
Abstract
Caring as a central focus within nursing has evolved into a relational ontology to guide practice and enhance well-being. Caring praxis has the potential to address the complexities of adolescent development and to allow for authentic engagement, breaking down the barriers of resistance to care. It is clear from the alarming statistics related to the prevalence of anxiety and depression in adolescents that teens are in distress. The authors in this article examine the construct of relatedness in adolescence through the lens of the theory of unitary caring and propose a trans-theoretical transdisciplinary model of relatedness that informs adolescent practice.
Caring as a central and defining concept within the discipline of nursing has been at the forefront of philosophical, theoretical, and contextual discourse for decades (Smith, 1999; Watson & Smith, 2002). This scholarly debate has fundamentally enriched our knowledge of caring science that focuses on the wholeness of one’s experience and the processes that support relationship, integration, and transformation. The authors’ aim to examine how a unitary caring worldview can inform the construct of relatedness in adolescent development and suggest a transtheoretical transdisciplinary model as a relational caring ontology to guide interprofessional practice in the care of adolescents. By understanding the issues adolescents encounter through the lens of the unitary caring theory, the meaning of relatedness can be expanded to guide nursing practice. The authors here present an overview of unitary caring science as a relational ontology, address the psychosocial and emotional concerns affecting adolescents today, discuss the influence of developmental encounters, examine relatedness as a construct essential for well-being, and review the middle-range theory of unitary caring as a guiding framework to enhance care.
Unitary Caring Science
Through a creative synthesis of two dominant discourses in nursing theory, the science of unitary human beings and transpersonal caring science, Watson and Smith (2002) proposed unitary caring science as a transtheoretical, transdisciplinary context of a relational caring ontology that informs knowledge in nursing and other disciplines. Ontology in unitary science embraces cosmology, a branch of metaphysics that focuses on the nature of the universe as open systems and addresses questions beyond the scope of physical science. From a metaphysical-ontological context, unitary caring science theories advocate the infinite human-environment energy fields distinguishable by patterns integral to the universe and aid in describing and explaining phenomena, assert values, and guide research and praxis (Watson & Smith, 2002).
