh et al.’s (2013) SCCT model can be applied to occupational turnover, and that it is important to incorporate strain as a predictor of career change (Medici et al., 2020).
Practical Implications
Workers’ affective occupational commitment was the most important predictor of occupational turnover intentions, which underlines the importance of the affective aspects of attitudes in understanding career change (e.g., Lee et al., 2000; Singh et al., 2018) and the necessity of designing effective interventions that prevent the attrition of qualified staff from the chosen field after starting a career. It might be important to pay particular attention to factors fostering and undermining workers’ affective occupational commitment, not only in the workplace but from the very beginning of the career development process (Salzmann et al., 2018). The results of this study provide evidence that emotional exhaustion undermines commitment and thereby influences occupational turnover intentions. Said results corroborate the importance of workers’ career-related outcome expectations and suggest that positive experiences related to growth foster occupational commitment, whereas positive experiences related to working conditions (e.g., work–life balance) are particularly important to prevent emotional exhaustion. In this regard, considering workers’ desire for professional development and listening to their opinions about how they would like to do tasks, giving them a certain amount of room to maneuver, and enabling them to experience self-determination seem to be particularly effective measures, while also individually being promising approaches to promote self-efficacy beliefs. These findings can be located within work autonomy and need satisfaction, a complex theme which is classified as essential in order to create attractive work environments (Pursio et al., 2021) and which turned out to be always beneficial with regard to supportive behavior in occupational contexts (Jungert et al., 2021). Although our data show that expected consequences in terms of professional growth are (still) more important in this career phase for career retention, these working conditions will increasingly play a greater role with regard to work-family conflict (Singh et al., 2018). An important avenue for future studies would be to measure workplace support and job resources in a more differentiated manner to determine which characteristics are important (e.g., form, source, and timing of support) for promoting workers’ social cognitive factors, job attitudes, and wellbeing.
Limitations and Future Directions
Our study focused on workers’ intention to leave the health and social care sectors 4 years after completing their VET. It would be of value to also examine occupational turnover intentions and related factors at a later point in time (e.g., 10 years after completing VET) to determine how occupational turnover intentions develop over time and to examine the reasons for such changes. Furthermore, the relationship between workers’ intention to leave and their actual turnover should be studied in more detail, which would require longitudinal data.
A methodological strength of this study is that the applied measures are widely used with adult populations. Our results can thus be contextualized in regard to those of previous studies using these measures. However, to our knowledge, some of the scales have not been previously used in the context of health and social care. More research is needed to test them in this context.
A first limitation of this study is related to the sample used. In total, 533 individuals responded to the questionnaire. Of these, 403 individuals were included in the analyses. We do not know to what extent non-participation was random or affected by some systematic factors that may have biased our findings. Replicating the study’s methodology across different contexts will reveal to what extent the findings from this study may be generalizable to other populations of employees in other sectors or in other countries. A second limitation is related to the design of the study. Because the data are cross-sectional, the tested model cannot be used to test cause-and-effect relationships. To prove causality, an experimental design would be required that maintains a time lag between the measurement of the predictor and criterion variables. Third, the measures of all variables were self-reported and obtained from the same person; this can be a potential source of common method biases. We do not know how strong the potential impact of common method biases on the measures of the constructs used are, and the same is true of the impact of method biases on the observed relationships between the measures. This limit could be alleviated in further studies by supplementing the data with third-party reports (e.g., from supervisors and coworkers).
Footnotes
Acknowledgments
We would like to express our gratitude to the Foundation Suzanne and Hans Biäsch, to the Federal Office of Public Health, Healthcare Professions Division, and to the St. Gallen University of Teacher Education, Switzerland for the financial support of this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Foundation Suzanne and Hans Biäsch, St. Gallen University of Teacher Education, Federal Office of Public Health, Healthcare Professions Division.