Human caring is an experience that is invisible and frequently overlooked in practice. Watson and Smith (2002) posited that the phenomenon and practice of human caring are essential for sustaining life itself. A central component of conceptualizing caring as the transpersonal relationship between nurse and patient is knowing the patient (Smith, 1999) as they coexist within the environment. Saewyc (2000) echoed Watson’s position on the importance of applying caring theories to adolescent practice. She posited caring as a central concept for nursing practice and emphasized the implicit need to embrace caring science as a guiding framework for establishing an authentic way of being with adolescents. Aligning with unitary caring science and Saewyc’s proposal, the middle-range theory of unitary caring (Smith, 1999, 2015, 2020) was chosen as a theoretical lens to frame the construct of relatedness. From this theoretical framework, encounters and changes in adolescence are observed through an irreducible human wholeness that transcends the conceptual labels of bio-psycho-social and acknowledges growth and development as the mutual process and rhythmic waves of energy fields, discovering patterns of wholeness that motivate human life and relationships (Smith, 1999, 2015, 2020).
Adolescent Well-Being: A Critical Need
There is a growing local and national concern regarding the alarming increase in adolescent mental health disorders, anxiety, depression, and suicide. Recent national surveys suggest that between 13% and 20% of children in the U.S. are diagnosed with mental, emotional, or behavioral disorders at some point during childhood or adolescence (Ghandour et al., 2019).
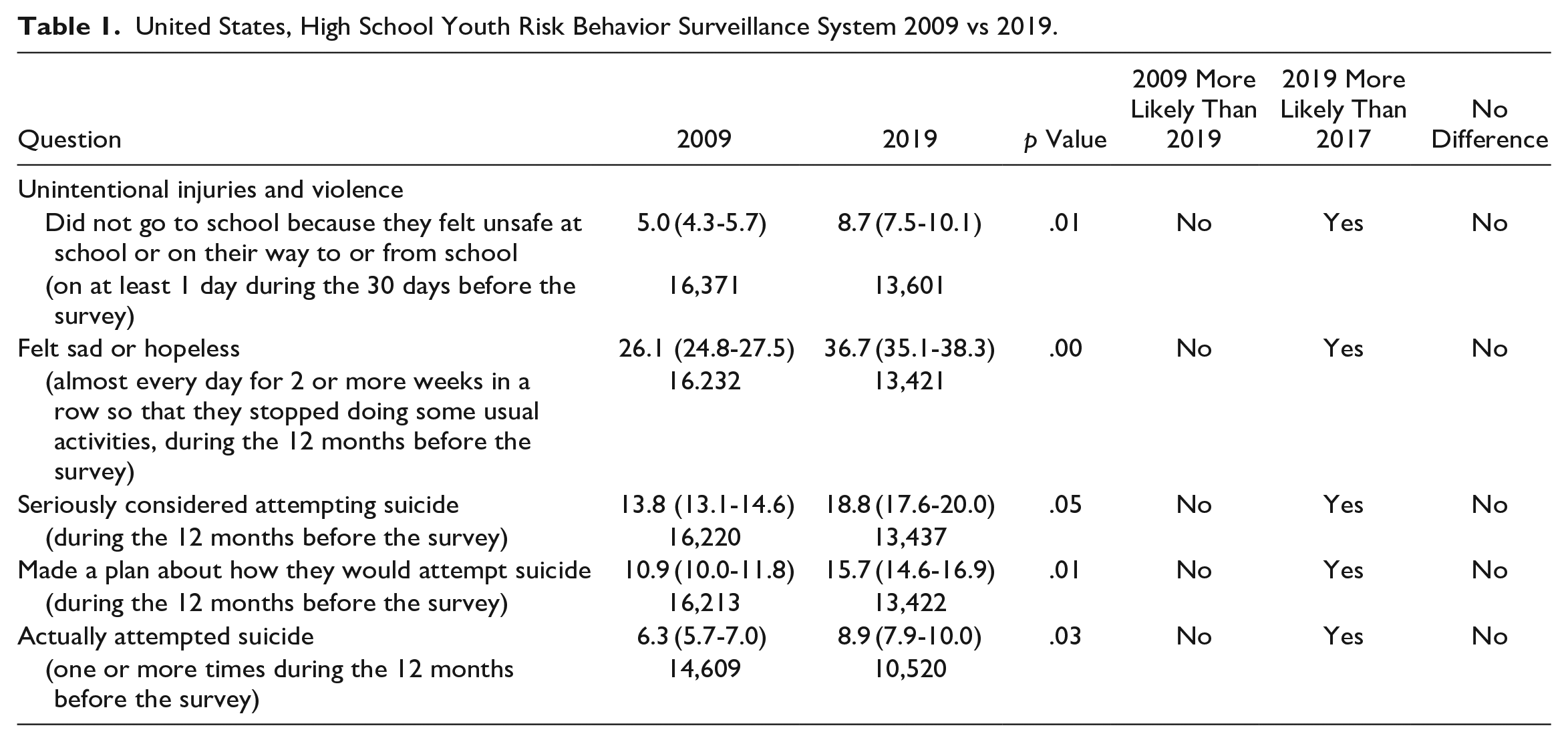
The Youth Risk Behavior Surveillance System (YRBSS) is a tool developed in 1990 by the Centers for Disease Control and Prevention (CDC) to monitor and track adolescent health behaviors that contribute to the leading causes of death, disability, and social problems (CDC, 2020b). The results of this survey, conducted every two years, provide a longitudinal picture and trendline of the priority health behaviors and experiences that affect the health and well-being of adolescents over time. According to recent results from the YRBSS (CDC, 2020b), five indicators that address anxiety, depression, and suicide have shown a statistically significant increase over the past 10 years, 2009 vs. 2019 (Table 1).
United States, High School Youth Risk Behavior Surveillance System 2009 vs 2019.
They have also demonstrated substantial growth over the past two years, 2017 vs. 2019 (Table 2).
United States, High School Youth Risk Behavior Surveillance System 2017 vs 2019.
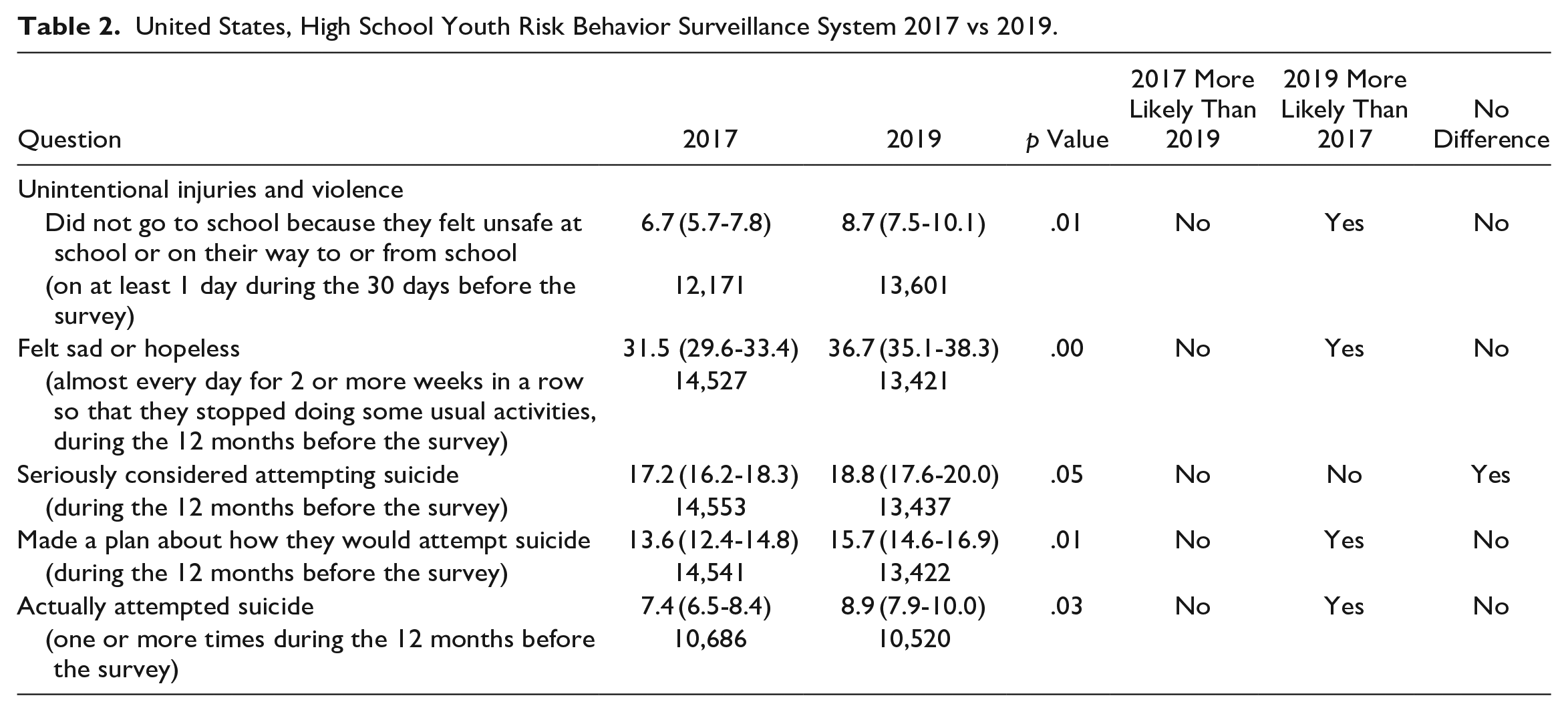
Of heightened concern are the 2019 increases for the following questions: not going to school for feeling it was unsafe (8.7%), feeling sad or hopeless (36.7%), seriously considered attempting suicide (18.8%), making a plan on how they would attempt suicide (15.7%), and actually attempted suicide (8.9%) (CDC, 2020b).
Despite these growing trends’ profound public health implications, mental health treatment utilization for adolescents remains low, with some children receiving no treatment at all (Ghandour et al., 2019). Although the numbers from the 2016 National Survey of Children’s Health monitoring the prevalence of youth experiencing psychological distress reflect higher treatment percentages, 80% for depression and 59% for anxiety, treatment adherence is questioned (Ghandour et al., 2019). Oruche and colleagues (2014) estimate that 40%-60% of the youth receiving mental health treatment drop out before completing their therapy sessions, contributing to worsening symptoms and unwillingness to participate in treatment in the future. Further data from this study suggested that the quality of the therapeutic relationship accounts for the most significant variance in treatment engagement and differentiates those who will complete treatment from those who drop out (Oruche et al., 2014).
Clinicians recognize that access to care and shortage of services influence initiation and treatment adherence (Ghandour et al., 2019). However, adolescent resistance to care is further amplified by the lack of youth-friendly interventions, adolescent-centered approaches, and depersonalized care, substantially widening the treatment gap for this population (Platell et al., 2020). These dispiriting challenges have significant implications on an individual’s service engagement, patterns of self-stigmatization, and mental health outcomes (Platell et al., 2020). Recognizing the barriers that have hindered the utilization and effectiveness of traditional mental healthcare for adolescents, nurses have the opportunity to research and develop innovative alternative therapeutic interventions and improve engagement with this population that might otherwise be resistant to care.
Heightening the urgency to address adolescent distress is the current stress, fear, grief, and uncertainty created by the COVID-19 pandemic (American Academy of Pediatrics [AAP], 2020). During a crisis like COVID-19, teens are more likely to experience feelings of isolation, anxiety, and depression, known risk factors for suicidal ideation and suicide (CDC, 2020a). In addition, adolescents may try to hide their struggles because of fear, shame, or a sense of responsibility to avoid troubling others (AAP, 2020). The current environmental conditions of a global pandemic and the disturbing patterns of adolescent mental health should be a catalyst for nurses working with adolescents to advocate for their care and heighten awareness and the urgent need for improved care. Teens need our help today.
Adolescent Development
Adolescence is a developmental phase where youth encounter biological, psychological, and emotional changes that transform children into young adults, preparing them for adulthood. As a complex transition, youth move from dependence to independence and interdependence, transforming from a dependent child to a more independent adult, seeking autonomy, and wanting freedom from their parents and acceptance from their peers (Newman & Newman, 2016).
Developmental transitions in the life process are central concepts of interest for nurse theorists, researchers, and clinicians, identified as a phenomenon of concern requiring inquiry and nursing knowledge development (Smith, 2019). Transitions expose individuals to personal and environmental challenges that trigger new roles, loss of networks, support systems, and response patterns that affect their psychosocial and emotional well-being (Meleis, 2010). Response patterns may show signs of an unhealthy transition, including distress, irritability, anxiety, and depression, accompanied by changes in self-concept, self-performance, and self-esteem (Meleis, 2010).
Erikson’s psychosocial theory acknowledges the stages of adolescent development and depicts the patterns of change in self-concept based on biopsychosocial encounters, including new cognitive capacities, new learning, and new relationships (Newman & Newman, 2016). Like the transitions theory, the psychosocial theory "seeks to explain changes in self-understanding, social relationships, and one’s relationship with society as a product of interactions among biological, psychological, and social systems" (Newman & Newman, 2016, p. 227). According to Erikson, the essential developmental tasks include resolving the identity versus role confusion crisis, developing a sense of identity, and finding the social environment where they can belong and establish meaningful relationships (Newman & Newman, 2016).
The struggle, or crisis, as identified by Erikson is that adolescents must resolve to find the balance between developing a genuine sense of identity while still feeling accepted and fitting in (Newman & Newman, 2016). The key to negotiating this crisis rests in the interactions with others. If adolescents successfully navigate this crisis, they will emerge with a clear understanding of their true identity or sense of self, emitting self-confidence and openly interacting with others without losing sight of who they are (Newman & Newman, 2016). However, if they are unable to navigate this task, they can become socially disconnected and struggle to understand their identity and self-worth. These beliefs and behaviors may affect their well-being, lasting well into adulthood (Newman & Newman, 2016; Resnick et al., 1997; Steiner et al., 2019).
Acknowledging the inherent challenges of the transition to adolescence, researchers seek to understand why some adolescents appear to navigate the transition with ease, while in contrast, others seem more susceptible to developmental stressors. Appreciating risk factors for teens who struggle during this phase is vast. However, data have emerged about protective factors that support and help teens cope with the uncertainty. These protective factors that enhance adolescent well-being include relatedness, connectedness, and belonging (Hagerty et al., 1993; Resnick et al., 1997; Steiner et al., 2019).
The seminal work of Resnick et al. (1997) identified the lack of connectedness in adolescence as the most powerful predictor of adolescent maladjustments, such as emotional distress, suicidal ideation, violence, and substance use. Recent work by Steiner and colleagues (2019) corroborates Resnick’s findings. The researchers followed adolescents from middle school into their 20s and 30s. The results showed that higher levels of connectedness were associated with as much as a 66% lower risk in the areas of mental health, violence, sexual exposure, and substance use. As a result of their work, the director of CDC’s Division of Adolescent and School Health, Kathleen Ethier, emphasized the need to encourage adolescent connectedness to help protect against significant health threats and increase feelings of belonging (CDC, 2019). Theorists agree that through meaningful connections, individuals can establish relatedness to self, others, and the environment, creating a way of being where persons coexist and co-evolve with their environment to survive, develop, and grow (Hagerty et al., 1993; Steiner et al., 2019). The importance of using relatedness models to equip clinicians has been stressed to better assist clients in seeing, understanding, and maximizing opportunities to improve connectedness to self and the world around them (Steiner et al., 2019).
Relatedness: A Pervasive Human Need
As understood from the literature on adolescence, relatedness is a fundamental construct that hinders or facilitates a healthy transition. As a universal phenomenon, philosophers and theorists across disciplines agree that relatedness to others, environment, and self is a pervasive human need. The theory of human relatedness (Hagerty et al., 1993) within the discipline of nursing provides a framework that identifies the phenomenon of relatedness, explains the concepts and characteristics, and generates theoretical propositions. Hagerty et al. (1993) defined relatedness as "an individual’s level of involvement with persons, objects, or groups or natural environments and the concurrent level of comfort or discomfort associated with the involvement" (p. 292). While Hagerty and colleagues’ (1993) theory provides a foundation to help nurses conceptualize the construct of relatedness, it assumes a separation of self from others and the world around them and does not capture the construct of relatedness from a unitary perspective. From a unitary lens, relatedness assumes an interconnectedness of all, where individuals cannot be understood in parts but rather as an integral whole of open systems in a mutual process. These systems are irreducible human-energy fields distinguished by dynamic patterns perceived as waves within a pandimensional nonlinear domain unbounded by space and time (Butcher, 2021). Pandimensional moves away from isolated self-recognizing events, embracing the simultaneous evolution of infinite interconnectedness of the human-environment energy field, including intentional participation in the mutual process. From this standpoint, the construct of relatedness in adolescent development discovers patterns of connection within the human-environment energy field, illustrating awareness and quality of connection with self, others, and the environment. Individuals fluctuate between different levels of relatedness in the energy fields characterized by dynamic flow in a constant mutual process, simultaneously influencing each other. The ebbing and flowing of rhythmic patterns of turbulence and ease in the life process will manifest in well-being. As individuals become aware of the inseparable energy fields in mutual process, they have the power to participate in patterning that co-creates dissonance or harmony (Butcher, 2021; Smith, 2020)
As understood from the unitary lens, where one is always connected, the awareness and positive quality of the connection afford a sense of well-being and ease within the life process. Smith (2020) explained ease as resonant harmony in the flow of human-environmental field patterning characterized by calm and familiar rhythms. In contrast, the feeling of disease occurs when individuals are unaware of or perceive an unwanted quality of connection with their energy fields, producing discomfort, anxiety, and an altered sense of well-being. These feelings of distress imply turbulence within the life process. "Turbulence creates a dissonant commotion in the flow of human-environment field patterning characterized by chaotic and unpredictable change" (Smith, 2020, p. 13). This understanding of relatedness or mutual process recognizes that not all involvement or ease will promote well-being and not all lack of participation or turbulence will foster distress (Hagerty et al., 1993). Relatedness in mutual process then encompasses all connections regardless of function, focusing instead on one’s perception of the experience. The individual’s perception of the quality of the experiences will produce turbulence or ease and determine their level of involvement or intentionality oscillating between varying patterns of relatedness within multiple domains at any given moment.
Hagerty et al. (1993) posited that the level at which one chooses to participate would determine the level of social processes (reciprocity, mutuality, and synchrony) and shape one’s sense of belonging. Though Hagerty’s processes reflect dyadic interactions, they can be assessed from the unitary lens as patterning in mutual process guided by one’s intentionality. The mutual process of relatedness proposes rhythmic patterning of connectedness that evolves from awareness and quality of connection (patterns of relatedness). Through turbulence and ease, one establishes conscious acceptance of the other as they exist in the moment (mutuality). Harmonic congruence ensues when internal flow and external calm are achieved (synchrony). And a sense of belonging is realized when conscious awareness and personal involvement reflect the wholeness of one within their reality, where individuals believe they have an integral role. The social process of belonging transcends disciplines as a universally recognized inherent human motivation necessary to develop and grow (Hagerty et al., 1993).
Relatedness is about sensing a mutual process in various ways, as one’s intentionality or level of engagement with their energy fields directly influences their flow in mutual process with themselves, others, and the environment. Understanding the construct of relatedness from a unitary caring worldview affords nurses a deeper understanding of the nature and direction of change encountered by individuals as they coexist as one with the universe. As a guiding framework, nurses can help adolescents flow through turbulence and recover ease through a new way of experiencing the reality of relatedness, discovering patterns of wholeness and belonging that motivates human life and cultivates creativity and growth.
Unitary Caring Theory
Examining the construct of relatedness through a unitary caring lens requires an intentional, authentic presence open to exploring ways of being in a mutual process. Smith’s (1999) middle-range theory of unitary caring provides a unified platform with the contextual congruence of relatedness and unitary science that nurses can use as their guiding framework for practice. The evolution of her theory sought to answer the question, "What is the quality of being in mutual process that is called ‘caring’ within other theoretical contexts?" (p. 20). Exploring this question addressed the importance of relatedness in nurse caring. This inquiry defined the five assumptions that guided the development of her theory. The five assumptions are:
1) Human beings are unitary or irreducible in mutual process with an environment that is coextensive with the universe, participating knowingly in patterning, and ever-evolving through expanding consciousness (Rogers, 1994).
2) Caring is a quality of participating knowingly in human-environment field patterning (Smith, 1999).
3) Caring is the process through which human wholeness is affirmed and potentiates the emergence of innovative patterning and possibilities (Cowling et al., 2008, p. E44).
4) Caring is a manifestation and reflection of expanding consciousness potentiating greater meaning, insight, and transformative ways of relating to self and others (Cowling et al., 2008).
5) Caring consciousness resonates with the pandimensional universe (Watson & Smith, 2002).
The concepts that emerged from Smith’s (1999) work are: manifesting intention, appreciating pattern, attuning to dynamic flow, experiencing the infinite, and inviting creative emergence. These five concepts became the foundation for the theory of unitary caring.
Manifesting intention is defined as embracing "actions that create a healing environment, preserve dignity, humanity, and reverence for personhood, focus attention to and concern for the other and facilitate authentic presence" (Smith, 2015, p. 511).
Appreciating patterns is "valuing and celebrating wholeness and uniqueness of persons, acknowledging pattern without attempting to change it, recognizing the person as perfect in the moment, being sensitive to the unfolding pattern of the whole, and coming to know the other" (Smith, 2015, p. 512).
Attuning to dynamic flow is sensing where to place focus and attention in a mutual process (Smith, 2015, p. 512). It was originally described as dancing to the rhythms within a continuous mutual process (Smith, 1999, p. 23).
Experiencing the infinite is defined as "pandimensional awareness of co-extensiveness with the universe occurring in the context of human relating" (Smith, 1999, p. 24). It is a recognition that the nurse-patient relationship is sacred, and when we are with others in this way, there are no limits to possibilities (Smith, 2015, p. 512).
Inviting creative emergence is attending the birth of innovative, emergent patterning through affirming the potential for change, nurturing the awareness of possibilities, imagining new directions, and clarifying hopes and dreams.
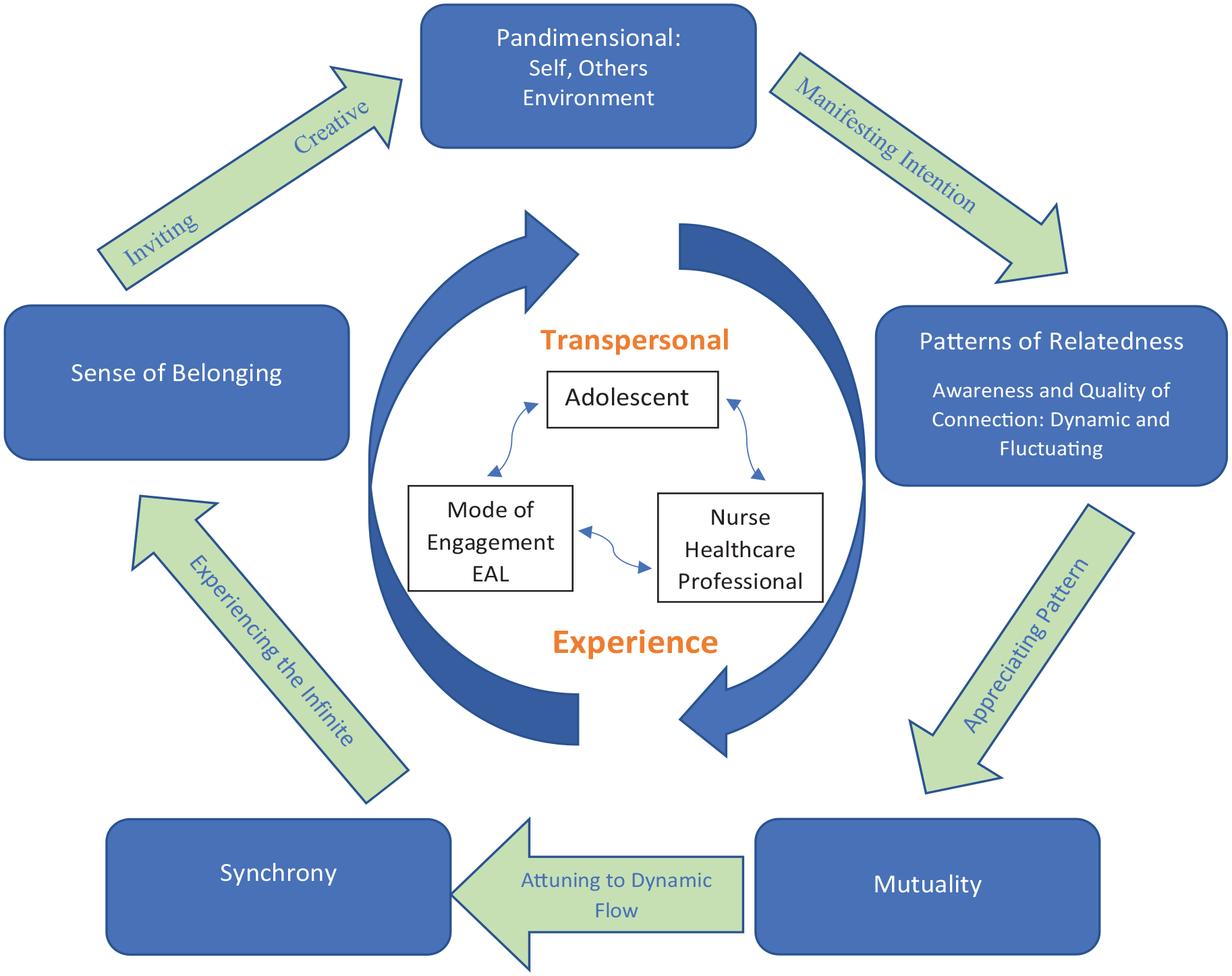
These concepts harmonically flow using the mutual process of relatedness. The proposed unitary caring model of adolescent relatedness (see Figure 1) depicts the mutual process of the pandimensional human-environment energy field. The model informs an intentional, authentic nurse presence, focused on awareness, caring, consciousness, patterning, and meaning, that invites creative emergence and change (Smith, 1999).
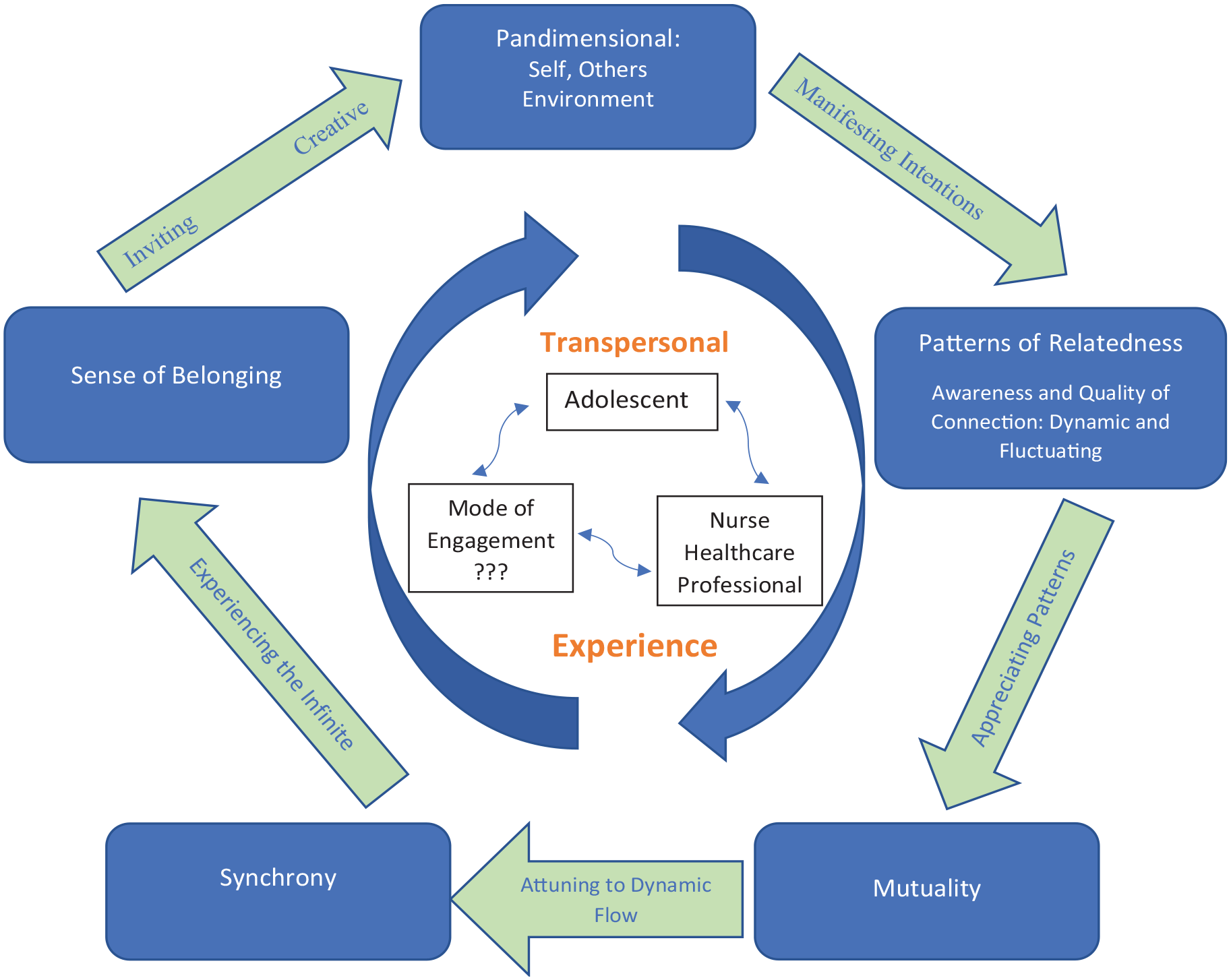
Unitary Caring Model of Adolescent Relatedness (developed by M. G. Mygatt, 2020, during doctoral dissertation synthesis).
Implications for Nursing Practice
With the disturbing backdrop of increasing adolescent mental health conditions and insufficient therapeutic options, nurses are challenged with providing effective quality care. By understanding adolescent development and underlying experiences of adolescence, the uncertainty of the social and environmental landscape, and the challenges of identity formation, nurses will be better equipped to address their needs and understand the importance of relatedness. Furthermore, by embracing the construct of relatedness as a universal phenomenon through which teens survive, develop, and grow, nurses are empowered to explore innovative modes of engagement that address the importance of meaningful connections to self, others, and the environment.
Recognizing that adolescents are often reluctant to seek help from adults, the transpersonal experience (nurse-teen) may require creativity and possibly an indirect encounter or an extension of the nurse to help individuals develop and grow. One such caring nurse practice is equine-assisted learning (EAL). EAL has grown as a therapeutic modality, where grounded and mounted interactions between horses, humans, and the environment are coordinated to help improve psychosocial and emotional distress. Coming together in nature fosters intentional presence. This grounding in the moment supports an open and authentic experience into the unknown, affording an awakening to the present self and the world around them, shedding light on the interconnectedness of all.
Exemplar
EAL facilitates awareness of the interconnectedness of all, where humans, horses, and nature come together unbounded by space and time. The uncertainty and explicit nature of change of the human-environment energy field within the arena create a pandimensional experience where existence and knowing are linked through awareness, intentionality, and interpretation. Horses within close proximity require an intentional presence and awareness of surroundings to engage in purposeful interaction. While manifesting intentions of being with, the triad, horse, adolescent, and nurse or healthcare professional, brings their evolving presence and integrality to the experience of coming to know one another. By recognizing patterns when faced with challenges and exploring new ways of responding by listening and cultivating patience, they flow through resonancy of turbulence and ease. The triad begin to establish a safe space of trial and error, where mutual respect and boundaries evolve.
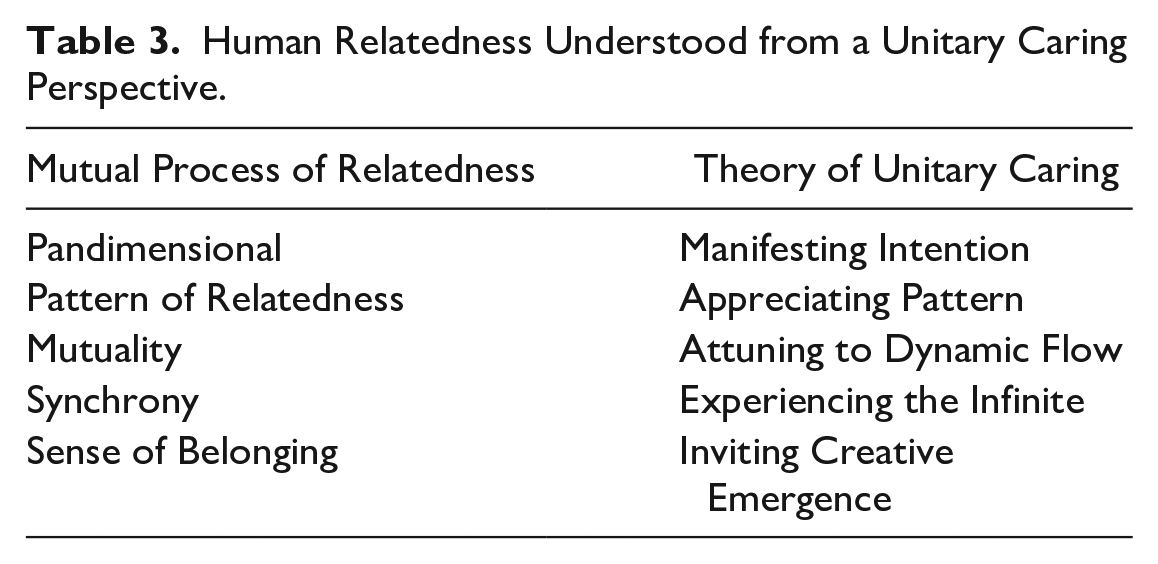
These patterns of relatedness are dynamic and fluctuating. By appreciating these patterns, the triad reaches an understanding of mutuality where the focus is on wholeness, being with and in a relationship. By attuning to dynamic flow in the relationship, each member of the triad senses where to place focus and intention within the mutual process. Here, the client and horse connection flows in harmony, completing tasks and recognizing each other’s role as integral to the other. There is rhythmic flow in harmonic synchronicity by attuned meaningful connections of these experiences and the human environment consciousness in the mutual process. This pattern of synchronicity invites deep human-horse, human-human, and human-to-environment connection as pandimensional awareness of co-existence with the universe that occurs in the context of human relating. This co-existence fosters a sense of belonging where one believes their involvement is an integral part of the experience (see Table 3).
Human Relatedness Understood from a Unitary Caring Perspective.
Ultimately, this sense of belonging invites the creative emergence of change. Adolescents become aware of the mutual process and patterns of the existential relational experiences from EAL and learn to translate this into their life outside the equine arena.
The unitary caring model, illustrated in Figure 1, is the conceptual model of unitary caring of adolescent relatedness that can be a theoretical template for adolescent nursing care.
Figure 2 depicts the conceptual model of unitary caring of adolescent relatedness as used in the exemplar with EAL proposed to inform the construct of relatedness that unfolds during EAL.
Unitary Caring Model of Adolescent Relatedness With EAL (developed by M. G. Mygatt, 2021, during doctoral dissertation synthesis).
Conclusion
The alarming adolescent trends, risk factor data, and global pandemic concern irrefutably confirm that our teens are struggling, and existing strategies to address their needs are not working. Recognizing the urgency for creative caring praxis and innovative therapeutic modalities, the authors explored the construct of relatedness in adolescence from a unitary caring lens and developed a transtheoretical model as a relational caring ontology. The proposed unitary caring model acknowledges adolescents from a unitary lens espousing irreducible human wholeness and aims to guide and expand nursing knowledge and guide practice. The authors posit that by understanding adolescents from this unitary perspective, nurses may experience new ways of being, thinking, and doing that may unlock creativity and enhance praxis.
Nurses are at the forefront of innovation, tasked with pioneering novel approaches that engage and sustain a population often resistant to care. As nurses embrace the theoretical and philosophical construct of relatedness as a foundation for adolescent growth, development, and well-being, the adolescent unitary caring model will help intentionally create an environment grounded in wholeness and allow the transpersonal nurse-patient experience to emerge.
True Belonging is. . . . belonging to yourself so deeply that you can share your most authentic self with the world and find sacredness in both being a part of something and standing alone in the wilderness. True belonging doesn’t require you to change who you are; it requires you to be who you are. ~Brené Brown (2017, p. 40)